
Abstract
Background:
The prescription of liothyronine (LT3) to treat hypothyroidism is increasing worldwide; however, the long-term safety of LT3 use has yet to be determined. Previous studies have suggested a possible association between LT3 use and breast cancer. The aim of this study was to examine the effects of LT3 use on cancer incidence and mortality.
Methods:
Our sample included the full adult population of individuals living in Sweden with at least three purchases of thyroid hormone therapy between July 2005 and December 2017. Individual-level data on drug purchases were linked to registry data on cancer incidence and mortality. There were 575,461 individuals with at least three purchases, of which 11,147 had made at least three purchases of LT3, including combinations of levothyroxine (LT4) and LT3. Individuals were followed for a median follow-up time of 8.1 years. We applied Cox regression with a time-varying exposure variable, comparing LT3 users (individuals with at least three cumulative purchases of LT3) with LT4-only users (the rest). Outcomes included breast cancer incidence, any cancer incidence, all-cause mortality, any cancer mortality, and breast cancer mortality. We adjusted for age, sex, previous thyroid cancer, previous other cancer, use of antithyroid preparations, use of sex hormones, and dose in multivariate analyses.
Results:
Multivariate analyses produced a hazard ratio of 0.93 (95% confidence interval [0.75–1.15]) for breast cancer incidence (only females), 0.97 (0.87–1.08) for any cancer incidence, 0.69 (0.61–0.77) for all-cause mortality, 0.78 (0.62–0.98) for any cancer mortality, and 0.91 (0.50–1.66) for breast cancer mortality (only females).
Conclusions:
In this large, Swedish, long-term registry-based study, the use of LT3 did not lead to increased breast cancer incidence, any cancer incidence, all-cause mortality, any cancer mortality, or breast cancer mortality compared with LT4 use. Somewhat surprisingly, there was evidence of lower mortality in LT3 users in models adjusting for dose, potentially an artifact of underlying associations between dose and health status/diagnosis.
Introduction
Hypothyroidism is a common disease affecting ∼5% of the population and is more common in females (1). The standard treatment for hypothyroidism is levothyroxine (LT4), and the disease is monitored by assessing the levels of thyrotropin (2,3). Although the majority of patients feel well with LT4 treatment, approximately 10–15% of patients report persisting hypothyroid symptoms despite normal laboratory tests (4 –6). LT4 treatment results in relatively higher normal levels of free thyroxine (T4) and relatively lower levels of free triiodothyronine (T3) than in euthyroid subjects without treatment (7,8), but the clinical relevance of this finding is unclear. It has been proposed that there is individual variation in the ability to transport LT4 and synthesize T3 from LT4 in peripheral tissues, possibly leading to intracellular hypothyroidism and incomplete reduction of symptoms after LT4 treatment. In theory, these symptoms could be relieved by adding the synthetic form of T3, liothyronine (LT3), to LT4 treatment. To date, at least 12 randomized controlled trials have examined the effect of combined LT4/LT3 treatment with varying results (9 –20). Five systematic reviews/meta-analyses concluded that the combined treatment was not superior to standard LT4 treatment with respect to persisting hypothyroid symptoms and quality of life (21 –24) or patient preference (25). Therefore, international guidelines consider LT3 treatment to be experimental (2,3). However, when letting the patient blindly choose treatment, most patients chose combined treatment in some (9 –13), but not all, studies (14,16).
Many unscientific claims of the positive effects of LT3 treatment are available, resulting in an increasing number of patients requesting treatment with LT3, typically in combination with LT4 (26). As a consequence, the amount of LT3 prescriptions has increased dramatically worldwide, including in Sweden. Defining users based on having made at least three purchases of a type of drug (drugs containing LT3 and drugs not containing LT3) during the year of interest, in Sweden, in 2006, there were 723 LT3 users and 257,078 LT4-only users; and in 2017, there were 5342 LT3 users and 375,073 LT4-only users (27). Nevertheless, in addition to the lack of consistent evidence of direct benefits, the potential long-term effects of LT3 treatment are also largely unknown. Meta-analyses have not been able to show evidence of differential morbidity between patients treated with LT3 and patients treated with LT4; however, the study period in any of the included individual studies did not exceed 12 months (21 –24). The only long-term study evaluating side effects of the LT3 treatment used data from Scotland and did not show an increased incidence of fractures or heart disease. However, an increased risk for breast cancer was observed with borderline significance (28). The possible association of LT3 treatment with breast cancer is of great concern as there have been previous reports suggesting such an association in both experimental (29,30) and clinical studies (31 –33).
The aim of this study was to examine the possible association of LT3 treatment with breast cancer incidence, any cancer incidence, all-cause mortality, any cancer mortality, and breast cancer mortality in a large, Swedish registry dataset.
Materials and Methods
The data were obtained from three different official registries maintained by the Swedish National Board of Health and Welfare (Socialstyrelsen). Specifically, data were extracted for the entire Swedish population of individuals aged 18 years and older with at least three prescriptions of thyroid hormone replacement therapy and with no history of breast cancer at the point when they obtained their first prescription. The registries were linked through personal identifiers.
The Prescribed Drug Registry (Läkemedelsregistret) provided information on all prescribed drugs dispensed at pharmacies in Sweden between July 2005 and December 2017. The data included age, sex, ATC code (H03AA, H03B, G03 with subgroups), date of purchase, number of tablets, and dose per tablet.
Patients with at least three records of obtaining drugs containing LT3 or combination treatments were classified as LT3 users from the point when their third drug containing LT3 or a combination treatment was obtained. Moreover, patients with at least three records of obtaining drugs containing
Drugs containing antithyroid preparations (H03BA-X) and sex hormones (G03A-X) were also identified; individuals were recorded as users of these if they had ever obtained a drug of the corresponding type at baseline.
The Cancer Registry (Cancerregistret) provided information on all newly detected cancer cases in the country between January 2005 and December 2017, including diagnoses (coded with the ICD-10 classification), date of diagnosis, and TNM classification (size or direct extent of primary tumor, degree of spread to regional lymph nodes, and presence of distant metastasis). For each patient, the first incidence of cancer (ICD codes C00-D48) as well as the first incidence of breast cancer (ICD code C50) was extracted. We also conducted an analysis of cancer incidence only including severe cases: T3/T4 (large extension of the primary tumor), N1/N2/N3 (large degree of regional lymph node involvement), and M1 (metastasis to distant organs).
The Cause of Death Registry (Dödsorsaksregistret) provided information on dates of all deaths and their causes (coded with the ICD-10 classification) spanning from July 2005 to December 2019.
Individuals were followed from baseline until death, other event of interest (first cancer or first breast cancer diagnosis, depending on the analysis), or the end of 2017. Analyses of cancer excluded patients with an observed cancer (of the type of interest) before baseline. Furthermore, analyses of breast cancer only included females. For other mortality and incidence outcomes, analyses were carried out for males and females combined as well as for males and females separately. In a sensitivity analysis, all analyses were also carried out omitting individuals with a history of thyroid cancer.
Means and standard deviations (SDs) are reported for continuous variables, except for the asymmetric variables, follow-up time and dose, for which instead median and interquartile range (IQR) are reported. For binary variables, proportions are reported. Cox proportional hazards (PH) regression models were applied with a time-varying treatment variable, while controlling for other covariates and time since baseline. The PH assumption was tested using Schoenfeld residuals; variables not fulfilling the PH assumption were accounted for through stratified Cox regression rather than by standard adjustment.
The intensity of treatment (i.e., dose) could differ between LT3 and LT4-only users, and it may thus be desirable to adjust for this variable. Previous literature has established a therapeutic substitution of 1:3 of LT3 for LT4 (34), and we therefore calculated an average equivalent dose per day, according to the following equation:
For individuals switching from LT4-only to LT3 user, the calculation was done separately for the two time periods; dose was thus used as a time-varying variable. Indeed, for LT4-only users, the above equation simply yields the average LT4 dose over the present time period. Quintiles of dose, as defined above, were created and entered into the regressions. It was not possible to follow individuals who were in the Prescribed Drug Registry before July 2005. For this reason, a sensitivity analysis was carried out, including only new users beginning their treatment in July 2006 or later.
Finally, while the focus of our study was to compare LT4 treatment and LT3 treatment, it is possible that these therapies could have some effects on the outcomes considered regardless of whether LT3, LT4, or a combination is used. While we had no access to individual-level data on the full population, the National Board of Health and Welfare publicly provides data that are aggregated at the sex, age, and year levels. This allowed us to compare incidences in our data with those in the population, reweighted to match our data with respect to sex, age group (5-year intervals), and year. The study was approved by the Swedish Ethical Review Authority (Dnr: 2019-01824).
Results
We identified 575,461 individuals with at least three purchases of thyroid replacement hormones, who thus constituted the study sample. Of these, 573,928 individuals were identified as LT4-only users and 11,147 were identified as LT3 users (Table 1). Notably, most individuals recorded as LT3 users (9614) were also recorded as LT4-only users before initiating their usage of LT3. The total follow-up time was 4,302,121 person-years, with a median of 8.1 years per person (IQR 3.7–11.7) and a maximum of 12.5 years. LT4-only users were followed for 4,256,204 years in total, with a median of 8.0 years (IQR 3.7–11.7); LT3 users were followed for 45,917 years in total, with a median of 2.9 years (IQR 1.3–6.5). LT3 users were notably younger than LT4-only users; the average age of LT4-only users at baseline was 58.6 years (SD 18.3), whereas the average age of LT3 users was 45.9 years (SD 13.3).
Descriptive Statistics
Restricted to women.
Individuals using combined LT4 and LT3 preparations (n = 575) were omitted from this analysis.
IQR, interquartile range; SD, standard deviation; LT3, liothyronine; LT4, levothyroxine.
Only considering new users of LT3 or LT4 (individuals with no recorded usage between July 2005 and June 2006) reduced the number of individuals by 44% and reduced the total follow-up time by 58%. In this subsample, the median follow-up time was 5.3 years for LT4-only users (IQR 2.4–8.5) and 2.5 years for LT3 users (IQR 1.2–5.1). The average age was 54.4 years in LT4-only users (SD 18.6) and 44.7 years in LT3 users (SD 13.2).
In regressions applied to the full sample (Table 2), univariate models suggested that being a LT3 user was associated with a lower risk of breast cancer, any cancer, mortality from breast cancer, mortality from any cancer, and all-cause mortality (p-values generally <0.001). The results were similar when considering males and females separately. However, in models that accounted for age and other variables, the estimated hazard ratios (HRs) approached one and were never significantly different from one at the 5% level. The final model, also adjusting for dose, produced lower estimates, with statistically significant protective effects of LT3 on cancer mortality as well as on all-cause mortality (except for males). For males and females combined, the HR was estimated to be 0.78 (confidence interval, CI [0.62–0.98], p = 0.03) for cancer mortality and 0.69 (CI [0.61–0.77], p = 0.00) for all-cause mortality.
Effects of Being a LT3 User on Cancer Incidence and Mortality in All Users
HRs estimated from Cox regression models. Ninety-five percent confidence intervals are given in brackets. Adjusted models accounted for age and sex through stratification and used standard adjustment to account for history of thyroid cancer, history of other cancer, usage of antithyroid preparations, and usage of sex hormones at baseline.
HR, hazard ratio.
Restricting the analysis to new users of thyroid replacement hormones, results (not shown) trended in the same direction; however, due to reduction in the sample size, these results were somewhat less precise. Moreover, omitting individuals with a history of thyroid cancer made virtually no difference for our estimates (results not shown).
Results for cancers with more extensive spread (Table 3) showed similar results. In unadjusted models, LT3 was strongly protective, but this tendency became weaker in adjusted models (where only the effect on tumors of extensive spread remained significant at the 5% level). In models also adjusting for dose, there was no evidence of LT3 having any effect at the 5% level.
Effects of Being a LT3 User on Severe Cancer Incidence
Both sexes are included. HRs estimated from Cox regression models. Ninety-five percent confidence intervals are given in brackets. Adjusted models accounted for age and sex through stratification and used standard adjustment to account for history of thyroid cancer, history of other cancer, usage of antithyroid preparations, and usage of sex hormones at baseline. Severity is determined according to the TNM classification system.
Figure 1 presents fully adjusted survival curves for the outcomes considered in this article (all curves except those pertaining to breast cancer were estimated based on all individuals; those for breast cancer were restricted to females). In line with the estimates previously presented, LT3 users tended to have fewer adverse outcomes compared with LT4-only users, a conclusion that holds regardless of the follow-up period. Table 4 displays the number of observed individuals in the two treatment groups that were observed at different follow-up times. Since treatment is a time-varying covariate and since most individuals start out as LT4-only users, the number of individuals observed as LT3 users initially increases by follow-up time.

Survival plots, fully adjusted. The graphs show estimated probability of survival (or event-free time) in a female of average age and with average dose, with zeros on all other explanatory variables. (
Number of Individuals Observed at Different Follow-Up Times, Displayed by Analyzed Outcome and Treatment Group
LT4 is the number of observed LT4-only users and LT3 is the number of observed LT3 users.
We further compared outcomes in our data (all users of thyroid preparations) with those in the general population, reweighted to match our data with respect to sex, age group (5-year intervals), and year (Fig. 2). The results suggested a somewhat lower incidence of breast cancer in our sample (incidence rate 0.94 among females when comparing the datasets), a higher incidence of any cancer (1.12), and similar incidences of breast cancer mortality (1.03 among females), cancer mortality (1.02), and all-cause mortality (1.02).
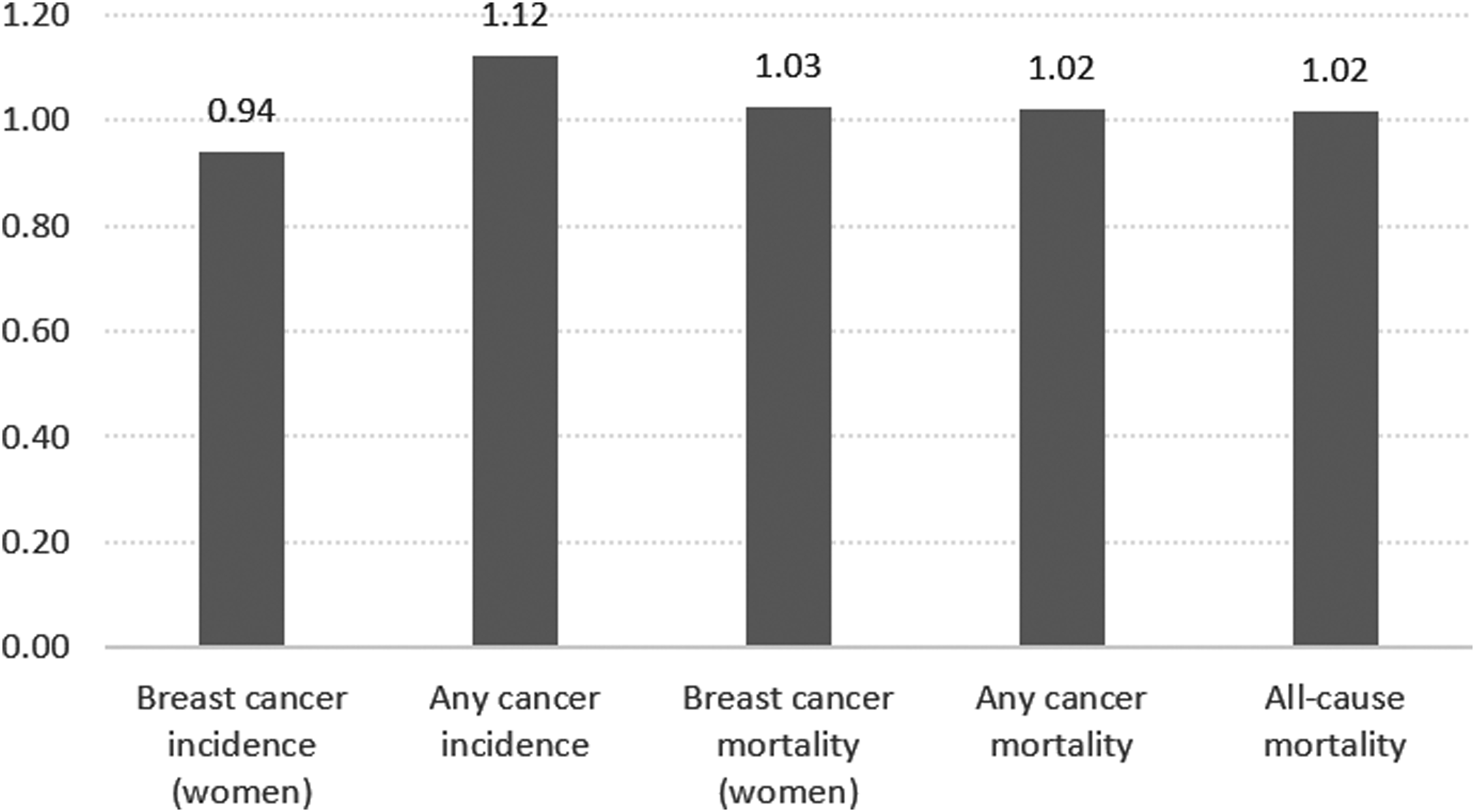
Mortality and incidence rate ratios for different outcomes in our data versus the general population (reweighted by age and sex to match our data).
Discussion
Few studies have examined the morbidity and mortality of individuals on long-term LT3 treatment. In this large, long-term registry-based study, including the full adult Swedish population on thyroid hormone replacement therapy, we did not observe any increase in breast cancer incidence, any cancer incidence, all-cause mortality, any cancer mortality, or breast cancer mortality in individuals using LT3 compared with LT4-only treatment. These results were similar after correcting for possible confounders. There was evidence of lower mortality in LT3 users in models adjusting for dose.
Other than the aforementioned Scottish study (28), this is the first study examining associations between LT3 treatment, cancer, and mortality. Interestingly, thyroid hormones have previously been of great concern in cancer research, mainly as potential accelerators of cancer cell proliferation in certain cancer types. However, the results of previous studies have been inconclusive [reviewed by Krashin et al. (35)]. Regarding breast cancer, several reports have suggested associations between endogenous T3 levels and breast cancer. In large, Swedish prospective studies, higher endogenous T3 levels were associated with an increased risk of breast cancer in postmenopausal women (31), breast cancer-specific mortality (32), and poorer prognostic factors such as larger tumors, the occurrence of lymph node metastasis, and negative estrogen receptor and progesterone receptor status (33). In experimental studies, T3 exhibited an estrogen-like effect in breast cancer, binding to the estrogen receptor and enhancing breast cancer cell proliferation (29,30). Therefore, the finding of a possible association of breast cancer with LT3 use in the Scottish study has been a major concern (28). Fortunately, our study does not support such a finding. In the Scottish study, the association of LT3 use and breast cancer was of borderline significance and not related to the number of prescriptions, thus raising doubts about a causal relationship. Considering the size of our study, we feel confident in concluding that there is no excess cancer risk and mortality in LT3 users compared with LT4-only users, at least not over the follow-up period considered.
Somewhat surprisingly, there was evidence of lower mortality in LT3 users in models adjusting for dose. While adjusting for dose is potentially relevant if doses differ systematically across LT4-only and LT3 users, there is also a notable drawback. Most likely, dose is not only influenced by whether an individual is a LT3 user but also by (unobserved) diagnostic status. That is, dose is a collider, and adjusting for it may yield a noncausal association between LT3 usage and diagnostic status. If, in turn, diagnostic status is related to the outcome of the study, adjustment for dose may yield a noncausal association between LT3 usage and the outcome (36,37). Results adjusted for dose do therefore need to be interpreted with caution.
Our study is subject to some limitations, the main limitation being the lack of laboratory data. In Sweden, the only available LT3 preparation that does not need individual approval by the Swedish Medical Products Agency contains 20 μg LT3. Many patients need smaller doses, such as 5 and 10 μg. Therefore, patients often divide their tablets themselves, possibly leading to unstable levels of T3. Combined treatment is considered more difficult to manage by many physicians than LT4 treatment alone. Thus, one can speculate that LT3 users had abnormal thyroid tests compared with LT4-only users, which would exaggerate the possible adverse outcomes. Another important drawback is the lack of clinical data such as the underlying cause of hypothyroidism, body–mass index, or smoking status, all of which can have an impact on cancer incidence, severity, and mortality. Our study had no data on compliance; however, given the size of our population, it is unlikely that this would have influenced our results. Another limitation of our study is the relatively short follow-up time for LT3 users, which introduced some uncertainty in interpretation of the mortality data and data on cancers with slower growth. There is still a possibility that smaller differences between study groups would become apparent with a longer follow-up time.
The majority of randomized controlled trials have shown no overall benefit of combined treatment compared with LT4 treatment alone, a conclusion that is supported by five meta-analyses (21 –25). Nevertheless, there is (worldwide) a group of patients who remain dissatisfied with their LT4 treatment despite normal laboratory tests, and a subgroup of these patients report benefits from combination therapy (3). An increasing number of patients ask their physicians for a prescription of combination therapy, often causing tensions. Thus, the question of whether combination therapy does any harm to patients is crucial. Our data provide reassuring evidence regarding the risk of cancer and mortality. However, there could still be other health risks associated with LT3 therapy not examined in this study, such as an increased incidence of psychiatric disorders (28). The cost-effectiveness of the combined treatment also remains an issue as it is more expensive than LT4 treatment alone (38) and usually requires more frequent laboratory testing.
Comparing the outcomes in users of thyroid hormone preparations and the general population, we observed a lower incidence of breast cancer in females, a higher incidence of any cancer, and similar incidences of mortality. No clear conclusion can be drawn based on these results regarding the general effect of thyroid hormone preparations on cancer or mortality.
In conclusion, this study did not identify any increase in breast cancer incidence, any cancer incidence, all-cause mortality, any cancer mortality, or breast cancer mortality between individuals using LT3 and LT4 treatments. In dose-adjusted models, we find strong relationships between dose and mortality outcomes, suggesting that dose may be related to the underlying health status. Our study contributes to current knowledge on the risk-to-benefit ratio of LT3 treatment.
Footnotes
Acknowledgment
The authors thank Professor Håkan Olsson for valuable advice.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from Lundgrens Stiftelse and SUS fonder.