
Abstract
Background:
Rituximab (RTX), a chimeric human-murine anti-CD20 monoclonal antibody, has been used for treatment of active moderate-severe Graves' orbitopathy (GO) since 2004 as second-line therapy in patients unresponsive to intravenous steroids. We conducted an open-label prospective study (EUDRACT 2012-001980-53) in which patients were treated with a single infusion of only 100 mg RTX to analyze the efficacy and safety of this low dose.
Methods:
Seventeen patients, of whom nine had disease that was unresponsive to intravenous methylprednisolone and eight with newly diagnosed GO, were enrolled. Disease activity was assessed with the clinical activity score (CAS) and severity with a composite ophthalmic score. Long-term surgical treatment and quality of life were also assessed, as well as treatment-related adverse events.
Results:
Mean baseline CAS was 4.56 ± 0.96 and decreased to 1.25 ± 1.14 at 24 weeks (p = 0.001). Disease inactivation occurred within 24 weeks in >90% of patients and was unrelated to disease duration. Severity improved in about 60% of patients, with no relapses. All patients showed peripheral depletion of CD20+ and CD19+ cells at the end of RTX infusion (60 minutes). Two patients required surgical orbital decompression because of optic neuropathy (ON). Among adverse events observed, there was one patient who developed a cytokine release syndrome.
Conclusions:
A dose of 100 mg RTX is effective in patients with active moderate-severe GO. Low doses are better tolerated, expose patients to immune suppression for a shorter period of time, and are extremely cost effective, compared with higher doses. This dose, consistently with all other immunosuppressants, does not prevent the progression of GO to dysthyroid ON.
Introduction
Graves'
RTX has been approved for the treatment of several autoimmune diseases over the last few years, such as rheumatoid arthritis and ANCA-related vasculitis (4). In GO, RTX has been shown to inactivate disease and to significantly modify its natural course, as suggested by the lack of disease reactivation shown in patients after treatment (5).
The dose of RTX initially used in the treatment of active moderate-severe GO was based on previous work in autoimmunity (6) and consisted of 1000 mg twice at a two-week interval (3,7,8). Due to the observation that in GO, total peripheral (and orbital) B cell depletion was occurring even after low doses of RTX (100 mg) (9), we have been effectively reducing the therapeutic dose to a single infusion of 500 mg RTX. This approach is justified by the results of a dose-finding analysis in a randomized trial comparing RTX with intravenous steroids (5) showing that 500 mg of RTX induces inactivation of GO as effectively as 2 × 1000 mg.
The advantages of using lower RTX doses are to expose patients to lower risks of potentially severe side effects (10 –12), and to limit the cost (€ 300–600 per patient) of the treatment, currently prescribed off label.
This open-label prospective study was designed to analyze the efficacy, in terms of disease inactivation and improvement of severity, of a single 100 mg RTX dose in a group of consecutive patients with active moderate-severe GO of different durations. The main objective of this study was to assess the cumulative evidence of the therapeutic benefit of RTX in GO versus the adverse events and safety implications.
Patients and Methods
Patients
Seventeen consecutive patients with active moderate-severe GO, 14 with GD, and 3 with Hashimoto's thyroiditis (HT), 14 women and 3 men, aged 28–72 years (mean ± standard deviation [SD], 51.5 ± 11.6) were recruited between 2012 and 2015 and treated with one single 100 mg dose of RTX. One woman with GD and active GO, treated according to the protocol, interrupted the infusion of RTX after only 25 mg, because of the onset of a rapid infusion reaction due to cytokine release (described below in detail).
The duration of active disease (de novo or reactivated after previous immunosuppressive treatment discontinued for at least 3 months) ranged between 0.8 and 10.4 months (mean ± SD, 4.2 ± 3.3). At the time of RTX therapy, 13 patients were euthyroid on methimazole treatment, one was untreated because of GD remission, patient was euthyroid one year after radioiodine therapy, one had euthyroid HT, while three patients were hypothyroid on L-thyroxine, of whom one after total thyroidectomy. The clinical characteristics of the patients are summarized in Table 1.
Clinical, Biochemical, and Immunological Characteristics of Patients at Baseline
All values are expressed as mean ± SD.
CAS, clinical activity score; fT3, free triiodothyronine; fT4, free thyroxine; n.v., normal values; OD, oculus dester (right eye); OS, oculus sinister (left eye); SD, standard deviation; TRAb, TSH receptor antibodies; TSH, thyrotropin.
Patients were seen in a joint thyroid and eye clinic (Graves' Orbitopathy Center, Endocrinology, Milan) and at each visit, blood was taken for thyroid function tests, serum autoantibody testing, and peripheral blood lymphocyte count. Twelve of 17 patients received previous steroid treatment, while five received RTX as first-line therapy. Patients were assessed at baseline and at 4, 8, 12, 16, 24, 32, 40, and 76 weeks after treatment. The ophthalmological examination included lid fissure and Hertel measurement, color vision, cover test, Hess-Lancaster screen, visual acuity, tonometry, fundus examination, and visual field. Disease activity was graded with the clinical activity score (CAS) (13). All patients had active GO as assessed by a baseline CAS ≥3/7 or >4/10 points, at subsequent examinations. Orbital computed tomography (CT) scan was performed only in patients who required the study of the optic nerve in suspected optic neuropathy.
Therapeutic protocol
Patients received RTX (MabThera; Hoffmann La Roche, Basel, Switzerland), according to the protocol, as a single dose of 100 mg infused over ∼1 hour and 15 minutes. One hour before RTX infusion, oral paracetamol (1 g), chlorphenamine (10 mg), and i.v. hydrocortisone (100 mg) were administered to prevent possible allergic reactions.
Contraindications to RTX therapy were pregnancy, breastfeeding, diabetes, known coronary artery disease, significant cardiac arrhythmias, severe congestive heart failure, serious chronic illness, active infection, a history of recurrent infection or recurrent bacterial infections, history of sarcoidosis, primary or secondary immunodeficiency, history of hypersensitivity, known anaphylaxis to mouse-derived proteins, positive purified protein derivative without documentation of treatment for TB infection, a history of cancer excluding resected basal or major squamous cell carcinoma, cervical dysplasia or in situ cervical cancer, denied consent to HIV testing, and allergy to paracetamol, chlorphenamine, and hydrocortisone (used for premedication).
The study protocol was registered (EUDRACT 2012-001980-53) and approved by the Ethics Committee of the Fondazione IRCCS Cà Granda of Milan. GORTX-2012, approved May 25, 2012. EU clinical trial registration details and documents are provided as Supplementary Data. All patients provided informed consent for participation in the trial.
Biochemical and immunological testing
Serum thyrotropin (TSH), free thyroxine, and free triiodothyronine concentrations and antithyroglobulin (TgAb) and antithyroperoxidase antibody (TPOAb) levels were measured using the AutoDELFIA™ technique (Perkin Elmer™-Life Sciences, Wallac Oy, Turku, Finland). Serum TSH receptor antibodies (TRAb), detected as TSH binding inhibitory immunoglobulins, were measured using a third-generation TRAK test (BRAHMS TRAK human KRYPTOR; Thermo Fisher Scientific, Germany).
Cytofluorimetric analysis
We studied the pattern of peripheral blood lymphocytes before RTX and throughout the study period. We analyzed the standard immunophenotypic panel (CD3+, CD3+4+, CD3+8+, CD3+DR+, CD20+, CD19+5+, CD56+16+3) on aliquots of around 105 lymphocytes, submitted to standard triple staining procedures to carry out immunogating with CD45, and the pairs of monoclonal antibodies to subpopulations of T, B, and natural killer cells, subsequently processed in the flow cytometer (BD FACScan, Cell-quest software).
Analysis of the therapeutic response
The changes of activity and severity parameters after RTX were studied by assessing (i) the decrease of the CAS ≥2 points compared with baseline (mourits); (ii) the prevalence and time of disease inactivation (number of patients with CAS <3); and (iii) the disease improvement at 24 weeks, by calculating a composite ophthalmic score (proposed by the EUGOGO guidelines) (2). Improvement was considered with a change in two or more of the following parameters, without deterioration of any of those in any of the eyes: (i) decrease of palpebral aperture of ≥3 mm; (ii) improvement in NOSPECS (No symptoms, Only signs, Soft tissue involvement, Proptosis, Extraocular muscle involvement, Corneal involvement, Sight loss) class 2 signs by ≥2 grades; (iii) decrease of one grade in the Bahn–Gorman diplopia score or improvement of ≥8° in ductions; (iv) reduction of proptosis of ≥2 mm; and (v) a decrease of the CAS of ≥2 points.
Disease deterioration was assessed as the development of dysthyroid optic neuropathy (DON) or occurrence of two of the following: (i) increase in palpebral aperture by at least 3 mm; (ii) increase of any of the class 2 signs of NOSPECS by at least two grades; (iii) increase of proptosis by at least 2 mm; (iv) decrease of ≥8° in motility or worsening of the diplopia score; and (v) deterioration of the CAS. If changes were of a smaller magnitude than these parameters, the therapeutic outcome was considered “no change.”
Quality of life
The therapeutic outcome was also assessed by administering the disease-specific quality-of-life (GO-QoL) questionnaire (14), for both patient's appearance and function at 24 weeks.
Assessment of adverse events
Treatment-related side effects were recorded and assessed as serious and minor events during therapy and in the follow-up period. Side effects were classified as major (cytokine release syndrome, occurrence of major depression, severe infections) and minor (urticaria, allergic reactions—nose itching, sore-throat-fever, flushing, myalgia, asthenia, nausea). Side effects occurring during the infusions were usually controlled and monitored by the endocrinologist and did not influence the ophthalmological picture. The development of cytokine release syndrome, previously reported in GO patients treated with RTX, was considered a serious adverse event. Disease progression to DON was not recorded as a side effect, but as ineffective treatment.
Statistical analysis
Sociodemographic and clinical continuous variables are expressed as means ± SDs and categorical data as frequencies and proportions. An analysis of covariance model for repeated measures was fitted to evaluate the trend of CAS values during the follow-up. To take into account the correlation among measurements on the same subject in different times, a variance-covariance matrix with Toeplitz structure was considered. A statistical significance of a trend was evaluated by the p-value of the variable time included in the model. Other covariates considered in the model were as follows: age, sex, and disease duration. A nonparametric analysis of interval-censored data was carried out to estimate the cumulative proportion (and relative 95% confidence interval [CI]) of the composite dichotomous endpoint. Patients undergoing surgical orbital decompression during the observation period, up to 24 weeks, were not included in the analysis of the disease outcomes.
Results
Analysis of efficacy on disease activity and severity
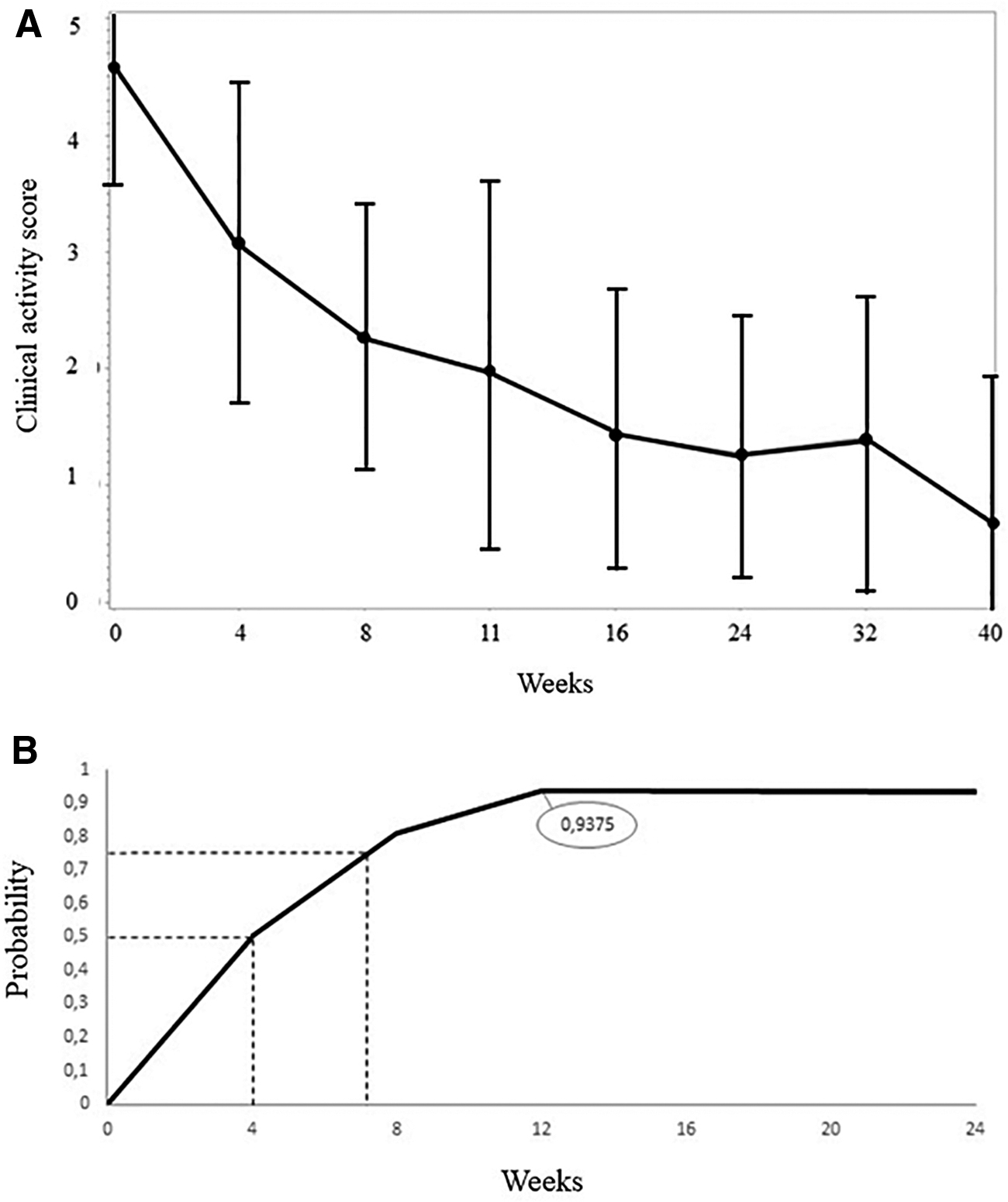
Disease activity was assessed in all patients as a CAS of at least 4 points out of 10. Mean baseline CAS was 4.56 ± 0.96 and decreased to 2.0 ± 1.57 at 12 weeks (p = 0.001), to 1.46 ± 1.2 at 16 weeks (p = 0.001), to 1.25 ± 1.14 at 24 weeks (p = 0.001), and to 1.4 ± 1.26 at 32 weeks (p = 0.001) (Fig. 1A). At 12 weeks, 13 of 15 patients had inactive GO (CAS <3) (86.6%), 1 patient had a decrease of CAS from 7 to 5, and one worsened with an increase of CAS from 4 to 5. We excluded one patient with unilateral GO who rapidly responded to RTX (4 weeks) and decided to undergo surgical orbital decompression before 12 weeks, for cosmetic reasons. The probability of cumulative inactivation rate after RTX was more than 50% after four weeks and increased to 93.8% (15 of 16 patients [CI 63.2–99.1%]) at week 12 without changes until week 40, as shown in Figure 1B. At 24 weeks, all patients were inactive. None of the patients showed GO relapses at 52 and 76 weeks of follow-up.
To study whether the duration of the disease might influence the therapeutic response to RTX, we analyzed disease inactivation in relation to the onset of active GO. Patients were divided into two groups based on the mean duration, which was 4.2 ± 3.3 months (range 0.5–10.3 months). Patients with a longer disease duration responded to RTX as well as those with a short duration, and in fact after week 4, the responses of the former group were overall better (p < 0.0001) (Fig. 2).
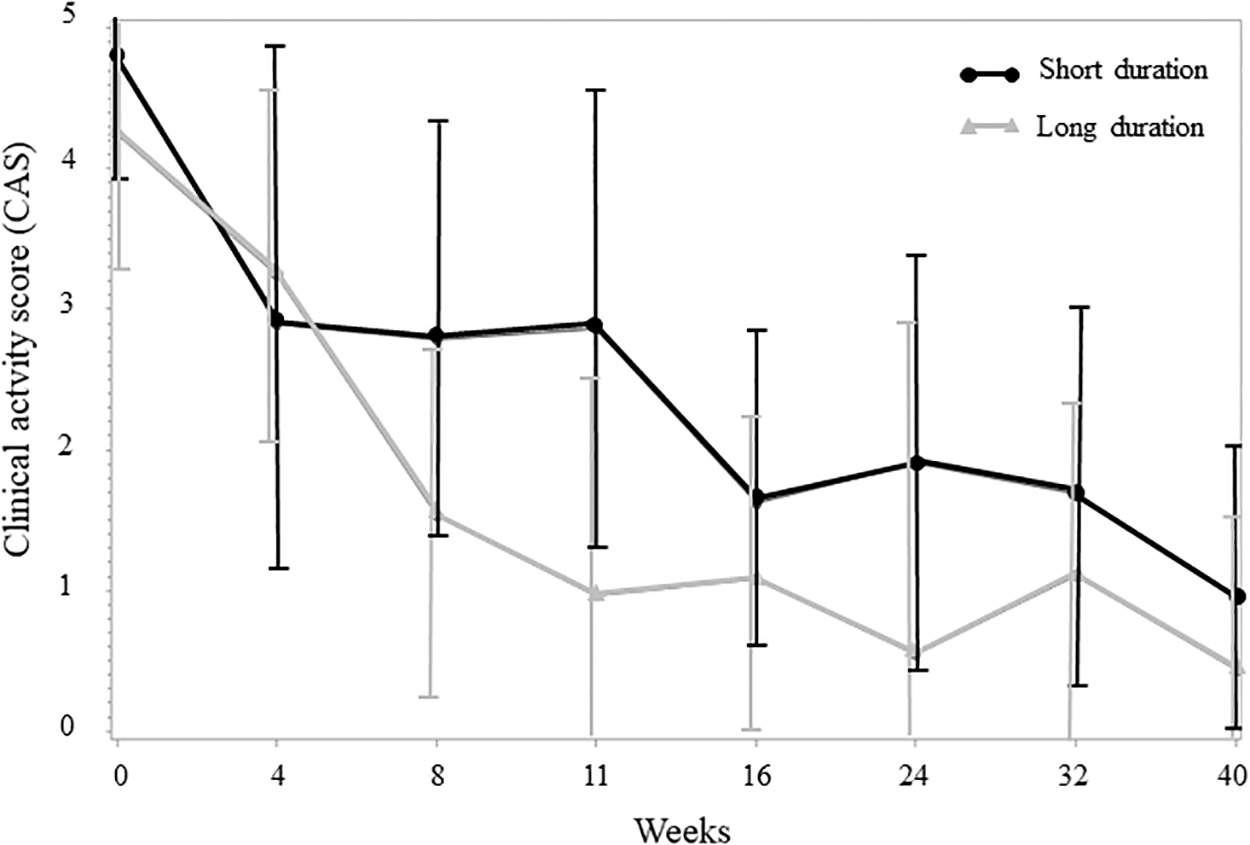
Decrease of the CAS in patients treated with a single 100 mg of RTX in relation to the duration of Graves' orbitopathy assessed as less or more than the median duration in months (4.2 ± 3.3; range 0.5–10.3 months).
At 24 weeks, severity improvement, assessed by the composite ophthalmic score, was observed in 7 of 12 patients (58.3%). In three patients, GO remained stable and in two worsened (lid fissure and proptosis, proptosis and CAS, respectively). Between 12 and 24 weeks from RTX treatment, two patients developed DON, possibly present in a subclinical form and not fully recognized at baseline examination, as frequently occurs in GO. Another patient with inactive disease underwent elective surgical orbital decompression for marked unilateral proptosis (Fig. 3).
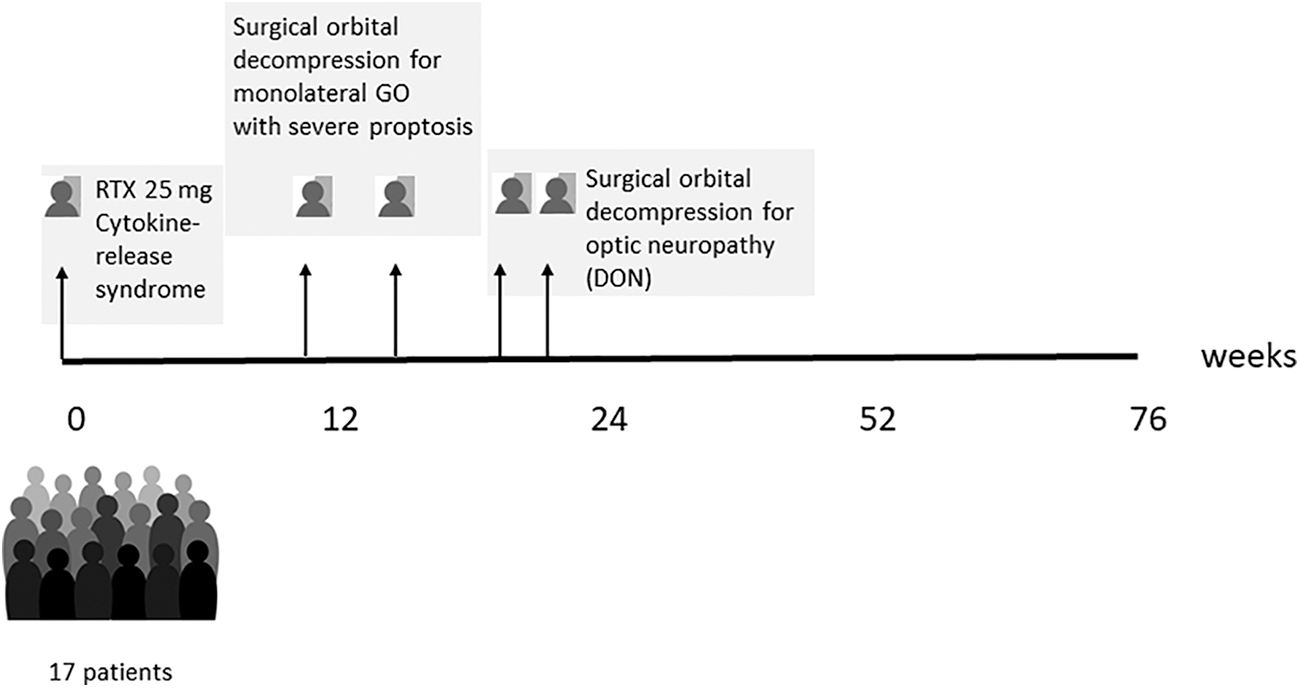
Flowchart diagram of patients included in the study. In detail, one patient only received 25 mg, two patients underwent early surgical orbital decompression (12–16 weeks) for monolateral marked proptosis, and two patients underwent surgical orbital DON between 12 and 24 weeks of follow-up. DON, decompression for optic neuropathy; GO, Graves' orbitopathy.
The degree of residual disease was studied at 76 weeks. Six patients did not require further treatments; five patients underwent elective surgical decompression. Seven and two patients underwent squint surgery and eye lid correction, respectively (Fig. 3).
The GO-QoL questionnaire was completed by 14 patients. At 24 weeks, the appearance score improved in eight patients, stabilized in two, and worsened in four. The function score improved in seven patients, stabilized in four, and worsened in three. The QoL appearance scale score was >50% in 11 patients at baseline and in 13 patients at both 12 and 24 weeks, while the QoL function score was >50% in 9 patients at baseline, in 10 at 12 weeks, and in 8 at 24 weeks.
B cell depletion after treatment
All patients showed peripheral depletion of CD20+ and CD19+ cells at the end of RTX infusion (60 minutes). B cells began repopulating after 4 to 12 weeks, and at 40 and 76 weeks of follow-up, we observed peripheral B cell return of nearly 53% and 70% (data not shown), respectively, compared with baseline. The CAS continued to decrease independently of B cell repopulation.
Effect on serum TSH-receptor antibodies
We measured serum TRAb levels at each follow-up visit in all patients and we observed a progressive decrease of the antibodies at 12 weeks (p = 0.14), reaching significance only at 24 weeks (p = 0.015) (not shown).
Side effects
The treatment was well tolerated by the majority of patients. Minor side effects, such as sore-throat and nose itching usually associated with the infusion of higher dose RTX, were not seen with a dose of 100 mg in this series of patients. One woman reported mild urticaria. which resolved with low-dose steroids.
A 69-year-old woman with contraindications to intravenous methylprednisolone therapy, due to previous steroid-induced pyelonephritis and subsequent nephrectomy, after administering 25 mg of RTX showed rapidly progressive edema accompanied by orbital pain and decrease of vision in OD (5/10). She had active GO in OD, with chemosis, edema, plica, and significant worsening of proptosis, with a CAS of 4/10 and inactive GO in OS. RTX was immediately withdrawn and 100 mg of hydrocortisone was administered.
Orbital pain improved over the next 15 minutes and visual acuity completely recovered in one hour without further treatment. Orbital CT imaging, carried out during amaurosis, ruled out optic nerve compression. A week later, GO was inactive (CAS 3/10) and her vision was back to normal (10/10). The patient's inflammatory signs and symptoms eventually resolved (CAS 0/10) with only residual proptosis and intermittent diplopia. Peripheral depletion of CD20+ and CD19+ cells was detected at 30 minutes, after 25 mg RTX (Fig. 4). The patient's quality of life showed significant improvement (57%) of the functioning scale compared with baseline, with resumption of daily activities.
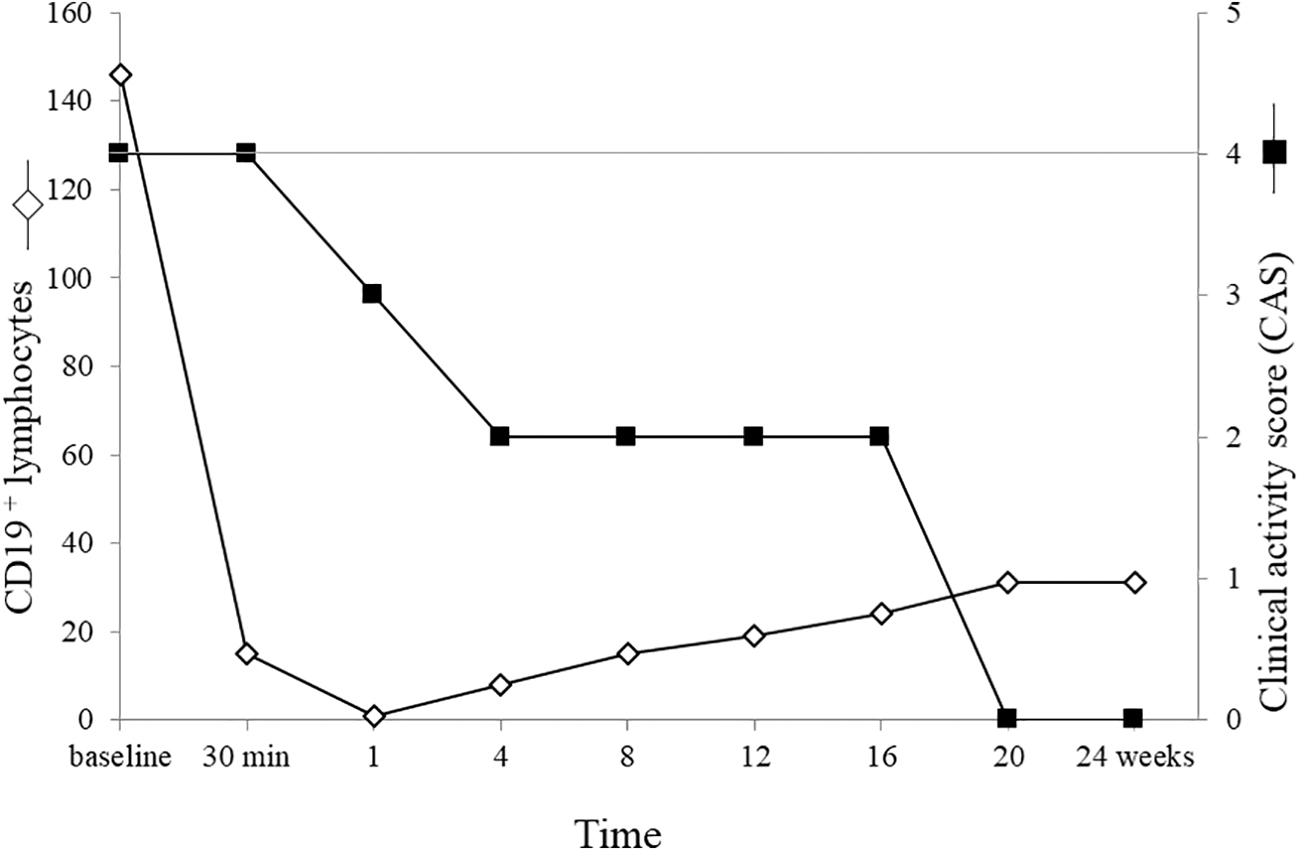
Total CD19 depletion at 30 minutes after the infusion of 25 mg RTX in one patient developing a moderate syndrome of cytokine release and the subsequent decrease of the CAS without further therapeutic intervention. B cells begin repopulation around four weeks.
Discussion
The first and most important finding of this study is that a very low dose of RTX induces total peripheral B cell depletion and is rapidly effective for the treatment of active moderate-severe GO. Based on these results, we have evidence that an RTX dose (100 mg) even 20-fold lower than that commonly used in other autoimmune disease may be used as a therapeutic option for GO (9), when first-line therapy fails (2). This study was designed to be open label and prospective, with the aim to analyze the pattern of response and the profile of efficacy of RTX in relation to safety. The use of low-dose RTX in GO may reduce the impact of generalized immunosuppression and protect the patients from the risks that may derive from prolonged B cell depletion (11).
One important observation, derived from comparison with higher RTX doses (1000 or 500 mg), is that even at this low dose, RTX inactivated GO very rapidly, within 12 weeks in 94% of patients, as shown by the analysis of cumulative rate of inactivation. In a recent retrospective study, Du Pasquier-Fediaevsky et al. (15) described similar results in patients with GO unresponsive to or relapsed after steroid treatment or external radiotherapy. They reported a success rate of 87% with no relapses at eight weeks, although all but two patients received at least two doses of 100 mg of RTX. They did not observe differences in the efficacy of RTX in relation to the cumulative dose administered, but did not analyze the response in relation to the duration of GO.
As we learned from the outcome of two randomized control trials of RTX in GO, the duration of the disease is likely a crucial factor that influences its effectiveness and the clinical response (16). For this reason, in the present series, we analyzed response in relation to GO duration and found that patients with longer duration had a more consistent decrease of the CAS than those with shorter duration. There may be several explanations for this unexpected finding: (i) all patients in our study had a relatively short duration of the eye disease (<10 months); (ii) based on the dyphasic course of GO (Rundle curve), RTX treatment might accelerate the transition from the dynamic to the stable phase of the disease, especially in patients whose progression is close to the apex of the curve (17). Although unlikely, we cannot rule out also that GO became inactive due to the natural course of disease.
While the overall improvement of severity parameters was observed in about 60% of patients, none of the responders had relapse of GO at the end of follow-up, suggesting that RTX may modify the natural course of disease. The lack of disease reactivation was observed despite that B cells repopulated earlier (4–12 weeks) when compared with higher RTX doses (20–32 weeks) (5). It is important to underscore that RTX was the only modality of treatment of all but two patients, who subsequently required surgical orbital decompression after developing DON. These data are consistent with recent results published by Karasek et al. (18) who treated 10 patients with a single dose of 100 mg RTX and reported DON in two patients.
Similarly to our observations, in their cohort, those two patients were steroid resistant and one with initial signs of DON at the time of treatment. Insull et al. (19) have used low-dose (100 mg) RTX in GO patients in association with low-dose steroids (mean dose 2.23 g) or other immunosuppressive agents with the objective of reducing the dose of systemic steroids and increasing the efficacy of therapy. They reported a 67% rate of disease inactivation and a 50% reduction of the severity score and no relapses at greater than six months. They also observed progression to DON in three patients. The efficacy of combined immunosuppressive therapy needs to be verified in a randomized-controlled trial. Furthermore, this approach might be accompanied by an increased risk of long-term adverse events, especially infections (20).
Progression of moderate-severe GO to DON has been reported in patients treated with any of the currently used immunosuppressive agents (21 –23). Consistent with previous trials of RTX with either high dose (16) or low dose (18,19), DON manifested also in two of the patients of the present study. Whether progression was due to unresponsiveness to RTX or to the presence of subclinical DON signs at the time of therapy is not clear, although by retrospectively reviewing these patients records we cannot rule out that they may have had suspected DON (18). These were the only two patients who required prompt additional treatment (decompressive surgery).
Rehabilitative surgery was required in about 50% of patients and in all of them was carried out within 76 weeks from initial treatment, as the lack of disease relapse observed after RTX was reassuring for earlier surgical intervention in these patients. The patients' quality of life, especially visual functioning, was positively affected by low-dose RTX, although the assessment of these parameters on a small series of patients may be of limited value. The observed decrease of serum TRAb levels may be due to a direct effect of RTX on TSH receptor stimulating antibodies in these patients (24,25) or indirectly as a consequence of attained remission of hyperthyroidism after antithyroid treatment (26). This was not investigated specifically in this study.
By using low-dose RTX, we did not observe the common mild infusion-related side effects described when using 1000 mg RTX (5). Unfortunately, dose reduction did not prevent the onset of the cytokine release syndrome that we observed in one patient after infusing as low as 25 mg RTX. For this reason, we suggest that this treatment should only be administered in specialized centers, where all the appropriate rescue measures can be undertaken. This syndrome is characterized by acute orbital edema and some degree of visual loss, which appear to be transient, followed by spontaneous recovery (9). A small dose of steroids has been used to control the acute event (27), but other drugs than steroids (i.e., tocilizumab) may be used for effectively treating the cytokine release syndrome (28). As shown by imaging, vision impairment was not caused by compression of the optic nerve at the orbital apex, suggesting a different mechanism.
Venous outflow is important in the pathophysiological processes occurring in the orbit, and congestion of the superior orbital vein plays a key role also in the inflammatory phase of GO, as demonstrated by CT and color Doppler imaging studies (29,30). The release of cytokines and the activation of the complement cascade after RTX may have caused transient impairment of the superior orbital vein flow, resulting in acute orbital vascular congestion, in marked edema of soft periorbital and intraorbital tissues (31), but only transient compressive effects on the optic nerve.
There are also some reports suggesting that RTX may induce arterial vasospasm, which may cause transient ischemia of the optic nerve and contribute to determine the visual symptoms. Acute coronary vasospasm has been reported as an infusion-related adverse effect of RTX (32) in a patient within 10 minutes from the first infusion, and retinal arteriolar spasm has been shown to cause transient monocular visual loss (33). The acute effect of RTX on the venous and arterial compartment may therefore explain the observed clinical picture, which is, however, transient and manageable in contrast with compressive DON, which requires urgent surgical orbital decompression.
The major limitation of this study is its uncontrolled design although, rather than comparing efficacy with standard steroid therapy for GO, the main objective was to analyze the timing of the therapeutic response to a small dose of RTX in relation to safety concerns in using this immunosuppressant. On the contrary, the study protocol was rigorous and gave us the opportunity to also treat a number of GO patients with a low dose of RTX as the only and first-line therapy, which proved to be effective.
In conclusion, the results of this study suggest that low-dose RTX is as effective as higher doses for the treatment for patients with active moderate-severe GO. Reduced RTX doses may be used in selected patients as first-line therapy instead of steroids. Besides being better tolerated, low-dose RTX exposes patients to B cell depletion and immune suppression for a shorter period of time, although we show in this study that 100 mg RTX, consistent with all other immunosuppressants, does not prevent the progression of GO to DON in predisposed patients. Another advantage for a single low-dose infusion of RTX is the reduction of hospital admissions and treatment costs, even if compared with standard intravenous steroid therapy. Currently the cost of 100 mg RTX is about € 350 per vial.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded by Fondazione IRCCS Cà Granda, Milan. (GORTX-2012; current research 2019).
Supplementary Material
Supplementary Data