
Abstract
Background:
Few small-scale studies have reported a genetic and familial predisposition in Hashimoto's thyroiditis (HT), however, quantified familial risk estimates from population-level data are unavailable. We aimed to estimate the incidence and familial risk of HT among first-degree relatives (FDR) according to age, sex, and family relationships.
Methods:
We conducted a population-based study in the general population of Korea from 2002 to 2017. Using the nationwide health insurance database, which has full population coverage and family relationship information, a cohort of 22 million individuals with blood-related FDR comprising 12 million families were followed up for a familial occurrence of HT. Age- and sex-adjusted incidence risk ratios (IRRs) were calculated in individuals with an affected FDR compared with those without an affected FDR.
Results:
Among 21,940,795 individuals, 234,912 had an HT-affected FDR, of whom 2425 familial cases developed HT with an incidence of 7.12/10,000 person-years. The familial risk for HT was 6.5-fold (95% confidence interval [CI]: 6.24–6.78) higher in individuals with versus without affected FDR. According to relationship, familial risks were IRR 102.71, IRR 7.80, IRR 5.54, and IRR 5.52 with an affected twin, sibling, mother, and father, respectively, and the corresponding incidence (/10,000 person-years) was 115.57, 10.66, 5.73, and 5.91. Same-sex twins had three times higher risk of developing HT than opposite-sex twins (IRR 121.01 vs. 21.46). The sex-specific familial risk was higher in males than females. The risks demonstrated age dependence, being higher in younger age groups.
Conclusions:
This study represents the largest population-based study of familial HT risk in Asia. We demonstrated elevated familial risk of incident HT among FDR, but with lower magnitude as those observed in previous studies. Familial risk increased with the degree of genetic relatedness among FDR indicating a prominent role of genetic factors in the familial aggregation of HT. Elevated risks in the younger age groups should motivate clinicians to screen people with a family history, especially those <30 years.
Introduction
Hashimoto's thyroiditis (HT) is an autoimmune chronic inflammation of the thyroid gland (1 –3). Its annual incidence is about 1 case/1000 persons and women are eight times more likely to be affected with HT than men (4 –7).
Although the underlying mechanisms in its pathogenesis are unclear, several risk factors have been proposed in the etiology of HT, such as hormones, or various environmental risk factors such as iodine intake, smoking, or infections (6,8). Genetic predisposition to HT has been suggested by small-scale family and twin studies that report disease concordance of 33% in siblings (9,10) and 55% in monozygotic twins compared with 0% in dizygotic twins (11,12). Also, several genome-wide association studies (GWASs) have identified a number of specific genes associated with the disease (13,14).
Previous familial aggregation studies have described a 21–32-fold (15,16) increased risk of HT among affected first-degree relatives (FDR). However, evidence for a genetic predisposition in familial HT remains limited, mainly because of the scarcity of studies available (15 –19). Moreover, existing studies have rather small sample sizes ranging from 20 to a few hundred cases and heterogeneous study designs. Due to low statistical power, detailed assessment of familial risk according to age, sex, and relationships was not possible; and because of their case/control study design, incidence and risk ratios could not be estimated. Moreover, most previous studies were conducted in specialized centers and may have included cases with more disease severity than in the general population.
Thus, precise quantification of familial risk estimates for HT from population-level data is essential, as an effort to understand the genetic scope in the pathogenesis of the disease.
We report here a population-based family study of HT, which included 22 million individuals with blood-related FDR, by using the Korean National Health Insurance (NHI) database that contains health care utilization and family relationship information of the entire population. We aimed to quantify the incidence and familial risk of HT among FDR of affected patients according to age, sex, and FDR relationship in the general Korean public.
Methods
Data source
The Korean NHI is a government-operated service that provides mandatory health insurance to the entire nation. Since this study used the NHI database, which has full population coverage and kinship information of all insured individuals and their dependents, it allows us to identify family members and their relationships, specifically FDR. The NHI data are also linked to the National Health Screening Program (NHSP) database that records results of standardized biannual health checkups, including details of lifestyle health behaviors such as smoking status (for details see Supplementary Data S1).
Study population
Among ∼50 million individuals, 21,940,795 individuals with blood-related FDR comprising 12 million families were included in this study, using the NHI and linked NHSP databases. Only individuals who had both biological parents and any full siblings were included.
Biological offspring were defined as individual(s) who were registered as a dependent from birth to a married couple as well as linked to the mother who had complete childbirth history and registered in the NHI database. Biological mother of an offspring was defined based on health care utilization details of pregnancy and birth history of the child who was also registered as a dependent in the NHI. Biological father of an offspring was the individual who married the biological mother before she conceived the specific child and was registered in the NHI database as a dependent. Two individuals sharing same biological parents were defined as full siblings, and twins were defined as full siblings who shared a birth date (±7 days).
To ensure only blood-related FDR were included, we excluded individuals with single parents, stepparents, and half siblings, and children not registered as dependents at their birth.
Identification of HT cases
We selected HT cases, based on our case algorithm that defined an individual having HT as the principle diagnosis as per International Classification of Disease 10th revision code E06.3, and at the same time underwent physical examination (goiter) and blood tests for HT (thyrotropin, thyroxine, and antithyroid autoantibodies), in at least two health care visits within the first year of initial diagnosis. The definition of HT in the general population was based on test activity, since thyroid testing results are not recorded in the NHI database, only the test activity is. In our validation study to verify the diagnostic accuracy of HT cases (Supplementary Data S2), the algorithm chosen had HT as the principle diagnosis twice or more with a specificity of 90% and a sensitivity of 95%.
Statistical analyses
The IRB number was KUIRB-2020-0202-01. The study population was followed from January 1, 2002, up to a diagnosis of HT, death, or end of follow-up on December 31, 2017, whichever came first. Individuals born after January 1, 2002, were followed since birth. Figure 1 shows the study flow diagram.
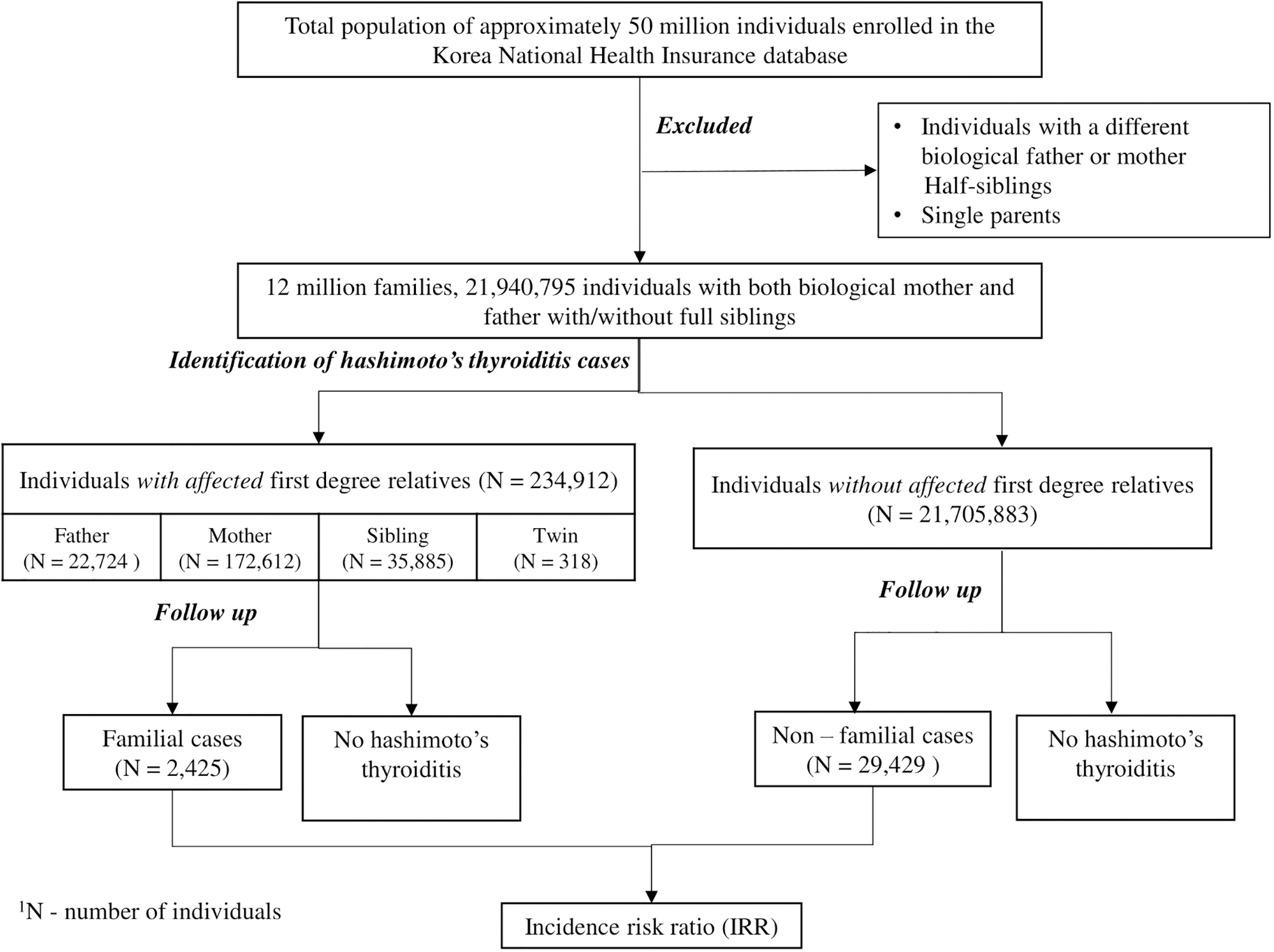
Study cohort selection flow diagram of HT among FDR in the population of Korea. FDR, first-degree relatives; HT, Hashimoto's thyroiditis; N, no. of individuals.
During the study period, once a family member was diagnosed with HT, other family members were considered “exposed” and assigned as “with affected FDR.” If a second family member become ill, that member was defined as the first “family case,” and remaining family members were considered exposed to two family cases starting from the date of diagnosis of the second case and assigned as “with >1 affected FDR.” A similar accretive pattern was followed when three family members were diagnosed and so forth. Of note, in assessing the familial risk for offspring with affected parents, we included cases of parents affected before offspring as well as offspring affected before parents (Supplementary Table S1).
Person-years were calculated for each study subject starting from the day of HT diagnosis up to their respective censored point. “Total person-years” was the sum of person-years of all study subjects. Incidence rate was calculated by dividing cases by the total person-years at risk. Poisson regression was used to estimate familial risk, represented as incidence risk ratios (IRRs) with 95% confidence intervals (CIs), by comparing the incidence rate of HT in individuals with versus without affected FDR. All IRRs were adjusted for age and sex. IRRs were calculated according to FDR relationships as well. We also assessed familial risk in offspring when both parents were affected.
To evaluate the effect of age or sex on familial risk, we conducted separate age- and sex-stratified familial analyses. Sex-specific familial risks were calculated separately for both sexes, by comparing HT incidence in males (or females) with versus without affected FDR. Age-specific familial risks were evaluated by analyzing IRRs separately according to age groups, that is, by comparing HT incidence in a particular age group of individuals with versus without affected FDR. In addition, age- and sex-specific familial risks were also analyzed according to FDR relationship.
To examine familial risk adjusted for smoking status, hazard ratios were calculated for a subset of subjects who had smoking status assessed in the NHSP.
All statistical analyses were performed using Stata/MP 13.1 (Stata Corp, College Station, TX).
Results
General cohort description
Table 1 presents the general demographics of 21,940,795 individuals with blood-related FDR identified from the NHI database. Of the included families, 3,290,494 (47%), 3,409,015 (46%), 477,618 (6%), and 43,010 (0.6%) had one, two, three, and four offspring, respectively. During the study period, 136,752 individuals developed HT (88.6% female, n = 121,201) corresponding to a female-to-male ratio of 8:1.
Demographics of Individuals With and Without First-Degree Relatives Affected by Hashimoto's Thyroiditis
FDR, first-degree relatives; n, number of individuals.
Familial risk analyses for HT
Table 2 shows family relationship analyses through which we identified 234,912 individuals with affected FDR, of whom 2425 familial cases developed HT with an incidence (person-years) of 7.12/10,000. And among 21,705,883 individuals without affected FDR, 29,429 nonfamilial cases developed the disease with an incidence of 0.96/10,000. Accordingly, familial risk of HT was significantly elevated in individuals with versus without affected FDR, with an IRR (CI) of 6.50 (6.24–6.78) (Table 2). Familial cases accounted for 8.24% of the total HT cases.
Familial Risk for Hashimoto's Thyroiditis in First-Degree Relatives
CI, 95% confidence interval; HT, Hashimoto's thyroiditis; IRR, incidence risk ratio.
After adjusting for smoking, familial risk showed slight attenuation (Supplementary Tables S2 and S3) from a 4.8- to 4.2-fold, suggesting limited contribution of smoking as a risk factor in the familial aggregation of HT.
According to family relationships, we found that familial risk increased with the degree of genetic relatedness (Table 2). HT incidence in offspring with affected father and affected mother was 5.91/10,000 and 5.73/10,000, respectively, and the corresponding IRRs were 5.52 (4.80–6.35) and 5.54 (5.26–5.85), representing similar risk of disease with either affected parent. On the contrary, we found that the risk was threefold higher in offspring when both parents were affected compared with one (Supplementary Table S4).
Familial risk in individuals with affected siblings was IRR 7.80 (7.20–8.46) with an incidence of 10.66/10,000, and those with affected twins had a markedly higher risk of HT with IRR 102.71 (78.24–134.81) and an incidence of 115.57/10,000. Among twins, 9.5% same-sex twins (50 cases/528 people) developed HT with an incidence of 140.06/10,000 and IRR 121.03 (91.71–159.73) and 3.3% opposite-sex twins (2 cases/60 people) developed the disease with incidence of 21.51/10,000 and IRR 21.46 (5.37–85.81) (Fig. 2). Having more than one affected FDR significantly increased the risk of HT to IRR 25.81 (22.22–29.98) with an incidence of 33.64/10,000.
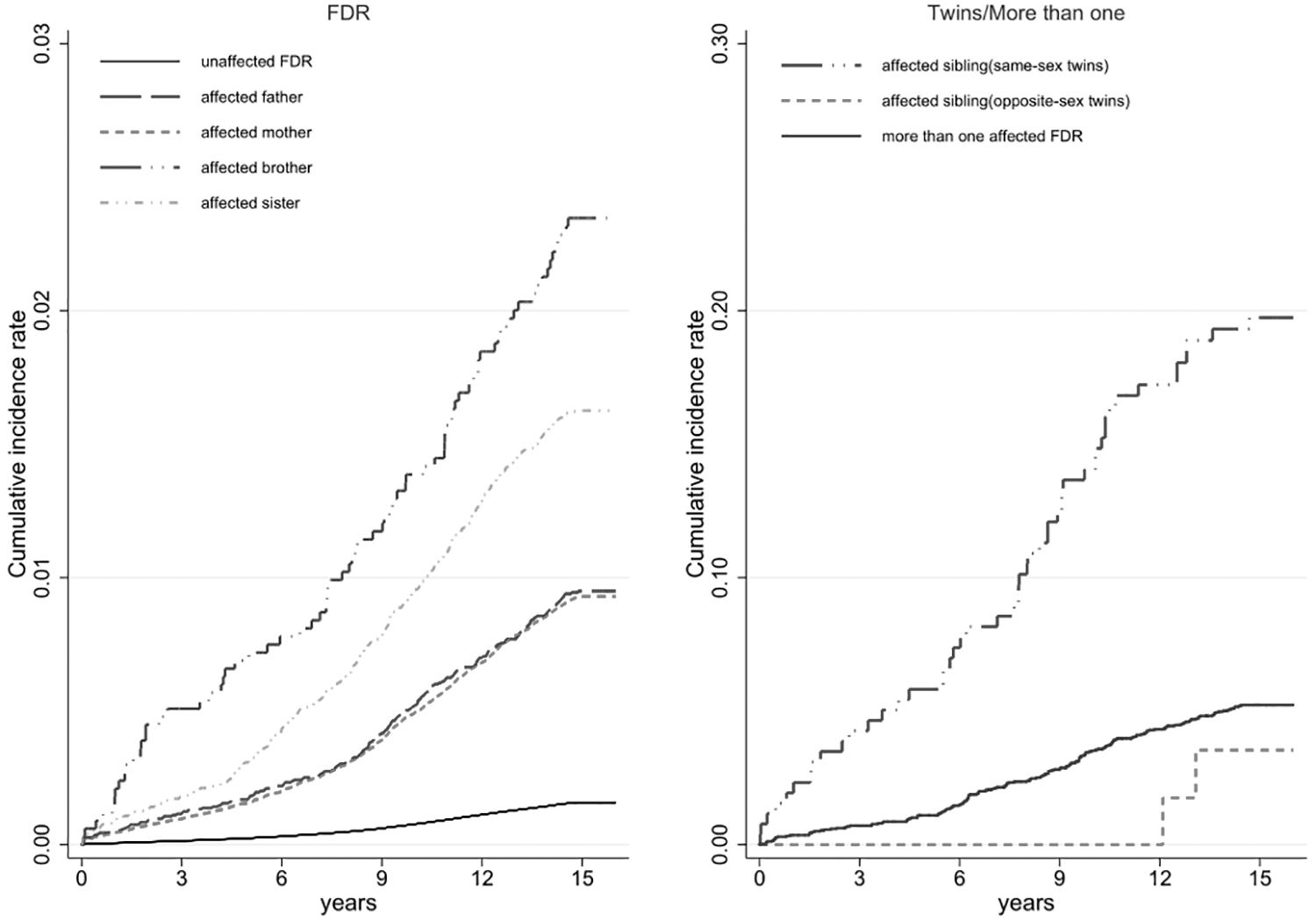
Time-related incidence of familial HT in FDR: left—according to relationships, right—according to sex of twins and more than one affected FDR.
Figure 2 shows the temporal relationship of the cumulative incidence with familial HT. Familial risk increased with the degree of genetic relatedness and the cumulative incidence of HT became more pronounced in those with a family history as time progressed.
Sex-specific familial risk
Table 3 presents the familial risk for HT according to sex. Sex-specific familial risk was higher in males compared with females, with IRRs 7.20 (6.41–8.08) and 6.12 (5.85–6.40), respectively. Meanwhile, HT incidence in familial cases was higher in females than males (13.75/10,000 vs. 1.68/10,000).
Sex-Specific Familial Risk for Hashimoto's Thyroiditis in First-Degree Relatives
Although risk of HT in offspring was similar to the mother and father (IRRs 5.54 vs. 5.52), the risk of disease in siblings was greater with an affected brother than an affected sister (IRRs 10.37 vs. 7.53).
In parent/offspring pairs according to sex, the risk of disease was higher in mother/son (IRR 5.85) compared with mother/daughter (IRR 5.29), and father/son (IRR 8.05) compared with father/daughter (IRR 5.01), reflecting a higher risk in males in familial transmission. A similar situation was observed in sibling pairs, where the risk of HT was higher in sister/brother (IRR 8.23) than sister/sister (IRR 7.00), and brother/brother (IRR 11.26) than brother/sister (IRR 8.63).
Age-specific familial risk
Table 4 shows that the familial risk was age dependent. Higher IRRs were observed in younger age groups followed by a gradual decline in risk with increasing age. This trend of age dependence was seen in familial risks in all FDR relationships (Fig. 3) and was most prominent among siblings. However, small numbers limited precise estimates for some categories.
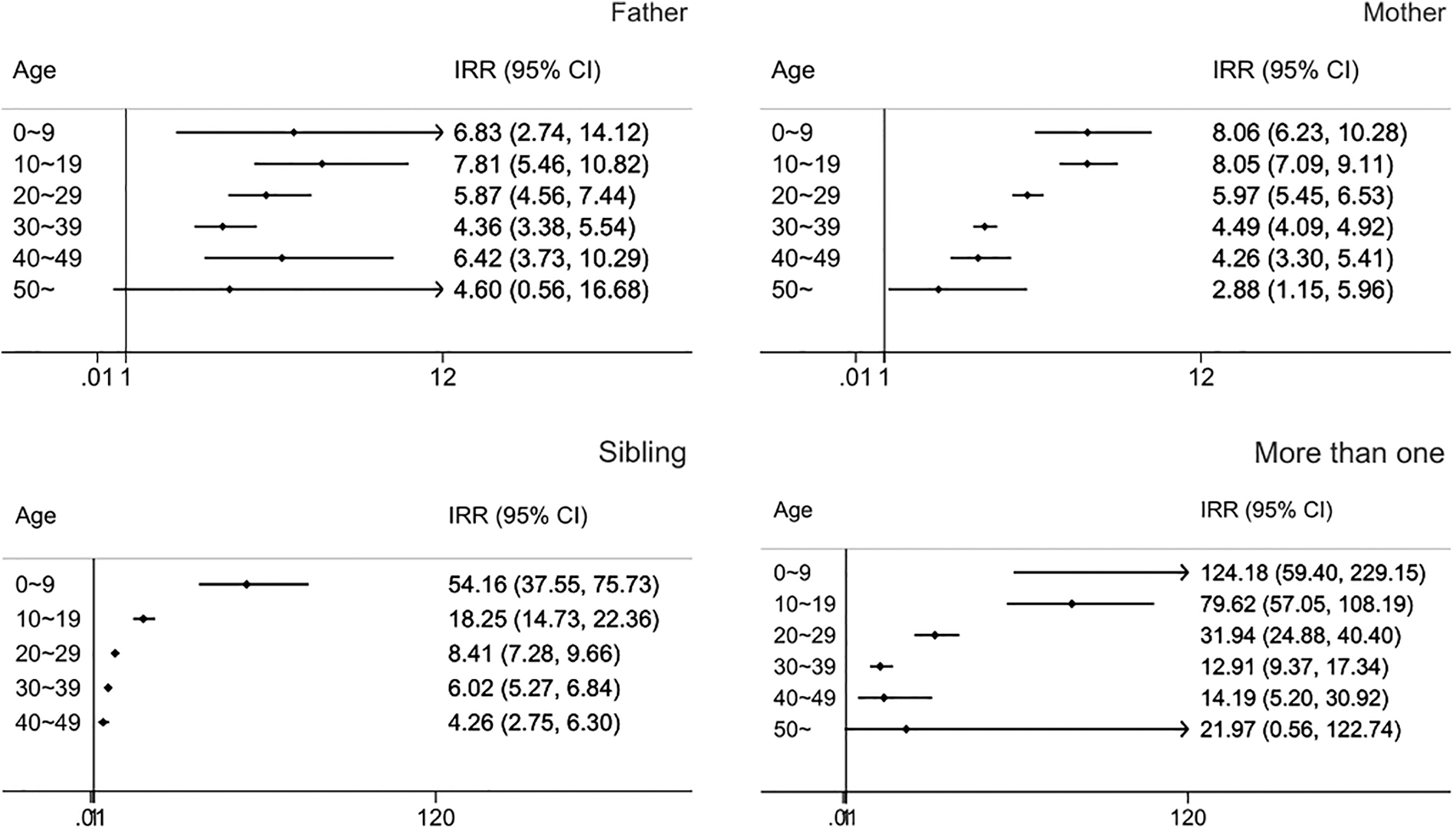
Age-specific familial risk of HT in individuals with affected FDR. 1Age groups are presented in 10-year intervals. IRR, incidence risk ratio.
Age-Specific Familial Risk for Hashimoto's Thyroiditis in First-Degree Relatives
Discussion
This population-based study used the NHI database to construct a large cohort of 21,940,795 individuals with both biological parents with or without full siblings and quantified the familial incidence and risk of HT according to age, sex, and FDR relationships. Overall, familial risk for HT was significantly higher, 6.5-fold, with an incidence of 7.12/10,000 person-years.
Familial aggregation in HT has been previously reported by a few small-scale studies. Altogether around four articles have documented the clustering of disease among family members—a multicenter cohort study with 400 HT patients (17), two studies with 39 cases each (16,18), and a U.S. study with 24 HT cases (15). Among them, two studies have reported 21–32-fold (16) and 28-fold (15) increased risk of HT in siblings and offspring of affected individuals.
Although our familial risk estimates are lower than previously reported, aforementioned studies used case/control study designs, which mostly used an up-line or a side-line approach to estimate risk ratios by following up parents or siblings of patients, and this could have resulted in overestimation of relative risks even if the ages or family sizes of the cases and controls were similar (20). Meanwhile, our down-line cohort study design followed offspring after identifying HT cases, which allowed us to evaluate disease risk according to family relationships. This could explain the relatively lower magnitude of familial risk in our study compared with previous data.
While previous studies mostly relied on obtaining HT diagnosis and family history data from interviews or questionnaires, we obtained this information by using the objective NHI data, thus minimizing recall errors. In addition, since prior studies were mostly hospital based, they possibly included more severe cases compared with patients in the community, which may have in turn affected familial risk estimates, whereas HT patients in our study were recruited from all health care institutions in Korea.
It is known that both genetic and shared environmental factors may contribute to the familial aggregation of a disease. Several findings in our study indicate that genetic determinants are the predominant drivers of familial aggregation in HT.
First, the familial risk for HT increased as the degree of genetic relatedness increased, with IRRs ranging from 5.53 with affected parents, 7.8 with affected siblings, and 102.71 with affected twins. Also, having >1 affected FDR resulted in a significant increase in familial risk. Moreover, we found that same-sex twins (IRR 121) were more likely to develop HT than opposite-sex twins (IRR 12). We consider that these same-sex twins are mainly monozygotic (≥80%), assuming they included all monozygotic twins and half of the dizygotic twins, given that the ratio of monozygotic:dizygotic in the general population is higher. The above findings along with the previously reported 55% HT concordance in monozygotic twins and 0% in dizygotic twins (11,12) indicate that the risk for developing HT is largely hereditary.
Second, the higher magnitude of familial risk for HT compared with other genetically determined diseases (approximately twofold) implies a significant contribution of genetic factors in disease pathogenesis. It is implausible that environmental factors alone could account for such a magnitude.
Third, familial risk estimates were more pronounced for younger ages. This finding is in accordance with epidemiological data that regard earlier age of disease onset in familial cases as a characteristic of genetic predisposition (21).
On the contrary, the 9.5% disease concordance among same-sex twins in our study and the 55% concordance rate in monozygotic twins in previous twin studies, both suggest environmental influences in the etiology of HT. Also, our results of familial risk adjusted for smoking status are in line with previous studies that have reported the protective effect of smoking in familial cases. These findings support that other unknown environmental factors may influence the development of HT.
According to several epidemiological studies, Asian countries have higher levels of both dietary iodine intake and HT incidence (22 –24), including Korea, where excessive iodine intake is commonly reported owing to various Korean cuisines that contain high iodine concentrations and are consumed ranging 250–750 μg/day (25). Accordingly, it can be considered that the higher sibling risk is possibly because of higher iodine intake in childhood and/or higher iodine intake over the years.
Although data on iodine intake were not available in the current study, we examined a recent Korean study (KNHANES) (25) that documented iodine intake in the general population of Korea for subjects aged 19–75 years over a time period of 16 years, which is in fact higher than other countries worldwide. For the age distribution of iodine intake, there was no significant difference between young and adult age groups. While for the time difference, mean iodine intake ranged from 641.6 μg in 1998 to 236.2 μg in 2014, indicating that the younger generation in our study who had higher familial risks for HT did not have more iodine sufficiency compared with their parents' generations. These findings suggest that environmental factors other than iodine must be explored.
The prevalence of thyroid antibodies has been variably reported by different countries. For instance, antibody prevalence in the United States is 11–13%, and similar results have been reported in Denmark (13.1%) and Tehran (11–13.6%) (26,27), and a higher antibody prevalence of 15% has been reported for Korea (28). While this high rate in Korea could be caused by genetic factors, it is also known that a high prevalence of thyroid antibodies and high HT incidence is associated with increased iodine intake. So, patients suspected for HT should be screened by measuring thyroid antibodies, especially in countries with high HT incidence and iodine sufficiency such as Korea.
Previous studies have suggested HT to be a polygenic disease (9,29) and several GWASs have identified many susceptibility genes such as HLA (9,30), PTPN22 (31,32), and CTLA (13) for HT. Our data of higher risk in younger age groups and increasing familial risk with narrowing genetic distance indirectly support that HT may have a polygenic mode of inheritance. A key finding in our results was the higher familial risk in siblings compared with offspring of affected parents, which can be explained by HLA expression codominant in each parent and shared by siblings, although not identically.
We demonstrated that although background incidence was lower in males, familial risk for HT was higher in men compared with women, implying that the impact of familial factors in HT pathogenesis is greater in the male sex. Moreover, risk in parent/offspring and sibling/sibling pairs reflected higher familial risk in males. Our finding of an increased familial risk of HT in males is noteworthy, since in other autoimmune diseases such as vitiligo (33) the risk of disease is higher in females. For underlying mechanisms, one may speculate a genetic predisposition in males, such as the suggested inactivation of the protective role of Y-linked genes (34,35), which needs to be further investigated.
Our findings of higher familial risks in younger age groups are known to be characteristic of genetic tendency (36), and thus, HT cases diagnosed in childhood should be considered for a likely genetic etiology and inspected for a family history. Although we think higher IRRs among younger age groups are mainly due to genetic factors, it could also be driven, in part, by a higher correlation between siblings as they share similar lifestyle patterns including dietary practices, which may contribute to the familial aggregation of HT. Also, partly by increased prevalence of antibodies in older adults, as a Korean study (28) has reported higher prevalence of thyroid antibodies in older age groups. This indicates that the older generations are already diseased and comparing their risk with siblings may exaggerate the sibling risks.
Limitations of the current study include accuracy of the HT diagnosis, which relied on administrative data. However, to maximize diagnostic accuracy, we developed case algorithms based on the number of hospital visits and selected an algorithm with the highest specificity and sensitivity.
One caveat in our study is ascertainment bias, as people with affected FDR may be more likely to seek health care utilization and/or more likely to be tested for HT than those without affected FDR. To examine for difference in ascertainment, we conducted a separate analysis and found that health care utilization for familial and nonfamilial cases was not very different (Supplementary Data S3, Supplementary Table S5). However, since the health care utilization is not specific for HT screening, there is still a potential for ascertainment bias as there is still a chance of not capturing subclinical disease.
Due to lack of zygosity information, we were not able to calculate separate risks for monozygotic and dizygotic twins. In addition, the follow-up period of the current study may not be sufficient enough to cover all familial occurrences.
In conclusion, based on a comprehensive population-based study of the entire South Korean population, we demonstrated a 6.5-fold significantly elevated familial risk of HT among FDR of affected individuals, but with a lower magnitude of familial risk compared with previous studies. Familial risk increased with the degree of genetic similarity among FDR indicating that genetic determinants are the predominant driver of familial aggregation in HT. Higher familial risks in siblings compared with parents/offspring suggest a role of gene/environment interactions, especially early-in-life shared environmental exposures such as dietary iodine, in the background of shared genetic susceptibility. Moreover, higher risks in younger age groups should motivate screening of people with a family history, especially those <30 years.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5