
Abstract
Background:
Hyperthyroidism is associated with bone mass reduction and increased fracture risk, but the effects on other important bone parameters have been sparsely examined. Therefore, we investigated bone microarchitecture and estimated bone strength by high-resolution peripheral quantitative computed tomography (HR-pQCT) in hyperthyroid patients at diagnosis and after being euthyroid for at least one year.
Methods:
Two approaches were used: (A) a case–control study comparing 61 hyperthyroid women with 61 euthyroid women matched for age and menopause status; (B) a follow-up study, in which 46 of the 61 women were re-examined after having been euthyroid for one year. HR-pQCT of the distal radius and tibia, and dual-energy X-ray absorptiometry (DXA) of the lumbar spine and the hip were performed.
Results:
In analysis A: In the radius, compared with the healthy controls, hyperthyroid patients had higher total area (16.9% ± 29.5%; p < 0.001), trabecular area (28.6% ± 45.7%; p < 0.001), and lower cortical area (−11.7% ± 23.2%; p < 0.001). Total volumetric bone mineral density (vBMD) (−13.9% ± 26.5%; p < 0.001), cortical vBMD (−5.8% ± 7.9%; p < 0.001), cortical thickness (−16.7% ± 26.0%; p < 0.001), and estimated bone strength (−6.6% ± 19.5%; p < 0.01) were lower. No significant differences were found in the tibia or in the DXA parameters. In analysis B: In the radius, significant improvements were observed in the cortical area (2.1% ± 4.6%; p < 0.01), cortical thickness (2.5% ± 5.1%; p < 0.001), and total vBMD (0.8% ± 3.0%; p < 0.05). Trabecular area decreased (−0.5% ± 1.0%; p < 0.01) and trabecular separation increased (2.0% ± 8.3%; p < 0.05). In the tibia, cortical area (3.6% ± 7.3%; p < 0.01) and cortical thickness (3.8% ± 7.6%; p < 0.01) increased, and trabecular area decreased (−0.5% ± 1.1%; p < 0.01). Areal BMD, measured by DXA, increased in the spine (1.1% ± 3.4%; p < 0.05) and in the hip (2.0% ± 3.8%; p < 0.01).
Conclusions:
Compared with the healthy control group, hyperthyroid women had lower vBMD, lower estimated bone strength, and compromised cortical microarchitecture in the radius. After restoration of euthyroidism, significant improvements in vBMD and cortical microarchitecture were observed, highlighting the importance of achieving and maintaining euthyroidism.
Introduction
Hyperthyroidism, caused by Graves' disease (GD) or toxic nodular goiter (TNG), is associated with a number of morbidities (1) and leads to excess mortality in a time-dependent manner, whether the hyperthyroidism is endogenous or exogenous (2 –4). Overt as well as mild hyperthyroidism is also a risk factor for osteoporosis (5,6) and bone fractures (7 –9). The mechanisms are complex and involve direct effects on the bones by thyrotropin (TSH), and the thyroid hormones thyroxine (T4) and triiodothyronine (T3). T3 binds to receptors in bone cells, inducing an accelerated bone turnover. Eventually, the imbalance between reduced bone formation and increased bone resorption (10,11) leads to a decrease in the bone mineral density (BMD). However, obtaining euthyroidism results in an improvement of BMD (12 –15) and decreases the fracture risk (16). Whether the impact on bone by mild hyperthyroidism reflects an effect of the decreased TSH per se or is due to high-normal levels of T3 and T4 remains unresolved (17,18).
Routinely, bone mass is measured as BMD using dual-energy X-ray absorptiometry (DXA). This method gives a reasonable, but not exact, estimate of the bone strength and the fracture risk in the individual patient. However, DXA yields no information on the bone microarchitecture, which in addition to bone mass is a determinant of bone strength. Earlier studies in hyperthyroid patients, based on bone biopsies, found a decreased trabecular bone volume and reduced cortical thickness due to increased osteoclastic activity and a decreased bone formation, with bone loss as the net result (19). However, bone biopsy is cumbersome and causes significant discomfort for the patient, making this unfeasible in daily clinical practice.
By the advent of high-resolution peripheral quantitative computed tomography (HR-pQCT), it has become possible to assess, three dimensionally and noninvasively, the bone microarchitecture and furthermore the method enables estimating the bone strength (20). HR-pQCT has been applied in nonthyroid disorders for exploring disease-specific bone pathophysiology and fragility (21), and the method can discriminate between individuals with and without bone fractures (22,23).
As no study has explored the impact of hyperthyroid diseases on bone by HR-pQCT and the effect of obtaining euthyroidism, our objectives were to examine bone microarchitecture and the estimated bone strength in hyperthyroid patients, as well as the effect of treatment of hyperthyroidism on pertinent bone variables, employing this method.
Materials and Methods
Study design and participants
This was a prospective study conducted at the Endocrine Outpatient Clinic, Odense University Hospital, Denmark, between May 2011 and January 2016. Women aged between 20 and 85 years with newly diagnosed overt or mild hyperthyroidism due to either GD or TNG were invited to participate. Patients were referred from their general practitioner or another department at the hospital. Exclusion criteria, for cases as well as controls, were: pregnancy or a wish to become pregnant during the study period; glucocorticoid treatment; decreased kidney function, as defined by a serum creatinine >100 μmol/L (reference interval 45–90 μmol/L) and/or eGFR <90 mL/min/1.73 m2; a diagnosis of osteoporosis, defined as either a history of a low-energy fracture or treatment with anti-osteoporotic agents; and other diseases (e.g., Cushing's syndrome, acromegaly) affecting bone metabolism.
Treatment with antithyroid drugs, thyroidectomy, or radioiodine was used for treatment according to the routine clinical care (24). To examine the effect of the treatment on the bone parameters, the participants were reexamined at least 12 months after euthyroidism was restored.
For the case–control comparison, each patient was matched by age, sex, and menopausal status with a healthy control subject randomly selected from the general population. The control subjects participated in a separate study examining age- and sex-related changes in bone microarchitecture in an adult population (25). Both patients and control subjects were recruited from the island of Funen, and the two studies were conducted simultaneously. Control individuals were examined once, using the same equipment and in a similar setup as used for the patients.
Body height was measured to the nearest 0.1 cm, and body weight was measured to the nearest 0.1 kg. The body mass index (BMI) was calculated as body weight divided by the square of the height (kg/m2).
The Regional Research Ethics Committee of Southern Denmark approved the study (S-2011-0018). Informed consent was obtained from each participant.
Study visits and biochemical tests
Overt hyperthyroidism was defined as subnormal or undetectable serum TSH, and T4 and/or T3 above the normal reference ranges, while mild hyperthyroidism was defined as subnormal or undetectable serum TSH and normal levels of serum T4 and T3. If the patients were positive for TSH receptor antibodies (TRAB >1 IU/L, measured using the TRAK human radioreceptor assay; Brahms Diagnostica, Germany), they were defined as having GD. If the patients were TRAB negative and had a nodular scintigraphy, they were defined as having TNG.
At the first study visit, HR-pQCT and DXA scans were performed, and fasting blood samples were drawn and stored at −20°C for later analysis. As part of the routine clinical care, thyroid function tests were performed every four to eight weeks. When a patient had been euthyroid for 12 months (defined by a normal serum TSH level), the second study visit, at which the bone scans and blood samples were repeated, was performed in a similar manner as at the initial measurements.
After study completion, stored samples from the two study visits were analyzed for TSH (normal reference level: 0.3–4.0 mIU/L), free triiodothyronine (fT3) (4.0–6.8 pmol/L), free thyroxine (fT4) (10.0–22.0 pmol/L), and vitamin D (25OHD; 50.0–160.0 nmol/L) by a two-site chemiluminescent immunometric assay on Cobas® 8000 (Roche Diagnostics). The coefficient of variation (CV) was 8.3% and 4.2% at TSH levels of 0.084 and 11.3 mIU/L, respectively; the CV was 2.1% and 2.0% at fT3 levels of 5.75 and 14.0 pmol/L, respectively; the CV was 7.1% and 4.4% at fT4 levels of 17 and 33 pmol/L, respectively; the CV was 5.1% and 5.7% at 25OHD levels of 53 and 106 nmol/L, respectively.
High-resolution peripheral quantitative computed tomography
HR-pQCT (XtremeCT; Scanco Medical, Brüttisellen, Switzerland) scans of the distal tibia and the nondominant distal radius were obtained at both study visits. The scan procedure and image evaluation have been described in detail previously (22). The scan region was initiated 9.5 and 22.5 mm from the radius and tibia endplate, respectively, and extended 9.02 mm proximally (22). Image analyses included total, cortical, and trabecular areas. Volumetric bone mineral density (vBMD) and trabecular microarchitecture parameters were extracted using standard software. These parameters included trabecular bone volume to total volume (BV/TV), trabecular thickness (
Dual energy X-ray absorptiometry
Areal BMD (aBMD) of the hip and the lumbar spine (L1–L4) was measured using DXA (Discovery; Hologic, Waltham, MA). The CV of the BMD measurements at our department is 1.5% in the spine as well as in the hip.
Statistical analyses
The distribution of the parameters was assessed using histograms and the Shapiro–Wilk test. The results are expressed as median and interquartile range or mean and standard deviation (SD), according to the distribution of the data. Student's t-test, the Wilcoxon signed rank, or the Wilcoxon rank sum test was used. Due to significant differences in body weight between patients and control subjects in the case–control study, a multiple linear regression was performed adjusting for weight. Assumptions for the linear regression models were checked using histogram and normal probability plots of residuals. If assumptions were not met, a Box–Cox regression analysis was performed, and the dependent parameter was transformed accordingly. Earlier studies have shown that the expected change in the bone parameter BV/TV as a result of treating hyperthyroidism is ∼10% (28,29). Our study was designed to detect such a difference with 80% power, with a significance level of 95%. To achieve this, at least 20 patients with hyperthyroidism (irrespective of its cause) had to complete the study.
To explore the effects of 25OHD status on bone microarchitecture, we reanalyzed our data for two subgroups, according to the 25OHD concentration being above or below the baseline median value, that is, 67.6 nmol/L in the case–control cohort and 62.3 nmol/L in the longitudinal. A multiple linear regression was performed adjusting for age. If the patient used 25OHD before inclusion, they could continue during follow-up, but change in intake of (start-up, dose change, or discontinuation) during the study period led to exclusion.
Differences were considered statistically significant in case of a two-sided p-value of ≤0.05. The statistical analyses were performed using StataIC version 15.0 (StataCorp LLC, TX).
Results
Basic characteristics
A total of 61 women were enrolled in the study. Ten patients were lost to follow-up, and an additionally five patients had an exclusion criterion. In all, 46 patients completed the follow-up study. We estimated the duration of the hyperthyroidism in each patient by using the date of the first blood sample with an abnormally low TSH measurement. The mean duration time from the first measured low TSH to the first bone scan was 15.9 months (range 1.0–92.5 months). The mean time span between the first and second study visits was 19 months (range 12.2–48.9 months). Table 1 shows the baseline characteristics of patients and controls. The mean body weight was 6.9 kg lower (SD: ±21.6 kg; p < 0.01) and the mean BMI was 4.8% lower (±29.4%; p = 0.01) in patients compared with the control subjects. Smoking habits did not differ between patients and control subjects.
Characteristics of Hyperthyroid Patients and Control Subjects at Study Visits
Data are shown as mean ± SD or median (interquartile range).
t-Test or Wilcoxon rank sum test: difference between all patients and controls.
Reference intervals: TSH: 0.3–4.0 mIU/L, fT3: 4.0–6.8 pmol/L, fT4: 10.0–22.0 pmol/L, vitamin D: 50.0–160.0 mol/L
The subgroups of overt and mild hyperthyroidism were defined based on the thyroid status at the first study visit, and not the thyroid status at the date of referral.
BMI, body mass index; SD, standard deviation; fT3, free triiodothyronine; fT4, free thyroxine; TSH, thyrotropin.
High-resolution peripheral quantitative computed tomography
Case–control study
HR-pQCT parameters of the case–control study are summarized in Table 2. In the radius, compared with the healthy controls, hyperthyroid patients had higher total area (16.9% ± 29.5%; p < 0.001), trabecular area (28.6% ± 45.7%; p < 0.001), and lower cortical area (−11.7% ± 23.2%; p < 0.001). Total vBMD (−13.9% ± 26.5%; p < 0.001), cortical vBMD (−5.8% ± 7.9%; p < 0.001), cortical thickness (−16.7% ± 26.0%; p < 0.001), and estimated bone strength (−6.6% ± 19.5%; p < 0.01) were lower. No significant differences were found in the tibia after adjusting for weight (Table 2).
Cross-sectional Control Study
HR-pQCT and DXA at baseline.
Data are shown as mean ± SD or median (interquartile range).
t-Test or Wilcoxon rank sum test.
BMD, bone mineral density; BV/TV, bone volume to total volume; DXA, dual-energy X-ray absorptiometry; HR-pQCT, high-resolution peripheral quantitative computed tomography.
Three patients were on estrogen replacement therapy (two postmenopausal women and one premenopausal woman) at the time of the first scan. Excluding these patients from the analysis did not change our findings (data not shown).
Follow-up study
The results of the follow-up study are shown in Figure 1. In the radius, an increase in cortical area (2.1% ± 4.6%; p < 0.01) and a decrease in trabecular area (−0.5% ± 1.0%; p < 0.01) were found. Furthermore, we found a significant increase in total vBMD (0.8% ± 3.0%; p < 0.05), cortical thickness (2.5% ± 5.1%; p < 0.01), and trabecular separation (2.0% ± 8.3%; p < 0.05) during the follow-up period. Estimated bone strength did not significantly change (1.1% ± 5.8%; p < 0.2). For the remaining parameters, we found no significant changes.
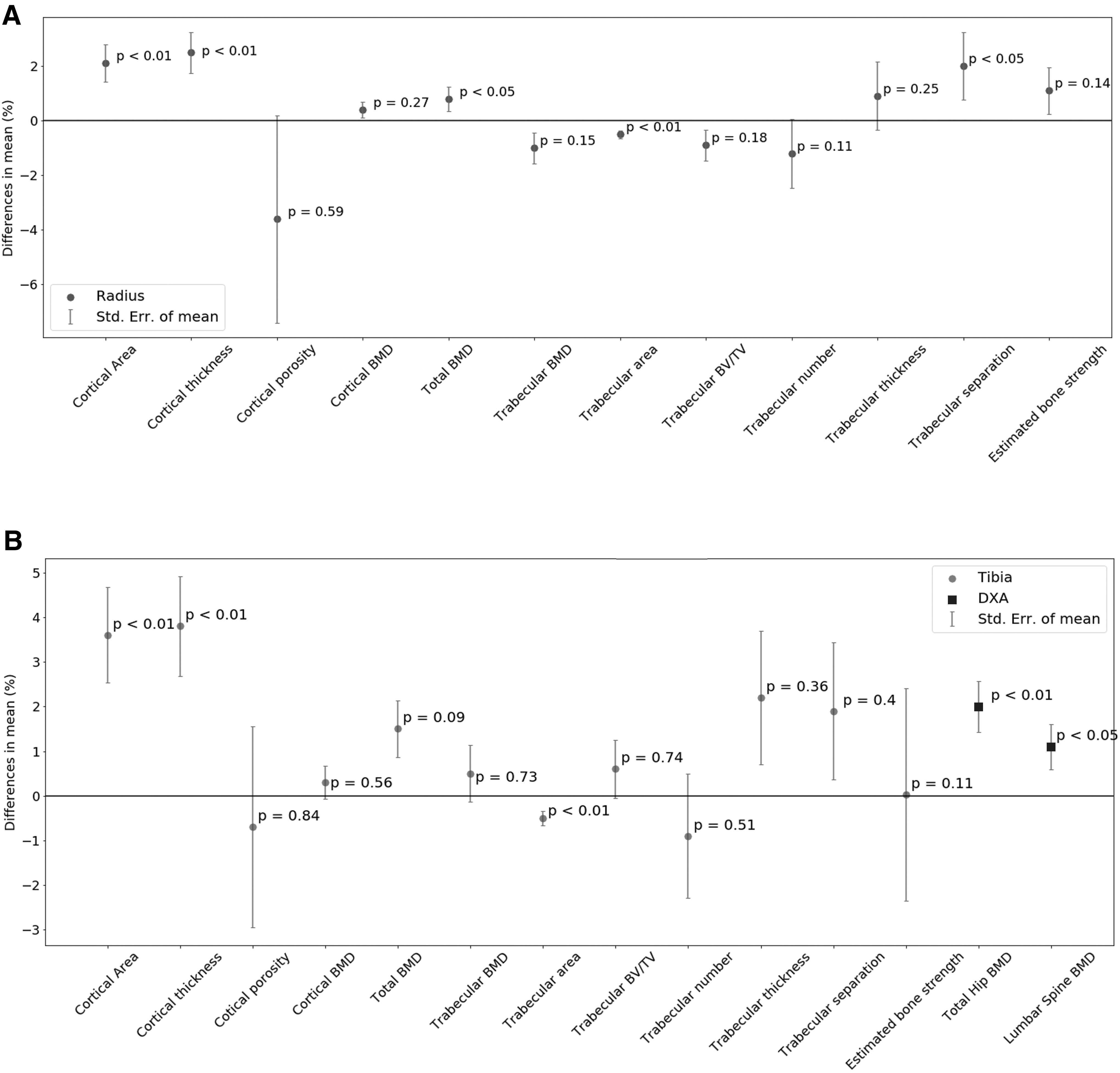
Effect on bone parameters following treatment of hyperthyroidism. (
In the tibia, significant changes were found for the cortical area (3.6% ± 7.3%; p < 0.01), trabecular area (−0.5% ± 1.1%; p < 0.01), and cortical thickness (3.8% ± 7.6%; p < 0.01). No significant changes were observed in estimated bone strength (0.03% ± 16.0%; p < 0.2). The remaining parameters were not significantly different (Fig. 1).
Dual-energy X-ray absorptiometry
Two patients were excluded from the hip BMD analysis, and one patient was excluded from the analysis of the lumbar spine BMD because of missing data at baseline. In the case–control study, no significant difference in aBMD was found, neither in the hip nor in the spine (Table 2). At follow-up, aBMD had increased significantly, both in the spine (1.1% ± 3.4%; p < 0.05) and in the hip (2.0% ± 3.8%; p < 0.01) (Fig. 1).
Influence of 25OHD status
Nineteen patients had a baseline 25OHD level of <50 nmol/L, two of whom had a level <25 nmol/L. In the case–control study, no significant differences were found between the low-level (<67.6 nmol/L) and the high-level (≥67.6 nmol/L) 25OHD group, neither for the HR-pQCT nor for the DXA parameters (data not shown). In contrast, the 25OHD level had significant impact on some variables in the follow-up study (Table 3). In general, the HR-pQCT parameters showed more positive dynamic changes (toward normalization) in the low-level group, compared with the high-level group, particularly in the radius. The 25OHD level changed to some degree during the study period in most patients, but correcting for this did not significantly alter the findings in the bone parameters.
Follow-up Study
HR-pQCT and DXA at follow-up, stratified into a high-level and a low-level vitamin-D group, according to the median value (i.e., 62.3 nmol/L).
Data are shown as mean ± SD or median (interquartile range).
t-Test or Wilcoxon rank sum test.
Impact of treatment initiated before the first study visit
Treatment of the hyperthyroidism was in some patients initiated before the first study visit. The median duration of this latency was 22 days. Nevertheless, some patients had partly normalized their thyroid function at the first bone scan. However, excluding these individuals (n = 11) did not change the overall results (data not shown).
Discussion
This is the first study, using HR-pQCT, to investigate the impact of hyperthyroidism as well as the effect of treatment on bone microarchitecture. Hyperthyroid women were found to have compromised cortical microarchitecture, lower vBMD, and lower estimated bone strength in the radius, compared with the healthy control subjects, while the tibia was not significantly affected. After one year of euthyroidism, significant improvements in vBMD and cortical microarchitecture were observed. These results seem to reflect an inappropriate bone remodeling in hyperthyroidism, inflicting an improper bone microarchitecture. Importantly, these bone alterations remained undetected by DXA, the method being used routinely for the diagnosis of osteoporosis. Our findings are consistent with earlier studies based on bone biopsies. Eriksen et al. (30) found higher resorption rates and a reduction in cortical thickness in hyperthyroid patients compared with control subjects, while Mosekilde and Melsen (31) found a lower trabecular bone volume, increased cortical porosity, and a markedly increased bone turnover. In hyperthyroid rats examined by bone biopsies, Hu et al. found lower BMD and compromised bone strength in both the trabecular and the cortical bone (32).
Effects of iatrogenic thyrotoxicosis on bone have been examined in patients with differentiated thyroid cancer treated, postoperatively, with TSH-suppressive doses of levothyroxine (33,34). In agreement with our findings, Tournis et al. (34) found lower cortical thickness in patients, compared with controls, in the radius but not in the tibia using pQCT, while there were no differences in trabecular bone mass or geometry. In contrast, no negative skeletal effects, as assessed by HR-pQCT, were observed in young adults treated with suppressive doses of levothyroxine for more than a decade (33).
It is well documented that BMD increases two to three years following treatment of hyperthyroidism when evaluated by DXA (12,14). Even in patients with mild hyperthyroidism, treatment is beneficial for BMD, as shown by Faber et al., while untreated patients are at risk for a decline in BMD (35). In the case–control study, we did not show any difference in BMD, evaluated by DXA between hyperthyroid cases and controls. One possible explanation could be that the effect of hyperthyroidism on bone is related to the length and severity of thyroid dysfunction. We cannot rule out that our patients may have had a shorter duration and/or milder biochemical features of hyperthyroidism compared with previous reports. However, studies in GD and in thyroid cancer patients on TSH-suppressive levothyroxine therapy demonstrated that negative skeletal effects may be observed despite unaffected standard DXA variables. Thus, it has been found that trabecular bone score at the lumbar spine was lower in patients with GD, and the prevalence of osteoporosis was higher when assessed by lumbar spine QCT compared with DXA (36,37). Based on these findings, it is evident that skeletal effects of hyperthyroidism may be undetectable using conventional DXA, while having subtle effects on cortical and trabecular bone at both peripheral and central skeletal sites.
Further details of the bone morphology following treatment are provided by HR-pQCT. In our study, cortical bone area and thickness increased significantly during follow-up, as did total vBMD and aBMD. The trabecular bone microarchitecture was not significantly altered apart from an increase in trabecular spacing in the radius. Although there were no significant alterations in trabecular number and of trabecular thickness, at this site, the trabecular number did numerically decline as did BV/TV, both of which infer an increase in trabecular separation. In other words, the observed increase in trabecular separation is most likely due to an inherent limitation related to the HR-pQCT technique, rather than a true effect of the treatment of hyperthyroidism.
The reason for this seemingly milder effect of hyperthyroidism in the tibia compared with the radius is unclear but may be related to the tibia being weight-bearing whereas the radius is not. Mechanical loading is crucial for maintaining skeletal health and weight-bearing activities particularly those involving impact loads are well known to enhance bone health. A pattern of relatively preserved bone morphology in the tibia compared with the radius has also been observed in other diseases such as primary hyperparathyroidism (21). Overall, the values of the bone parameters did not reach those found in the healthy control subjects matched for age and menopause status. In the euthyroid state, a bone remodeling cycle takes approximately six months to complete, which eventually alters bone mass and architecture. Therefore, a one-year euthyroid period is probably of too short duration to obtain complete normalization of the bone mass and microarchitecture, if at all possible.
Our patients had a larger trabecular area compared with the control subjects, but this difference diminished during the follow-up. A possible explanation for this finding is that the endocortical surface, harboring the transition zone between the trabecular and cortical bone, is more adaptive with a higher rate of bone remodeling, than the periosteal surface, as shown by Birkhold et al. (38). The faster bone remodeling in hyperthyroid patients leads to cortical thinning from the inside of the bone, enlarging the trabecular space. Restoration of euthyroidism seems to revert these changes.
Generally, body weight correlates positively with BMD, and it has been shown that obese individuals have higher vBMD compared with normal-weight individuals (39). In our study, body weight was significantly higher in the control subjects than in the patients, which may have affected the difference in bone parameters between the two groups. Since weight loss is an inherent consequence of hyperthyroidism, it can be questioned whether adjustment for body weight is justified in this context. In the weight-adjusted analyses, the results were overall very similar to those in the nonadjusted analyses, suggesting that the observed differences were indeed related to the hyperthyroid state rather than the weight difference.
25OHD deficiency significantly affects the bone structure and bone metabolism (40 –42). In our study, the patients with the lowest levels of 25OHD at baseline showed the greatest improvement in the bone microarchitecture following treatment. In addition to becoming euthyroid, some patients changed their 25OHD status during the study period. Correcting for this did not significantly affect our results, but our study was not powered to evaluate the impact of euthyroidism and change in the 25OHD level separately.
Our study has important strengths. DXA and HR-pQCT were performed simultaneously both before and after treatment. HR-pQCT provides a greater and more in-depth knowledge of the bone structure and strength than is possible by DXA. Indices obtained by HR-pQCT have been shown to improve prediction of bone fracture beyond what can be achieved by aBMD or the Fracture Risk Assessment Tool (FRAX) (43,44). Moreover, our study was performed in a clinical setting, comprising women of a broad age range suffering from a variation in severity and duration of hyperthyroidism as well as having the common causes of hyperthyroid.
Some limitations to our study exist. First, although we matched patients and control subjects for age and menopause status, the study remains prone to selection bias. Second, the sample size calculation was performed according to the follow-up study and therefore not directly applicable to the case–control study. Third, due to limited power, we did not stratify analyses for the cause of hyperthyroidism (GD or TNG), the severity or duration of hyperthyroidism. Fourth, some patients initiated treatment before the first study visit. However, excluding those patients who had accomplished a near-normal thyroid function at this point did not significantly change our findings. This is consistent with the fact that the bone remodeling cycle is of long duration, and we believe that it is unlikely that the bone structure should have changed significantly in the short time frame from treatment initiation (median 22 days) until performance of the bone scans. Finally, we tried to estimate the duration of the hyperthyroid state, but the exact duration was unknown in many of our patients due to the insidious onset of the disease or lack of symptoms. Therefore, we are not able to assess the effect of the disease duration, which has been shown to affect risk of major bone fractures (7,9) and therefore most likely also has impact on bone microarchitecture.
In conclusion, we show that hyperthyroidism has negative impact on bone microarchitecture, primarily in the radius, but with improvement following treatment. Whether HR-pQCT parameters have any predictive value in relation to the fracture risk in hyperthyroid patients remains to be elucidated in larger scale and longer term follow-up studies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study received funding from The Music Publishers Agnes and Knut Mørk's Foundation, the Danish Thyroid Foundation, the William Demant Foundation, and from Odense University Hospital.