
Abstract
Background:
A significant increase in the incidence of papillary thyroid carcinoma (PTC) in subjects exposed to radiation at a young age is a well-documented health consequence of the Chernobyl accident. The ongoing Thyroid Ultrasound Examination (TUE) program in children and adolescents of Fukushima Prefecture in Japan also indicated a high prevalence of PTC although its attribution to radiation exposure is a subject of debate. The objective of this study was to perform histopathological analysis of tumor architecture and invasive properties in (i) radiogenic post-Chernobyl and sporadic PTCs from Ukraine, and (ii) PTCs in patients from Fukushima and other Prefectures of Japan of comparable age groups.
Methods:
The Ukrainian radiogenic PTCs included 245 PTCs from patients who resided in three highly 131I-contaminated regions and 165 sporadic PTCs diagnosed in residents of the same regions who were born after the accident and therefore not exposed to radioiodine. The Japanese series included 115 PTCs detected during the preliminary and the first full-scale surveys of the TUE in Fukushima and 223 PTCs from patients resident in other Prefectures. All of the subjects were included in the main statistical analysis. Three additional analyses were performed limiting the subjects to children, adolescents, and adults.
Results:
Ukrainian radiogenic PTC was characterized by the higher frequency of tumors with a dominant solid-trabecular growth pattern and higher invasiveness, more frequent extrathyroidal extension, lymphatic/vascular invasion, regional and distant metastases when compared with sporadic Ukrainian PTC. The integrative “invasiveness score,” based on five cancer characteristics, was also higher in the radiogenic group. The differences were most pronounced in children. In contrast, no significant differences in tumor morphology or invasiveness were observed between the two Japanese groups or the three age subgroups. The only statistically significant findings were the higher proportion of male patients, smaller mean tumor size, and higher frequency of T1b tumors in the Fukushima group.
Conclusions:
The difference in morphological features that indicate biological behavior of PTC between the radiation-related and sporadic groups from Ukraine, together with the lack of such in the two groups from Japan, strongly suggest a nonradiogenic etiology of PTC from Fukushima and other Prefectures.
Introduction
Previous studies, both from our own and other groups, showed a significant increase in the incidence of radiation-related thyroid cancer in Ukraine after the Chernobyl accident, predominantly papillary thyroid carcinoma (PTC). This increase was first observed in 1990 in subjects who were children and adolescents at the time of exposure and resided in the most contaminated by the 131I fallout regions of Ukraine. Thus, the minimum latent period of radiogenic PTC in Chernobyl-affected areas is about four years (1 –5). PTCs developing after this shorter latency have been shown to be more aggressive than those with a longer latency (6). Furthermore, we have recently demonstrated that Chernobyl PTCs display more invasive features than sporadic tumors (7 –9).
The Thyroid Ultrasound Examination (TUE) of children and adolescents of Fukushima Prefecture, which forms part of the Fukushima Health Management Survey, has also resulted in a high detection rate of PTC, most notably in the first and second rounds of screening four to five years after the Fukushima accident. However, radiogenic etiology for these cancers is highly unlikely (10 –17). Our investigation of histopathological characteristics of PTC detected greater than four to five years after the Fukushima Dai-ichi nuclear power plant accident found no significant differences from those diagnosed during the initial four years after the accident (18).
The direct pathological comparison of Chernobyl with Fukushima PTC is not reasonable in view of known morphological differences between the Ukrainian and Japanese PTCs in patients of any age (19 –21). Therefore, using an appropriate “geographic control,” we set out to analyze the differences in tumor architecture and invasive properties between (i) Ukrainian radiogenic Chernobyl and Ukrainian sporadic PTC, and (ii) Fukushima PTC and Japanese sporadic PTC diagnosed in patients from other Prefectures of Japan.
Materials and Methods
Patients
The study was approved by the ethic committees of all participating institutions. A total of 748 (410 Ukrainian and 338 Japanese) PTCs were included.
The Ukrainian radiogenic series comprised 245 PTCs from patients exposed to the Chernobyl radiation. All patients were from 4 to ≤23 years at the time of surgery for PTC, which was performed at the Institute of Endocrinology and Metabolism, Kyiv, Ukraine (IEM) between 1990 and 2015. Since the highest risk of thyroid cancer following the Chernobyl accident is observed in the youngest children residing in the most contaminated by 131I regions (2,4,5,22), the radiogenic cases were selected from those who were ≤4 years old in 1986 and lived in Kyiv, Chernihiv, or Zhytomyr regions.
The group of sporadic PTCs comprised 165 nonexposed to radiation patients who were born after the accident beginning from January 1, 1987, or later, and lived in the same regions as the radiogenic cases or in Kyiv city. The sporadic cases were diagnosed between 1997 and 2015; the patients' age at surgery was from 6 to ≤23 years old. The radiogenic and sporadic groups in the present work are a subset of the larger group of PTC patients from Ukraine described in our previous study (8), but limited here to those who were 23 years old or younger, to be consistent with the age characteristics of patients in the Japanese series (see the next paragraph). None of the Ukrainian cases was detected in the course of ultrasound screening programs. No familial cases were registered in the Ukrainian series.
The Japanese series comprised 115 cases detected during the preliminary and the first full-scale surveys (the first and the second screening cycles, respectively) of the TUE in subjects who were aged ≤18 years at the time of Fukushima accident. These patients were 9–23 years old at the time of their operations, which were carried out at the Fukushima Medical University (FMU) between 2012 and 2016 (the Fukushima group). All cases were combined in one group, regardless of time of diagnosis for the present analysis, as a significant difference had not been found in our previous study (18) of the histopathological characteristics of Fukushima PTCs between these two time periods (i.e., less than four years and four to five years after the Fukushima accident).
Our research strategy, similar for the Ukrainian and the Japanese series, was to compare post-Chernobyl and post-Fukushima PTCs with an adequate geographically and age-matched series of sporadic PTCs. In Ukraine, by the time of the study beginning, a sufficient number of sporadic cases from patients born after Chernobyl had been accumulated.
In Japan, by and at the time of the study, the age of subjects born after the Fukushima accident could not be older than four years. Therefore, the Japanese age-matched sporadic PTCs were from patients who lived in Prefectures of Japan other than the Fukushima Prefecture. A total of 223 PTCs from patients aged ≤23 (6 –23) years at surgery, and operated on between 1983 and 2016, were selected from the archives of Kuma Hospital at Kobe city (the Kuma group). None of these patients had a history of radiation exposure. No familial thyroid cancer cases were registered in the Japanese series.
Both the Ukrainian and Japanese PTCs were analyzed as one group and in three age subgroups defined as children ≤14, adolescents 15 to ≤18, and adults 19 to ≤23 years old at surgery to compare differences between radiogenic and nonradiogenic PTCs from Ukraine, and Fukushima and Kuma PTCs from Japan. The upper limit of 23 years of age for the Ukrainian patients was determined by the oldest possible age of the patients in the Fukushima group. Given the inclusion criteria of the TUE (≤18 years old in 2011) and operation period (from 2012 to 2016), the oldest possible age for a patient in the Fukushima group was 23 years.
Histopathology
The pathological classification was based on the World Health Organization classification (23). Histopathological examination of hematoxylin/eosin-stained paraffin sections was initially performed at local institutions by experienced pathologists (T.I.B. and L.Y.Z. in IEM; Y.H. and M.I. in FMU; M.H. and T.H. in Kuma Hospital). Diagnosis of PTC for the Ukrainian cases had been confirmed by the international pathology panel of the Chernobyl Tissue Bank project (T.I.B. and M.I., members, coauthors of this work). Diagnosis of PTC for the Fukushima cases was additionally confirmed by the Fukushima Pathology Consensus Panel (M.H., M.I., A.S., H.N., members, coauthors of this work).
In this study, we followed the joint protocol of pathological analysis used in our previous investigations (8,18), in which T.I.B. reviewed all available slides of the tumor, extratumoral tissue, and all removed lymph nodes. The number of slides per case varied with tumor size and volume of operation being cumulatively about 10 for small tumors and more than 40 for large volumes of operation. Data were entered into an electronic spreadsheet, which was sent to all coauthors for comments and corrections before data analysis.
For the purpose of the current analysis, tumors were classified according to the dominant histological growth pattern into three categories: papillary, follicular, or solid-trabecular, when the corresponding structural component exceeded 50% of a tumor section surface. We also distinguished focal and severe oncocytic (oxyphilic/Hurtle) cell changes in the tumor epithelium as previously described (8,24).
The tumor (T) category was defined according to the 7th (25) and 8th (26) editions of TNM classification system to analyze both the minimal and gross extrathyroidal extension. Tumor extension into the fat and connective tissue, detected only on postoperative histology (27,28), corresponds to pT3 according to the 7th edition, but is removed from the definition of pT3 in the 8th edition; only gross extension into the strap muscles is pT3b according to the latter.
We also introduced a variable, the “invasiveness score,” which included each instance of N1, M1 (commonly detected by diagnostic imaging), any extrathyroidal extension (i.e., minimal or gross), multifocality, and lymphatic/vascular invasion, either isolated or in combination with other(s) for each tumor. Thus defined, the invasiveness score ranged from 0 (no invasive feature presents) to 5 (all features present).
Statistical analysis
The univariate Fisher's exact test or the Fisher–Freeman–Halton exact test was used for categorical data, and the Mann–Whitney test for continuous data was used for comparisons between any two (sub)groups. Multivariable logistic regression models were adjusted for age at surgery and sex. Analyses with very small numbers of outcomes (<5 per cell) were conducted using Firth's approach to bias-reducing penalized maximum likelihood fit. Calculations were performed using IBM SPSS Statistics Version 24 software (International Business Machines Corp., Armonk, NY) or the 3.71 release of SAS Studio for the 9.4M5 version of SAS (SAS Institute, Cary, NC). All tests were two-sided and maximum likelihood ratio based; p < 0.05 was considered statistically significant.
Correspondence analysis (29) was performed using R with the ca, FactoMineR, factoextra, gplots, tidyverse, and corrplot packages. The colgreen option was used to calculate biplot principal coordinates for columns (the four PTC groups) and contribution coordinates, which are the standard coordinates multiplied by the square root of the corresponding masses, for rows (categorical clinicopathological variables).
Results
Ukrainian radiogenic versus sporadic PTCs
The mean age of patients in the radiogenic group was slightly younger (0.92 [0.88–0.97], p = 9.070E-04, hereinafter the odds ratio (OR; 95% confidence interval [CI]) and p-value are indicated for multivariate analyses, Table 1), and the proportion of male patients was higher than in the sporadic group (1.77 [1.12–2.79], p = 0.014). For this reason, we adjusted odds ratios for all other variables for age and sex. The mean size of radiogenic PTC was slightly greater than that of sporadic tumors on univariate comparison, but on multivariate analysis the difference was not significant. However, there was a significant difference in the distribution by tumor size—micro-PTCs (largest diameter ≤10 mm) were less frequent (0.41 [0.24–0.69], p = 6.710E-04), while tumors measuring from 11 to 20 mm were more frequent in the radiogenic group (1.81 [1.19–2.76], p = 0.006). Encapsulated tumors were less frequent in the radiogenic group (0.54 [0.32–0.91], p = 0.020).
Characteristics of Ukrainian Sporadic and Radiogenic Papillary Thyroid Carcinoma
% For count data, median and interquartile range for continuous variables.
Adjusted for age and sex unless otherwise specified.
Adjusted for sex.
Adjusted for age, female sex was used as a reference.
Mann–Whitney test.
Fisher–Freeman–Halton exact test (for frequencies).
pT category according to the 7th edition of the TNM Classification of Malignant Tumors.
pT category according to the 8th edition of the TNM Classification of Malignant Tumors.
Invasiveness score included each instance of N1, M1, any extrathyroidal extension, multifocality or lymphatic/vascular invasion, either isolated or in combination with other(s).
CI, 95% confidence interval; NA, not available; OR, odds ratio.
A dominant papillary growth pattern was significantly less frequently observed in the radiogenic group (0.30 [0.19–0.46], p = 5.15E-08), while a dominant solid-trabecular structure was more frequent (2.48 [1.57–3.92], p = 1.03E-04). Radiogenic PTC, in contrast to sporadic, displayed less frequent oncocytic changes in tumor epithelium and the signs of concomitant chronic thyroiditis in extratumoral tissue (0.13 [0.07–0.25], p = 1.73E-10 and 0.34 [0.20–0.58], p = 8.80E-05, respectively).
Tumor stage according to the pTNM classification, namely the pT category, showed significant difference between the radiogenic and sporadic groups either according to the 7th or 8th editions of classification (1.43 [1.14–1.80], p = 0.002 and 1.34 [1.01–1.78], p = 0.039, respectively). It is worth noting that exclusion of tumors with signs of minimal extrathyroidal extension to the fat and connective tissue from the pT3 category in the 8th TNM edition led to an increase in the frequency of pT1 and pT2 tumors and a decrease of pT3 tumors in both Ukrainian groups. Nevertheless, the frequency of the 8th edition's pT3 tumors remained significantly higher in the radiogenic group (2.79 [1.46–5.30], p = 0.002), and this was due to the advanced pT3b tumors (8.19 [2.50–27.40], p = 0.001), while the frequency pT3a tumors was practically the same in both groups.
Regional (N1) and distant (M1) metastases were more frequently observed in the radiogenic group (1.62 [1.06–2.47], p = 0.025 and 3.96 [1.60–9.82], p = 0.003, respectively), and so was lymphatic/vascular invasion (1.98 [1.28–3.05], p = 0.002). Thus, except for multifocality, all indicators of PTC invasiveness considered in this study were more frequent in the radiogenic group. Assessment of the invasiveness score, which included each instance of either invasive feature occurrence in a tumor, confirmed the higher chance of having more of such features among the radiation-related PTCs (1.39 [1.18–1.64], p < 7.57E-05). Furthermore, the distribution of the invasiveness score demonstrated a shift of higher tumor invasiveness toward the radiogenic group with a statistically significant uptrend in odds ratios (1.62 ± 0.50 [b ± SE, the regression coefficient ± standard error], p = 0.047, Table 1).
Age-matched subgroups of radiogenic and sporadic PTCs from Ukraine
The comparative characteristics of sporadic and radiogenic Ukrainian PTCs in the whole group and in age-matched subgroups are presented in Figure 1; statistical details are shown in Supplementary Tables S1–S3.
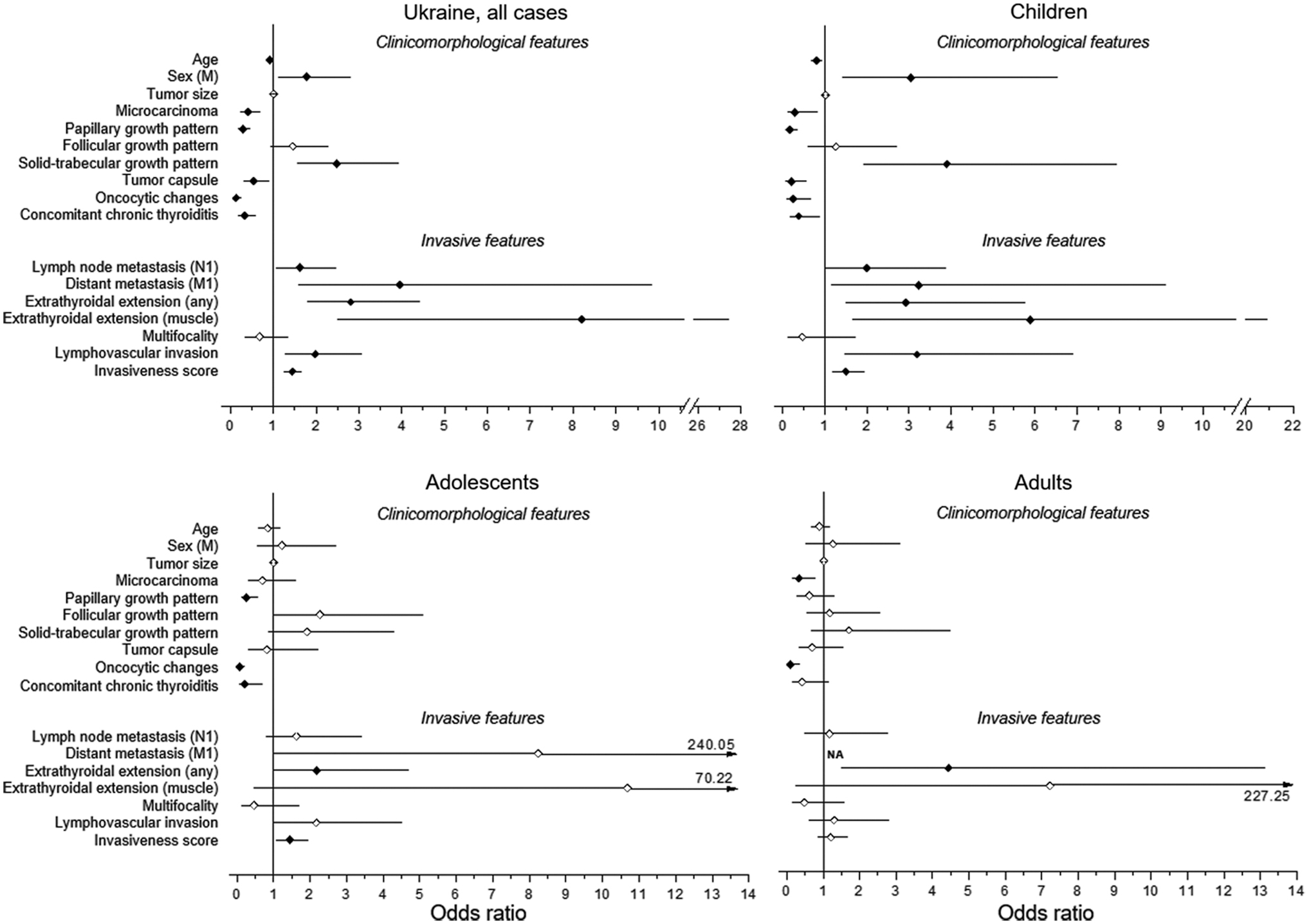
Clinicomorphological and invasive features of the radiogenic Ukrainian PTC in comparison with sporadic PTC. The odds ratios adjusted for age and sex are shown, using the corresponding sporadic PTC (sub)groups as the reference. Filled symbols indicate statistically significant differences. NA, not available; PTC, papillary thyroid carcinoma.
All statistically significant comparisons found in the whole Ukrainian series were seen in the childhood subgroup (patients with radiogenic or sporadic PTC aged ≤14 years at surgery, Fig. 1 Children and Supplementary Table S1). Specifically, significant differences were observed in the radiogenic group for patients' age (0.80 [0.68–0.93], p = 0.004), male sex (3.05 [1.42–6.55], p = 0.004), tumor encapsulation (0.20 [0.07–0.56], p = 0.003), frequencies of microcarcinomas (0.29 [0.10–0.82], p = 0.020), dominant papillary (0.16 [0.08–0.35], p = 3.00E-06) and solid-trabecular growth patterns (3.90 [1.92–7.93], p = 1.76E-04), oncocytic changes in tumor cells (0.25 [0.10–0.66], p = 0.005), concomitant chronic thyroiditis (0.38 [0.17–0.87], p = 0.022) and indicators of invasiveness; nodal disease (2.00 [1.03–3.88], p = 0.041), distant metastasis (3.24 [1.15–9.11], p = 0.026), extrathyroidal extension (2.93 [1.49–5.76], p = 0.002), and lymphatic/vascular invasion (3.19 [1.47–6.91], p = 0.003). The invasiveness score was also higher in the radiogenic group (1.50 [1.17–1.93], p = 0.002).
In the subgroup of adolescents aged 15–18 years at surgery, the number of variables displaying statistically significant differences between radiogenic and sporadic PTCs was lower than in children, yet still present (Fig. 1 Adolescents and Supplementary Table S2). In exposed patients, significant decreases in frequencies were observed for the dominant papillary growth pattern (0.26 [0.12–0.58], p = 9.41E-04), oncocytic changes (0.07 [0.02–0.23], p = 3.00E-05), and concomitant chronic thyroiditis (0.22 [0.08–0.67], p = 0.008). Signs of any extrathyroidal extension were more frequently seen among the radiogenic PTCs (2.17 [1.00–4.69], p = 0.050). Extrathyroidal extension into the muscles (pT3b category, the 8th TNM edition) was more frequent on univariate analysis (p = 0.032), but was not significant on multivariate analysis (10.67 [0.47–240.05], p = 0.132). A higher frequency of distant metastases (M1 category) in the radiogenic group was just marginally significant (8.24 [0.97–70.22], p = 0.054). The invasiveness score was significantly higher in the radiogenic group of adolescent patients (1.44 [1.07–1.95], p = 0.017), as had been observed in the childhood subgroup.
In the subgroup of adults aged 19–23 years at surgery, significant differences between radiogenic and sporadic PTCs were detected for three parameters. In radiogenic PTCs, the frequencies of microcarcinomas (0.33 [0.14–0.78], p = 0.012) and of oncocytic changes (0.09 [0.03–0.34], p = 3.18E-04) were lower, and that of any extrathyroidal extension (4.44 [1.50–13.12], p = 0.007) was higher than that in sporadic PTCs.
It should be noted that the dominant growth pattern largely reflects the histological subtype/variant of PTC. Rarer PTC subtypes such as diffuse-sclerosing (DSV) and Warthin-like variants were identified in a small number of cases. DSV was observed in childhood and adolescent subgroups of radiogenic PTC in 8/121 cases (6.6%) and in 1/66 (1.5%), respectively. In all radiogenic cases, DSV tumors displayed the solid foci spreading to both thyroid lobes. In sporadic PTC, DSV was detected only in children, 2/60 (3.3%). In the whole series, DSV was 3.1 times more frequent in radiogenic (9/245, 3.7%) than in sporadic PTCs (2/165, 1.2%), but the difference was not statistically significant (p = 0.244).
The Warthin-like variant of PTC was absent in children, but was found in 1/66 (1.5%) of radiogenic and 1/54 (1.9%) of sporadic adolescent PTCs, and in 4/51 (7.8%) of sporadic adult PTCs. All Warthin-like PTCs had a dominant papillary growth pattern. Overall, the Warthin-like variant of PTC was 7.5 times less frequent in radiogenic (1/245, 0.4%) than in sporadic PTC (5/165, 3.0%), but the difference was not statistically significant (0.19 [0.02–1.66], p = 0.132). No tall cell or columnar cell variants of PTC were found in the entire Ukrainian series.
Comparison of the Japanese PTCs in Kuma and Fukushima groups
Our comparison of the Japanese PTCs operated at FMU (the Fukushima group) and Kuma hospital (the Kuma group) showed that the mean age of patients did not differ significantly between the two groups (1.08 [0.99–1.16], p = 0.073, hereinafter the OR (CI) and p-value are indicated for multivariate analyses), but the proportion of male patients was significantly higher in the Fukushima group (2.28 [1.37–3.79], p < 0.002, Table 2 and Fig. 2).
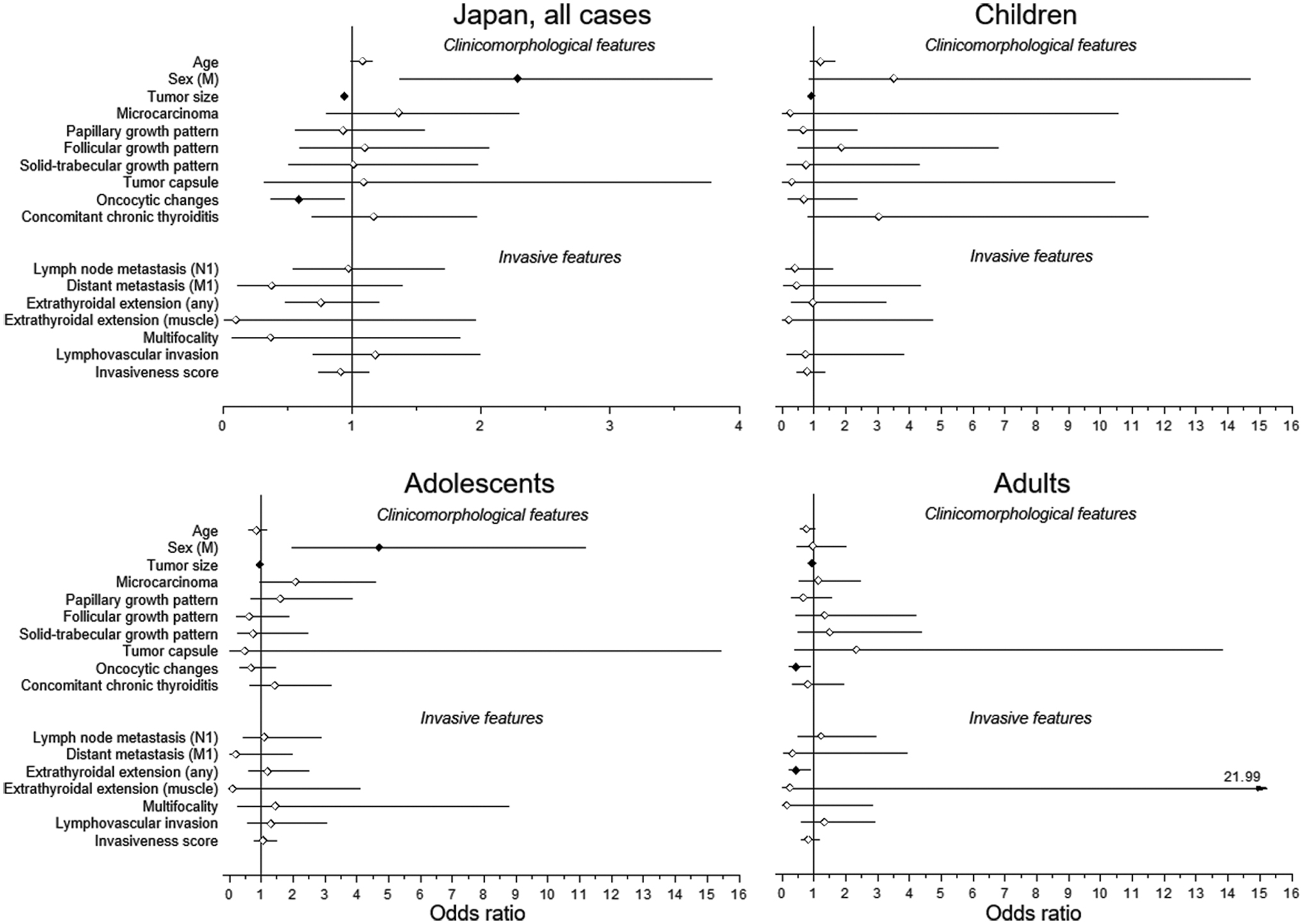
Clinicomorphological and invasive features of the Fukushima PTC in comparison with Kuma PTC. The odds ratios adjusted for age and sex are shown, the corresponding Kuma PTC (sub)groups were used as the reference. Filled symbols indicate statistically significant differences.
Characteristics of Kuma and Fukushima Papillary Thyroid Carcinoma
% For count data, median and interquartile range for continuous variables.
Adjusted for age and sex unless otherwise specified.
Adjusted for sex.
Adjusted for age, female sex was used as a reference.
Mann–Whitney test.
Fisher–Freeman–Halton exact test (for frequencies).
pT category according to the 7th edition of the TNM Classification of Malignant Tumors.
pT category according to the 8th edition of the TNM Classification of Malignant Tumors.
Invasiveness score included each instance of N1, M1, any extrathyroidal extension, multifocality or lymphatic/vascular invasion, either isolated or in combination with other(s).
The mean size of tumors in the Fukushima group was significantly smaller than in the Kuma group (0.94 [0.92–0.97], p = 3.00E-06). This was mostly due to the higher frequency of PTCs measuring 11–20 mm (3.51 [2.15–5.73], p = 5.20E-07), and the lower frequencies of PTCs sized 21–40 mm (0.25 [0.14–0.45], p = 3.00E-06) and 41+ mm (0.16 [0.04–0.71], p = 0.016) in the Fukushima group. The frequency of fully encapsulated tumors was generally very low in the whole Japanese series (below 4%) and was not significantly different across the groups (1.09 [0.32–3.78], p = 1.000). The frequencies of the dominant growth patterns and concomitant thyroid pathology did not differ significantly. Only the frequency of oncocytic changes in tumor cells of the Fukushima group was significantly lower (0.59 [0.37–0.94], p = 0.025).
According to the 7th edition of TNM classification, the frequency of PTCs of the pT1 category was significantly higher in the Fukushima group, namely T1b category (4.39 [2.48–7.78], p = 4.01E-07). In contrast, PTCs of pT2 category in the Fukushima group were significantly less frequent than in the Kuma group (0.22 [0.08–0.58], p = 0.002). The frequency of PTCs of the pT3 category in the two groups did not differ significantly (0.75 [0.47–1.19], p = 0.215), and the widely invasive tumors of the pT4 category were registered in 1.8% of cases only in the Kuma group (Table 2).
Reassessment of the Japanese PTCs according to the 8th edition of TNM classification did not principally change the findings with regard to the pT1, pT2, and pT4 categories, yet led to a significant decrease in the frequency of pT3 PTCs in the Fukushima group (0.15 [0.03–0.63], p = 0.010). Moreover, tumors of the T3b category were not seen in the Fukushima group (p = 0.018 on univariate analysis, although not significant on multivariate analysis, 0.10 [0.01–1.96], p = 0.127).
The frequency of regional metastases (pN1) was almost identical in both groups (∼80%, 0.97 [0.54–1.72], p = 0.907), while that of distant metastases to the lung (M1 category) was lower in the Fukushima group, but without statistical significance (0.38 [0.11–1.39], p = 0.145). No statistically significant difference was found for the invasiveness score between the two groups (0.91 [0.74–1.13], p = 0.400). The distribution of invasiveness score demonstrated a statistically significant downtrend in ORs of higher tumor invasiveness in the Fukushima group (-0.56 ± 0.07 [b ± SE], p = 0.016, Table 2).
Comparison of the Japanese PTCs in age-matched subgroups of Kuma and Fukushima cases
Comparative characteristics of tumors in the whole Kuma and Fukushima groups and in age-matched subgroups are presented in Figure 2; statistical details are shown in Supplementary Tables S4–S6.
The mean tumor size was consistently smaller in all Fukushima age subgroups (0.91 [0.85–0.98], p = 0.018 in children; 0.95 [0.91–0.98], p = 0.004 in adolescents, and 0.94 [0.90–0.98], p = 0.003 in young adults). There was a significantly higher frequency of PTCs sized 11–20 mm in the Fukushima subgroups (8.12 [2.07–31.78], p = 0.003 in children; 2.38 [1.10–5.13], p = 0.027 in adolescents, and 4.41 [1.95–9.94], p = 3.54E-04 in young adults), while tumors of larger sizes were less frequent, although without statistical significance.
Of note, no significant differences between Fukushima and Kuma PTCs other than for smaller mean tumor size and higher frequency of tumors measuring 11–20 mm were found in children aged ≤14 years at surgery. A few other statistically significant differences included the higher frequency of male patients in adolescents (4.70 [1.97–11.20], p = 4.80E-04), and the lower frequencies of oncocytic changes (0.43 [0.20–0.92], p = 0.029) and of any extrathyroidal extension (0.43 [0.20–0.91], p = 0.028) in adults from Fukushima.
In all age subgroups, there were no differences between Fukushima and Kuma PTCs in the distribution of tumors by the dominant growth pattern. In the Japanese PTCs, as in the Ukrainian PTCs, the dominant growth pattern largely corresponds to histological subtype/variant of PTC. Rare PTC subtypes such as DSV, Warthin-like, and tall cell were identified in a small number of cases. The DSV was observed only in children: in 2/42 of Kuma PTCs (4.8%) and in 2/15 of Fukushima PTCs (13.3%, p = 0.281). The Warthin-like variant was absent in the Fukushima group, but was found in 1/42 (2.4%) childhood and 1/118 (0.8%) adolescent Kuma PTCs (statistically nonsignificant differences). The tall cell variant was present in 1/42 (2.4%) of Kuma children, and in 4/118 (3.4%) of Kuma and in 2/44 of Fukushima adolescents (4.5%, p = 0.663). All rare PTC subtypes had a dominant papillary or solid-trabecular growth pattern.
The morphological features of tumor invasiveness did not reveal significant differences between Fukushima and Kuma PTCs in any age subgroup except for the lower frequency of any extrathyroidal extension in the Fukushima group of adult patients as mentioned above.
Generalization of findings in the Ukrainian and Japanese PTC series
To obtain an integrative view of the major associations in four PTC groups from two countries, we performed correspondence analysis, which is a statistical technique conceptually related to principal component analysis but intended to explore and graphically present relationships between categorical (qualitative) variables in a low-dimension plot (29). The results of this analysis (Fig. 3; cross-tabulation of the four PTC groups by their characteristics is presented in Supplementary Table S7) demonstrate a striking similarity between the Fukushima and Kuma PTCs of Japan. These tumors were apparently associating with the adolescent age of patients, absence of tumor capsule, and intermediate invasiveness.
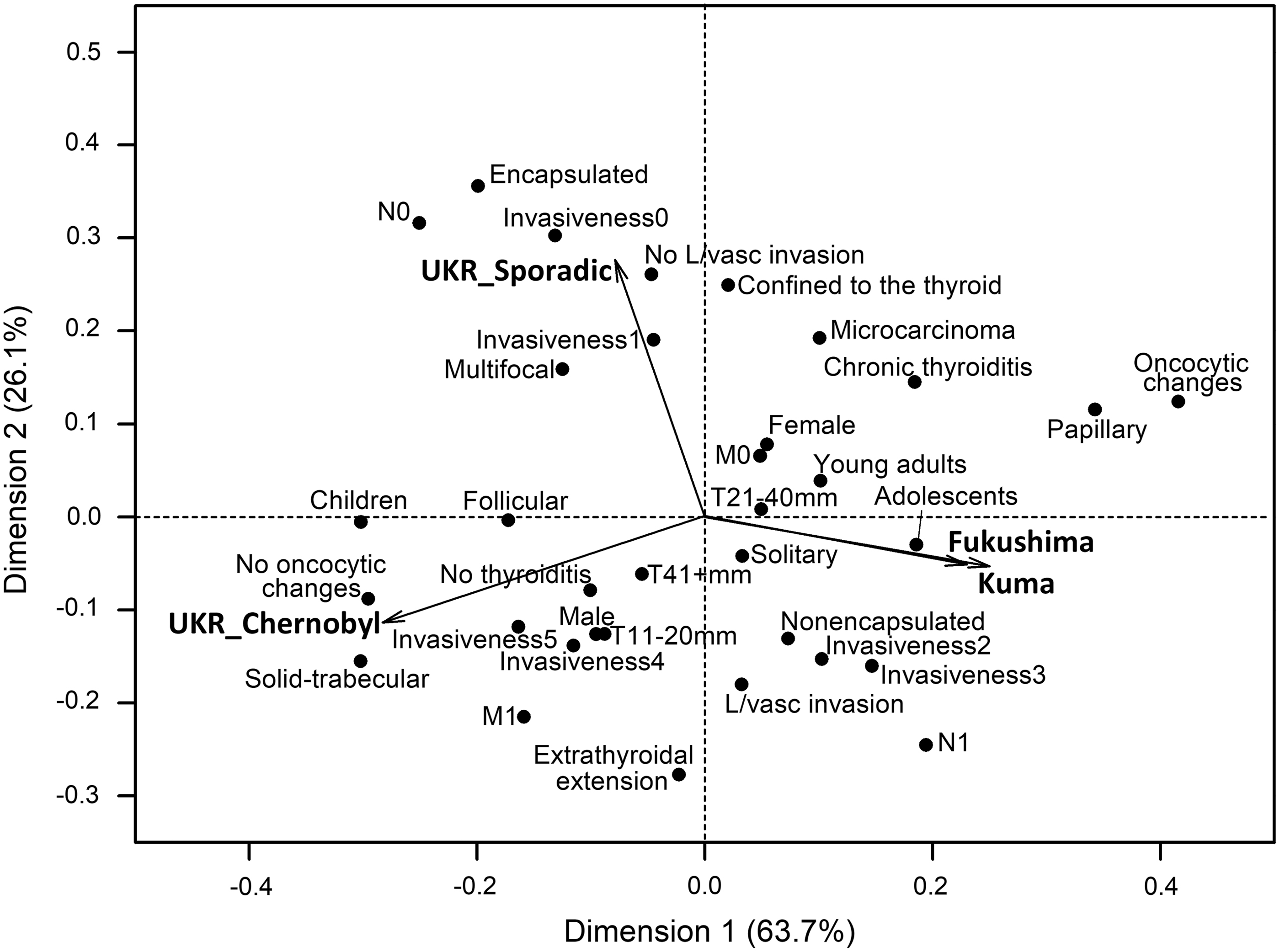
Correspondence analysis (29) of the association of PTCs of different etiology from Ukraine and of two groups from Japan with respect to major histopathological characteristics and tumor invasive features. One graphic output of correspondence analysis is a biplot, shown in the figure, that displays columns (here, the four PTC groups) in principal coordinates and rows (categorical clinicopathological variables) in contribution coordinates (Supplementary Table S8). Such coordinates enable to interpret the distance between row and column points as reflecting, to some extent, the association between them (e.g., Chernobyl PTCs display solid-trabecular growth pattern more frequently, while papillary growth pattern and oncocytic changes are less frequent; the Japanese PTCs are unlikely to be devoid of nodal disease and unlikely to be encapsulated). The distance between a point and the origin (“vector length”) is proportional to the discrimination ability of a given variable (e.g., variables extrathyroidal extension, encapsulation, solid-trabecular growth pattern, and oncocytic changes could be expected to have a strong discrimination ability). The smaller angle between the column points (when connected to the origin) indicates the stronger correlation, and right or obtuse angle indicates that the points are uncorrelated. Arrows are shown for the four PTC groups (column points) in the graph for easier visualization of angles between them (e.g., compare Fukushima and Kuma PTCs vs. Ukrainian Chernobyl and sporadic PTCs). For row points (i.e., clinicopathological characteristics), the smaller angle indicates similarity in response pattern (e.g., an invasiveness score 0 would be expected to frequently coexist with tumor capsule or N0 category). The number of dimensions retained in the present analysis is determined by the minimum of categories for either row (n = 34, Supplementary Tables S7 and S8) or column (n = 4) variables minus 1, thus 3; presented on the biplot are two major ones, Dimensions 1 and 2, which accounted for 89.8% of variance, and Dimension 3 accounted for the remaining 10.2%. Dimension 1 is mostly defined by morphological characteristics such as solid-trabecular and papillary dominant growth patterns, and the presence or absence of oncocytic changes. Dimension 2 is defined by tumor invasiveness: extrathyroidal extension, distant metastasis, and the absence of nodal disease and the presence of tumor capsule.
In contrast, the Ukrainian radiation-related and sporadic groups displayed marked differences in their characteristics, and furthermore, neither PTC group from Ukraine correlated with any of the Japanese PTC groups (note obtuse angles between those). Tumors in exposed patients were likely to be associated with a solid-trabecular growth pattern, absence of oncocytic changes, and higher invasiveness, whereas sporadic PTCs from Ukraine did not display obvious association with a particular growth pattern and appeared to be the least invasive. These observations are in line with the results of our statistical analyses presented above and suggest etiological resemblance of PTCs from the two Japanese groups, at variance with two PTC groups from Ukraine.
In addition, the differences in tumor invasiveness between the Ukrainian radiogenic and sporadic PTCs, and a lack of such in both Japanese PTC groups when either multivariate statistical analyses or correspondence analysis was used, prompted us to further investigate this issue. Besides the analysis of each individual feature of tumor aggressiveness, we also used the “invasiveness score,” which included each instance of any invasive feature, either isolated or in combination with other(s) within a tumor.
Of interest were the trends in ORs for different invasiveness scores in the tumors from the two countries (Tables 1 and 2). There was a principal difference in the chance of observing tumors with the higher invasiveness scores between the radiogenic versus sporadic Ukrainian PTCs and Fukushima versus Kuma Japanese PTCs. As illustrated in Figure 4, an apparent uptrend in the odds ratios for increasing invasiveness score was seen in the Ukrainian series, and, in contrast, the downtrend occurred in the Japanese PTCs; the difference in slopes was statistically significant (p = 1.69E-05). This finding underscores the difference between the comparative aggressiveness of the Chernobyl and Fukushima PTCs.

Odds ratio changes by invasiveness score display the opposite trends in the Ukrainian and Japanese PTC series. Country-specific ORs adjusted for age and sex (see Tables 1 and 2 for Ukraine and Japan, respectively) were linearly regressed on the invasiveness score, and the slopes were compared using Satterthwaite degrees of freedom parameter in the Welch's t-test (42,43).
Discussion
Here, we performed a comparison of PTCs from Ukraine and Japan using a unified set of morphological features of tumor architecture and invasive properties to determine whether the pathological scenario of radiation-related carcinogenesis in Ukraine after the Chernobyl accident could or could not be seen in Japan after the nuclear accident in Fukushima.
Our analyses demonstrated that Ukrainian radiogenic PTCs significantly differed from sporadic PTCs. Radiation-related tumors had a solid-trabecular growth pattern and displayed morphological features of aggressive biological behavior such as extrathyroidal extension, and regional and distant metastasis more frequently than sporadic ones. It should be noted that sporadic cases were not detected by active screening, and therefore, their lower aggressiveness could not be ascribed to early cancer detection. Overall, our findings are consistent with previous pathological analyses of Chernobyl PTC in Ukraine and Belarus (6 –9,30 –33). In our present and earlier studies, the differences in tumor architecture and invasive properties were seen in radiogenic PTC, compared with sporadic PTC in Ukraine, not only in children but also in older age groups, although to a lesser extent (8,9) (Table 1, Fig. 1, and Supplementary Tables S1–S3).
In contrast, Fukushima PTCs showed very few significant differences in clinicomorphological characteristics and invasive features from the Kuma tumors, either on the whole group comparison or in age-matched subgroups (Table 2, Fig. 2, and Supplementary Tables S4–S6). The two differences deserve particular attention. First, the mean size of Fukushima PTC was smaller than that of tumors from Kuma hospital, and the frequency of pT1 tumors was higher. The likeliest explanation would be the early detection of thyroid nodules during the large-scale TUE in Fukushima Prefecture, which is not the case in the Kuma group. The high frequency of smaller tumors has been repeatedly shown in several screening studies (34 –37).
Second, there was a higher frequency of male patients in the Fukushima group; 36.5% versus 19.3% in Kuma. We again ascribe this to ultrasound screening when a target population is examined regardless the sex or other (applicable) conditions. While clinically apparent PTC is more common in female patients, an overview of autopsy studies indicates the lack of sex disparity in the frequency of small tumors measuring 1–1.5 cm without a pronounced overall age-related difference in the prevalence rate (38). It is therefore possible that the female:male ratio of 1.7:1 among Fukushima patients may represent the real sex ratio in young patients with PTC nodules in the population, which is half the average of 3.7:1 seen in the cancer registries in Japan (ICD-10 C73, age at diagnosis 5–29 years, data for 1985–2012) (39).
With regard to the morphological features of tumor aggressiveness, it should be noted that in 2017, the criteria for assigning well-differentiated thyroid carcinomas the pT3 category were revised in the 8th edition of TNM classification (26). Accordingly, tumors larger than 40 mm without extrathyroidal extension belong to the pT3a category. The new pT3b category includes tumors of any size, but only if there are signs of tumor invasion into the strap muscles.
In the series under study, when the 8th edition of the TNM classification was applied, 80 radiation-related and 38 sporadic Ukrainian PTCs, and 47 Fukushima and 87 Kuma PTCs migrated from the pT3 to the pT1 or pT2 categories (Tables 1 and 2). Since in our previous works on Chernobyl or Fukushima thyroid cancer we used the 7th edition of TNM classification (7,9,18,20), in the present study, we provided pT categories for both the 7th and the 8th TNM classifications, and used the term “extrathyroidal extension (any)” to assess not only gross tumor invasion but also extension into the fat and connective tissues surrounding the thyroid.
The difference in tumor invasiveness between the Ukrainian radiogenic and sporadic PTCs and the lack of similar difference between Fukushima and Kuma PTCs of Japan might be related to tumor biology. Although the molecular analysis of tumors could not be performed in this study, the results of previous works may suggest an explanation for such a difference.
The radiogenic Chernobyl PTC in young patients was characterized by a significantly higher frequency of fusion oncogenes than that in sporadic PTC in the age-matched but relatively small study of patients from Ukraine (40). The genetic profile of Fukushima PTC, on the contrary, is largely associated with BRAFV600E mutation (15), whose frequency is comparable with that in sporadic PTC from young patients from Japan (41). In view of the differences in molecular profiles, it is plausible to suggest that fusion oncogene drivers may confer higher tumor aggressiveness than point mutation in young patients, although this might be further modified by different dietary iodine consumption (or other environmental factors) and distinct genetic background between patients from the two countries.
The clinical relevance of our findings should be considered in the context of PTC in young individuals. The Ukrainian series demonstrates that PTC in young patients with a history of radiation at childhood age may potentially be more aggressive, especially in prepubertal individuals. This knowledge has major implications for disease evaluation, choice of more extensive therapy, and long-term management of patients from the high-risk group.
Observations in the Japanese PTCs provide valuable insights regarding tumors detected by active screening of individuals whose history of radiation exposure is unclear or questionable. Our data indicate that such tumors may be smaller in size, in line with early cancer detection by screening. However, it is important to note that despite the smaller size, morphological features of tumor aggressiveness did not appear to be less frequent in Fukushima patients. Indeed, regional metastasis was observed in about 80% of both Kuma and Fukushima patients, extrathyroidal extension in some 40–50%, and lymphovascular invasion in about 70% being quite close. While an individual risk in young patients diagnosed with PTC due to screening may vary from low to high, our data suggest that clinical strategies toward such patients should not be generally different from those used for nonscreened PTC patients.
Our study has certain strength and limitations. With regard to the Ukrainian series, both radiogenic and sporadic cases were selected from a single institution (IEM) and were well matched by the place of residence and age at operation. We also managed to create an appropriate group of nonexposed patients from Japan. Ideally, these would also be residents of Fukushima Prefecture, but the relatively short time after the accident at the Fukushima Dai-ichi nuclear power plant and low incidence of thyroid cancer in the young population precluded such a study design. On the other hand, inclusion of patients who lived in the Prefectures other than Fukushima is a good reason to consider those nonexposed to additional environmental radiation.
While neither Ukrainian nor Japanese patients were not matched on sex, statistical models were appropriately adjusted to avoid confounding. A uniform protocol of pathological assessment of PTCs is also a strength of the current study. Limitations of the study stem from differences in times of diagnoses both in the Ukrainian and the Japanese PTC series: it could not be ruled out that some observations may be due, in part, to period or birth cohort effects. Also, we acknowledge that a large number of statistical tests were performed; therefore, some statistically significant findings should be considered with caution.
In conclusion, the Ukrainian radiogenic PTC, when compared with sporadic PTC in young patients, was characterized by the differences in tumor growth pattern and higher frequency of pathological features of tumor aggressiveness. PTCs detected during two cycles of TUE after the Fukushima accident did not display significant differences from those diagnosed in young patients from other Prefectures of Japan, neither in terms of tumor morphology nor in invasive characteristics. A significantly smaller mean tumor size and the higher frequency of male patients in the Fukushima group likely reflect the effect of mass ultrasound screening. Our study demonstrates the differences in morphological features of biological behavior of PTC diagnosed after the Chernobyl and Fukushima radiation accidents, suggesting a nonradiogenic etiology of the latter.
Footnotes
Acknowledgments
The authors acknowledge the commitment of the staff of the Laboratory of Morphology of Endocrine System and the staff of the Department of Surgery of Endocrine System of IEM; the staff of the Departments of Diagnostic Pathology and of Thyroid and Endocrinology of FMU; and the staff of the Departments of Diagnostic Pathology and of Surgery of Kuma Hospital who prepared the pathological material for the study and operated on the patients. They gratefully acknowledge the confirmation of Ukrainian diagnoses provided by the International Pathology Panel of the Chernobyl Tissue Bank: Professors A. Abrosimov, T. Bogdanova, G. Fadda, J. Hunt, M. Ito, V. Livolsi, J. Rosai, E.D. Williams, and Dr. N. Dvinskyh, and Japanese diagnoses provided by the members of the Fukushima Pathology Consensus Panel: A. Sakamoto (Chairman), M. Hirokawa, M. Ito, H. Naganuma.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported, in part, by KAKENHI Grant Number 19KK02670001 from the Japan Society for the Promotion of Science and intramural funding from the Atomic Bomb Disease Institute of Nagasaki University.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8