
Abstract
Background:
The incidence of thyroid cancer has increased worldwide. We investigated nationwide trends in the incidence and treatment course of pediatric thyroid cancer in South Korea.
Methods:
Using the National Health Information Database, we analyzed 1580 patients (324 males) <20 years of age diagnosed with thyroid cancer during 2004–2016 in South Korea. The annual percentage change (APC) in the age-standardized incidence rate (ASR) was calculated by joinpoint regression analysis. The initial treatment modality was categorized as either surgery only or surgery with radioactive-iodine treatment (surgery+RAIT), and we defined new treatment events as reoperations or additional RAITs among 1464 patients followed up for ≥12 months.
Results:
During 2004–2016, the mean ASR per 100,000 person-years increased from 0.6 [confidence interval; CI 0.5–0.8] to 0.9 [CI 0.8–1.1], with a mean APC of 4.0% [CI 1.8–6.2]. The ASRs (APCs) among 0–9-, 10–14-, 15–17-, and 18–19-year olds were 0.07 (9.9% [CI 0.08–20.7]), 0.6 (4.6% [CI 0.2–9.2]), 2.2 (3.9 [CI 1.7–6.0]), and 4.2 (3.5% [CI 0.9–6.2]), respectively. The lobectomy and lymph-node-dissection rates increased (from 18.5% to 33.6%, p = 0.0014; and from 29.6% to 84.5%, p < 0.001; respectively), but the RAIT rate decreased (67.9–39.7%, p < 0.001) during the study period. During a median 6.3-year follow-up, two patients died. New treatment events occurred in 56 (10.7%) of patients in the initial surgery-only group (n = 523). In the initial surgery+RAIT group (n = 941), 316 patients received two or more RAITs within 2 years, and 80 (12.8%) of the remaining 625 patients underwent new treatment events. In the surgery+RAIT subgroup, the event-free survival rate was lower in 0–14-year olds than in 18–19-year olds (hazard ratio 2.5 [CI 1.4–4.4]).
Conclusions:
The pediatric thyroid cancer incidence increased from 2004 to 2012 in South Korea. The lobectomy and lymph-node-dissection rates increased, but the RAIT rate decreased. The higher risk for new treatment events in patients younger than 15 years requiring initial RAIT may be linked to advanced stage at diagnosis, and it needs to be further evaluated.
Introduction
The incidence of pediatric thyroid cancer depends on age, sex, and country. In Europe during 1988–1997, the age-standardized incidence rates (ASRs) per 100,000 individuals were 0.17–0.18 among children aged <15 years (1) and 0.83 among those aged 15–19 years (2). In the United States, the ASR per 100,000 individuals was 0.6 during 1976–2013 among patients younger than 20 years of age, and the annual percentage change (APC) significantly increased from 1.1% during 1973–2006 to 9.6% during 2006–2013 (3). An increasing incidence of pediatric thyroid cancer has been demonstrated worldwide (4 –8).
South Korea has the highest incidence of thyroid cancer worldwide (7). The Korea National Cancer Incidence Database (9) recorded a 22.6% increase in the ASR for thyroid cancer during the 1999–2011 period. The crude incidence rate (CR) and ASR per 100,000 individuals were 0.24 and 0.2 (0.08 for males and 0.33 for females), respectively, among 0–14-year olds during 1993–2011 (10), and the CRs per 100,000 individuals were 0.85 for males and 4.44 for females among 15–19-year olds during 1999–2010 (11), indicating an increase in the pediatric thyroid cancer incidence. However, neither ASR data by pediatric age group nor the APC in incidence in South Korea has been reported.
Screening contributed to the increased incidence of adulthood thyroid cancer, which may increase the presymptomatic screening of offspring. However, health screenings had little effect, if any, on the increased incidence of pediatric thyroid cancer in Korea (11), and thyroid cancer tended to be more advanced at diagnosis in children than in adults (12). Pediatric thyroid cancer has higher rates of recurrence and persistent disease, but a lower rate of mortality than adult thyroid cancer (12). Therefore, age-optimized management and guidelines are needed. A population-based nationwide study would enable identification of the treatment course and outcome according to age. We investigated the trends in incidence and initial treatment in pediatric patients with thyroid cancer during 2004–2016 in South Korea using the National Health Information Database (NHID) of the National Health Insurance Service (NHIS). We also analyzed the postoperative complications, treatment course, and outcomes of patients followed up for 12 months or longer.
Materials and Methods
Study population
We used NHID data from the Ministry for Health, Welfare, and Family Affairs, which cover the entire Korean population (13). All hospitals in South Korea submit their outpatient and inpatient data on diagnosis and treatment costs to the NHIS to claim for patient care. The Korean Health Insurance Review and Assessment Service construct the database as an accurate claim review and quality assessment system for the NHIS. The NHIS National Sample Cohort project was approved by the Institutional Review Board (IRB) of the NHIS. This study was approved by the IRB of Korea University Medical Center, Seoul, South Korea (IRN No. KU-IRB-17-EX-253-A-1).
According to the International Classification of Diseases (ICD), 10th edition, thyroid cancer is coded as C73. The NHID identified 1580 patients (324 males, 1256 females) <20 years of age who underwent thyroidectomy between January 2004 and December 2016.
The NHID does not include pathologic findings or metastatic status. Initial treatment modality was defined as follows. Extent of surgery was classified as total thyroidectomy (TT; P4552 or P4561), subtotal thyroidectomy (ST; P4554), and lobectomy (L; P4551 or P4553). TT included completion surgery within six months of the initial L or ST. Information on cervical (unilateral or bilateral) and/or mediastinal lymph node dissection (LND) was also obtained (codes P2102–2103, P2112–2119, and O1596). Initial LND included simultaneous LND with thyroidectomy at diagnosis and subsequent LND within six months after the first surgery. For radioactive-iodine therapy (RAIT), the timing and 131 I dose were identified. Initial RAIT was defined as the first RAIT within 12 months after diagnosis.
Definitions of clinical courses
Among the 1580 subjects, we evaluated the treatment outcomes in 1464 patients followed up for 12 months or longer (median 6.3 years, range 1.0–12.9 years). Because we could not evaluate persistent or recurrent disease using the NHID, we categorized the subjects into the more- and less-treatment groups to estimate outcomes. The more-treatment group included those who required two or more RAITs or those who developed a new treatment event. We defined a new treatment event as “reoperation after 6 months of initial treatment” and/or “additional RAIT after 12 months of initial treatment.” The less-treatment group included those who did not need additional treatment after completing the initial treatment.
Statistical analyses
Continuous variables are summarized as means ± standard deviations or medians (interquartile range), and categorical variables as numbers (%). Comparisons of continuous variables and categorical variables between the two groups were performed using Student's t-test and chi-squared test or Fisher's exact test, respectively. Comparisons of three or more groups were conducted by the chi-squared test for linear trend or logistic regression analysis.
The ASR was estimated using the National Cancer Institute's SEER*Stat software package (ver. 8.3.6; National Cancer Institute, Bethesda, MD) using the World Health Organization (WHO) standard population (14), and is expressed per 100,000 person-years. The APC of the ASR and its confidence interval [CI] were estimated using the joinpoint regression analysis program (ver. 4.7.0.0; National Cancer Institute). Student's t-test was used to examine the difference in APC from zero. The best-fitted log-linear regression model was used to identify calendar years (i.e., joinpoints) with a significant change in APCs (3). A multivariate logistic regression model was used to identify predictors of postoperative calcium (Ca) and/or vitamin D (VitD) medications. The event-free cumulative incidence and its CI were calculated using the Kaplan–Meier method, and we performed univariable Cox's proportional hazard regression analyses to compare variables between groups. We only had a few missing values in age groups (n = 6) and LND variables (n = 2), and we did not perform missing value imputations for missing observations. All statistical analyses, except for ASR and APC evaluation, were performed using SAS software ver. 9.4 (SAS Institute, Inc., Cary, NC). All presented p-values are two-tailed, and we considered all p-values <0.05 as statistically significant.
Results
Trends in incidence
The ASR per 100,000 person-years during 2004–2016 was 0.92. Table 1 shows the numbers of cases, ASRs, and APCs. Females and 15–19-year olds accounted for the majority of the cases. Overall, the ASR increased from 0.6 [CI 0.5–0.8] in 2004 to 0.9 [CI 0.8–1.1] in 2016, with a mean APC of 4.0% [CI 1.8–6.2]. The ASR increased significantly from 2004 to 2012 (APC, 7.7% [CI 5.1–10.3] and remained unchanged from 2012 to 2016 (APC, −4.7% [CI −10.7–1.6]; Table 1 and Fig. 1A). In females, the ASR per 100,000 person-years significantly increased from 1.1 in 2004 to 2.0 in 2014 with a mean APC of 5.2%, and then nonsignificantly decreased. In males, the ASR consistently increased from 0.2 in 2004 to 0.6 in 2016 with a mean APC of 7.6% (Table 1 and Fig. 1B).
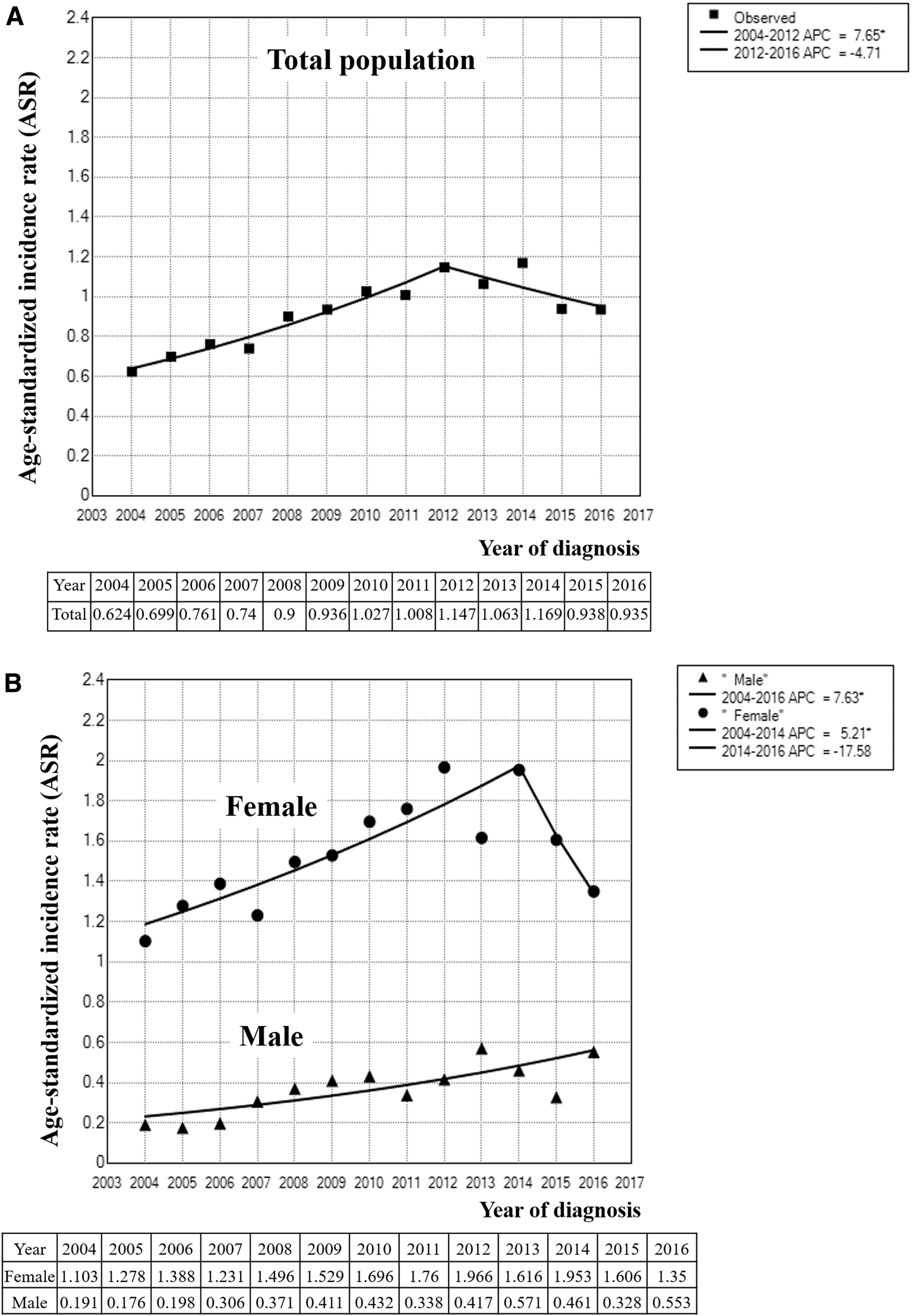
Trends in age-standardized incidence of pediatric thyroid cancer during 2004–2016 among (
Number of Cases, Age-Standardized Incidence Rates, and Annual Percentage Changes of Pediatric Thyroid Cancer by Sex and Age Group During 2004–2016
ASR is expressed as cases per 100,000 person-years; APC is expressed as the percentage per year according to the result of a joinpoint regression analysis.
APC, annual percentage change; ASR, age-standardized incidence rate; CI, confidence interval.
When analyzed by age group, the ASRs (APCs) among 0–9-, 10–14-, 15–17-, and 18–19-year olds were 0.07 (9.9%), 0.06 (4.6%), 2.2 (3.9%), and 4.2 (3.5%), respectively. The ASR increased with age, and the APC increased from 2004 to 2016 in all age groups except 15–17-year olds (Table 1).
Trends in initial treatment modality, 2004–2016
Among 1580 patients, 289 (18.3%) and 33 (2.1%) underwent L and ST, respectively, 1024 (64.8%) received LND, and 987 (62.5%) received RAIT as the initial treatment (Fig. 2 and Supplementary Table S1). The mean age at surgery was 16.5 ± 2.8 years, and the median follow-up duration was 5.7 (0.03–13.0) years. The L, LND, and RAIT rates significantly changed during 2004–2016 as follows: that of Ls increased from 18.5% to 33.6% (p for trend = 0.014; Fig. 2A), that of LNDs increased from 29.6% to 84.5% (p for trend <0.0001; Fig. 2B), and that of RAIT decreased from 67.9% to 39.7% (p for trend <0.0001; Fig. 2C).

Trends in initial treatment modality during 2004–2016 for (
Postoperative medications
Among 1464 patients followed up for ≥12 months, 1014 (69.3%) received Ca and/or VitD medications after surgery (postoperative Ca/VitD [yes]), and 542 (37.0%) of them continued the medication for more than 1 year (postoperative Ca/VitD [≥1 year]), shown in Supplementary Table S2. The rate of Ca/VitD medications prescribed immediately after surgery was higher among females (OR 1.5), but no difference in age group was found. The extent of surgery (OR 1.4 for L with LND, OR 1.9 for ST/TT, and OR 3.0 for ST/TT with LND vs. L only) and RAIT (OR 3.0) were significant predictors for postoperative medications (Ca/VitD [yes]). These findings were similar in patients who continued to receive Ca/VitD for ≥1 year after surgery (OR 1.4, 3.6, and 7.3 for extent of surgery, respectively, and 5.0 for RAIT). When we compared patients who received postoperative Ca/VitD for ≥1 year with those who received them for <1 year, no significant differences were found (Supplementary Tables S2 and S3).
Among the 245 patients who underwent initial L or ST (± LND) without a new treatment event, 45 had taken levothyroxine before surgery. After excluding these patients, 157 (78.5% of 200) received levothyroxine postoperatively, and 134 (67%) continued to receive it for more than 1 year.
Follow-up treatment course after initial treatment
Among the 1580 patients, we evaluated 1464 who were followed up for 12 months or longer (median 6.3 years, range 1.0–13.0 years). The initial treatment modality was categorized as (1) surgery only (L, ST, or TT with or without LND, n = 523) or (2) surgery with initial RAIT (surgery+RAIT, n = 941), as shown in Figure 3. The total number of deaths was two, one of which was due to thyroid cancer. When we compared the baseline characteristics between the surgery-only (n = 523) and surgery+RAIT (n = 941) groups, no significant difference in sex or age group was found. As expected, the surgery+RAIT group received more extensive thyroidectomy (p < 0.001 for L, ST, L/ST+completion, to TT) and LND (p < 0.001 for none, unilateral, to bilateral LND), leading to more extensive surgery (p < 0.001 for L, L + LND, ST/TT, to ST/TT+LND), compared with the surgery-only group (Supplementary Table S4).
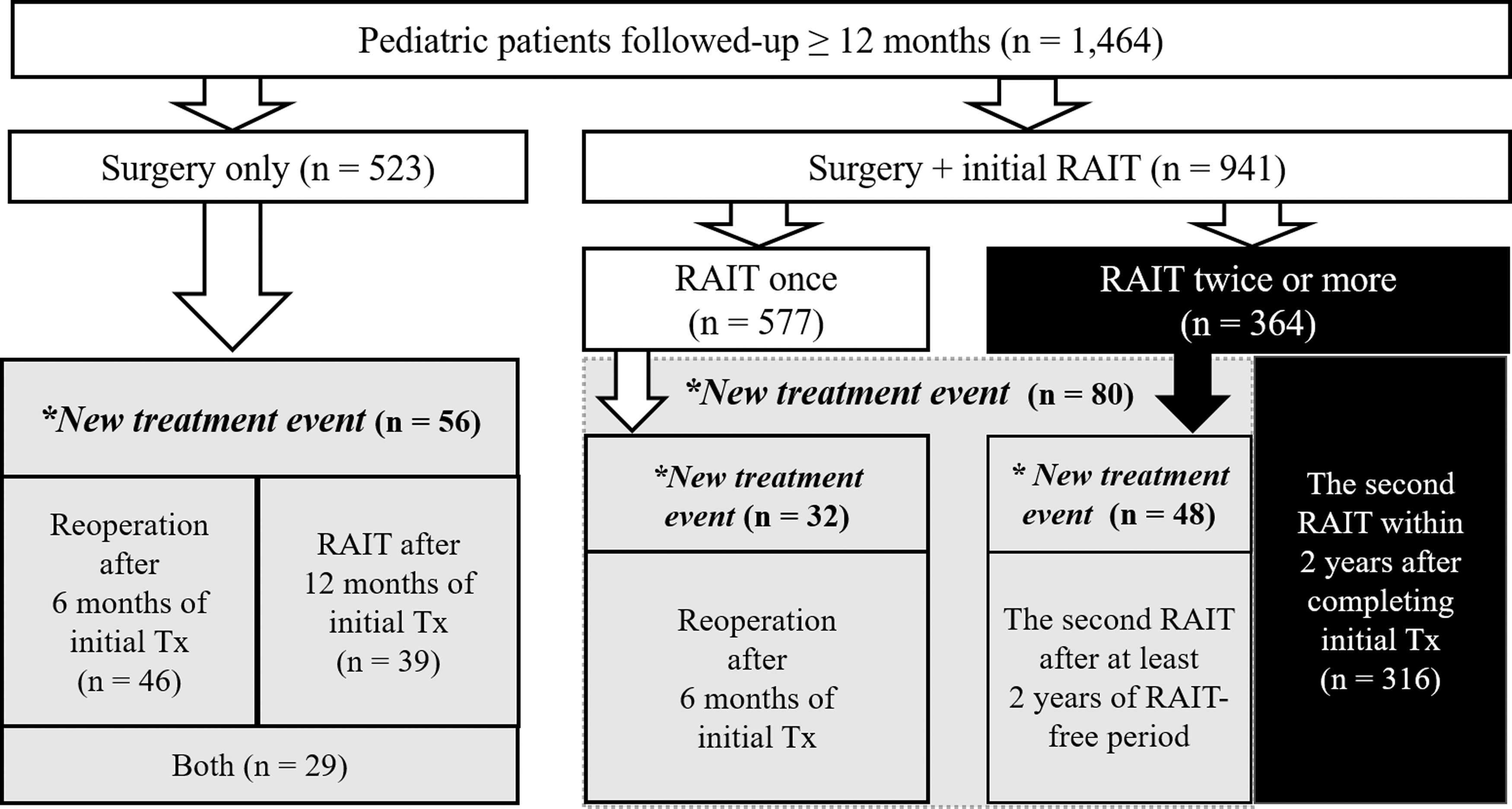
Treatment course of patients followed up for more than 12 months. A new treatment event was defined as “reoperation after 6 months of initial treatment” and/or “additional RAIT after 12 months of initial treatment.”
Among the patients in the surgery-only group (5.7 years of follow-up, range 1.0–12.9 years), 56 (10.7%) were categorized into the more-treatment group (Fig. 3); they had undergone less extensive surgery at diagnosis (p for trend = 0.026) than the patients in the less-treatment group, without difference in sex or age between the two groups (Supplementary Fig. S1A). Among the patients in the surgery+RAIT group (6.2 years of follow-up, range 1.0–13.0 years), 396 (42.1%) were classified into the more-treatment group (Fig. 3); they had a higher proportion of male sex (54.1% vs. 39.0%, p = 0.0003) and were younger (63.1% of 0–14-year olds, 39.5% of 15–17-year olds, and 35.2% of 18–19-year olds in the more-treatment group, p < 0.001) than the less-treatment group, although the extent of surgery did not differ between the two groups (Supplementary Fig. S1B).
A new treatment event occurred in 10.7% (n = 56, 17 reoperation only, 10 RAIT only, and 29 reoperation with RAIT) in the surgery-only group, and 12.8% (n = 80, 32 reoperation and 48 additional RAIT) in the surgery+RAIT group (Fig. 3). To compare new treatment event-free survival between the surgery-only and surgery+RAIT groups, 316 patients who received a second RAIT within 2 years were excluded. The surgery+RAIT group (n = 625) received more extensive surgery at diagnosis (p < 0.001 for extent of surgery, thyroidectomy, and LND) compared with the surgery-only group (n = 523; Supplementary Table S4). The event-free survival rate of the surgery+RAIT group was not different from that of the surgery-only group (Fig. 4A). In the surgery-only group, we found similar event-free survival rates among patients of different age, sex, and extent of surgery subgroups (Fig. 4B–D). However, in the surgery+RAIT group, the event-free survival rate was lower in 0–14-year olds than in 18–19-year olds (hazard ratio 2.5 [CI 1.4–4.4]) (Fig. 4E), but sex and extent of surgery were not (Fig. 4F, G).
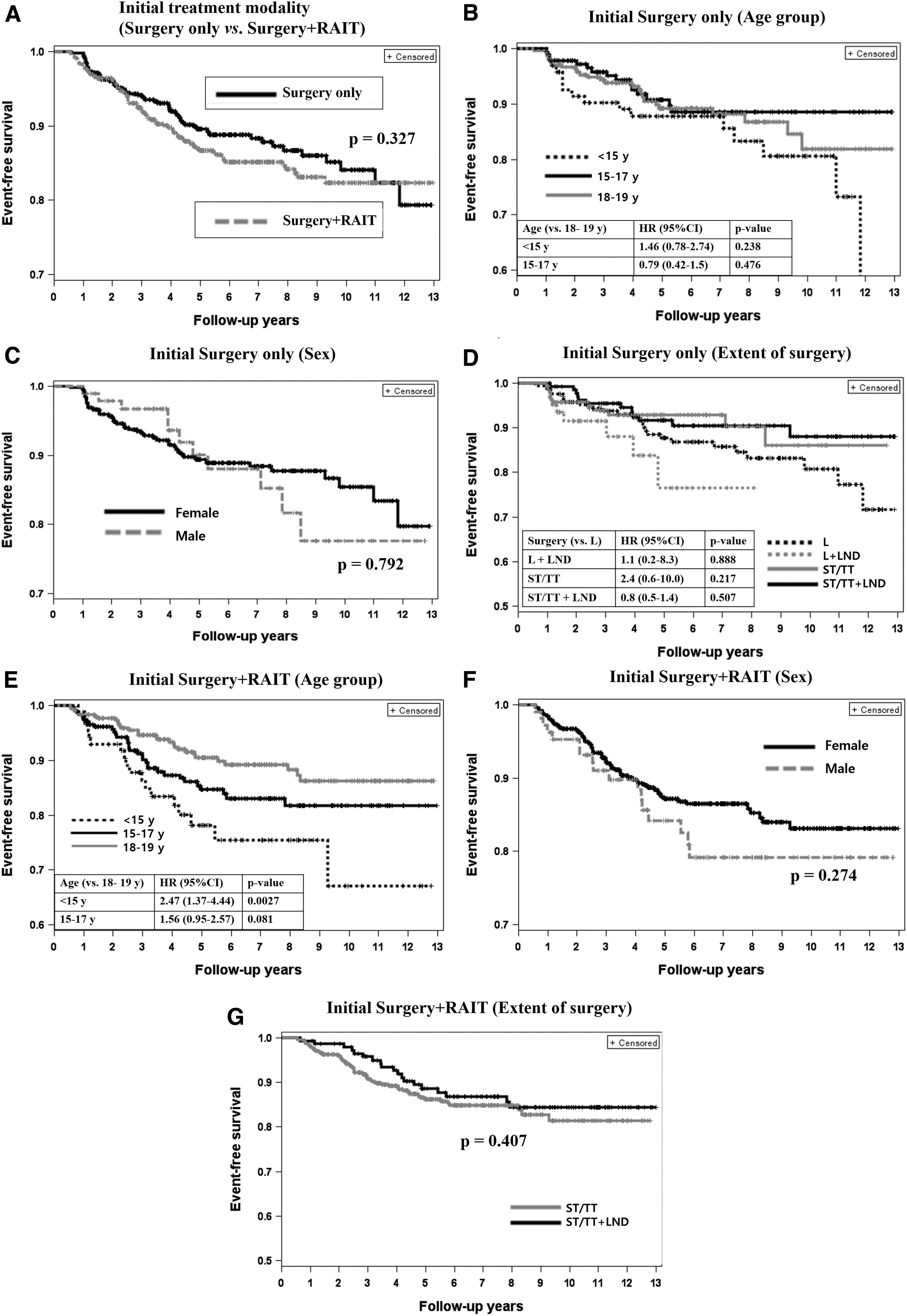
Event-free survival curves. (
Discussion
The ASR of pediatric thyroid cancer was 0.92 per 100,000 person-years during 2004–2016 with an APC of 4.0% in South Korea, and significantly increased during 2004–2012, with an APC of 7.7%, and nonsignificantly decreased thereafter. For the initial treatment, more than two-thirds of the patients received TT with an increasing trend of LND and decreasing trend of RAIT during that period. Among the patients followed up for ≥12 months, 69.3% were on postoperative Ca/VitD medications and 37.0% were still using the medications at 1 year after the surgery, and the risk factors for postoperative Ca/VitD medications were female sex, extensive surgery, and RAIT. New treatment events occurred in 10.7% of the surgery-only group and 12.8% of the surgery+RAIT group. When we compared new treatment events such as reoperation or additional RAIT, the event-free survival rates were lower in 0–14-year olds than in 18–19-year olds.
The incidence of pediatric thyroid cancer varied by age, sex, and race/ethnicity. Although pediatric data on ASRs are sparse, pediatric thyroid cancer incidence seems to be higher in South Korea than elsewhere (7,15 –18) and differs slightly among countries compared with adults (7). The ASR per 100,000 person-years in South Korea during 2004–2012 was 0.873, while it was 0.68 during 2001–2009 (18), 0.67 during 1983–2013 (16), and 0.60 during 1973–2013 (3) in the United States. The incidence in South Korea significantly increased, with an APC of 7.6% during 2004–2012. The incidence in the United States gradually increased during 1973–2006, with an APC of 1.11%, and markedly increased during 2006–2013 with an APC of 9.56% (3). In Denmark during 1980–2014, the ASR per 100,000 persons increased from 0.36 to 0.97, with a 2.9% APC; this increase was also evident among 18–24-year olds, but not among 0–17-year olds (7). In the United Kingdom, the ASR per million was 0.33 during 1976–2005, with a significantly increasing trend, although no APC data were reported (8). In this study, the incidence nonsignificantly decreased after 2012, likely due to female cases and 15–17-year olds (Table 1).
The increasing trend in ASR was significant for both sexes, although more pronounced in males. The mean ASR increased in all pediatric age groups. The mean ASR was highest in 0–9-year olds (9.9% [CI 0.08–20]) with an APC of 3.5–4.6%, but comparison across different age groups was not possible due to the wide CIs. Increasing trends in incidence among 10–19-year olds have been reported in the United States, although the change in the ASR of 0–9-year olds could not be calculated due to the small number of patients (3,17). A recent U.S. study reported no significantly increased incidence in 0–9-year olds (16).
A combination of enhanced diagnosis and a true increase may explain this increasing trend, although the effect of screening may be smaller in children than in adults. When considering thyroid cancer risk in survivors of the Chernobyl accident (19) and the atomic bomb (20), and potentially in individuals exposed to medical radiation, in particular, computed tomography (CT) (21,22), the key environmental factor is ionizing radiation. Although the contribution of CT radiation to this increase is unclear, the frequency of overall, facial bone, and neck CT use in emergency departments in South Korean pediatric patients increased during 2001–2010 (23,24). Also, excess adiposity and obesity may be linked to thyroid cancer through estrogen-related and insulin-resistance mechanisms (25). Considering the growth-promoting effect of estrogen on thyroid cells (26), the increasing incidence of childhood obesity (27) and precocious puberty (7) might be some causes in South Korea. In addition, exposure to endocrine-disrupting chemicals (e.g., bisphenol A, pesticides, and polybrominated diphenyl ethers [PBDE]) may increase the risk of thyroid cancer (28). For example, PBDEs were detected in all floor-dust samples from South Korean elementary schools (29), and exposure to flame retardants was associated with the occurrence and severity of papillary thyroid cancer (30).
The incidence of postoperative hypoparathyroidism ranges from 13.6% to 34.1% for transient hypoparathyroidism, and from 1.5% to 23.8% for permanent hypoparathyroidism (15). To evaluate the frequency of postoperative hypoparathyroidism, information on postoperative serum Ca and parathyroid hormone levels, preexisting hypoparathyroidism, and previous prescriptions of active VitD is needed. However, we could not strictly define hypoparathyroidism, because the NHID does not include laboratory data or Ca and VitD dosages. Instead, we investigated the frequency of postoperative Ca/VitD medications, and found that a large proportion of patients, more than one-third at one year after surgery, had taken such medications. This frequency cannot tell us about the precise incidence of postoperative hypoparathyroidism and was higher than that of prior reports (15,31). However, considering our findings that more extensive surgery and initial RAIT were associated with a higher rate for postoperative Ca/VitD medications, we can suggest the importance of careful consideration of the risks and benefits of the extent of surgery or adjuvant RAIT.
Among a total of 1464 patients, the more-treatment group accounted for 30.9% (n = 452); 10.7% in the surgery-only group and 42.1% in the surgery+RAIT group. Among them, 316 (21.6% of total) underwent a second RAIT within 2 years after the initial RAIT, and 136 (9.3%) experienced a new treatment event. Among 136 patients, 88 (6.0%) had a reoperation (Fig. 3). Although we could not identify recurrent or persistent disease status using the NHID data, this result is similar to that in our previous study (5-year recurrence rates of 15.5% during 2000–2009) (12) and other pediatric series (16.2–21.6% rate of recurrent or persistent disease) (32,33), but higher than the 5.8% rate reported in Korean adult patients during 1999–2009 (34). Patients younger than 15 years had a higher rate of receiving more treatment and of developing new treatment events than those between 18 and 19 years, possibly due to advanced disease in the younger group (12). Although we could not determine the stage at diagnosis or disease outcome using the NHID, younger patients are more likely to present with advanced disease at diagnosis (12,35,36). This study, which had only two cases of mortality, indicates that pediatric patients have a relatively low mortality rate. The risk of mortality due to thyroid cancer in children is exceedingly low (3).
This study has several limitations because we used information provided by the NHID. There was no information on histologic findings, reasons for diagnosis, history of exposure, or disease status during follow-up, and so, we assessed disease status using surrogate definitions, and could not evaluate the effects of histologic or demographic data. Because some histological variables, such as the histologic subtype or lymph node involvement, are prognostic factors, multivariate analysis is needed to evaluate the associations of age with the risk of receiving more treatment or recurrence after adjusting for disease severity at diagnosis. In addition, we could not investigate the proportion of patients with a prior malignancy and/or history of therapeutic radiation therapy, since the NHID only provides patient data on disease diagnosis and treatment during 2004–2016, but not before 2004. Nevertheless, the NHID includes information on all populations; therefore, this was the first population-based nationwide study on the secular trends in the ASR of pediatric thyroid cancer in South Korea.
In conclusion, the incidence of pediatric thyroid cancer increased during 2004–2012. The L and LND rates increased, but the RAIT rate decreased. The mortality rate was low. The finding that patients younger than 15 years with tumor(s) requiring initial RAIT had a higher risk for developing new treatment events may be linked to advanced stage at diagnosis, and it needs to be further investigated.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (Grant No. HI17C1926).
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4