
Abstract
Background:
There is a growing awareness that nutritional habits may influence risk of several inflammatory and immune-mediated disorders, including autoimmune diseases, through various mechanisms. The aim of the present study was to investigate dietary habits and their relationship with redox homeostasis in the setting of thyroid autoimmunity.
Materials and Methods:
Two hundred subjects (173 females and 27 males; median age, 37 years) were enrolled. None were under any pharmacological treatment. Exclusion criteria were any infectious/inflammatory/autoimmune comorbidity, kidney failure, diabetes, and cancer. In each subject, serum thyrotropin (TSH), free thyroxine, antithyroid antibodies, and circulating oxidative stress markers were measured. A questionnaire on dietary habits, evaluating the intake frequencies of food groups and adherence to the Mediterranean diet, was submitted to each participant.
Results:
Among the 200 recruited subjects, 81 (71 females and 10 males) were diagnosed with euthyroid Hashimoto's thyroiditis (HT); the remaining 119 (102 females and 17 males) served as controls. In questionnaires, HT subjects reported higher intake frequencies of animal foods (meat, p = 0.0001; fish, p = 0.0001; dairy products, p = 0.004) compared with controls, who reported higher intake frequencies of plant foods (legumes, p = 0.001; fruits and vegetables, p = 0.030; nuts, p = 0.0005). The number of subjects who preferentially consumed poultry instead of red/processed meat was lower in HT subjects than in controls (p = 0.0141). In logistic regression analysis, meat consumption was associated with increased odds ratio of developing thyroid autoimmunity, while the Mediterranean diet traits were protective. In HT subjects, serum advanced glycation end products (markers of oxidative stress) were significantly higher (p = 0.0001) than in controls, while the activity of glutathione peroxidase and thioredoxin reductase, as well as total plasma antioxidant activity, were lower (p = 0.020, p = 0.023, and p = 0.002, respectively), indicating a condition of oxidative stress. Stepwise regression models demonstrated a significant dependence of oxidative stress parameters on consumption of animal foods, mainly meat.
Conclusions
: The present study suggests a protective effect of low intake of animal foods toward thyroid autoimmunity and a positive influence of such nutritional patterns on redox balance and potentially on oxidative stress-related disorders.
Introduction
Hashimoto's thyroiditis (HT) is the most common autoimmune endocrine disease and the main cause of hypothyroidism in iodine-sufficient areas (1). Incidence has increased significantly over the last few decades (2,3), paralleling the steady rise in frequency of other autoimmune disorders (ADs) mostly in Western countries compared with the East and Global South (4,5). This rapid increase of ADs in developed countries and its clear relationship with socioeconomic status point to a strong influence of changing environmental factors in driving such geoepidemiologic trends as opposed to constancy of genetic basis (5,6).
Among the many environmental triggers of autoimmunity, growing interest has been focused on the Western lifestyle since several significant changes have occurred over the past decades in more industrialized and richer societies. They include modified infectious habitat and personal hygiene, increased pollution exposure, psychological stress overload, sedentary lifestyle, and changes in dietary habits (5 –12). In particular, in Westernized countries, a diet rich in calories, fats, and proteins, high in salt and refined sugars, and low in fibers is often preferred to dietary regimens rich in fruits and vegetables, along with more frequent consumption of processed and fast foods. This dietary regimen, the so-called Western-type diet, might influence risk of ADs either directly by increasing inflammation and altering immune (CD4+ effector and regulatory T cells) balance and intestinal microbiota composition or indirectly through increasing fat mass and obesity (10 –14). Another possible mechanism is enhanced oxidative stress, which is an imbalance between reactive oxygen species (ROS) production and removal by antioxidant mechanisms (15,16). A correlation between increased oxidative stress and the Western-type diet has been demonstrated since consumption of large amounts of fats and refined sugar in the long run results in intestinal dysbiosis and inflammation with ROS overproduction, while low intake of fruits and vegetables causes lack of exogenous antioxidants (16,17).
Several studies have evaluated the possible association between nutrition and autoimmunity in different settings of patients and consistently suggest dietary traits as risk factors for rheumatoid arthritis (RA), multiple sclerosis, psoriasis, and celiac and inflammatory bowel diseases (13,17 –23). In the field of thyroid diseases, however, very few studies have evaluated the role of different dietary patterns, mainly in relation to thyroid dysfunction rather than autoimmunity per se (24,25), and none have investigated the possible relationship with oxidative stress. The present study investigated nutritional habits in euthyroid HT subjects compared with healthy controls and their relationship with changes in redox balance.
Materials and Methods
Subjects
All subjects were recruited randomly from voluntary participants (>18 years old) in thyroid disorders awareness campaigns that were run at the Endocrinology Unit of the University Hospital “Policlinico G. Martino” of Messina, Italy, during International Thyroid Awareness week, World Thyroid Day, and in the preceding weeks to stimulate population awareness. To obtain as homogeneous a study population as possible with regard to geographic location, ethnic group, and lifestyle/diet, inclusion criteria at recruitment were Caucasian subjects stably living in the city of Messina, those with stable dietary habits in the last five years, and no history of pharmacological treatment, antioxidant agent, and/or vitamin supplements in the preceding six months. Exclusion criteria were obesity (body mass index [BMI] >30 kg/m2); diabetes mellitus; kidney failure; history of neoplastic disease; existence of any comorbid cardiovascular, autoimmune, infectious, or inflammatory disease; current or past smoking history; and current or former alcohol abuse. Patients who had already been diagnosed with thyroid disorders or who had already been treated for thyroid dysfunction were also excluded.
A total of 200 healthy subjects (173 females and 27 males; median age, 37 years), who agreed to thyroid function and autoantibodies tests and provide a blood sample, took part in the study and were administered a validated Italian questionnaire aimed at collecting data regarding lifestyle and dietary habits (26). Each subject underwent a careful history, physical examination, and thyroid ultrasonography. A food frequency questionnaire was used to evaluate the intake frequencies of food groups (meat, fish, cereals, fruits and vegetables, and dairy products). With this step, the 14 items included in PREDIMED, a validated questionnaire on the Mediterranean diet adherence, were also obtained (27); thus, adherence to the Mediterranean diet in the present cohort was assessed. Briefly, the PREDIMED score was calculated as follows: for each item, a score of 1 or 0 was assigned; a score of 0–5 meant low adherence, 6–9 represented average adherence, and ≥10 equated to high adherence (27). Concerning the iodine nutritional status, all subjects were from the same area of mild iodine deficiency (28). The design of the present study did not include individual urinary iodine measurements. However, all participants were asked if they used iodized salt to evaluate any difference in the iodine nutritional habits of the study population. All subjects were informed of the study aims according to the Declaration of Helsinki and provided written informed consent. The study was approved by the Ethics Committee of the University Hospital, AOU Policlinico G. Martino of Messina (study number 19-17).
Blood collection and biochemical analysis
Venous peripheral blood samples were collected after overnight fasting. Blood samples were centrifuged at 1450 g at 4°C for 10 minutes, and each sample was divided into aliquots. Processing and scoring of samples were performed blind and concurrently. At the end of the study, information regarding thyroid status and data from the questionnaire were linked to a code number and became available for statistical analysis.
Main metabolic parameters (fasting glucose, insulin, and lipids) and thyroid function indices were immediately measured. Serum thyrotropin (TSH), free thyroxine (fT4), and antithyroperoxidase antibodies (TPOAb) were measured by electrochemiluminescence immunoassay (Roche Diagnostics, Mannheim, Germany). Normal values were 0.27–4.5 mIU/L of TSH, 9.0–22.0 pmol/L of fT4, and 0–10 IU/mL of TPOAb. For all assays, the intra- or inter-assay coefficient of variation was <5% and <10%, respectively.
Aliquots for other assays were stored at −20°C. Two markers of oxidative stress, advanced glycation end products (AGEs) and advanced oxidation protein products (AOPPs), were measured in serum samples as previously reported (29). Activity of antioxidant enzymes superoxide dismutase (SOD), glutathione reductase (GR), glutathione peroxidase (GPx), thioredoxin reductase (TRxR), and total plasma antioxidant activity (TEAA) were measured in plasma samples as described elsewhere (Supplementary Data) (30,31). Overall, determination of the study parameters occurred within two months from sera collection.
Statistical analyses
Numerical data are expressed as median and range (minimum and maximum), and categorical variables are expressed as number and percentage. A nonparametric approach was used since most numerical variables were not normally distributed, as verified by the Kolmogorov–Smirnov test. To assess the existence of significant differences between HT subjects and controls, the Mann–Whitney test (for numerical parameters) and the chi-square, Fisher exact, or likelihood ratio tests were applied as appropriate (for categorical variables). The Spearman correlation was applied to evaluate interdependence between the studied oxidative stress markers, both in all subjects and in each group (HT subjects and controls, separately). Multivariate linear regression models (with stepwise procedure) were estimated to assess the possible dependence of each oxidative stress parameter (AGEs, AOPPs, SOD, GPx, GR, TRxR, and TEEA) on some potential explicative covariates, including age, sex, BMI, biochemical parameters (homeostatic model assessment, high-density lipoprotein cholesterol [HDL-C], triglycerides, thyroid function indices, and antithyroid antibodies), and dietary habits (food group intake frequencies, and adherence to the Mediterranean diet evaluated by the PREDIMED score). Finally, a multivariate logistic regression model (with stepwise procedure) was estimated to identify significant predictive factors of TPOAb positivity; covariates were age, sex (female 0, male 1), BMI, PREDIMED score, and intake frequency of main food groups (fish, meat, dairy products, eggs, cereals, fruits, and vegetables). Statistical analyses were performed using SPSS 22.0 for Windows. A p value <0.05 was considered statistically significant.
Results
Demographic, clinical, and biochemical features of the study population are summarized in Table 1. Eighty-one subjects (71 females and 10 males; median age, 40 years; age range, 18–66 years) were diagnosed with euthyroid HT by currently accepted laboratory and ultrasonographic criteria (serum antithyroid antibody positivity and/or heterogeneous echostructure with diffuse or patchy hypoechogenicity at ultrasound) (1). The remaining 119 subjects (102 females and 17 males; median age, 37 years; age range, 18–65 years) had no evidence of thyroid disease (normal thyroid function, absence of serum thyroid autoantibodies, and no ultrasound alterations) and served as controls. The two groups of age- and sex-matched HT subjects and healthy controls did not differ significantly regarding main anthropometric and metabolic parameters, with the exception of HDL-C (Table 1). All subjects were euthyroid, naive to levothyroxine therapy, and not taking any drugs affecting thyroid function at the time of sampling nor during the previous six months. However, HT subjects had higher TSH and lower fT4 values, although within normal ranges, compared with controls (p = 0.006 and p = 0.0001, respectively).
Demographic, Clinical, and Biochemical Characteristics of the Study Population
Data are expressed as median and range, in parenthesis. Level of significance at p < 0.05. Statistically significant p-values are in bold. Normal values are specified under the Materials and Methods section.
The BMI was calculated by dividing the body weight (kg) with the square of height in meters.
WHR, calculated by the formula waist circumference (cm)/hip circumference (cm).
Insulin resistance was estimated by the HOMA index.
BMI, body mass index; fT4, free thyroxine; HDL-C, high-density lipoprotein cholesterol; HOMA, homeostatic model assessment index; LDL-C, low-density lipoprotein cholesterol; TPOAb, antithyroperoxidase antibodies; TSH, thyrotropin; WHR, waist hip ratio.
Concerning oxidative stress parameters, AGEs were increased in HT subjects (p = 0.0001), while AOPP levels were similar between HT subjects and controls (p = 0.162). In the same HT subjects, GPx, TRxR, and TEAA were lower than in controls (p = 0.020, p = 0.023, and p = 0.002, respectively), indicating a condition of oxidative stress (Table 2). Correlation analysis assessing interdependence between oxidative stress markers demonstrated a significant inverse correlation between AGEs and TEAA in all participants (p = 0.018), as well as in HT subjects (p = 0.013), but not healthy controls (p = 0.747).
Circulating Levels of Oxidative Stress Parameters in Subjects with Hashimoto's Thyroiditis Compared with Healthy Controls
Data are expressed as median and range, in parenthesis. Comparison was made by the Mann–Whitney test. p-Values in bold are significant (p ≤ 0.05).
AU/g prot: arbitrary units (AU) per gram of protein.
μmol eqClT/L, chloramine-T units.
mM TE, millimole of Trolox equivalents.
AGEs, advanced glycation end products; AOPPs, advanced oxidation protein products; GR, glutathione reductase; GPx, glutathione peroxidase; HT, Hashimoto's thyroiditis; SOD, superoxide dismutase; TEAA, total plasma antioxidant activity; TRxR, thioredoxin reductase.
In questionnaires, HT subjects reported higher intake frequencies of animal foods (meat, p = 0.0001; fish, p = 0.0001; dairy products, p = 0.004) compared with controls, who, in turn, reported higher intake frequencies of plant foods, including legumes (p = 0.001) and fresh fruits and vegetables (p = 0.030) (Figs. 1 and 2). The two groups mainly differed regarding consumption of meat, as HT subjects reported higher intake frequencies of animal meat in general, specifically red/processed meat, compared with controls. Indeed, the number of subjects who reported preferential consumption of white meat and poultry instead of red/processed meat was significantly lower in the HT group than in the control group (29% vs. 52%; p = 0.014). None of the subjects who did not eat meat at all or no more than twice a month were found to have thyroid autoantibodies. Moreover, consumption of other animal foods, such as fish and dairy products, was higher in HT individuals than in controls, but no difference in egg consumption was observed (p = 0.081). Finally, the number of subjects who reported consumption of ≥3 servings per week of nuts was significantly lower in HT subjects compared with controls (23% vs. 55%; p = 0.0005).
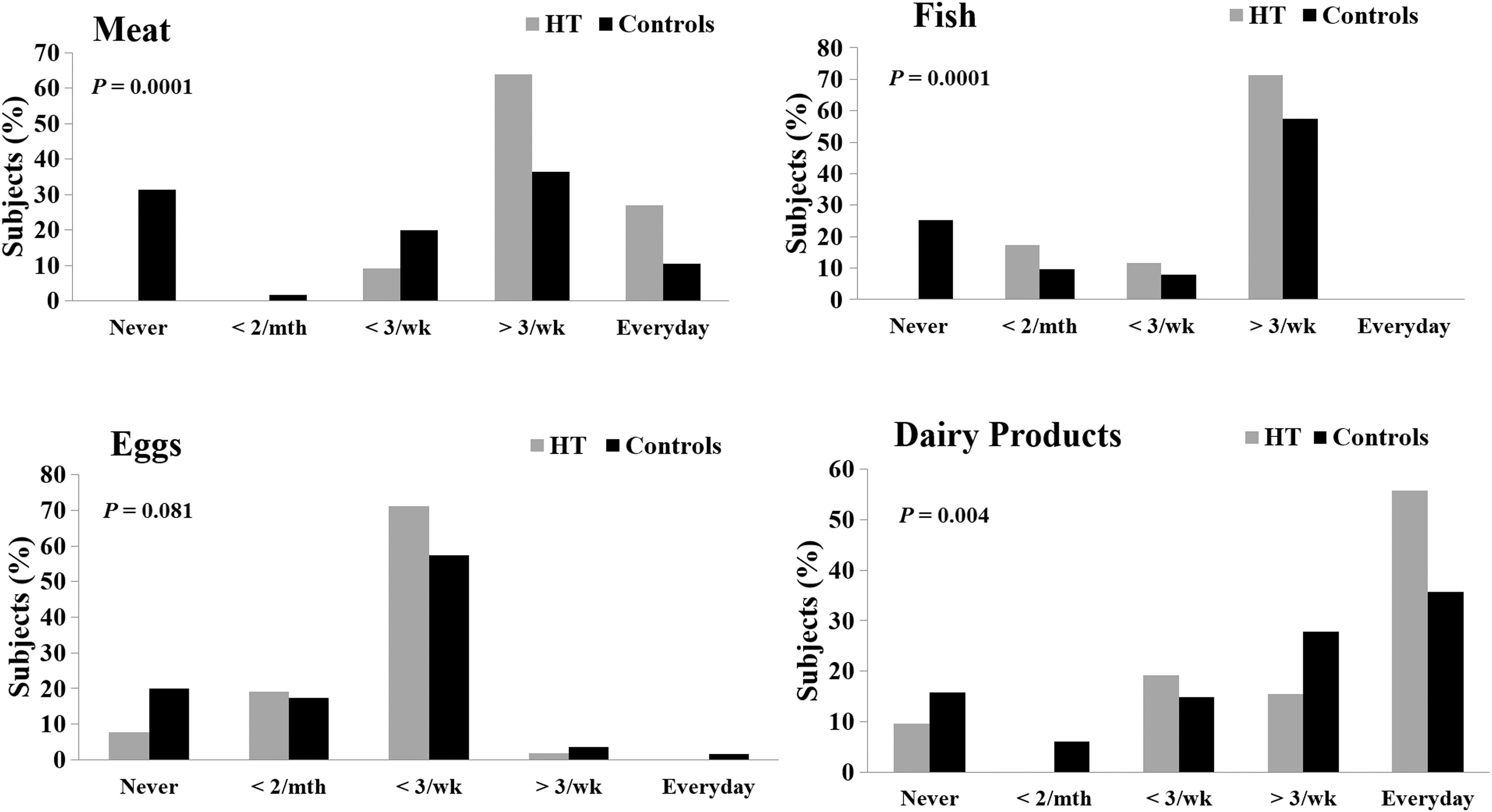
Intake frequencies of animal foods in HT subjects and healthy controls, as reported in food frequency questionnaires. HT subjects reported higher intake frequencies of animal products, including meat, fish, and dairy products, compared with controls. HT, Hashimoto's thyroiditis.
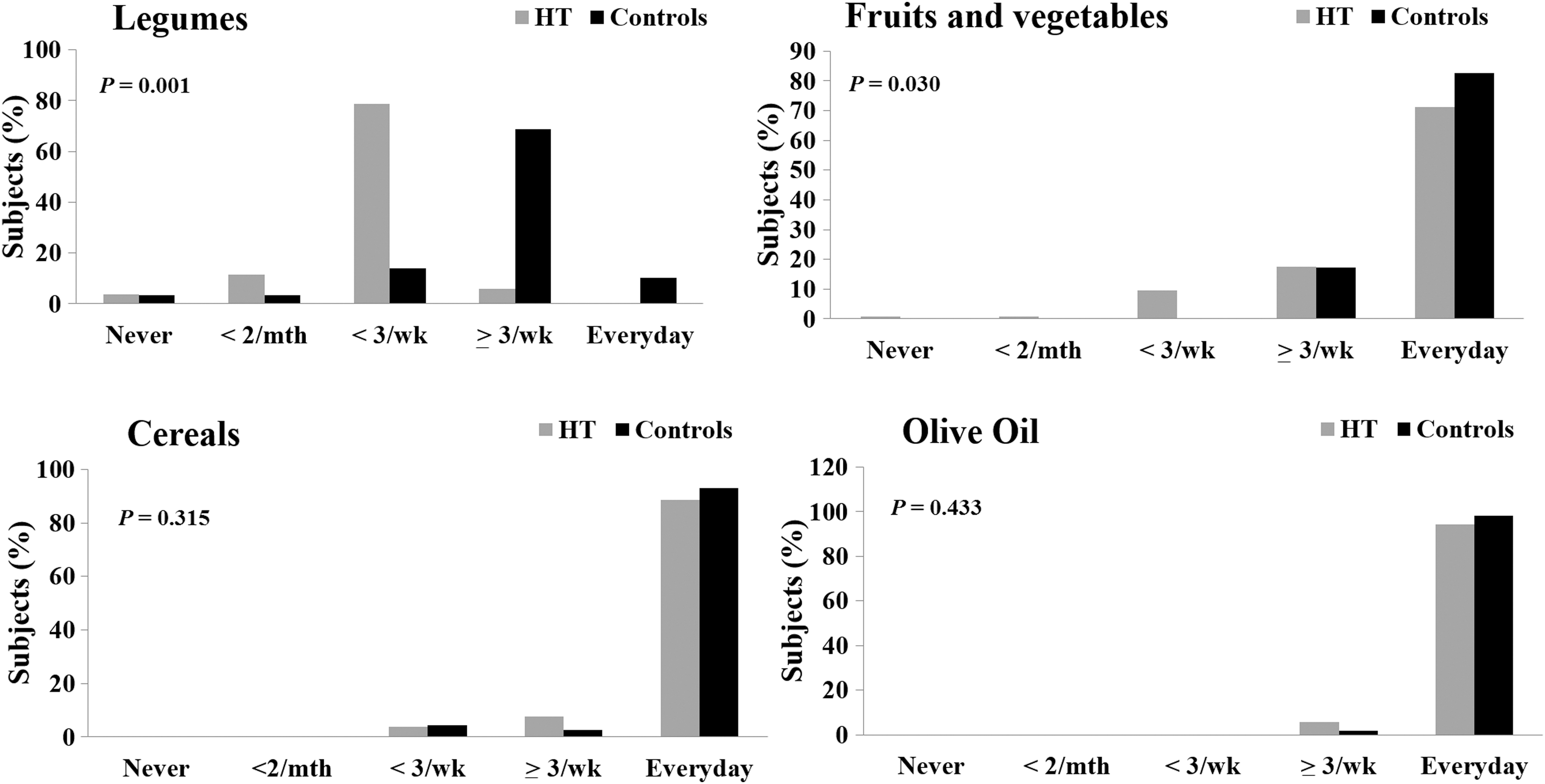
Intake frequencies of plant foods in HT subjects and healthy controls, as reported in food frequency questionnaires. HT subjects reported lower intake frequencies of legumes, fruits, and vegetables compared with controls. The two groups did not differ concerning olive oil and cereals consumption.
The HT and control groups did not differ concerning intake of cereals (88.5% vs. 93%, p = 0.315) and whole grain (51% vs. 58%, p = 0.563). Furthermore, most subjects reported use of olive oil as main culinary fat (at least four tablespoons daily), without difference between HT and control subjects (94% vs. 98%, p = 0.433). Similarly, most subjects in both groups did not use butter or cream at all, while less than one third of subjects consumed butter, margarine, or cream <3 day/week, without differences between the groups (p = 0.733). Finally, HT subjects reported a higher frequency of consumption of fats and refined sugars from commercial sweets (p = 0.010) despite no differences in the consumption of sweetened or carbonated beverages (all <1 per day). Moreover, control and HT subjects did not differ concerning weekly consumption of wine or general alcohol intake (p > 0.05). Finally, there was no difference in the use of iodized salt between HT subjects and controls, but individual urinary iodine concentrations were not available.
Concerning lifestyle, most of the subjects reported doing physical activity no more than twice a week (70% of HT subjects vs. 60% of controls), without significant differences between subjects with or without HT (p = 0.176). Current or past smokers were excluded to avoid biases. The largest part of the cohort presented a medium–high grade of adherence to the Mediterranean diet according to the PREDIMED scores. However, HT subjects displayed significantly lower scores than controls (p = 0.0001; Fig. 3). The main determinants of this difference were the higher consumption of animal meat in general, red/processed meat in particular, the lower consumption of vegetables, fruits, and legumes, the higher consumption of commercial sweets or pastries, and the lower consumption of nuts in HT subjects compared with controls.

Adherence to the Mediterranean diet in our cohort, as evaluated by a validated 14-items questionnaire (PREDIMED score). The PREDIMED score was significantly lower in HT subjects compared with healthy controls (top). Accordingly, HT subjects exhibited a significantly lower grade of adherence to the Mediterranean diet than controls, calculated as follows: a score of 0–5 meant low adherence, 6–9 represented average adherence, and ≥10 equated to high adherence (bottom).
In the multivariate logistic regression model, adherence to the Mediterranean diet, as evaluated by the PREDIMED score, was a significant predictive factor of TPOAb positivity. A higher score of adherence to the Mediterranean diet along with higher intake frequencies of fruits, vegetables, and cereals was protective against the risk for developing thyroid autoimmunity, while higher intake frequency of meat and dairy products was significantly associated with an increased risk of thyroid autoimmunity (Table 3). As expected, increasing age and female sex were also associated with an increased probability of developing thyroid autoantibodies in the regression model (Table 3).
Multivariate Logistic Regression Model with Stepwise Procedure a
The PREDIMED score was calculated as specified under the Materials and Methods section to assess adherence to the Mediterranean diet.
Level of significance at p < 0.05. Statistically significant p-values are in bold.
CI, 95% confidence interval.
Stepwise regression models demonstrated a significant dependence of oxidative stress parameters on age and consumption of animal foods; meat intake was associated with lower levels of the antioxidants GPx (p = 0.048), GR (p = 0.010), and TRxR (p = 0.007) but higher levels of the oxidants AGEs (p = 0.045) and AOPPs (p = 0.048). Similarly, dairy product intake was associated with low levels of both GR (p = 0.048) and TEAA (p = 0.020; Table 4). Eggs, which represent a source of animal proteins and saturated fats, were slightly but significantly associated with reduced levels of GPx (p = 0.010) despite consumption being similar between the two groups (p = 0.221; Table 4). Finally, TPOAb positivity was an independent predictor of increased AGEs and reduced GPx and GR activities in multivariate analysis (Table 4).
Multivariate Linear Regression Models with Stepwise Procedure
Level of significance at p < 0.05. Statistically significant p-values are in bold. The PREDIMED score was calculated as specified under the Materials and Methods section to assess adherence to the Mediterranean diet.
PA, physical activity; SE, standard error; TG, triglycerides.
Discussion
In the present pilot study, the nutritional habits of a cohort of euthyroid HT subjects compared with healthy subjects, and the relationship between intake of different foods and changes in redox balance was investigated. A main finding was that dietary habits significantly differed between subjects with and without HT. HT subjects reported a higher intake of animal products and a lower level of adherence to the Mediterranean diet than healthy controls, who reported higher intake of plant foods. Overall, the nutritional pattern of HT subjects according to the survey was characterized by increased consumption of animal proteins, higher intake of saturated fats and refined sugars, and lower intake of fibers and antioxidants compared with healthy subjects. In other words, nutritional patterns of HT subjects resembled the Western-type diet, while controls displayed a higher level of adherence to the Mediterranean diet. Such a significant difference supports the hypothesis of a possible predisposing role of nutritional patterns in autoimmunity.
The association between diet and risk of developing ADs was proposed as early as 50 years ago by Trowell, who observed that a number of ADs, including RA, type 1 diabetes, and HT, were extremely rare among isolated rural sub-Saharan populations following traditional near-vegan diets (32,33). A similar low incidence of ADs was reported in Asian societies whose diets were almost vegan (33). In the last few decades, further evidence has accumulated on the influence of nutritional factors in the development of several ADs, including RA, celiac and inflammatory bowel diseases, type 1 diabetes, multiple sclerosis, and psoriasis (13,17 –23). To date, only two studies have assessed the dietary habits of subjects suffering from thyroid diseases. In 2013, Tonstad et al., using data from the Adventist Health Study-2 (AHS-2), evaluated the prevalence and incidence of hypothyroidism among a large cohort (n = 65,981) of Seventh-day Adventist church members who exhibited a wide range of diets from vegan to omnivorous, with a high proportion of vegetarians (24). They found a lower, although not significant, prevalence and incidence of hypothyroidism among subjects following vegan diets compared with omnivorous diets, even after adjusting for BMI and demographic variables (24). Among the same population from the AHS-2 study, a strongly reduced risk of hyperthyroidism was also reported in those consuming a vegan diet when compared with omnivores, while lacto-ovo and pesco vegetarian diets were associated with intermediate protection (25). These two studies provided congruent, although not always statistically significant, data in favor of a protective role of diets excluding meat against both hypo- and hyperthyroidism, commonly autoimmune in etiology (24,25).
The present study further points to meat in omnivorous diets as a main nutritional factor associated with increased risk of thyroid autoimmunity. Also, intake of animal proteins and saturated fats from dairy products seems to be relevant to the development of HT, while plant foods, containing high amounts of antioxidants and fibers and no fats, may be protective. Compared with healthy controls, HT subjects reported the highest intake of saturated and trans fats from animal products as well as commercial sweets and pastries. In the survey, HT subjects reported significantly higher intake of fish than controls. These results partially contradict previous reports on the protective role of seafood and fish oil supplementation against ADs, including HT (21,23,32,34). Perhaps this different influence could be related to the variable content of polyunsaturated fatty acids, such as ω-3 polyunsaturated acids, in the fish species consumed (oily fishes or other species). Since we assessed the frequencies but not the quality of consumed seafood in our survey, we can only infer that protein content may account for the association between fish consumption and thyroid autoimmunity.
Finally, HT subjects in the present cohort displayed significantly lower adherence to the Mediterranean diet compared with healthy controls, and the PREDIMED score was an independent predictor of the presence of thyroid autoantibodies, suggesting that the Mediterranean diet is associated with reduced risk for thyroid autoimmunity. The Mediterranean diet is a nutritional model inspired by traditional dietary regimens of populations living in the Mediterranean basin and is characterized by high intake of vegetables, legumes, fresh fruits, nuts, whole grains, and olive oil; frequent and moderate consumption of red wine; moderate intake of seafood, dairy products, poultry, and eggs; and low consumption of red meat and processed meat products (35). This dietary pattern is rich in fibers, natural antioxidants, and vitamins, and consequently, had anti-inflammatory and antioxidant effects, which are beneficial to health status (33,34). Much evidence exists in favor of the protection imparted by the Mediterranean diet against diseases associated with chronic inflammation, including diabetes, obesity, cardiovascular diseases, cancer, and cognitive disorders (36). The current study provides the first evidence of a protective role of the Mediterranean diet also against thyroid ADs. It is conceivable that adoption of this dietary pattern could also be protective against ADs, counteracting the deleterious effects of oxidative stress and exerting anti-inflammatory and immunomodulatory actions, most likely by affecting cytokine production and gut microbiota composition. Indeed, gut dysbiosis may represent another possible pathogenetic mechanism linking diet to autoimmunity (10,37).
Notably, despite the excess caloric intake of their nutritional habits (high-fat and high-sugar), HT subjects did not differ from controls regarding body weight and BMI. This suggests that the pathogenetic link between diet and thyroid autoimmunity cannot be represented by being overweight or obesity, whose proinflammatory effects are well known, at least in this current cohort. Indeed, BMI was not a significant predictor of thyroid autoantibody positivity nor alterations in oxidative stress parameters in regression models.
Another important finding of the present study was the significant influence of nutritional pattern on oxidative stress parameters. Oxidative stress, defined as an imbalance between free radical production and antioxidant defense mechanisms, has been implicated in the pathogenesis of several inflammatory and immune-mediated disorders, including thyroid ADs, and the role of antioxidants is intensely debated (29,38 –42). Excess ROS production due to environmental agents could induce modification of tissue proteins or may dysregulate the immune system, influencing the onset of an AD. Moreover, excess ROS increases the proinflammatory state and leads to tissue damage, further contributing to the progression of ADs (43). In the current cohort of euthyroid HT subjects, measured oxidants were increased and antioxidants decreased, confirming redox dysregulation in HT subjects compared with controls. Enhanced oxidative stress seems to be related to chronic autoimmune inflammation rather than variations of thyroid hormone levels despite the fact that a slightly intracellular decrease of thyroid hormones cannot be ruled out in such subjects. The dietary habits of the subjects seemed to influence the redox balance independent from thyroid autoimmunity and function. Indeed, in all subjects, the intake of animal foods, mostly meat, significantly increased levels of oxidants and significantly lowered levels of antioxidants.
A major strength of the present study was the collection of nutritional data in a group, which was homogeneous for race/ethnicity, stable residence, stable dietary habits, and normal anthropometric and metabolic parameters. Another key strength was all recruited subjects had well-characterized thyroid profiles, with thyroid autoantibodies and hormones as well as oxidative stress parameters measured to investigate possible pathogenetic links between nutrition and thyroid autoimmunity. Major limitations of the present study were the relatively small number of recruited subjects and rather high prevalence of HT in the study group. Despite an involuntary selection bias that cannot be excluded, this finding of a high prevalence of HT subjects was in line with previous studies, which reported a higher frequency of HT in the Messina area than in neighboring areas. Moreover, a more relevant increase in HT incidence has been reported in this area in recent decades (44,45). Consequently, this study group cannot be considered representative of the general population or other populations. Moreover, the observational design of the study, which reports descriptive data, does not allow establishment of any causal relationship between imbalanced redox ratios and HT as well as diet.
In conclusion, pending confirmation with a large samples series and other populations, the present study suggests that low intake of animal foods has a potentially protective effect on thyroid autoimmunity as a result of the positive influence of this dietary habit on redox balance and consequent oxidative stress-related disorders. Reducing the intake of animal proteins and fats and increasing that of plant foods may represent a useful lifestyle strategy for reducing the risk for autoimmune thyroid disorders. In particular, a predominantly plant-based Mediterranean diet may represent a healthy food model in the setting of ADs.
Authors' Contribution
Each author contributed substantially to the article and approved the final version for publication.
Disclaimer
All subjects were informed of the study aims according to the Declaration of Helsinki and provided written informed consent. The study was approved by the Local Ethics Committee.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data