
Abstract
Background:
In the past two decades, new evidence and guidelines have emerged to refine recommendations for the use of radioactive iodine (RAI) therapy after thyroidectomy for cancer. We aim to describe national trends in RAI utilization, assess the impact of individual hospitals on RAI utilization, and examine whether variation in prescribing habits has declined over time.
Methods:
The National Cancer Database (NCDB) was queried from 2004 to 2016 for patients with papillary thyroid cancer (PTC) who received total thyroidectomy. Trends were analyzed using Joinpoint analysis. Hospital-specific effects and variation in prescribing habits were assessed through a hierarchical, mixed regression model.
Results:
RAI utilization declined from 61.0% in 2004 to 43.9% in 2016. RAI use declined most profoundly in patients with T1a, N0/X, M0 PTC without extrathyroidal extension (34.8% in 2004 to 9.5% in 2015), but continues to be used commonly in patients with advanced disease for whom it is routinely recommended (73.4% in 2004 to 72.0% in 2015). Furthermore, ∼80% of hospitals in 2016 utilized at or below the median utilization rate in 2006. Variation in RAI utilization across hospitals decreased by ∼50% from 2004 to 2016 (Levene's test p < 0.001), with a significant decline (p = 0.002) in the variation after 2012 (confidence interval: 2010 to 2014).
Conclusions:
Recommendations for whom to prescribe RAI appear to have impacted both the number of patients receiving RAI and the variation in prescribing habits across hospitals. Hospital selection has contributed less to the probability of receiving RAI over time.
Introduction
Papillary thyroid cancer (PTC), a type of well-differentiated thyroid cancer with a favorable prognosis, is the most common type of thyroid cancer (1). It is estimated that there will be 52,890 new cases of thyroid cancer in the United States in 2020, with PTC likely to account for ∼80% of these cases (2). Treatment for PTC commonly includes surgery, most often in the form of total thyroidectomy; however, thyroid lobectomy is sometimes performed in low-risk PTC (3). Following total thyroidectomy, radioactive iodine (RAI) therapy may be used for several purposes, including ablation of remnant normal thyroid tissue to allow for more sensitive follow-up screening, ablation of remnant microscopic tumor, and ablation of metastatic disease (4,5).
As noted in the treatment guidelines for well-differentiated thyroid cancer published by the American Thyroid Association (ATA) in 1996, many experts advocated for the use of RAI for nearly all patients after undergoing total thyroidectomy (6). Therefore, it is unsurprising that studies showed dramatic increases in RAI utilization from 1990 to 2008 using the National Cancer Database (NCDB) and from 1973 to 2007 using the Surveillance, Epidemiology, and End Results (SEER) database (7,8).
Both the ATA and the National Comprehensive Cancer Network (NCCN) provide recommendations for whom to prescribe RAI (5,9,10). Beginning with the 2006 ATA guidelines, which were updated in 2009 due to a growing body of literature on the treatment of differentiated thyroid cancer, more selective use of RAI was recommended (9,10). Since then, the 2015 ATA guidelines have called for even more sparing use of RAI and provided a more nuanced risk stratification system for patients with PTC (11,12).
Such guidelines advising less aggressive treatment of lower risk PTC are particularly relevant given that much of the growth in thyroid cancer incidence over the past several decades has been driven by a rise in diagnoses of lower risk cancers, which may be due to more sensitive screening tests (13 –17). One study showed possible inappropriate use of RAI in over 20% of PTCs <1 cm without adverse features, including nodal or metastatic spread, extrathyroidal extension, or positive surgical margins, diagnosed between 1998 and 2011 (17). This potential inappropriate use was associated with a sizeable cost burden to the health care system (18). Other studies have used national data to show a short-term decline in RAI utilization after publication of the 2006 and 2009 ATA guidelines (19 –21), and another recent study has demonstrated a decline in RAI use for low-risk thyroid cancer in California since the publication of the 2009 ATA guidelines (22).
However, no studies have specifically analyzed RAI utilization in clinical cohorts defined by ATA guidelines, and no studies have examined the long-term guideline adherence using national data. Furthermore, no studies have reported on changes in prescribing habits at the institutional level, which can help set benchmarks for intrainstitutional audit and review. Given the call for more selective and standardized treatment with RAI by the ATA in 2006 and 2009, we generated three hypotheses regarding RAI utilization in subsequent years: (i) there would be a decrease in RAI utilization overall, and especially in cases for which the guidelines recommend against RAI; (ii) the specific hospital at which a patient was treated would impact his or her probability of receiving RAI; and (iii) over time, the treating hospital would have less of an impact on a patient's probability of receiving RAI. Through analysis of national data from the NCDB, we tested each of these three hypotheses.
Materials and Methods
This work was granted an exemption from Institutional Review Board review by the Yale Human Research Protection Program.
Patient selection and inclusion criteria
Patients were selected by querying the NCDB for PTC diagnosed between 2004 and 2016 using ICD-O-3 histology/behavior codes (8050/3, 8260/3, 8340/3, 8341/3, 8343/3, and 8344/3, 8450/3). This group was refined by applying additional inclusion criteria: cancer staging using the 6th or 7th editions of the American Joint Committee on Cancer (AJCC) staging systems and patients who had total thyroidectomy (surgery code 50). Only patients who explicitly received radioisotopes or explicitly received no form of radiation therapy were further included. Recoding and temporal analysis were performed using SPSS versions 25 and 26 (Armonk, NY).
Analysis of the trends in RAI utilization was performed across three categories of patients based on the 2009 ATA practice guidelines: (i) patients for whom RAI is recommended, (ii) patients for whom RAI is not recommended, and (iii) patients for whom selective use of RAI is recommended. The 2009 ATA guidelines recommend RAI ablation in patients ≥45 years of age with a tumor >4 cm, patients with a tumor of any size with gross extrathyroidal extension, patients with residual disease after surgery, and patients with metastatic disease (M1). The guidelines do not recommend RAI for patients with nonmetastatic intrathyroidal tumors <1 cm (either unifocal or multifocal cancer with all foci <1 cm) and no nodal involvement (Nx/N0) or other concerning clinical or pathologic features. The guidelines recommend selective use of RAI in patients with nonmetastatic intrathyroidal tumors that are 1–4 cm, patients younger than the age of 45 with nonmetastatic intrathyroidal tumors >4 cm, patients with nonmetastatic multifocal intrathyroidal disease when at least one focus is >1 cm, patients with minimal extrathyroidal extension regardless of tumor size, and patients with nodal involvement (N1) (9). To best capture the abovementioned criteria, collaborative staging (CS) variables were used, which were coded for in the NCDB until 2015. Therefore, cases diagnosed in 2016 were not optimal for trend analysis, and were not included in trend analysis only. Patients for whom the RAI recommendation group could not be determined due to missing data were excluded from the trend analysis.
Statistical analyses
Trends in RAI utilization across each of the three patient categories outlined above were analyzed using the National Cancer Institute's Joinpoint program (version 4.7.0.0). Joinpoint analysis was performed on a linear scale, using at least 3 years to generate a line, and at least 2 years between joinpoints. Since two sets of ATA guidelines were issued during the study period (in 2006 and in 2009), a maximum number of two joinpoints were tested. The 2009 ATA guidelines were applied to identify cohorts of patients with high-, intermediate-, and low-risk thyroid cancer, and to investigate how RAI utilization had changed in these cohorts. All statistics were performed at an α = 0.05, with two-sided testing when applicable.
We also investigated how individual hospital prescribing habits impact the national average rate of RAI utilization using a hierarchical multivariable regression model. This model is similar, yet different from a traditional logistic regression. While a traditional logistic regression enters in “fixed” patient demographic, clinical, and oncologic factors to help predict which patients are more or less likely to receive RAI, it assumes that there is one large “average” facility to which all patients go for treatment. To address this limitation, and because facilities in the NCDB represent a sampling of all hospitals in the United States, each facility can be entered into a type of modified logistic regression model called a mixed hierarchical regression model as a “random” variable. It is “mixed” because it accounts for fixed patient demographic factors (i.e., age, sex, race/ethnicity, geographic location), patient clinical factors (i.e., comorbidity score, insurance status), hospital factors (i.e., facility reporting/case volume, facility type), and oncologic factors (i.e., pT, pN, cM, tumor multifocality, surgical margins), as well as the “random” hospital-specific factors (i.e., institutional habits).
Regression modeling was performed in SAS version 9.4 (SAS Institute, Inc., Cary, NC) using PROC GLIMMIX, as previously described (7). The model included fixed effects, described above, and random effects, including individual hospitals as the subjects and a random hospital-specific intercept. The analysis was performed for each year from 2004 to 2016. A final model was created through backward elimination of covariates that were not statistically significant in any year (p ≥ 0.05). Through this method, the covariates of the urban/rural continuum and Hispanic origin were excluded, as they did not improve the model.
From the final model, the probability for each patient receiving RAI adjusting for (i) fixed and random effects (PF
+R
), or (ii) just the fixed effects alone (PF
), was outputted. The difference of these two probabilities (1 and 2; PF
+R
− PF
) results in an estimate of the random effects alone (ΔP). In other words, PF
+R
estimates the probability of each patient receiving RAI after adjusting for patient demographic factors, clinical factors, hospital factors, and institutional preferences; PF
is equivalent to a traditional logistic regression that estimates the probability of each patient receiving RAI adjusting only for patient presentation and fixed clinical factors; and ΔP estimates how much more or less likely a patient is to receive RAI at a given hospital than expected based on a patient's demographic, clinical, and oncologic factors.
To assess the average probability of all patients at a given hospital to receive RAI, the average across patients at each institution (j) was calculated. These probabilities (P M,j , PF ,j , ΔPj ) were ordered from smallest to largest to rank hospitals for each year. Since the number of institutions captured by the NCDB changes over time, the hospital rank is reported as percentile.
We next assessed temporal trends in the variation in RAI utilization by hospital (i.e., how much more or less likely an individual institution prescribes RAI than expected, or ΔP). Variance over time in the distribution of ΔP (i.e., variation from expected) was fitted using a piecewise function, as no standard error could be specified for Joinpoint analysis. Homogeneity of variances over time was compared using Levene's test.
Results
Utilization of RAI has changed over time
After applying the inclusion criteria to the NCDB from 2004 to 2016, 273,046 subjects were selected for analysis (Fig. 1). Of patients diagnosed between 2004 and 2007, 61.2% received RAI therapy. By 2016, the percentage of patients receiving RAI therapy had declined to 43.9% (Fig. 2A). Using Joinpoint analysis, we identified that the decline in RAI began in 2007 (confidence interval [CI]: 2007 to 2009), at a linear rate of −2.0% (CI: −2.1 to −1.9) fewer patients per year receiving RAI. Since this analysis formed the foundation for subsequent analyses, this observation was validated in the population-based SEER data set (data not shown).

Flow diagram detailing inclusion criteria into the study with total number of subjects (n) remaining.
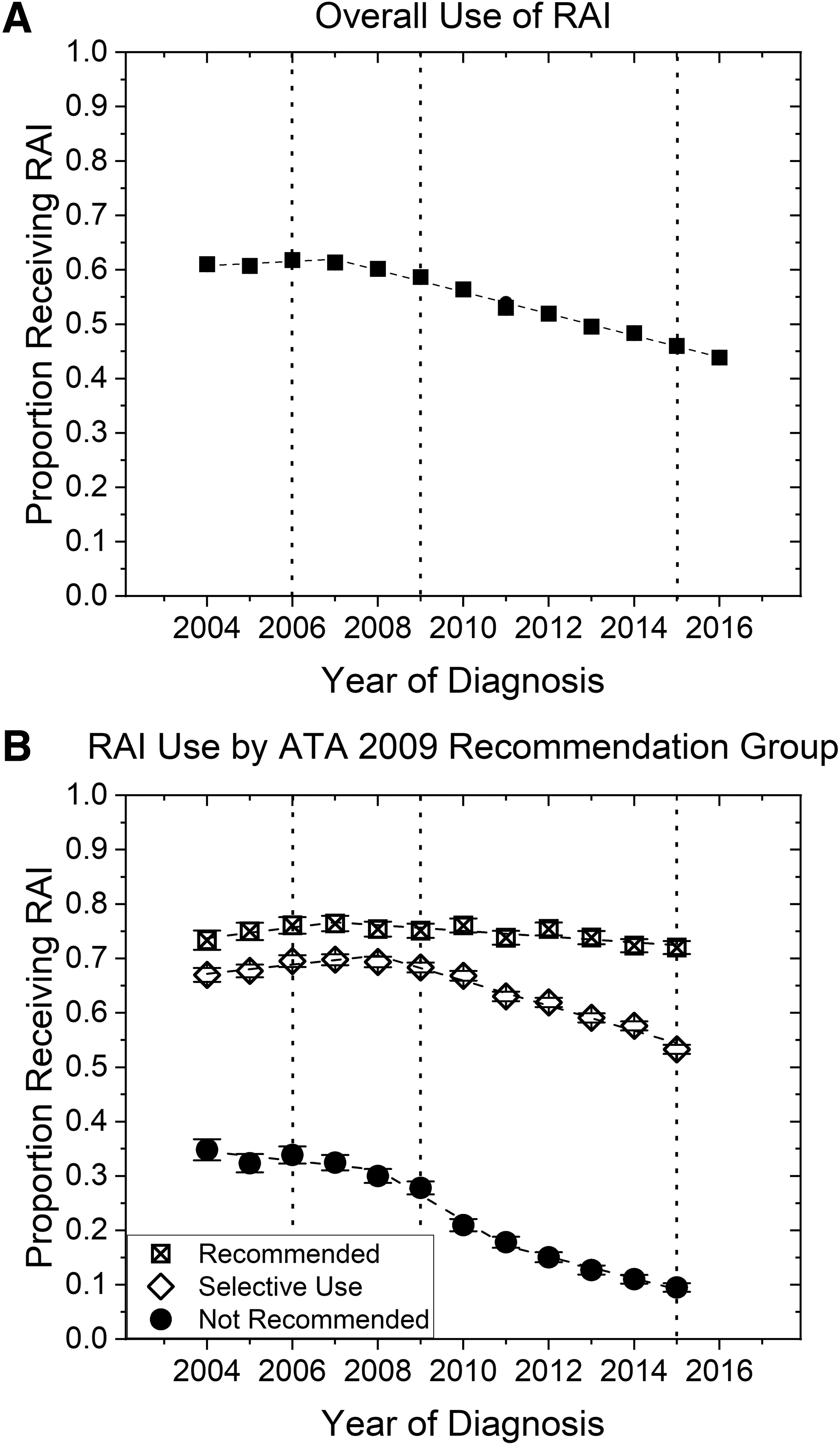
Temporal trends in the utilization of RAI (
Applying the 2009 ATA guidelines for RAI therapy, it was determined that in 2015, RAI therapy was administered to 72.0%, 53.3%, and 9.5% of patients for whom RAI was recommended, selectively recommended, and not recommended, respectively (Fig. 2B). In the recommended group, there has been a statistically significant decline (p = 0.020) in the use of RAI since 2007 (CI: 2007 to 2012) at a rate of −0.53% (CI: −0.79 to −0.27) of patients per year. In the selectively recommended group, there has been a statistically significant decline (p < 0.001) in RAI utilization since 2008 (CI: 2007 to 2010) at a rate of −2.3% (CI: −2.6 to −2.0) of patients per year. Finally, in the not recommended group, there were two statistically significant joinpoints (p = 0.002): one in 2008 (CI: 2007 to 2009) and a second in 2011 (CI: 2010 to 2012). From 2008 through 2010, RAI use declined at a rate of −4.7% (CI: −6.4 to −2.9) of patients per year, and from 2011 through 2015, RAI use declined at a rate of −2.0% (CI: −2.4 to −1.6) of patients per year. The relative percentage of patients in each group has remained approximately constant from 2004 to 2015 (data not shown).
We performed post hoc analyses to analyze trends in prescribing rates by hospital reporting volume and geographic location (Supplementary Fig. S1). In high-volume institutions (>75th percentile), RAI utilization rates decreased 6.0% and 9.0% more than rates at low-volume institutions (≤25th percentile) in patients for whom RAI was not recommended or selectively recommended, respectively (Supplementary Fig. S1A, B). There has been no net change in RAI utilization from 2004 to 2016 in patients for whom RAI was recommended between low- and high-volume institutions (Supplementary Fig. S1C). In terms of geographic differences, institutions on the east coast routinely prescribed RAI at lower rates than those in other areas of the country, regardless of the recommendation group (Supplementary Fig. S1D–F). Finally, to explain the decline in RAI utilization in patients for whom RAI was recommended based on 2009 guidelines, we stratified RAI utilization by indication for RAI (Supplementary Fig. S2). Only patients with positive surgical margins saw a statistically significant decrease in RAI utilization (−0.75% per year, CI: −1.0 to −0.49) since the joinpoint in 2007.
Individual hospitals prescribe RAI at different rates
We next assessed changes in prescribing habits over time based on the prescribing patterns of individual hospitals. To do so, we estimated the average probability for each hospital to provide RAI therapy to its patients after adjusting for patient-specific effects and hospital-specific effects, including a marker of individual institutional preference using “random” variables. In accordance with the overall trend in RAI utilization (Fig. 2A), we found that in 2006, the median hospital prescribed RAI to 60.7% of patients, while in 2016, the median hospital prescribed RAI to 43.9% of patients (Fig. 3A). We further quantitated the change in RAI prescribing habits by comparing the distributions of the estimated probabilities (Fig. 3A, B). By 2016, 79% of hospitals administered RAI at or below the rate of the median hospital in 2006, and that the median hospital in 2016 prescribed RAI at the rate of the hospital in the 25th percentile in 2006. Finally, in a marker of between-hospital variability, the interquartile range reduced in range from 0.30 in 2006 to 0.26 in 2016.
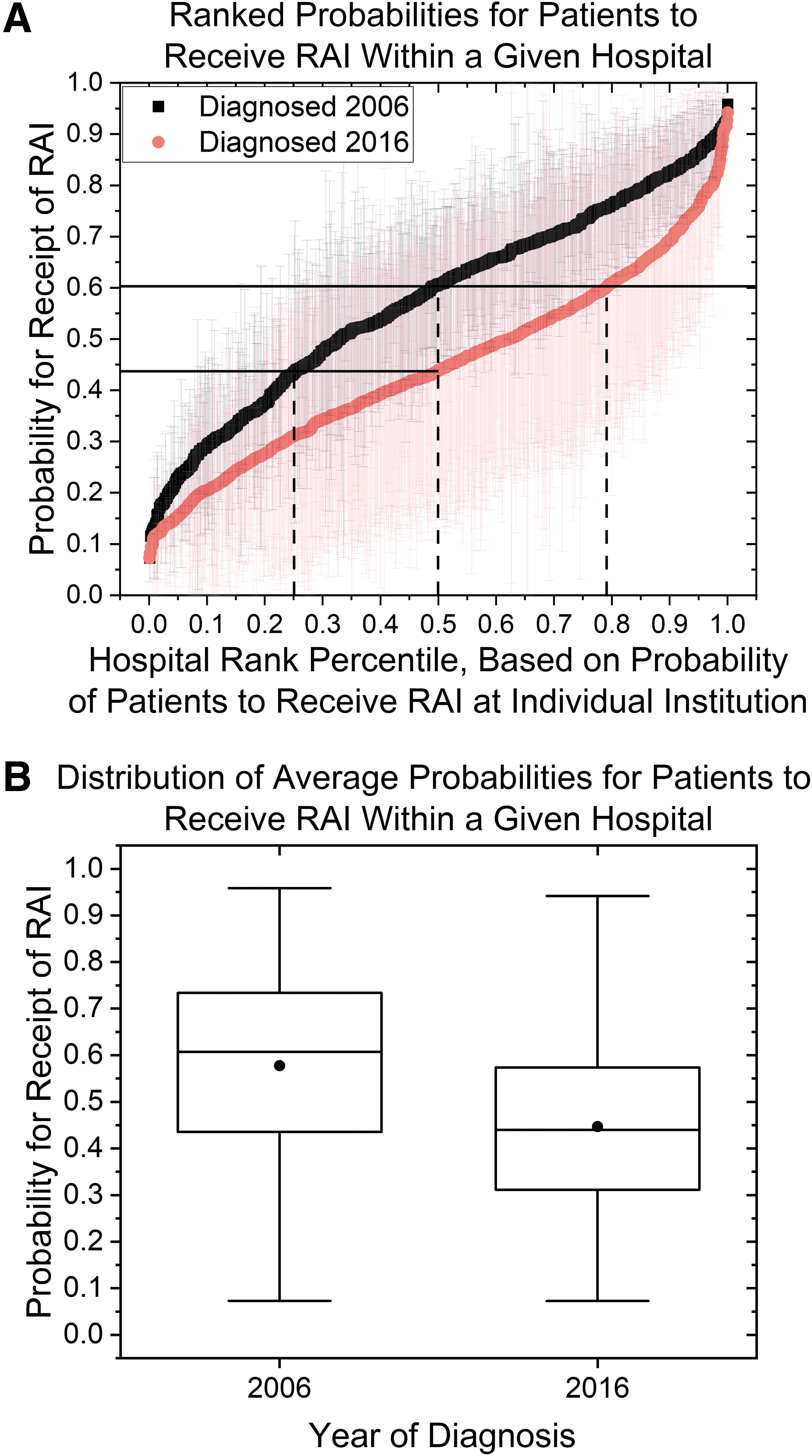
Assessment of probability for patients to receive RAI. (
There is less variability in RAI prescribing habits across hospitals over time
The above analysis could not distinguish between whether RAI was being prescribed more or less commonly in a given hospital due to patient-specific factors, such as the example of a tertiary care hospital that only treats advanced disease, or due to institutional culture. Therefore, a function, ΔP, was derived to approximate the percent more or less likely for each hospital to prescribe RAI than would be expected based on the type of patient seen at that type of hospital. When comparing the distributions of ΔP from 2004 to 2016 (Fig. 4), we saw that variance of each distribution (i.e., variation in prescribing habits across hospitals) got smaller over time. This approximate halving in variance from 0.0231 to 0.0115 between 2004 and 2016, respectively, (Fig. 4B) was statistically significant (Levene's test p < 0.001). On piecewise linear fitting, the variance of ΔP started to decline in 2012 (CI: 2010 to 2014) by a magnitude −0.0017 per year (CI: −0.0024 to −0.00089).
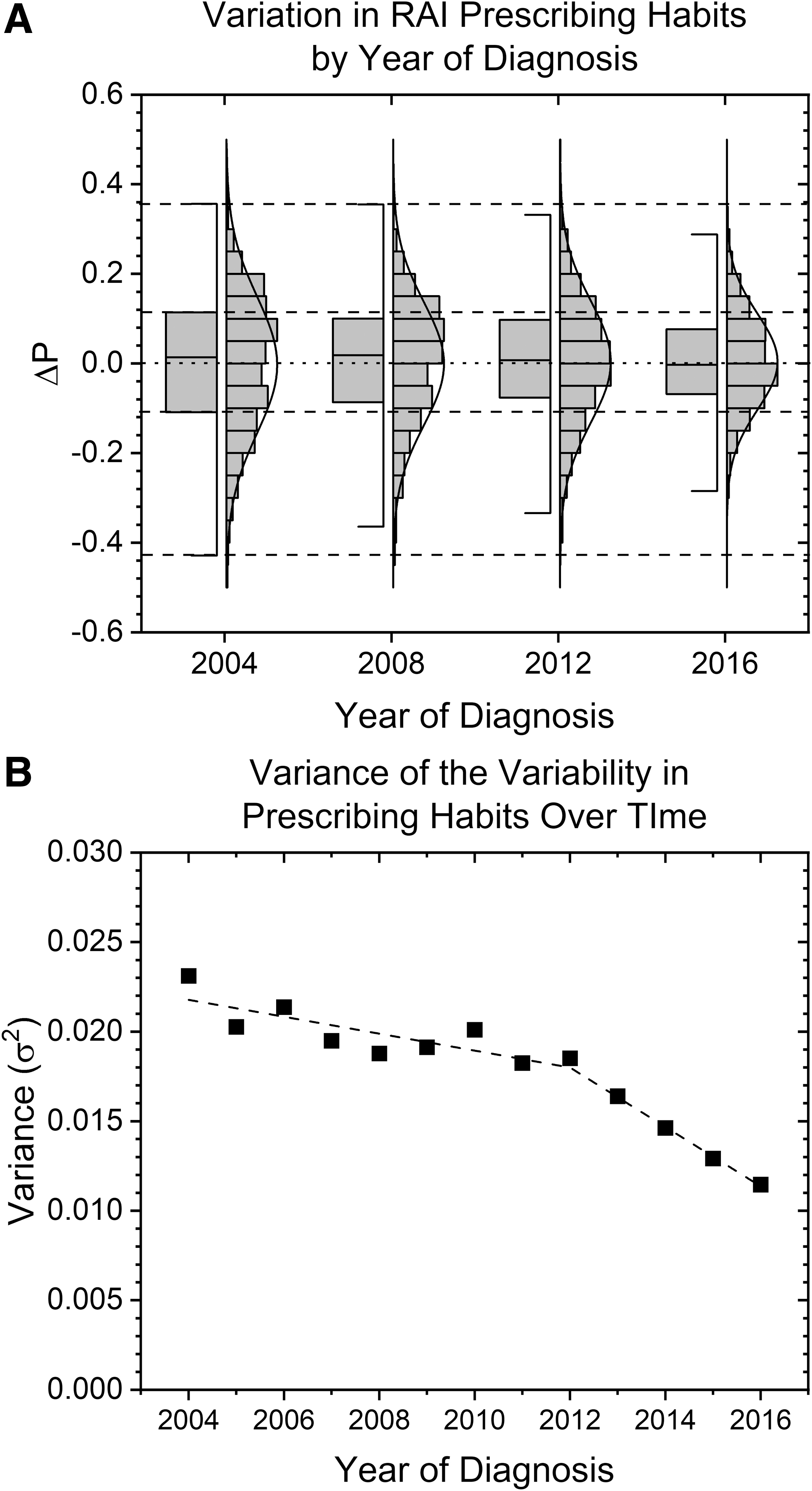
Assessment of variation in RAI prescribing patterns over time across hospitals. ΔP is the estimated effect of an individual institution's preferences on prescribing RAI above (ΔP > 0) or below (ΔP < 0) expected based on the characteristics of the patients it evaluates. (
Discussion
RAI for PTC after total thyroidectomy has potential benefits for the majority of patients, but it may cause unnecessary morbidity in patients for whom it has no evidence to reduce recurrence or mortality. To reduce overprescription, clinical research and guidelines have been published to help identify who should receive RAI therapy. An unstated aim of these reports includes the goal of reducing variability in prescribing habits across institutions by encouraging evidence-based prescribing and reducing prescribing based on provider or institutional opinions. In this study, we show that there has been a large decline in RAI utilization in patients with small (<1 cm), nonmetastatic (lymph node and distant), intrathyroidal disease since ∼2009, while utilization in those with more advanced or concerning disease has remained high and has seen a minimal decline in utilization.
Although there is a temporal association between the decline in RAI utilization and a shift in guidelines, we cannot definitively say that the change in guidelines was the sole or primary driver of decreased use of RAI ablation. It is possible that the same mounting evidence that led the ATA to modify its guidelines is what actually drove some or most physicians to change their behavior, with the guidelines themselves playing a less important role. However, whether from guidelines or primary literature, conclusions from these works appear to have impacted care and prescribing patterns in a clinically meaningful way that deserves acknowledgment, reinforcement, and research.
As noted above, RAI ablation has been linked to patient morbidity, including sialadenitis, xerostomia, dental caries, mouth pain, pulmonary fibrosis, nasolacrimal outflow obstruction, and second primary malignancy (23). Therefore, the decrease in RAI ablation in patients with the lowest risk forms of PTC may be viewed as a success. However, despite the dramatic decline in RAI use, in 2015 nearly 10% of patients for whom RAI was not recommended did still receive RAI.
Existing literature on guideline nonadherence suggests several possible reasons for why RAI ablation continues to be used in some low-risk PTC patients. These include lack of guideline awareness, lack of familiarity (i.e., a physician is aware that guidelines exist but not well-versed in the specific recommendations), lack of agreement with the guidelines, and inertia of previous clinical practice (24). In particular, lack of agreement may be at play in this case, as evidence for the guidelines is based on retrospective observational analysis and expert opinion with no prospective randomized studies to inform clinical practice. It has been noted that greater variation in care may exist when guidelines are based on expert opinion rather than stronger forms of evidence (25,26). Notably, there are ongoing prospective studies that may begin reporting results as soon as 2020 (27).
We also show that variation in prescribing habits across hospitals has decreased since 2004, with a statistically significant decline starting in 2012. This decrease in variation appears slightly delayed to the decline in the actual proportion of patients receiving RAI in 2007. This indicates that, even though, on average, hospitals reduced their administration of RAI, they continued to under- or overprescribe therapy to the same degree until ∼2012. Only after 2012 did they prescribe closer to what would be expected based on the patients they evaluate. Such a finding potentially suggests that widespread adoption of new evidence and guidelines across hospitals lagged several years behind their availability, with a significant effect on aggregate levels of RAI prescribing occurring sooner.
Although practice patterns and variation in utilization of RAI after total thyroidectomy between institutions have declined over time, variation in prescribing habits remains. This finding, as noted above, may be due to the current lack of evidence from prospective randomized clinical trials. Furthermore, the guidelines do not have a definitive recommendation for a sizeable segment of patients (those in whom “selective use” is recommended), which may lead to greater variability than if all patients fell into a “recommended” or “not recommended” category.
While we show significant but decreasing variability in practice patterns between institutions, we are unable to comment on the extent of intrainstitutional variation, as physicians within a single hospital may have different standard practices for RAI therapy. We also acknowledge that rural institutions and institutions that do not offer comprehensive oncology-related services are underrepresented in the NCDB due to lack of Commission on Cancer certification (28). This study also has several limitations associated with the use of large national data sets. Most importantly, the database lacks specific clinical patient information aside from the comorbidity index, preventing the identification of patients who may have received RAI due to high thyroglobulin (Tg) levels after surgery. This would be an important covariate to consider, since NCCN guidelines recommend RAI therapy for an unstimulated Tg >1 ng/mL (5). Similarly, we were unable to assess outcomes related to morbidity associated with RAI therapy, such as xerostomia incidence, patient quality-of-life measures, or disease recurrence. Radiation therapy in the NCDB is limited to a patient's initial course of therapy, so patients receiving RAI for the development of metastases after initial therapy were not analyzed. Furthermore, given the termination of CS coding after 2015, we decided to prioritize more accurate coding for recommendation groupings at the expense of not including data for patients diagnosed in 2016. We believe that loss of information coded in CS may negatively impact future research and advocate for continued high-quality, detailed coding within the NCDB and other databases. Finally, given that the ATA 2015 guidelines were released toward the end of 2015, and published in 2016, we are careful to not draw conclusions regarding the potential impact of these guideline revisions on RAI utilization.
However, there are limited differences between the 2009 and 2015 guidelines regarding which patients should receive RAI, so the results presented in this study remain clinically meaningful. More specifically, the 2015 ATA guidelines characterize low-volume nodal metastases, defined as ≤5 lymph nodes that are all <0.2 cm, as low-risk disease in the absence of other risk factors. Therefore, these patients may forgo RAI therapy. However, if patients with low-volume nodal metastases do receive RAI therapy, lower dosages of RAI are recommended (11,12). On the contrary, patients with N1 disease with any lymph nodes ≥3 cm are considered high risk for recurrence (11,12). All other nodal involvements on clinical or pathologic examination remain intermediate risk. Finally, patients with multifocal microcarcinoma with extrathyroidal extension and BRAFV600E mutation are considered intermediate risk for recurrence (11).
Despite the limitations associated with the NCDB, this study has the potential to inform system-level, institution-level, and provider-level care. Knowledge of average national prescribing patterns sets benchmarks by which hospitals and providers can assess their individual prescribing patterns. In the field of implementation science, which studies the successes and failures of the adoption of new practices, audit and feedback are a strategy utilized to increase adherence to policies (29,30). As such, our analysis may serve as a basis for hospitals and providers to accurately assess in what percentile of prescribing they fall based on the 2016 data. Furthermore, we use longer term data to substantiate previous claims that conclusions from both scientific literature and guidelines appear to have been adopted into clinical practice by RAI prescribers on the system level (19 –21). We further show that such guideline adoption was not transient. Such evidence suggests that literature may continue to change practice patterns and should continue to be developed. In the field of implementation science, both reinforcement and confidence that other providers are utilizing clinical care guidelines and knowledge that guidelines improve patient outcomes are motivators for guideline adoption (31). This study may provide motivation for continued and sustained change. Finally, on the provider level, providers may use knowledge of national prescribing practices to reassure patients with low-risk disease that RAI is rarely received by similar patients. Similarly, it may help motivate skeptical patients with intermediate- and high-risk disease to receive RAI after seeing that most patients receive such therapy.
In conclusion, we show that changes in evidence and guidelines regarding patient selection for RAI therapy have coincided with decreases in the proportion of patients receiving RAI. Moreover, the probability that a patient receives RAI is less dependent on hospital selection.
Footnotes
Acknowledgments
The data used in the study are derived from a deidentified NCDB file. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology used, or the conclusions drawn from these data by the investigator. This publication was made possible by the William U. Gardner Memorial Student Research Fellowship and the James G. Hirsch Endowed Medical Student Research Fellowship at the Yale University School of Medicine.
Author Disclosure Statement
D.J. was supported by the William U. Gardner Memorial Student Research Fellowship at the Yale University School of Medicine. C.T.B. was supported by the James G. Hirsch Endowed Medical Student Research Fellowship at the Yale University School of Medicine. All other authors have no disclosures.
Funding Information
This publication was made possible by the William U. Gardner Memorial Student Research Fellowship and the James G. Hirsch Endowed Medical Student Research Fellowship at Yale University School of Medicine.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2