
Abstract
Background:
Management of patients with advanced medullary thyroid cancer (MTC) remains a therapeutic challenge. The multi-tyrosine kinase inhibitors (TKIs) vandetanib and cabozantinib have been approved for the treatment of progressive MTC based on prolonged progression-free survival (PFS) in phase 3 clinical trials.
Patients and Methods:
To evaluate clinical characteristics, treatment regimens, efficacy, and treatment emergent adverse events (TEAEs) of vandetanib and cabozantinib in MTC patients outside clinical trials at four German tertiary care centers. Forty-eight patients diagnosed between 1990 and 2018 were included. PFS and overall survival (OS) probabilities were estimated using the Kaplan–Meier method and compared by log-rank test.
Results:
The median age at diagnosis was 46 years (15–80 years); a germ line RET (rearranged during transfection) mutation was known in 6 (13%) patients. Thirty-two (67%) patients showed progressive disease before TKI initiation. Forty-seven (98%) patients were treated with vandetanib and 23 (48%) patients with cabozantinib. Vandetanib was first-line treatment in 41 (85%) patients and cabozantinib in 7 (15%) patients. Partial response was the best response in 12 (26%) patients treated with vandetanib and in 5 (22%) patients treated with cabozantinib. Sixteen (34%) patients treated with vandetanib and 3 (13%) patients treated with cabozantinib had stable disease ≥24 weeks. The median PFS for vandetanib and cabozantinib was 17 months [95% confidence interval, CI, 9.3–24.6 months] and 4 months [CI 3.1–4.9 months], respectively. The 6- and 12-month survival rates were 98% and 86% for vandetanib and 78% and 70% for cabozantinib, respectively. The median OS for vandetanib and cabozantinib was 53 months [CI 43.7–62.3 months] and 24 months [CI 5.9–42.1 months], respectively. In vandetanib-treated patients, the PFS and OS were significantly longer in patients aged ≤60 years at TKI initiation and in patients with ≥5 TEAEs. Additionally, the PFS was longer in the absence of bone metastases. In cabozantinib-treated patients, the PFS was significantly longer in patients experiencing TEAEs and in patients aged ≤60 years, and the OS was significantly longer in patients who had TEAEs and in patients with ≥5 TEAEs.
Conclusions:
Vandetanib and cabozantinib are effective treatment options in the majority of MTC patients. We hypothesize that the poorer prognosis of cabozantinib-treated patients in our retrospective analysis is most likely due to its use as second-line treatment after treatment failure on vandetanib. However, different degrees of efficacy of the two drugs are possible.
Introduction
Medullary thyroid cancer (MTC) arises from calcitonin-producing parafollicular C cells of the thyroid gland and accounts for 2–5% of all thyroid malignancies (1). In about 25% of cases, MTC is inherited as part of multiple endocrine neoplasia type 2 (MEN2), which is caused by oncogenic germ line rearranged during transfection (RET) mutations. Up to 65% of patients with sporadic disease have somatic RET mutations, among which RETM918T is the most common and associated with adverse outcome (2 –5). At diagnosis, cervical lymph node metastases are present in about half of patients and distant metastases in around 10% of MTC patients (6). While localized disease has a 10-year disease-specific survival (DSS) of 96%, 10-year DSS is only 44% in patients with distant metastases (7,8).
Surgery remains the only curative therapy in localized disease. Patients with evidence of locally advanced disease not amenable to surgical intervention or distant metastases may require systemic treatment. While radiation therapy and cytotoxic chemotherapy offer limited benefit (5,9), multi-tyrosine kinase inhibitors (TKIs) vandetanib and cabozantinib have been approved by the United States Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for patients with significant tumor burden, symptomatic and/or progressive metastatic disease (9).
Vandetanib inhibits tyrosine kinases RET (50% inhibitory concentration [IC50] of 130 nM), vascular endothelial growth factor receptor (VEGFR) 2 (IC50 40 nM) and 3 (IC50 110 nM), and epidermal growth factor receptor (IC50 500 nM), and cabozantinib targets RET (IC50 4 nM), VEGFR2 (IC50 0.035 nM), and hepatocyte growth factor receptor c-Met (IC50 1.8 nM) (10 –13). The incidence of aggressive and advanced MTC with a need for TKI treatment is exceedingly low with only 1 case per 1–1.5 million inhabitants per year (14).
In the randomized phase 3 trial (ZETA study), 331 patients with locally advanced or metastatic MTC received vandetanib 300 mg/day (n = 231) or placebo (n = 100). It showed a significantly longer median progression-free survival (PFS) of 30.5 months in the vandetanib arm compared with 19.3 months in the placebo arm (hazard ratio [HR] 0.46, p < 0.001) (2). Objective response was more frequently observed in the vandetanib arm (45%) compared with the placebo arm (13%, odds ratio 5.48 [95% confidence interval, CI, 2.99–10.79], p < 0.001). No advantage of vandetanib on overall survival (OS) was observed most likely due to open-label crossover treatment with vandetanib in the placebo arm (2).
The phase 3 randomized EXAM study compared cabozantinib 140 mg/day with placebo in patients with metastatic MTC and documented progression on imaging within 14 months before enrollment (15). After random assignment to cabozantinib 140 mg/day or placebo, no crossover was permitted if tumor progression occurred in the placebo arm. The median PFS and OS were 11.2 and 26.6 months in the cabozantinib arm versus 4.0 and 21.1 months in the placebo arm (HR 0.28, p < 0.001, HR 0.85, p = 0.24), respectively (15). Cabozantinib appeared to be more active in patients who were RETM918T positive than in those who were RETM918T negative: RETM918T-positive patients had longer PFS and higher objective response rate versus RETM918T-negative patients (16). The results of the two studies are not directly comparable since the ZETA study also included patients without progression and allowed a crossover if progression occurred in the placebo arm, both of which were not permitted in the EXAM study.
Limited evidence is available for the use of vandetanib and cabozantinib outside clinical trials for the treatment of advanced MTC. In this retrospective study, we aim to analyze patient characteristics, TKI treatment parameters and efficacy, as well as TKI treatment emergent adverse events (TEAEs) in MTC patients receiving cabozantinib and/or vandetanib at four German tertiary medical centers.
Patients and Methods
Setting
This registry study was conducted as part of the German Study Group for rare malignant tumors of the thyroid and parathyroid glands. Prospectively and retrospectively collected data were obtained from records of patients diagnosed with MTC between 1990 and 2018 in four German tertiary care centers. All patients provided written informed consent, and the study was approved by the ethics committee of the University of Würzburg (96/13) and subsequently by the ethics committees of all participating centers.
Data acquisition
Eligible patients were adults with histopathological evidence of MTC with locally advanced disease and/or evidence of distant metastases who underwent TKI treatment with vandetanib and/or cabozantinib. The primary endpoint of this study was assessment of the response rate (based on routine clinical imaging along the lines of RECIST 1.0 and 1.1.) during TKI treatment. The secondary endpoints were assessment of PFS, OS, and prognostic factors of survival. In our analysis, in none of our patients, assessment of therapy response was based on evaluation of bone metastases as target lesions; only new occurrence of bone metastases was counted as progressive disease (PD). Patients still alive were censored at last follow-up. Treatment and follow-up of patients were performed according to local practice of participating centers. Efficacy was assessed locally by imaging (positron emission tomography-computed tomography [PET/CT], CT, magnetic resonance imaging of the liver and bone scintigraphy) and measurement of serum calcitonin and carcinoembryonic antigen (CEA) levels every three to six months.
Clinical data such as date of diagnosis, symptoms and tumor stage at initial diagnosis, RET germ line mutation status, prior treatments including surgical interventions and previous systemic therapies (e.g., peptide receptor radionuclide therapy [PRRT], cytotoxic chemotherapy, radiotherapy), date of diagnosis of metastatic disease, metastatic sites, serum concentrations of calcitonin and CEA, number of TKI treatment lines, treatment duration, treatment response, TKI-TEAE, and antiresorptive therapy (ART) were recorded by trained personnel at all sites.
Statistical analyses
PFS and OS probabilities were estimated using the Kaplan–Meier method and compared by log-rank test. For data with nonnormal distribution, we used the Mann–Whitney U test to detect differences between two points in time. p-Values <0.05 were considered statistically significant. Statistical analyses were performed with SPSS Version 25 (IBM, Chicago, IL).
Results
Clinical characteristics
Forty-eight patients (33 male, 15 female) with locally advanced MTC and/or evidence of distant metastases undergoing TKI treatment in four German tertiary care centers were included. Baseline clinical characteristics of the study population are shown in Table 1. The median follow-up from initial MTC diagnosis was 7 years (range 0–30 years). Most patients presented had sporadic disease (36; 75%), while 6 (13%) patients had a hereditary form of MTC (MEN2A or MEN2B). The germ line RET mutation status was not available for 6 (13%) patients. The median age at initial diagnosis of sporadic MTC was 46 years (range 15–80 years), and 40 years (range 15–61 years) for patients with hereditary MTC.
Patient Characteristics of the Study Cohort
CDT, calcitonin doubling time; CEA, carcinoembryonic antigen; MTC, medullary thyroid cancer; RET, rearranged during transfection; TKI, tyrosine kinase inhibitor.
At the time of initial diagnosis, 42 patients had locoregional lymph node metastases and 25 patients had distant metastases (brain 0 [0%], mediastinal lymph nodes 8 [32%], lung 11 [44%], liver 11 [44%], and bone 13 [52%]). Of the 15 (31%) patients without distant metastases, 13 (87%) had evidence of locoregional lymph node metastases. Data from 8 (17%) patients were not obtainable. The median age at diagnosis of metastatic disease was 50 years and was made at initial diagnosis of MTC in 25 (52%) patients. In patients in whom metastatic disease was detected, the median time between initial diagnosis and evidence of metastatic disease was 0 months (range 0–232 months). The median calcitonin doubling time (CDT) was 7 months (range 2–78 months) before TKI treatment initiation. The median age at TKI treatment initiation was 56 years (range 22–81 years), and the median time between initial diagnosis and starting TKI treatment was 58 months (range 0–316 months). In patients with distant metastases at initial diagnosis, the median time between initial diagnosis and starting TKI treatment was 53 months (range 0–199 months).
Tumor-specific therapy
Forty-three (90%) patients underwent thyroidectomy as initial therapy; in five (10%) patients, surgical resection of the primary tumor was not feasible. Treatment for local recurrence before TKI treatment was surgery in 28 (58%) patients, 9 (19%) patients underwent external beam radiation for neck recurrence, and 7 (15%) patients received combination treatment. Treatment of distant metastases included surgery in 11 (23%) patients, PRRT with 177Lu-DOTA-TATE in 4 (8%) patients, transarterial chemoembolization of liver metastases in 3 (6%) patients, selective internal radiation therapy of liver metastases in 1 patient (2%), and cytotoxic chemotherapy in 3 (6%) patients (doxorubicin, carboplatin/paclitaxel, and dacarbazine/5-fluorouracil).
By the time of TKI treatment initiation, 41 (85%) patients had locoregional lymph node metastases and 46 (96%) patients had distant metastases (brain 1 [2%], mediastinal lymph nodes 16 [35%], lung 26 [57%], liver 26 [57%], bone 30 [65%]). One patient had no distant metastases but unresectable local disease, and the data of another patient were not obtainable.
The median follow-up from the start of TKI treatment was 25 months (range 0–146 months). Targeted therapies with vandetanib and/or cabozantinib were administered in all 48 patients (Table 2). Specifically, all but one patient received vandetanib (47, 98%), and 23 (48%) patients additionally received cabozantinib. One patient received only cabozantinib. Assessing sequential therapies, 30 (63%) patients received two TKIs, 7 (15%) patients received three TKIs, and 3 (6%) patients received four TKIs (TKIs used: lenvatinib, nintedanib, pazopanib, sorafenib, sunitinib). Indications for TKI treatment were PD in 32 (67%) patients and high tumor burden at time of diagnosis in 15 (31%) patients. Data from one patient could not be obtained. In cases with documented PD, the median time until TKI initiation was 12 months. The median starting doses of vandetanib and cabozantinib were 300 mg/day (range 100–300 mg/day) and 80 mg/day (range 60–140 mg/day), respectively.
Tyrosine Kinase Inhibitor Treatment Characteristics and Response Rates a
Patients who received both TKIs were considered twice.
CI, 95% confidence interval; OS, overall survival; PFS, progression-free survival; PR, partial response; SD, stable disease.
Twenty-three (77%) patients with bone metastases received ART. Fourteen (61%) patients received bisphosphonates, 5 (22%) patients received denosumab, and 4 (17%) patients were sequentially treated with bisphosphonates and denosumab.
Vandetanib as first-line treatment
Characteristics of first-line treatment with vandetanib are summarized in Table 3. The median CDT before vandetanib initiation was 8 months. If PD was the reason for initiation of vandetanib treatment, the median time until TKI initiation was 12 months from the start of progression. The median time between primary diagnosis of MTC and vandetanib initiation was 65 months (range 0–316 months). Forty-one (85%) patients received vandetanib as first-line treatment: 25 patients before EMA approval of cabozantinib in March 2014 (52% of the whole patient cohort; 100% of the patients who were started on TKI before EMA approval of cabozantinib), and 16 patients after EMA approval of cabozantinib (33% of the whole patient cohort; 70% of the patients who were started on TKI after EMA approval of cabozantinib).
Therapeutic Characteristics in Patients Receiving Vandetanib or Cabozantinib as First-Line Treatment
EMA, European Medicines Agency.
The median duration of treatment was 21 months (range 1–120 months), and the median follow-up from the start of vandetanib was 24 months (range 2–146 months). Twenty-five (61%) patients started vandetanib treatment with the approved dosage of 300 mg/day, 5 (12%) patients received 200 mg/day, and 6 (15%) patients received 100 mg/day. Data from 5 (12%) patients could not be obtained. Twenty-five (61%) patients had bone metastases. After EMA approval of cabozantinib, 9 (56%) patients with bone metastases were started on first-line treatment with vandetanib. Concomitant therapies of bone metastases were ART in 6 (67%) patients (2 [33%] patients received denosumab and 4 [67%] patients received bisphosphonates). No patient received radiation therapy of bone metastases. Seven (44%) patients without bone metastases were started on vandetanib as first-line treatment after EMA approval of cabozantinib.
Cabozantinib as first-line treatment
Characteristics of first-line treatment with cabozantinib are shown in Table 3. The median CDT before TKI treatment was 4 months. If PD was the reason for initiation of cabozantinib treatment, the median time until TKI initiation was 11 months from the start of progression. The median time between primary MTC diagnosis and TKI initiation was 11 months (range 2–108 months). Seven patients (15% of the whole patient cohort; 30% of the patients who were started on TKI after EMA approval of cabozantinib) received cabozantinib as first-line treatment. Treatment was initiated for the following reasons: 3 (43%) physician's preference, 2 (29%) bone metastases, 1 (14%) PD, and in 1 (14%) case, it was patients' preference. The median starting dose was 60 mg/day (range 60–140 mg/day), and the median duration of treatment was 10 months (range 6–24 months). The median follow-up from the start of cabozantinib was 18 months (range 15–53 months). Only 1 (14%) patient received the approved dosage of 140 mg from the beginning. The physicians started with a reduced dose of cabozantinib to lower the potential risk of toxicity. Five (71%) patients had bone metastases. Concomitant therapies of bone metastases were radiation therapy in 3 (60%) patients and ART in 5 (100%) patients (2 [40%] patients received denosumab, 2 [40%] patients were sequentially treated with bisphosphonates and denosumab, and 1 [20%] patient received bisphosphonates).
Efficacy of vandetanib versus cabozantinib
Efficacy data are summarized in Table 2. The median duration of TKI treatment with vandetanib and cabozantinib was 17 and 9 months, respectively. Eighteen (38%) patients received vandetanib ≥24 months; 2 (9%) patients received cabozantinib ≥24 months. At the data cutoff, 15 (31%) patients were still receiving TKI treatment. Dose reduction was required in 14 (30%) patients receiving vandetanib and in 14 (61%) patients receiving cabozantinib. Twenty-three (49%) patients taking vandetanib and 9 (39%) patients taking cabozantinib discontinued treatment due to PD.
No patient had a complete response (CR). Partial response (PR) was the best morphological response in 12 (26%) patients taking vandetanib and in 5 (22%) patients taking cabozantinib. Stable disease (SD) ≥24 weeks was detected in 16 (34%) patients taking vandetanib and in 3 (13%) patients taking cabozantinib; SD ≥8 weeks but <24 weeks was observed in 8 (17%) patients taking vandetanib and in 5 (22%) patients taking cabozantinib. Ten (21%) patients taking vandetanib and 8 (35%) patients taking cabozantinib showed PD. Data from one patient taking vandetanib and from two patients taking cabozantinib could not be obtained.
The median PFS from vandetanib initiation was 17 months [CI 9.3–24.6 months], and the median PFS from cabozantinib initiation was 4 months [CI 3.1–4.9 months] (Fig. 1A, C). The 6- and 12-month survival rates were 98% and 86% for vandetanib and 78% and 70% for cabozantinib, respectively. The median OS from the start of vandetanib was 53 months [CI 43.7–62.3 months] and 24 months [CI 5.9–42.1 months] for cabozantinib (Fig. 1B, D). At the end of data collection, 24 (50%) patients had died, and 0 patients were lost to follow-up.

PFS and OS in months in patients taking cabozantinib (n = 23) and in patients taking vandetanib (n = 47). (
Calcitonin as well as CEA showed a significant reduction in patients treated with vandetanib (***p < 0.001, **p = 0.002), and in patients treated with cabozantinib, only calcitonin was significantly reduced (*p = 0.035).
Efficacy of first-line treatment versus second-line treatment
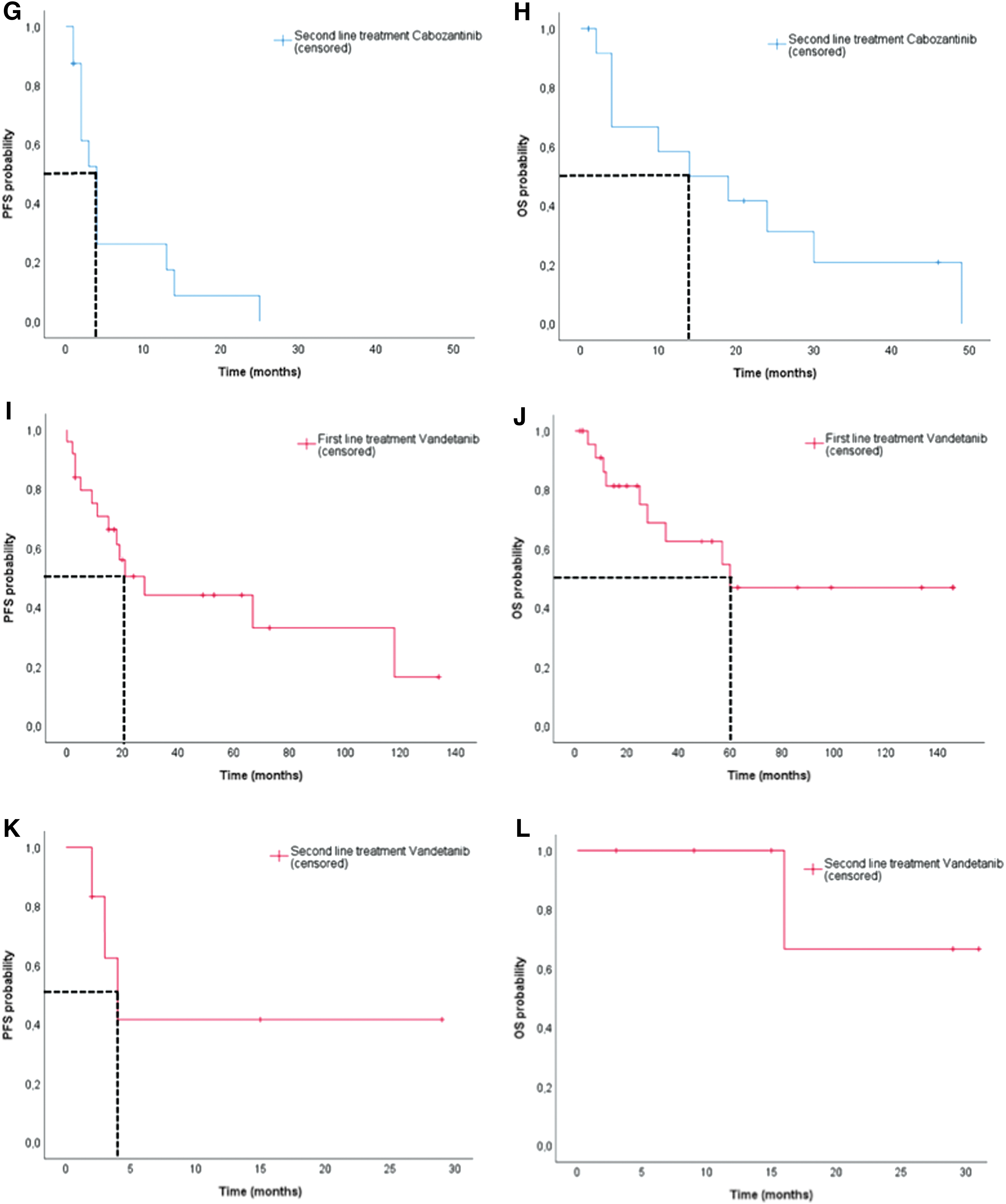
Efficacy data are summarized in Table 2 and Figure 2A–L. PR was the best response in 10 (24%) patients receiving vandetanib as first-line treatment; no patient receiving cabozantinib as first-line treatment showed PR. SD ≥24 weeks was detected in 16 (39%) patients receiving vandetanib and in 3 (43%) patients receiving cabozantinib as first-line treatment; SD ≥8 weeks but <24 weeks was observed in 5 (12%) patients taking vandetanib and in 1 (14%) patient taking cabozantinib as first-line treatment. When considering first-line treatment, 8 (20%) patients taking vandetanib and 2 (29%) patients taking cabozantinib showed PD.
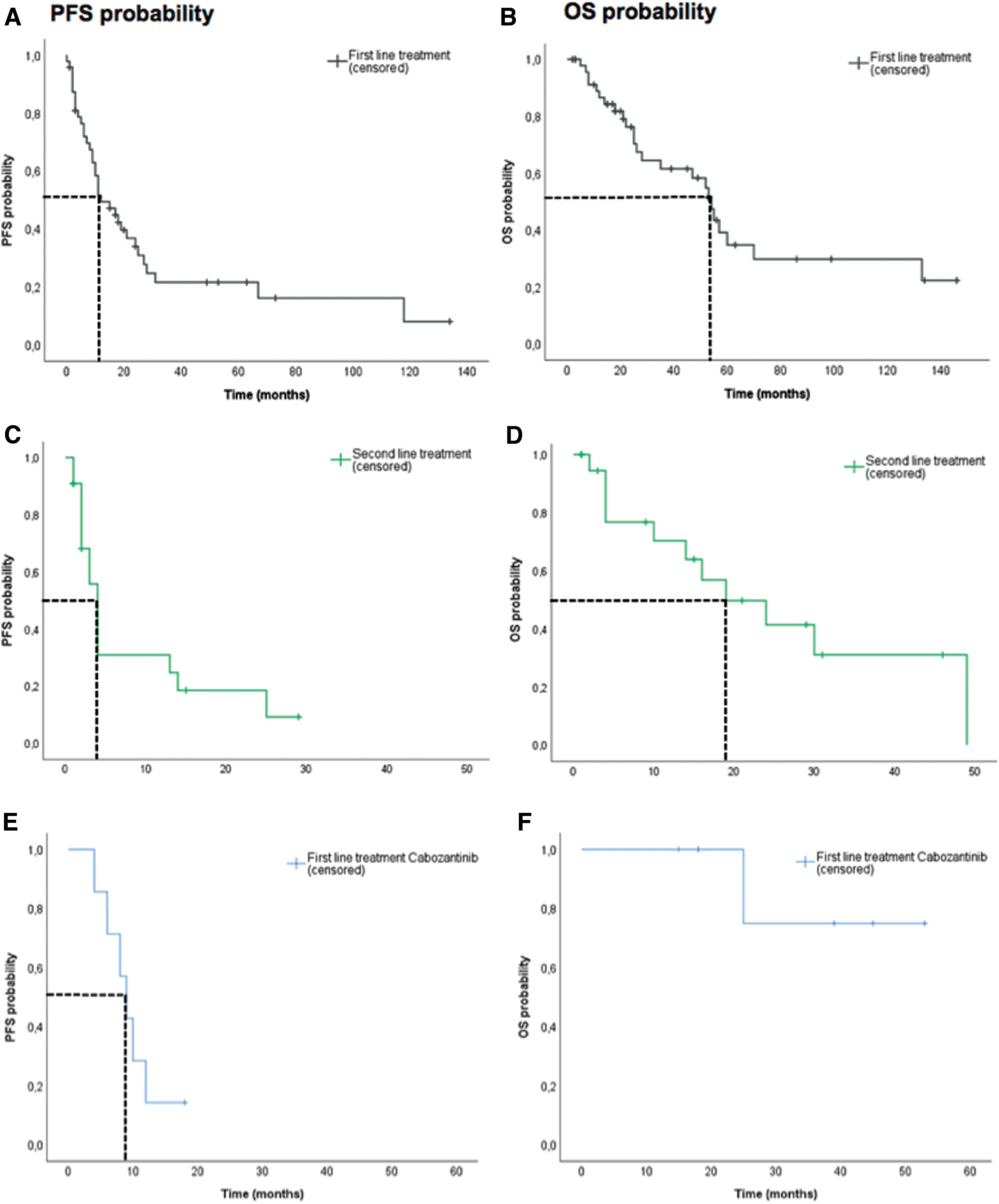
PFS and OS in months for first- and second-line treatment. (
Comparing patients with bone metastases, response to vandetanib was PR in 7 (28%) patients, SD ≥24 weeks in 10 (40%) patients, SD ≥8 weeks but <24 weeks in 2 (8%) patients, and PD in 6 (24%) patients. No patient with bone metastases had a PR to treatment with cabozantinib. SD ≥24 weeks was detected in 2 (40%) patients, SD ≥8 weeks but <24 weeks in 1 (20%) patient, and PD in 2 (40%) patients. In patients with bone metastases, the median PFS was 17 months [CI 7.8–26.2 months] and the median OS was 52 months [CI 14.3–89.7 months] for vandetanib, and the median PFS was 9 months [CI 6.4–11.6 months] for cabozantinib in the first-line setting; the median OS was not reached for cabozantinib-treated patients.
Twenty-four (59%) patients showed a decrease of calcitonin levels during first-line treatment with vandetanib, and 18 (44%) patients showed a decrease of CEA levels. Four (57%) patients showed a decrease of calcitonin levels during first-line treatment with cabozantinib, and 3 (43%) patients showed a decrease of CEA levels.
The median duration of second-line treatment with vandetanib and cabozantinib was 9 and 9 months, respectively. Analysis of the efficacy in the second-line setting showed PR in 2 (33%) patients taking vandetanib and in 5 (31%) patients taking cabozantinib; no patient showed SD ≥24 weeks. SD ≥8 weeks but <24 weeks was observed in 2 (33%) patients taking vandetanib and in 4 (25%) patients taking cabozantinib, while PD was observed in 2 (33%) patients taking vandetanib and in 7 (44%) patients taking cabozantinib.
Safety and tolerability
Nine (19%) patients taking vandetanib and 12 (52%) patients taking cabozantinib discontinued treatment due to TEAEs.
In vandetanib-treated patients, the most frequently reported TEAEs were diarrhea (40%), skin rash (38%), and fatigue (28%). In cabozantinib-treated patients, diarrhea (57%), loss of appetite/loss of weight (56%), and fatigue (39%) were the most frequently reported TEAEs. Patients taking cabozantinib showed a higher incidence of laboratory abnormalities including blood count changes, change in electrolytes, and thyrotropin elevation in comparison to vandetanib-treated patients. No patient taking cabozantinib had a documented prolongation of the QT interval, while 10 (21%) patients receiving vandetanib showed prolongation of QT interval. Hand-foot syndrome was more frequent in patients taking cabozantinib than in those taking vandetanib (7 [30%] vs. 1 [2%]).
Association between different features and PFS and OS
The association between different features and PFS as well as OS is summarized in Table 4. The PFS in patients taking vandetanib was significantly associated with the total number of TEAEs, patient age at TKI treatment initiation, and the presence of bone metastases: patients with ≥5 TEAEs in comparison to those with 0–4 TEAEs, patients aged ≤60 years, and patients without bone metastases showed a significantly longer PFS. The OS in patients taking vandetanib was significantly associated with total number of TEAEs and patient age at TKI treatment initiation: patients having ≥5 TEAEs and patients aged ≤60 years showed a significantly longer OS. Sex, germ line RET mutation status, and liver metastases status were not significantly associated with the PFS and OS in patients treated with vandetanib.
Association of Different Features with Progression-Free Survival and Overall Survival by Log-Rank Test
In multiple Cox regression with stepwise forward selection of the potential prognostic factors such as age (≤/>60 years), sex, RET germline mutation status (wild type, mutated, unknown), TEAE (absent, present), liver metastases (absent, present), and bone metastases (absent, present), variables that were relevant in univariate analyses were confirmed as single independent prognostic variables for PFS and OS with vandetanib and for OS with cabozantinib. Age was confirmed as single independent prognostic variable of PFS with cabozantinib.
p < 0.05; ** p < 0.01; *** p < 0.001.
TEAE, treatment emergent adverse event.
The PFS in patients taking cabozantinib was significantly associated TEAEs and patient age at TKI treatment initiation: patients without TEAEs and patients aged >60 years showed a significantly shorter PFS than patients experiencing TEAEs and patients aged ≤60 years. The OS in patients taking cabozantinib was significantly associated with TEAEs and the total number of TEAEs: patients having TEAEs and patients with a total number of ≥5 TEAEs showed a significantly longer OS than patients without TEAEs and those with 0–4 TEAEs. Sex, germ line RET mutation status, bone metastases, and liver metastases were not significantly associated with the PFS and OS in patients treated with cabozantinib.
Discussion
The main goal of this study was to investigate real-world clinical data from patients with metastatic or locally advanced MTC who received treatment with vandetanib and/or cabozantinib outside the framework of a clinical trial.
The results of our retrospective analysis confirm that vandetanib and cabozantinib are effective treatment options in the majority of MTC patients. The efficacy of vandetanib in our retrospective analysis is consistent with previously reported results (14). The difference in comparison to the phase 3 ZETA trial, with an estimated PFS of 30.5 months, is most probably due to differences in patient selection, since PD was not required for study inclusion in the ZETA trial in contrast to the patients in this retrospective analysis, where the majority of patients had PD at the start of treatment (2,17). The fact that our cohort showed a median time of 0 months between initial diagnosis and evidence of metastatic disease and a CDT <1 year before TKI initiation also illustrates the aggressive course of the disease in these patients. It is well established that the CDT is an independent predictor of recurrence and survival (18 –20). Despite the fact that a majority of patients had metastatic disease at the time of diagnosis, the time between the initial MTC diagnosis and TKI treatment initiation was 4.8 years, and even after PD was diagnosed, TKI treatment was started only after an average of 12 months, which demonstrates that all included centers used active surveillance strategy even in metastatic disease according to current guideline recommendations (9,20).
In terms of tumor evaluation, our results for PR (26%) and SD ≥24 weeks (34%) in vandetanib-treated patients are in agreement with the French data from Chougnet et al. showing a PR in 20% and a SD ≥24 weeks in 38% of patients (14). The lack of CRs achieved in patients treated with vandetanib is consistent with the results from the ZETA trial and a recent meta-analysis by Trimboli et al. showing vandetanib resulted in CR in <1 in 100 MTC patients (21). Safety and tolerability including rate of treatment discontinuation due to TEAE in vandetanib-treated patients were consistent with the results of prior studies (2,14,17,22,23). The median treatment duration of vandetanib is in agreement with the clinical trials (18.8, 20.7 months), but longer than that in two French cohorts (9.7 and 7 months) (2,14,17,24), which may be due to increasing experience and improved side effect management using vandetanib over the years in our cohort.
Real-world data from 15 MTC patients treated with cabozantinib outside a clinical trial were reported by Tiedje et al. showing a median PFS of 4.6 months in their retrospective study (25). This is consistent with our data showing a median PFS of 4 months but low than the EXAM trial (PFS 11.2 months in cabozantinib-treated patients) (15). We hypothesize that the lower response rates of cabozantinib-treated patients in comparison with vandetanib-treated patients are most likely due the fact that cabozantinib was mainly used as a second-line treatment after PD on vandetanib as initial therapy. However, based on our retrospective data analysis, we cannot fully exclude different degrees of efficacy of the two drugs. In addition, reasons for first-line treatment with cabozantinib were distinct patient characteristics, such as bone metastases, that are known to be an independent poor prognostic factor (26), and rapid disease progression, based on the results of the EXAM trial showing therapeutic efficacy in the subgroup analysis of patients with bone metastases and the design of the EXAM trial where in contrast to the ZETA trial only patients with fairly rapidly PD with a PFS of 4 months in the placebo group were included (15,27). This suggests a selection of patients with more aggressive clinical course for first-line treatment with cabozantinib, at least in part contributing to the worse PFS and OS. Furthermore, only 30% of patients received the full dosage of 140 mg/day at treatment and a high proportion of patients (61%) required a dose reduction due to TEAE. This confirms the data from the EXAM trial that TEAEs are frequent in cabozantinib-treated patients and use of the full dosage leads to a dose reduction and discontinuation of treatment in a high number of patients (15). Based on these observations, expert consensus is currently favoring a starting dose of 60 mg/day (5). The TEAE profile in cabozantinib-treated patients is consistent with the EXAM study (most frequent TEAEs: diarrhea, loss of appetite/loss of weight, fatigue) (15), also resulting in a similar treatment duration.
Our data suggest that – based on the different trial design with requirement of PD by RECIST criteria only in the EXAM trial with a PFS in the placebo group of 4 months versus 19.3 months in the ZETA trial – cabozantinib was used in patients with a more aggressive course of disease (2,15,27). Patients treated with cabozantinib in the first-line setting showed a much shorter time period between primary diagnosis of MTC and TKI treatment initiation (11 months vs. 65 months for vandetanib), a shorter CDT (4 months vs. 8 months for vandetanib), compared with patients receiving vandetanib in the first-line setting. However, there is no clear evidence for a higher efficacy of cabozantinib in patients with more aggressive disease compared with vandetanib due to the lack of a comparative trial. In our analysis, also patients receiving vandetanib had metastatic disease and most often showed PD before starting TKI treatment. Compared with cabozantinib, first-line treatment with vandetanib was associated with a considerable PR rate of 24% (vs. 0% for cabozantinib) and a PFS of 12 months (vs. 9 months for cabozantinib). Cabozantinib-treated patients showed SD as the best response without achievement of PR. Our efficacy data seem to favor first-line treatment with vandetanib; however, the low number of patients receiving first-line treatment with cabozantinib and their more aggressive course of disease need to be taken into account.
The high proportion of patients receiving vandetanib as first-line treatment is at least in part caused by the FDA and EMA approval of vandetanib two years before cabozantinib. Nevertheless, even after the approval of cabozantinib, 70% of patients were treated with vandetanib as first-line treatment including patients with high tumor burden, PD, and bone metastases, probably due to the lower toxicity profile of vandetanib and the more extensive clinical experience that had been gathered with vandetanib.
Both TKIs demonstrated similar efficacy in the second-line setting resulting in PR in around 30% of patients.
Even in patients with bone metastases, only one third of patients were started on cabozantinib; two thirds of patients received vandetanib showing similar efficacy of both drugs, in regard to PR rate and PFS, vandetanib seems to be even more effective. Nevertheless, these data need to be interpreted with caution due to a limited number of patients receiving first-line treatment with cabozantinib and their more aggressive course of disease.
In vandetanib-treated patients, the PFS and OS were significantly associated with age; older age at TKI treatment initiation (>60 years) was associated with poorer outcome. This is in line with new data from Valerio et al. showing that younger age in MTC patients treated with vandetanib was significantly correlated with a better outcome (28). In cabozantinib-treated patients, this trend was only observed with regard to PFS. Furthermore, in both vandetanib- and cabozantinib-treated patients, occurrence of TEAEs and total number of TEAEs were significantly associated with survival, showing that either the occurrence of TEAE at all or ≥5 TEAEs had a positive impact on patients' outcome. This could be also due to a bias since patients with a longer treatment duration have a higher likelihood of developing a higher number of TEAEs. A higher number of TEAEs could also result from a higher level of compliance in these patients, also providing an explanation for the improved outcome. In line with this observation, new Italian data from long-term vandetanib-treated patients confirm a significant correlation of treatment-emergent hypertension and adverse events with a better outcome (28,29).
Our analysis provides evidence for reduction of PFS in vandetanib-treated patients in the presence of bone metastases in comparison to vandetanib-treated patients without bone metastases. In patients receiving cabozantinib, the presence of bone metastases was not significantly associated with survival, which may suggest a superiority of cabozantinib over vandetanib in patients with bone metastases. These data are consistent with the subgroup analysis of patients with bone metastases in the EXAM trial showing therapeutic efficacy of cabozantinib (16).
Our study of 48 MTC patients treated with TKIs at four specialized centers in Germany has some limitations: missing data due to its retrospective nature, small patient number in the different subgroups, in particular in the group of first-line treatment with cabozantinib, lack of uniform and systematic follow-up, heterogeneity of patient management, and the evaluation of images by different radiologists.
In our study, active surveillance was followed despite the presence of metastatic disease in a majority of patients at initial diagnosis. These results emphasize that vandetanib and cabozantinib are effective drugs in MTC patients with an aggressive course of disease as first- and second-line treatments.
Footnotes
Author Disclosure Statement
Viktoria F. Koehler has received honoraria for lectures and travel expenses from Novartis and Sanofi. Stephanie Allelein has received honoraria for lectures and travel expenses from Sanofi. Matthias Schott has received honoraria for advisory boards and lectures from Sanofi, Eisai and Ipsen. Matthias Kroiss has received institutional research support from Ipsen, Loxo Oncology and Lilly, travel support from Eisai, Ipsen, HRA Pharma, MCI Germany and Lilly, honoraria for lectures from Bristol-Myers Squibb, Eisai, Lilly, and MSD and consultancy honoraria from Lilly. Christine Spitzweg has received honoraria for advisory boards and lectures from Ipsen, Lilly, Bayer, Eisai, Genzyme. Pia Adam, Karin Frank-Raue, Friedhelm Raue, Elke Berg and Eva Hoster have no competing financial interests.
Funding Information
This work was supported by the Deutsche Forschungsgemeinschaft, Priority Programme SPP1629 (SP 581/6-2) and Collaborative Research Center SFB 824 (project C8), and by the “Förderprogramm für Forschung und Lehre (FöFoLe), Reg.-Nr. 1031” of the medical faculty of the LMU Munich. The German Study Group for Rare Malignant Tumors of the Thyroid and Parathyroid Glands received unrestricted grant support from Bayer and Eisai.