
Abstract
Background:
Iodine deficiency is one of the most prevalent causes of intellectual disability and can lead to impaired thyroid function and other iodine deficiency disorders (IDDs). Despite progress made on eradicating iodine deficiency in the last decades in Europe, IDDs are still prevalent. Currently, evidence-based information on the benefit/harm balance of IDD prevention in Europe is lacking. We developed a decision-analytic model and conducted a public health decision analysis for the long-term net benefit of a mandatory IDD prevention program for the German population with moderate iodine deficiency, as a case example for a European country.
Methods:
We developed a decision-analytic Markov model simulating the incidence and consequences of IDDs in the absence or presence of a mandatory IDD prevention program (iodine fortification of salt) in an open population with current demographic characteristics in Germany and with moderate ID. We collected data on the prevalence, incidence, mortality, and quality of life from European studies for all health states of the model. Our primary net-benefit outcome was quality-adjusted life years (QALYs) predicted over a period of 120 years. In addition, we calculated incremental life years and disease events over time. We performed a systematic and comprehensive uncertainty assessment using multiple deterministic one-way sensitivity analyses.
Results:
In the base-case analysis, the IDD prevention program is more beneficial than no prevention, both in terms of QALYs and life years. Health gains predicted for the open cohort over a time horizon of 120 years for the German population (82.2 million inhabitants) were 33 million QALYs and 5 million life years. Nevertheless, prevention is not beneficial for all individuals since it causes additional hyperthyroidism (2.7 million additional cases). Results for QALY gains were stable in sensitivity analyses.
Conclusions:
IDD prevention via mandatory iodine fortification of salt increases quality-adjusted life expectancy in a European population with moderate ID, and is therefore beneficial on a population level. However, further ethical aspects should be considered before implementing a mandatory IDD prevention program. Costs for IDD prevention and treatment should be determined to evaluate the cost effectiveness of IDD prevention.
Introduction
Iodine deficiency is one of the most prevalent causes of mental development disorders in children causing poor school performance and reduced work capacity. It can lead to impaired thyroid function and goiter, as well as other iodine deficiency disorders (IDDs) (1). In addition, iodine deficiency is associated with spontaneous miscarriage, stillbirth, and perinatal mortality (2).
Switzerland was the first European country to introduce iodized salt for the prevention of goiter in 1922. One year later, the prevalence of goiter decreased in schoolchildren receiving iodized salt on a regular basis (3). Since then, substantial progress has been made in the last decades in eliminating iodine deficiency. However, IDDs, such as goiter and thyroid nodules, are still prevalent in European countries (4).
There are several studies on the efficacy of IDD prevention programs (2,5). However, to our knowledge, there is no public health study available, investigating the long-term effectiveness of IDD prevention programs including all patient-relevant outcomes, such as avoided IDDs or quality of life (6). The empirical evidence on the effectiveness of population-based programs for primary prevention is limited. For example, relevant effects for individuals and society, such as diseases avoided, are usually only observable in the distant future. Therefore, most empirical IDD monitoring studies are limited on intermediate surrogate endpoints, such as the median urinary iodine concentration of a population, which cannot directly be linked to patient-relevant endpoints (7). In addition, prevention programs may also cause harm (8). Therefore, there is a need for a comprehensive benefit/risk assessment, including the entire spectrum of IDDs and their consequences on a population level.
Decision-analytic modeling is an approach that allows for synthesizing current evidence to support decision-making by including all available interventions (e.g., therapeutic or preventive strategies) and all possible health consequences of the different alternatives and to compare these interventions with regard to the outcome of interest (9,10). Decision analysis can be used to combine evidence from clinical trials and epidemiological studies and to extrapolate efficacy beyond the time horizon of observational or monitoring studies. A comprehensive decision-analytic model can transfer evidence from one health care system to another (e.g., to another country) (10). In addition, a decision-analytic model allows simultaneous consideration of multiple fatal and nonfatal outcomes, by generating integrative health measures, such as quality-adjusted life years (QALYs) (11).
Currently, comprehensive benefit/harm analyses considering the full effects of a population-wide IDD prevention program on the population's life expectancy and quality of life are lacking (6). Therefore, the aim of this public health assessment was to develop a decision-analytic model (10,12) to evaluate the long-term population net benefit of a mandatory IDD prevention program for the German population, as a case example for a European country with moderate iodine deficiency.
Methods
Decision-analytic framework
We developed a decision-analytic state-transition cohort model with annual time cycles simulating the incidence and consequences of IDDs in the absence or presence of mandatory iodine fortification of salt (i.e., iodization of household salt and salt in processed food regulated by law) as an IDD prevention program in an open population, allowing the simulation of new children born into the cohort. The target population of the model consists of individuals with current demographic characteristics in Germany and with moderate iodine deficiency as an example for a European country.
We chose a state-transition cohort model as model type, because IDDs can be well described in terms of (health) states and respective transition probabilities. We performed a cohort simulation, as the number of health states was moderate (12,13).
The decision model allows for simulating three different populations over time. Model 1 (“open cohort model”) includes an open population with both the currently alive German population and their children born during the analytic time horizon. We did not consider immigration and emigration in our open cohort model. Model 2 (“newborn model”) simulates a closed newborn cohort starting at birth. Model 3 (“closed cohort model”) includes a closed population reflecting the age structure of the current German population and age-specific prevalence of IDDs of a moderate iodine-deficient population without consideration of new births.
Our primary net-benefit outcome reflecting the benefit/harm trade-off was undiscounted gains in QALYs predicted over a time horizon of 120 years. We performed scenario analyses with discounting applying reduced weights to future health gains and losses (i.e., benefits and harms) compared with those that occur in the present (14). We estimated total and incremental QALYs as well as total and incremental life years for the different cohort simulations.
Furthermore, we calculated cumulative incidences for thyroidectomies, cases of goiter/benign thyroid nodules, cases of intellectual disability, cases of hypothyroidism, stillbirths/miscarriages, and additional cases of hyperthyroidism after the implementation of a mandatory IDD prevention program in the open cohort model. The base-case analysis was performed without discounting. In further scenario analysis, we applied a 0%, 3%, and 5% discount rate to reflect societal preferences giving more weight to the lives (and life years) in the present than in the future.
International guidelines for good practice in decision-analytic modeling (9,15) suggest that the time horizon of a decision-analytic model should be long enough to include important differences between the long-term health consequences of alternative options. As IDDs and their prevention can have an important impact on quality of life throughout a person's life and their newly born descendants, we used model 1 with an open cohort for our base-case analysis. This allowed us to consider the complete public health effect of the prevention program on the currently living population as well as the partial effects accumulated by future generations within the analytical time horizon of 120 years.
In additional scenario analyses, we performed closed cohort simulations with a lifelong time horizon using the newborn model (model 2) and the closed population model (model 3). Current guidelines suggest that half-cycle correction should be used in the first cycle and in the final cycle of a state-transition model if not using a lifetime horizon (12). Therefore, we used half-cycle correction to minimize bias due to cycle length. Reporting was based on the modeling guidelines of the ISPOR-SMDM Joint Modeling Good Research Practices Task Force (9,12,15 –17). The study received ethical approval from the Research Committee for Scientific and Ethical Questions at the UMIT – University for Health Sciences, Medical Informatics and Technology, Hall in Tirol, Austria.
The EUthyroid decision model
The model structure, health states, and transitions of the state-transition model are based on 2 surveys among 13 clinical experts and additional expert interviews. The natural history model simulates potential health consequences related to iodine deficiency occurring in the absence of a population-wide mandatory IDD prevention program. The natural history model serves as a comparator strategy to calculate incremental benefits (QALYs gained, life years gained, and averted cases of IDD) arising from an IDD prevention program. The model part simulating the consequences of an IDD prevention program adopts the same structure and the same parameters as the natural history model but differs in model parameter values to account for health effects of IDD prevention. The state-transition diagram of the model in Figure 1 shows the health states and transition pathways between the health states.
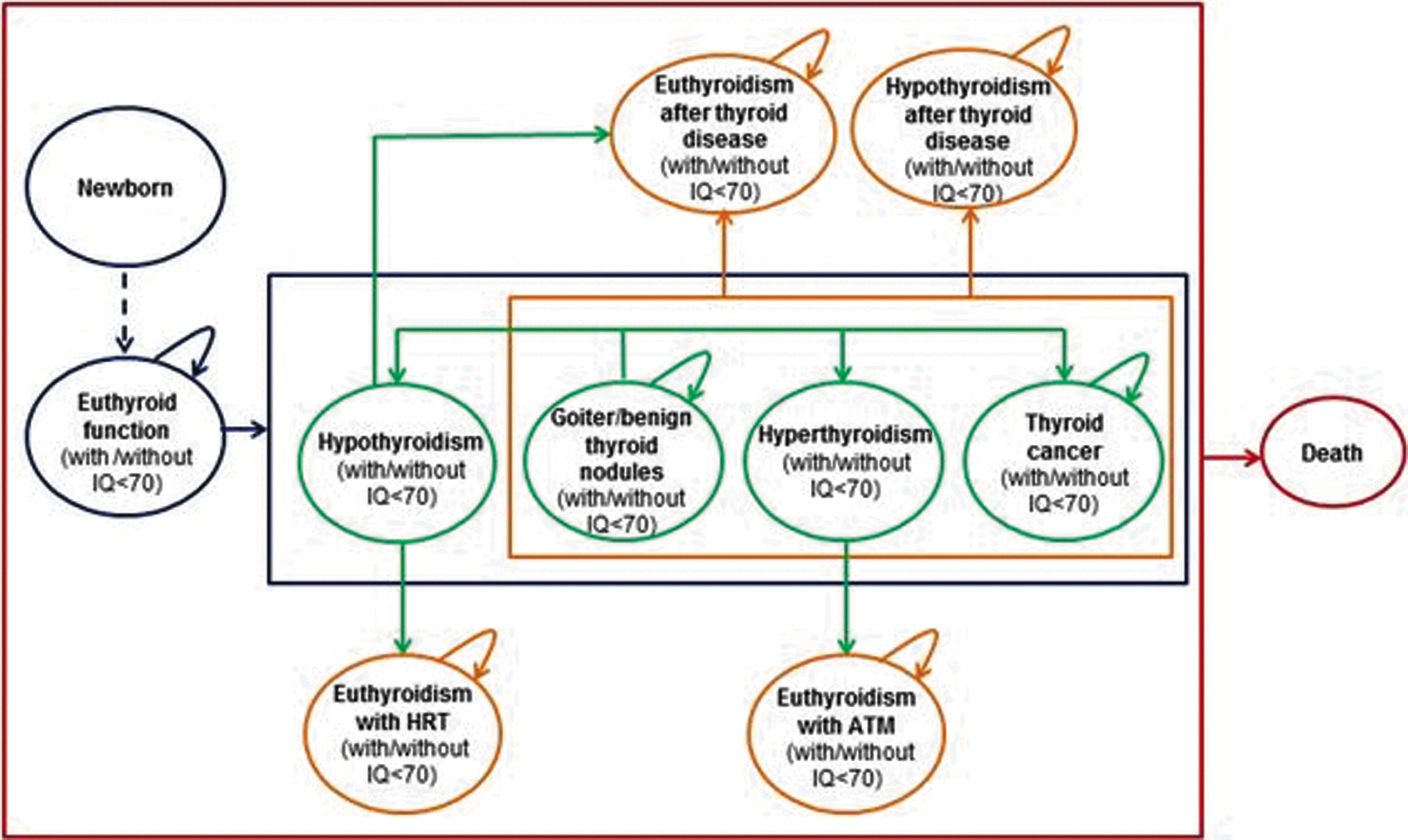
State-transition diagram of the EUthyroid state-transition model. Individuals progressing through the model can move from euthyroid function (with or without intellectual disability) to any health state in the blue box and to the health state euthyroidism after thyroid disease (with or without intellectual disability) or hypothyroidism after thyroid disease (with or without intellectual disability) from each health state in the orange box according to different transition probabilities between the different health states. Individuals can die in each health state in the red box and move to the state death. Causes of death considered in the model are non-IDD-related mortality, thyroid cancer mortality, and deaths due to thyroidectomy. Green bubbles represent different IDDs and diseases potentially related to iodine deficiency within the model. The blue bubbles represent the health states for persons with normal thyroid function (with or without intellectual disability) and persons in the newborn health state. Orange bubbles represent health states to which a person can move after the treatment of a thyroid disease. A person will stay in this health state until death. The red bubble represents the death state. Stillbirths are not implemented as health states but captured via transition rewards. ATM, antithyroid medication; HRT, hormone replacement therapy; IDD, iodine deficiency disorder; IQ, intelligence quotient.
The model considers the following mutually exclusive health states: newborn, euthyroid function, goiter/benign thyroid nodules, hypothyroidism, hyperthyroidism, thyroid cancer, hypothyroidism after thyroid disease (divided into: hypothyroidism after thyroid cancer, hypothyroidism after hyperthyroidism, hypothyroidism after goiter/benign thyroid nodules), euthyroidism after thyroid disease (divided into: euthyroidism after thyroid cancer, euthyroidism after hyperthyroidism, euthyroidism after goiter/benign thyroid nodules), euthyroidism with antithyroid medication (ATM), and euthyroidism with hormone replacement therapy (HRT).
Stillbirths are not included as health states but are accounted for via negative transition rewards. All health states except the newborn state, where individuals are only staying in their first year of life, are further divided into states with and without intellectual disability (i.e., intelligence quotient [IQ] below 70). Each health state, except that of newborns, consists of 120 tunnel stages representing different years of age to allow cohort simulation of populations with a heterogeneous age distribution.
In the newborn model (model 2), all individuals start in the newborn state and move to the health state euthyroid function (with or without intellectual disability) within their first year of life. In the consecutive years, individuals in the euthyroid function state can stay in this health state until death or move to one of the other health states within the model representing different IDDs (with or without intellectual disability). In the closed population model (model 3), the population starts at different ages and in different health states reflecting the population's age distribution and age-specific IDD prevalence data observed in a moderately iodine-deficient population.
In the open cohort model (model 1), newly born descendants enter the open population via the newborn health state. If a woman of the current population becomes pregnant, she can have a live birth or stillbirth according to German data on stillbirths and fertility. Children born without intellectual disability move to the health state normal thyroid function without intellectual disability, and subsequently may transit to any other health state without intellectual disability within the model. If a child is born with intellectual disability, newborns move to euthyroid function with intellectual disability and subsequently can move to any other health state with intellectual disability.
The health state goiter/benign thyroid nodules include toxic and nontoxic goiter as well as diffuse and nodular goiter and all types of benign thyroid nodules. If a person has no symptoms due to goiter or benign thyroid nodules, we assumed that the person stays in this health state with continued monitoring. However, persons under monitoring can also move to the health states hypothyroidism, hyperthyroidism, or thyroid cancer according to different progression probabilities. Persons with symptoms from goiter, such as tracheal compression or dysphagia, are treated with thyroidectomy or radioactive iodine (RAI) therapy. Persons treated with thyroidectomy or RAI therapy can develop hypothyroidism and move to the health state hypothyroidism after goiter/benign thyroid nodules or to the health state euthyroidism after goiter/benign thyroid nodules, if the thyroid gland is working well after therapy.
Individuals can be in or move to the health state hyperthyroidism, including Graves' disease and thyroid autonomy. If hyperthyroidism is diagnosed, a person can be treated with antithyroid medication (ATM), thyroidectomy, or RAI therapy. Persons with ATM will move to the health state euthyroidism with ATM. Persons receiving thyroidectomy or RAI therapy can develop hypothyroidism and move into the health state hypothyroidism after hyperthyroidism or to the health state euthyroidism after hyperthyroidism if the thyroid gland is working well after therapy.
Persons can be in or move to the health state hypothyroidism, including Hashimoto's disease. If hypothyroidism is diagnosed, a person may receive temporary or long-term hormone replacement therapy (HRT). Persons with temporary HRT transit to the health state euthyroidism after hypothyroidism. Persons with long-term HRT transit to the health state euthyroidism with HRT.
Persons can be in or move to the health state thyroid cancer. All patients in this health state undergo thyroidectomy and a certain proportion of patients receive subsequent RAI therapy. After treatment, persons can develop hypothyroidism and move to the health state hypothyroidism after thyroid cancer or move to the health state euthyroidism after thyroid cancer, if the thyroid gland is working well after therapy. In case of a relapse, the patient will stay in the health sate thyroid cancer and progress through the different treatment options again.
In our model, individuals in the health states euthyroidism after thyroid disease, hypothyroidism after thyroid disease, euthyroidism with HRT, and euthyroidism with ATM remain in these health states with continuous monitoring until death. In each health state, a person can die and move to the death state. Causes of death considered in the model are age-specific non-IDD-related mortality, thyroid cancer mortality, and deaths due to thyroidectomy.
Model parameters
All model parameters are summarized in Table 1. For all possible health states, we defined and collected information, including data on the prevalence, incidence, mortality, and utilities (health-related quality-of-life indices).
Parameters of the EUthyroid Model
Legend for model parameters is also shown in the Supplementary Material C.
ATM, antithyroid medication; CI, confidence interval; HRT, hormone replacement therapy; IDD, iodine deficiency disorder; IQ, intelligence quotient; RAI, radioactive iodine.
Natural history
The core part of the model is a natural history model simulating potential iodine deficiency-related health consequences occurring in the absence of a mandatory population-wide IDD prevention program. We included age-specific prevalence and incidence data from moderately iodine-deficient countries. We used the incidence data for hypothyroidism, hyperthyroidism, and thyroid cancer from Denmark in the year 1990 before the implementation of an IDD prevention program (8,18,19). Prevalence data for intellectual disability, goiter, and benign thyroid nodules were derived from studies conducted in moderately iodine-deficient regions in Portugal and Denmark (19,20).
Incidence and prevalence of thyroid cancer were reported for age groups of 5 years and the incidence of hypothyroidism and hyperthyroidism was reported in age groups of 10 years. In these cases, we assumed the same prevalence/incidence of the disease for all ages in one cumulated age group (8,19).
The DanThyr study reported prevalence of goiter and thyroid nodules for women in four age groups (18–22 years, 25–30 years, 40–45 years, and 60–65 years) and men in one age group (60–65 years) (19). Therefore, logarithmic functions were fitted to the respective study data for the estimation of the prevalence and incidence rates in every age group. In addition, we assumed a proportional factor for the age groups 60–65 years to calculate age-specific prevalence for men in the other age groups. We assumed a 1:1 sex ratio to estimate an average overall prevalence for both sexes.
Age-specific incidence data of goiter and benign thyroid nodules were unavailable and therefore calibrated to match age-specific prevalence data. Unavailable age-specific prevalence data of hyperthyroidism and hypothyroidism were calibrated from age-specific incidence data. Age-specific prevalence data for all post-treatment states were unavailable as well and therefore were derived from predictions of the newborn model.
We also included patient pathways and associated transition probabilities estimated from the literature [e.g., clinical guidelines (21 –29)]. If we were not able to find evidence in the literature, we asked clinical experts to provide parameter estimates.
We used age- and sex-specific mortality data from the official statistical life tables for Germany (30).
Epidemiological data, treatment data, and related references are summarized in Table 1.
Effectiveness
We performed a systematic literature review in PubMed/MEDLINE, Tufts CEA Registry, NHS EED, and Cochrane searching for studies on the effectiveness of IDD prevention programs (details provided in the Supplementary Material A). We found a recently conducted comprehensive review and meta-analysis by the World Health Organization (WHO) (31) assessing the effects and safety of consumption of iodized salt in IDD prevention. In addition, we found a Cochrane review and meta-analysis by Harding et al. (32) comparing women with and without iodine supplementation during pregnancy in terms of different health outcomes for mother and child. All primary studies that we identified by our literature search were already included in the meta-analysis of these two reviews. We used relative risks and odds ratios extracted from Aburto et al. for the effect of salt iodization on the incidence of intellectual disability, hypothyroidism, hyperthyroidism, goiter, and benign thyroid nodules (31).
In the absence of a study evaluating the effect of salt fortification on miscarriage, we used results reported by Harding et al. for the effect of an IDD prevention program on the incidence of stillbirth/miscarriage (32).
To account for a potential shift toward less severe cancer types due to iodine supplementation, we used a multiplicative reduction factor on the German thyroid cancer mortality derived from relative survival data from the Munich Cancer Registry (MCR), Germany before and after the implementation of an IDD prevention program (33).
The effects of IDD prevention on the incidence of iodine deficiency-related health conditions and events were included in the model by multiplying incidence parameters with risk decreasing or increasing factors derived from the literature and the MCR. Effectiveness parameters and related references are summarized in Table 1.
Utilities
The health-related quality of life can be expressed as a single index number, so-called health utility. Utilities are measured on a cardinal scale between 0 (death) and 1 (full health) reflecting patient preferences for a given state of health. We conducted a comprehensive systematic literature review in PubMed/MEDLINE, Tufts CEA Registry, NHS EED, and Cochrane to identify studies that reported health state utilities for several health states associated with iodine deficiency (34,35). The identified studies report health utility values related to hypothyroidism (n = 7), hyperthyroidism (n = 2), goiter (n = 1), thyroid nodules (n = 11), thyroid cancer (n = 16), and intellectual disability (n = 5).
We extracted utilities for goiter/benign thyroid nodules, hyperthyroidism (with long-term ATM), hypothyroidism (with long-term HRT), thyroid cancer, thyroidectomy, RAI therapy, temporary HRT, stillbirth/miscarriage, and for having an IQ <70 from the studies with the most appropriate measures, including time trade-off, standard gamble, Health Utilities Index MARK 2, or expert opinion. For thyroidectomy, RAI therapy, temporary HRT, and stillbirth/miscarriage, we used absolute utility decrements applied for one cycle. The utility decrement due to stillbirth/miscarriage was only applied for one cycle to mothers. The utility of having IQ <70 was used as a multiplicative factor on other utility parameters. For euthyroid health states, we assumed age-specific utilities from the general population derived from a study by Huber et al. (36) evaluating the health perception in a representative sample of the general German population.
In addition, we implemented age-specific utilities as a multiplicative factor on disease-specific utilities applied in noneuthyroid health states. Since rating scale values tend to underestimate utilities compared with utilities generated by standard gamble or time trade-off, we adjusted the rating scale value using a power function developed by Torrance et al. (37). Utility parameters and related references are summarized in Table 1.
Model analyses
Base-case analysis
In the base-case analysis, IDDs are present in the current population considering the prevalence data of a moderate iodine-deficient country. To capture the full public health effect of IDD prevention on intellectual disability as well, we applied the open cohort model (model 1), which also simulates descendants born newly with or without intellectual disability within the analytic time horizon.
Comparative long-term effectiveness was estimated as total and incremental QALYs, as well as total and incremental life years. Numbers were calculated both per index person (i.e., persons in the starting cohorts) and for the complete population. In addition, we predicted cumulative events avoided by the prevention strategy over time, including thyroidectomies, stillbirths/miscarriages, and cases of IDDs (goiter/benign thyroid nodules, hypothyroidism, hyperthyroidism, and intellectual disability).
Sensitivity analyses and scenario analyses
To assess the robustness of our results, we performed a systematic and comprehensive uncertainty assessment. We conducted multiple deterministic one-way sensitivity analyses to evaluate the influence of specific uncertain parameters on QALYs and life years gained. We used lower and upper confidence interval (CI) limits from the published literature. If no CIs were available, we calculated the range for the sensitivity analysis as +/− 20% of the parameter point estimate (16). Parameter ranges used in sensitivity analyses are summarized in Table 1.
The results of the one-way sensitivity analyses are summarized in a tornado diagram showing horizontal bars quantifying the spread of the predicted outcome caused by the variation of single-model parameters within their limits of uncertainty. The vertical axis shows all varied parameters sorted by descending width of the outcome spread. Thus, the topmost parameter with the longest bar indicates the most influential of the varied parameters (16). A vertical line cutting through all horizontal bars represents the outcome of the base-case (expected value of the base-case analysis).
In a multivariate deterministic sensitivity analysis, we evaluated the long-term effectiveness of IDD prevention in a best- and worst-case effectiveness scenario with the open population model. For the worst-case scenario, all effectiveness parameters were simultaneously set to their upper CI limit, while for the best-case scenario, all were simultaneously set to the lower limit.
In further scenario analyses, we assessed the effect of an IDD prevention program in different (restricted) cohorts. We applied the newborn model (model 2) starting with all individuals in the newborn state and we also applied the closed population model (model 3), simulating the currently alive population without newborns entering the model. According to German guidelines (38), we also conducted scenario analyses using a discount rate of 0%, 3%, and 5%, respectively, to reflect reduced preferences for future outcomes.
Model programming, debugging, and validation
The decision-analytic model was programmed using TreeAge Pro 2018 (TreeAge Software, Inc., Williamstown, MA). Current international guidelines for best practices in decision-analytic modeling were applied to validate the model (9,12,15,16). Guidelines recommend five main types of validation: face validity (extent to which a model corresponds to current evidence), internal validity (addresses whether the model behaves as intended and has been implemented correctly), cross validity (comparing a model with the results of other models), external validity (the predicted outcomes of the model are compared with real-world data), and predictive validity (uses the model to forecast events and compare outcomes with the actual ones) (9,12,15,16).
Technical validation was performed by the developer and additionally by an independent modeling researcher. For the current study, the model structure was presented to and discussed with experts in endocrinology, epidemiology, and decision-analytic modeling to assure face validity. Internal validity was tested using technical debugging and various plausibility checks, which yielded expected results (e.g., when reproducing input data). The population extrapolation was compared with national population statistics forecasts. The disease model under a policy of no prevention was externally validated by comparing model outcomes for the start year (number of thyroidectomies, number of goiters) with published data. The numbers of cancers, hypothyroidism and hyperthyroidism, goiters and thyroidectomies were checked for plausibility relative to each other over time. We could not apply cross-model validation since, to our knowledge, there is no other comprehensive decision-analytic model for the evaluation of an IDD prevention program thus far.
Results
Base-case analysis
The evaluation of the open cohort model over a time horizon of 120 years yielded the average amount of QALYs and life years gained per index-person in the starting cohort, by a mandatory population-wide prevention program in a population with moderate iodine deficiency.
Table 2 presents net benefits of the IDD prevention program compared with no prevention. The IDD prevention program is shown to be more beneficial than no prevention, both in terms of life years and QALYs. Undiscounted health gains predicted per index person of the open cohort are 0.06 life years and 0.40 QALYs, respectively. Thus, for the total population in Germany (∼82.2 million persons), health gains would add up to ∼5 million life years and 32 million QALYs, respectively, over a time horizon of 120 years.
Results of the Base-Case Analysis (Open Cohort Model) per Index Person
To determine the results for the total population, values need to be multiplied by the total number of individuals in the initial population (e.g., Germany: around 82.2 million). Time horizon: 120 years.
QALY, quality-adjusted life years.
Table 3 displays the estimated total incremental benefits and incremental harms of the IDD prevention program during the 120-year time horizon in the German population. The IDD prevention program leads to the prevention of an estimated benefit of 29 million cases of goiter/benign thyroid nodules avoided, and to an estimated harm of 2.7 million additional cases of hyperthyroidism. In other words, based on our decision analysis, for 11 cases of goiter/benign thyroid nodules avoided, there is 1 additional case of hyperthyroidism. Similarly, for two cases of intellectual disability avoided, there are three additional cases of hyperthyroidism.
Total Effect During the 120-Year Analytic Time Horizon in the German Population (Open Cohort Model)
Overall, the IDD prevention program leads to ∼32 million QALYs (5.0 million life years) gained, which relates to an incremental benefit/harm ratio around 12 QALYs gained per additional case of hyperthyroidism.
Figure 2 shows the predicted cumulative effects of an IDD prevention program for QALYs, life years, and several ID-related health outcomes over time after program implementation. Each graph presents undiscounted results from the base-case analysis (solid line) as well as results from the best-case (dotted line) and worst-case (dashed line) scenario analyses. As indicated by the graphs, IDD prevention is predicted to gain additional QALYs and life years and to reduce thyroidectomies, goiter/benign thyroid nodules, intellectual disability, and stillbirths. On the contrary, the model predicts an increase in hyperthyroidism, and hypothyroidism remains unaffected under base-case assumptions.
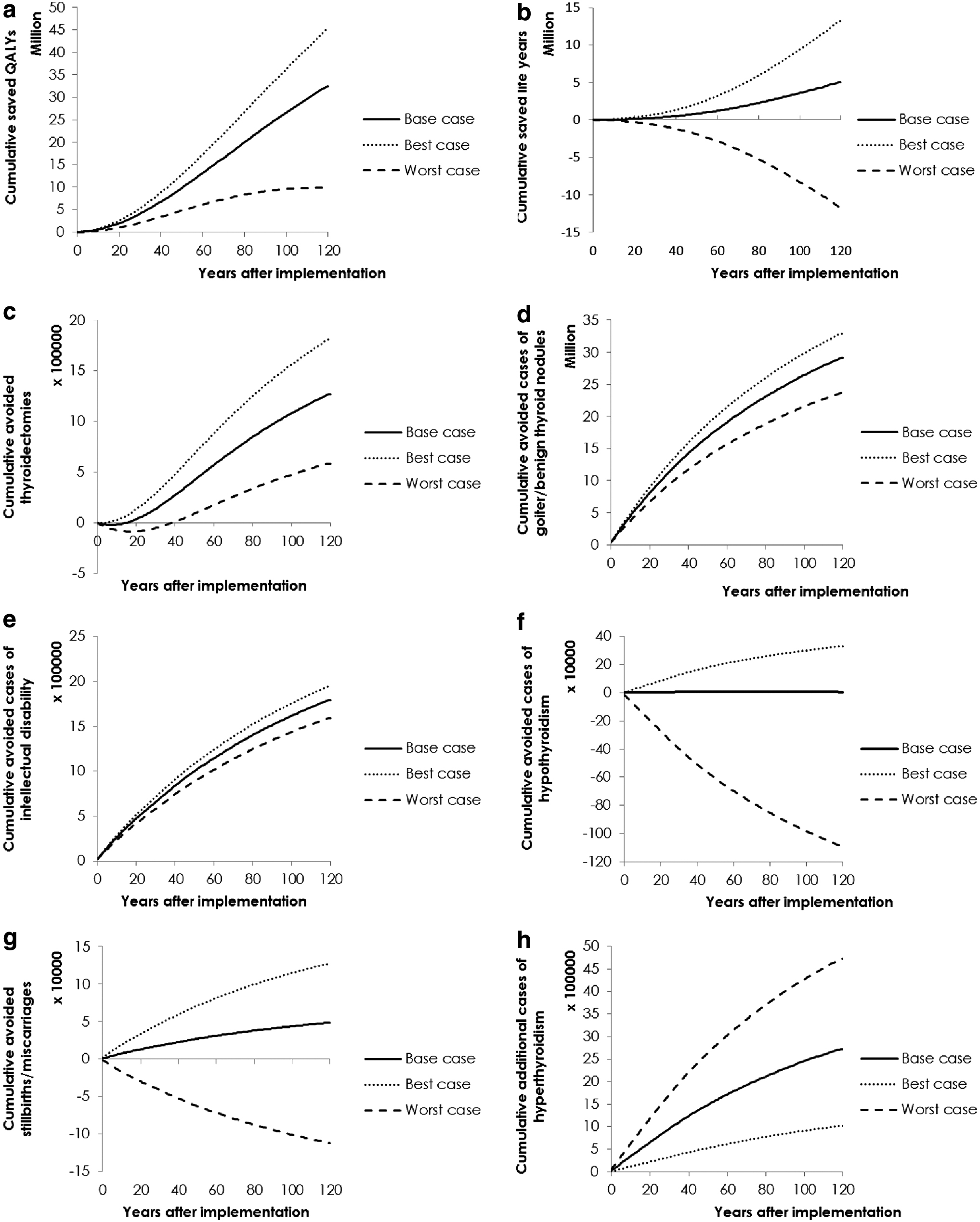
Cumulative outcomes of the IDD prevention program by year after implementation; German population, with moderate iodine deficiency (open cohort model). Solid lines represent results for the base-case analysis (open cohort model). Dashed lines represent worst-case scenario analyses simultaneously using the upper limits of the [CI] of the IDD prevention effectiveness parameters. Dotted lines represent best-case scenario analyses simultaneously using the lower limits of the [CI] for the effect of an IDD prevention program on quality-adjusted life years (
Sensitivity analyses and scenario analyses
Tornado diagrams displaying the effect of single-parameter uncertainties on incremental QALYs and life years are displayed in the Supplementary Material B. For QALYs, the variation of the utilities in the health state goiter/benign thyroid nodules had the greatest effect. Most influential parameters for the effect on life years were the multiplicative effect of iodine prophylaxis on the probability that a pregnant woman has a stillbirth/miscarriage and the stillbirth/miscarriage to live birth ratio.
Results of the best- and worst-case scenario are presented in Table 4. The worst-case scenario yielded a decrease of incremental life years but still an increase of QALYs. The results of additional scenario analyses (newborn model and closed population model) are summarized in Table 5. The IDD prevention program is not beneficial in terms of life years compared with no prevention in the newborn model and the closed population model. However, there is still an increase of QALYs in both models.
Results of the Best-Case and Worst-Case Scenario in the Open Cohort Model
Results of the open cohort model including the lower (best-case) and the upper (worst-case) values of the CIs (in favor of the IDD prevention strategy) for all effectiveness parameters (scenario analyses). Results are total numbers per average person in the initial population of the open cohort. Time horizon: 120 years.
Incr., incremental.
Results of the Newborn Model and the Closed Cohort Model
Results of the newborn model and the closed cohort model (scenario analyses). Results are total numbers per average person in the initial population of the open cohort. Time horizon: 120 years.
Further scenario analyses showing the effect of different discount rates are summarized in the Supplementary Material D. None of our three models predicted gains in life years, when a 5% discount rate was applied. However, all models still predicted gains in QALYs.
Discussion
We developed a decision-analytic Markov state-transition model to evaluate the long-term population effectiveness of an IDD prevention program based on mandatory iodine fortification of salt for the German population with moderate iodine deficiency. To date, no decision-analytic model evaluating the full impact of a population-based approach for IDD prevention has been published (6).
Based on our decision analysis, we found that the implementation of the IDD prevention program yields an increase both in QALYs and life years. These results were robust in most scenario and sensitivity analyses. In addition, our results suggest that thyroidectomies, cases of goiter/benign thyroid nodules, cases of intellectual disability, cases of hypothyroidism, and stillbirths/miscarriages could be reduced by implementing an IDD prevention program. On the contrary, the mandatory implementation of a nationwide IDD prevention program may generate some harm through additional cases of hyperthyroidism. Overall, the IDD prevention program leads to an incremental benefit/harm ratio of ∼12 QALYs gained per additional case of hyperthyroidism.
The WHO stated that IDDs negatively affect quality of life, and that universal salt iodization is the most effective method for the prevention of IDDs (39). Our results underline that from a public health perspective, IDD prevention yields a reduction of thyroidectomies, goiter/benign thyroid nodules, intellectual disability, and stillbirths, and an increase of QALYs and life years within a moderately iodine-deficient population.
There are only a limited number of systematic benefit/harm analyses on IDD prevention programs available. Monahan et al. evaluated the benefits and costs of iodine supplementation for pregnant women in a mildly to moderately iodine-deficient population in terms of IQ points. They concluded that iodine supplementation is beneficial in terms of IQ points gained in the U.K. context (40).
Correa et al. estimated the value of improvements due to an IDD prevention program and found an increase of the IQ, reduction of cretinism, and an increase of the income. In addition, they found that iodization was more effective than a number of other interventions, for example, education, infant nutrition, and physical capital (39).
However, none of these studies evaluated an IDD prevention program on the population level based on iodine fortification of salt in a European country with moderate iodine deficiency, including all relevant long-term consequences of iodine deficiency. In addition, a significant strength of our analysis is the systematic, evidence-based and comprehensive evaluation of the long-term effectiveness of an IDD prevention program compared with no prevention.
We conducted the first decision-analytic modeling study that captures the full effect on intellectual disability by simulating children born newly into the cohort with or without intellectual disability. The longer time horizon of the model additionally captures the effect of a salt fortification program on multiple generations. In addition, our model allows for a newborn cohort simulating the effect of an IDD prevention program on newborns and a closed population cohort reflecting the current German population without consideration of new births.
Furthermore, we adjusted the survival for health-related quality of life to integrate diverse patient-relevant benefit and harm outcomes in a single benefit/harm measure and considering a nonfatal health outcome. Reporting composite measures, such as QALYs, can help decision makers to evaluate the benefit/harm trade-off, since one measure allows integrating all relevant benefits and harms of an action.
As all decision analyses, our study has several limitations regarding modeling in general, and also with regard to the specific model structure, the modeling of our risk functions, the choice of IDDs, data inputs, and validation, which need to be considered.
First, the model structure and health states within the model are based on two surveys among clinical experts. We assume that persons of the cohorts we modeled can only be treated once in a lifetime for any thyroid disorder, except thyroid cancer, before they move to a permanent post-treatment health state, in which they are monitored continuously until death. Therefore, our model does not consider the development of the same or any other disease for a second time, except in yet untreated patients, who are under surveillance because of goiter/nodules. This may lead to an underestimation of the benefits of IDD prevention.
Second, the effectiveness data in our model are based on two meta-analyses conducted by Aburto et al. (31) and Harding et al. (32). In the absence of a study evaluating the effect of salt fortification on miscarriage, we used results reported in Harding et al. We could not find separate results for voluntary and mandatory prevention programs. However, salt was provided on a mandatory basis in most of the studies included in the two meta-analyses. Limitations (e.g., inclusion of studies with lower quality) of these meta-analyses can also influence the results of our analysis and under- or overestimate the effect of the IDD prevention program.
A recent study by Petersen et al. (41) published after our model calculations reported follow-up results from the DanThyr study, showing that mandatory iodine fortification may even reduce hyperthyroidism in a moderately iodine-deficient population. Therefore, the results of our study may underestimate the true effect of an IDD prevention program.
Third, most utilities derived from the literature were estimated using expert judgments or surveys among nurses or physicians, and there were no utilities available specifically for the German setting. In addition, results may differ when stakeholders are asked in different settings for their preferences (e.g., patients, healthy persons, or health care providers in different countries) or when different utility instruments are used (42). Only few quality-of-life studies are available evaluating the health utility values of thyroid disorders and IDDs. If future quality-of-life studies are conducted, the model should be updated with regard to these utility values.
We also used four short-term utility decrements: a utility decrement due to thyroidectomy, a utility decrement due to RAI therapy, a utility decrement due to temporary HRT, and a utility decrement due to stillbirth (also listed in Table 1). Since we could not estimate the exact duration of the quality-of-life loss, we applied these disutilities technically as one-time cumulative “tolls” in the time cycle of the occurring event.
However, utility values for the different diseases were reviewed and found to be plausible by clinical experts. When utility values were varied in sensitivity analyses, results for QALYs and life years remained stable, indicating robustness of our results. Furthermore, we presented both life years and QALYs enabling health policy decision makers and other stakeholders to compare the different prevention strategies based on life years, which do not depend on utilities.
Finally, our model only differentiates between IQ >70 and IQ <70. However, children may also have other cognitive deficits due to iodine deficiency in the mother. For example, Bath et al. (43) found differences in verbal IQ, reading accuracy, and reading comprehension in children born to mothers with different iodine status. These differences may have an impact on quality of life even if these children would have an IQ of >70. In this case, our model could under- or overestimate the true effect of an IDD prevention program.
Our population-based results suggest that IDD prevention yields an increase of expected QALYs and life years within a moderately iodine-deficient population. However, these results must be interpreted as an average benefit for the population. There are individuals not benefiting from the prevention or even being harmed by adverse events due to the iodine fortification of salt (e.g., by developing hyperthyroidism).
Therefore, ethical aspects, such as the autonomy of the individuals in the target population or the distribution of benefits and harms, should be considered before implementing a mandatory IDD prevention program. Besides QALYs and life years, we provided disaggregated results to inform an evidence-based discussion on ethical trade-offs between the health of individuals and the population.
Even if the effect of an IDD prevention program may be or may have been similar in other European countries with moderate iodine deficiency, the initial situation of each country may be different, for example, with regard to age distribution and prevalence of the different IDDs. However, our model is flexible and can be adapted to new data or other health care settings in the future.
More effectiveness studies would be needed to estimate the effect of salt iodization, especially in terms of the effect on the incidence of intellectual disability, stillbirth/miscarriage, hypothyroidism, and hyperthyroidism. In addition, quality-of-life studies in the field of IDDs are needed in European countries to make more suitable predictions. As a next step, costs of IDDs and IDD prevention should be included in the decision-analytic model to also evaluate the cost effectiveness of an IDD prevention program. This is an important step in terms of supporting decision-making, for example, by providing information about cost savings. Therefore, cost data collection, especially for the diagnosis and treatment of IDD and for IDD prevention programs, should be prioritized for future research in the field of IDD prevention.
Based on our evidence-based decision-analytic modeling study, IDD prevention via mandatory iodine fortification of salt increases quality-adjusted life expectancy in a population with moderate iodine deficiency, and is therefore beneficial on a population level. These results may be used to support the decision on implementing, continuing, or promoting an IDD prevention program in a European country and should be considered when developing public health guidelines for IDD prevention.
However, our study also suggests that IDD prevention may cause adverse health outcomes in a small fraction of the population such as increasing the risk of hyperthyroidism. Therefore, in addition to a favorable population benefit/harm balance, further ethical aspects, such as the autonomy of individuals, must be considered before implementing an IDD prevention program that is mandatory. Our decision-analytic model can also be used to evaluate the cost effectiveness of IDD prevention. Further studies on the effectiveness of IDD prevention programs and the quality of life of IDDs can help to even further consolidate our findings.
Footnotes
Acknowledgments
We thank Marija Mladenovic for assistance with literature searches and data extraction. We would also like to show our gratitude to the EUthyroid consortium for sharing their knowledge with us and for giving their feedback on the earlier versions of the decision-analytic model.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by EUthyroid. The project has received funding from the European Union's Horizon 2020 research and innovation programme under grant agreement number 634453. This work was, in part, financially supported through the Erasmus Mundus Western Balkans (ERAWEB), a project funded by the European Commission.
Supplementary Material
Supplementary Material A
Supplementary Material B
Supplementary Material C
Supplementary Material D