
Abstract
Background:
Iodine-induced hyperthyroidism (IIH) was a common issue in the early twentieth century after introduction of iodine supplementation in dietary salt. Currently, IIH is mostly encountered in Western countries as a consequence of radiographic procedures involving the administration of iodinated contrast media (ICM). However, little is known about the magnitude and clinical relevance of this issue. To assess the incidence of hyperthyroidism after ICM exposure, we performed a systematic review and meta-analysis of the literature.
Methods:
MEDLINE, Embase, and the Cochrane Library were systematically searched for studies published between 1946 and May 2018. Studies were considered eligible if they investigated the association between hyperthyroidism and iodinated contrast. Data on study design, baseline characteristics, and outcomes were extracted independently by two reviewers.
Results:
Thirty out of 1493 retrieved studies were included in the analysis. The time endpoint to assess thyroid hormone levels after ICM exposure varied between 1 and 541 days among studies, with most studies having a time endpoint between 7 and 56 days. The overall estimated prevalence of overt hyperthyroidism after ICM exposure was extremely low (0.1% [confidence interval, CI 0–0.6%]), and did not change after adjustments for baseline thyroid function status (0.3% in euthyroid patients at baseline [CI 0–1.7%]). There were no cases with overt hyperthyroidism at 7 days after ICM exposure, and the incidence was very low at 30 days (0.2% [CI 0–0.8%]).
Conclusion:
The incidence of IIH after ICM administration during radiographic procedures is extremely low.
Introduction
Iodine is an essential micronutrient in the synthesis of thyroid hormones. Its recommended daily allowance (RDA) by the World Health Organization (WHO) is 150 μg for nonpregnant adults; of this amount, about 80 μg are necessary to maintain adequate thyroid hormone production, the remainder accounts for fecal and urinary losses (1). Iodine is predominantly present in its organically bound form, but it occurs in many oxidation states including iodide (I−), which is most commonly encountered as a component of iodized salt. Iodide is trapped and actively concentrated by the thyroid gland through the sodium–iodine symporter (NIS) and is essential for the synthesis of the thyroid hormones, triiodothyronine (T3), and thyroxine (T4).
Exposure to high amounts of iodine causes an acute inhibitory effect on the synthesis of thyroid hormones. This phenomenon was first described in 1948 and is known as the “Wolff–Chaikoff effect.” It is normally followed by resumption of normal thyroid function within 2 days (2). An impairment of the acute Wolff–Chaikoff effect is typically observed in individuals with latent Graves' disease or autonomous thyroid nodules (3). The incidence of focal autonomy increases with age and is higher in areas with iodine deficiency; these individuals may develop iodine-induced hyperthyroidism (IIH) when exposed to higher amounts of iodine because the increase in substrate results in the excessive synthesis and release of thyroid hormones by the autonomous tissue, a mechanism referred to as Jod-Basedow phenomenon (4).
IIH was commonly observed shortly after introduction of iodine prophylaxis in deficient areas (e.g., up to 7% in Sweden after initiation of iodination programs), but its incidence has decreased during the past decades (5). However, IIH can still represent a medical issue secondary to the administration of high doses of iodine associated with the administration of iodinated contrast agents for radiographic procedures. It has, for example, been estimated that 80 million doses of iodinated contrast media (ICM) were administrated worldwide in 2005 (6). Whereas patients with Graves' disease and focal autonomy are thought to be at higher risk for developing hyperthyroidism after ICM administration, IIH has been described even in patients without prior thyroid dysfunction and with an apparently normal thyroid gland, although the pathophysiological mechanism in this situation remains unclear (5).
In commonly used radiographic contrast media, the content of organic iodine ranges from 300 to 370 mg/mL, with higher contents in low-osmolar compared with high-osmolar agents. Low- and iso-osmolar agents are preferred in patients with impaired renal function, as the risk of contrast-induced nephropathy is reduced (1). The usual amount of ICM administered during a computed tomogram (CT) scan is 50–100 mL, equivalent to 15–37 g of iodine, which exceeds the RDA hundred thousand times (7). A fraction of the organoiodine is subject to deiodination, thus resulting in substrate for NIS and explaining the high urinary iodine concentration found in patients several weeks after ICM administration.
The prevalence of IIH varies widely between 0.05% and 5% among studies (8). This variability is explained by the heterogeneity of the study design of published studies and the variability in nutritional iodine intake. Moreover, most prospective studies only included small numbers of patients. As the number of radiographic procedures involving ICM grows steadily, it is of importance to get a more precise estimate of the prevalence, severity and clinical impact of IIH, and to identify which subjects may be at risk for IIH. For these reasons, we performed a systematic review and meta-analysis of the literature to investigate the prevalence of hyperthyroidism after administration of iodinated contrast agents for radiographic procedures.
Methods
A systematic review of published data according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement for the conduct of meta-analyses (9) was performed to estimate the prevalence of IIH after the administration of ICM for radiographic procedures. Human subjects or the public were not involved in any way in our study.
Eligibility criteria
All original studies containing data about ICM-induced hyperthyroidism were eligible for inclusion. Exclusion criteria were case reports, letters, editorials and reviews, studies conducted on animals, subjects <18 years of age or on pregnant women, articles with only abstract available, duplications of articles, articles written in a language not known to the two reviewers (i.e., other than English, German, Italian, and French), and articles on hyperthyroidism induced by other sources of iodine than iodinated radiographic contrast (i.e., iodine nutrient supplements and iodized salts).
Search strategy and study selection
We conducted a literature search in MEDLINE (Supplementary Appendix SA1), Embase, and the Cochrane library for studies published between 1946 and May 2018. Search terms were “hyperthyroidism,” “thyrotoxicosis,” “thyroid (dys)function,” “thyroid autonomy,” “urinary iodine” AND “iodine-induced,” “iodinated contrast (media),” “ICM,” “radiographic procedures/contrast,” “contrast-induced,” “computed tomogram,” “CT scan” or “coronary angiography.” The search was done without language restriction; however, we considered only studies written in languages known by the two reviewers.
After abstract screening and retrieval of potentially eligible studies, the full-text articles were assessed for eligibility. References of the retrieved articles were manually scanned to identify additional relevant publications. Duplicate studies were excluded, as were articles with no full text available. All articles were reviewed independently by two reviewers (S.B. and R.T.) and any disagreement was resolved by consensus.
Data extraction and management
Two reviewers (S.B. and R.T.) independently extracted data from included studies. Information was extracted and tabulated in a datasheet. Any disagreement was resolved by consensus. The data collected included time and location (including nutritional iodine supply status of the region) of the study, age, thyroid status of patients, relevant comorbidities, urinary iodine concentration, goiter and nodules (assessed by ultrasound), autonomy (assessed by scintigraphy) at baseline; type of radiographic procedure; type, administration route, and amount of ICM; assay used to measure thyroid hormones; and thyroid status as an endpoint of the study. If thyroid hormone levels were measured at multiple timepoints, the timepoint closest to 30 days was chosen as the endpoint, as this would be the time by which relevant overt hyperthyroidism is expected to be most prevalent. To avoid missing subjects with transient hyperthyroidism, we additionally looked into the prevalence of thyrotoxicosis at 1 week after ICM administration, whenever such data were available. Furthermore, data about the prevalence of hyperthyroidism in presumed high-risk subgroups (i.e., autonomy, subclinical hyperthyroidism, and goiter) were extracted.
Data analysis
Individual study results are presented as percentage accompanied by Wilson score confidence intervals (CIs). We pooled studies with a random effects model using the method of DerSimonian and Laird (10). To stabilize variances of individual studies, we used the Freeman–Tukey arcsine transformation. Between-study heterogeneity is quantified by the tau2 and I 2 statistic. The approximate prediction interval was calculated based on the method proposed by Higgins and Thompson (11). All analyses were performed using Stata Release 15 (College Station, TX) and the metaprop command.
Quality assessment and risk of bias
For quality assessment, the following factors were considered: Study design (study type and retrospective/prospective) Research question: Whether the prevalence/incidence of IIH after administration of ICM was the primary endpoint of the study? Selection criteria: (a) Whether the sampling method allowed for a representative sample of the source population? (b) Whether inclusion and exclusion criteria were appropriate (particularly with regard to thyroid status and pre-exposure to iodine)? Measurement of exposures and outcomes: (a) Whether the assays used for thyroid hormone measurements can be regarded as valid (the following tests were considered to be valid: enzyme-linked immunosorbent assay, immunoluminometric, and fluoroimmunometric assays)? (b) Whether methods to ascertain participants characteristics were both valid and reliable (the following procedures were considered to be valid: for the assessment of thyroid size and structure: ultrasound or CT scan; to assess the presence of autonomy: radioiodine scan)? (c) Whether follow-up was long enough for the endpoint of interest? Appropriateness of analytical methods: (a) Whether the statistical method was appropriate for the outcome data? (b) Whether >80% of the individuals had their samples analyzed? (c) Whether comparisons between individuals whose samples were analyzed and dropouts (i.e., lost to follow-up) were presented, and whether they were similar?
The methodological quality of the included studies was independently assessed by the two reviewers (S.B. and R.T.) in compliance with the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) guidelines (12,13) and disagreements were adjudicated. The overall level of evidence was rated as “high” when there was a high level of confidence that the pooled estimate lied close to the true population estimate, or as “very low” when the confidence was very low, with “low” and “moderate” being the in-between categories. According to the GRADE guidelines, the initial level of confidence in the estimates from observational studies was rated as “low.” The five GRADE domains (risk of bias, inconsistency, indirectness, imprecision, and publication bias) were considered in downgrading confidence in the overall estimate; in contrast, large effect, dose–response gradient, and direction of plausible confounding were the criteria considered in upgrading the confidence in the estimates.
Results
Search results and study characteristics
The literature search yielded 1493 articles (Fig. 1). Of these, 38 were reviewed in full text and 30 articles met the final selection criteria and were included in the analysis. For one article (14), we only considered baseline characteristics, as endpoint thyroid hormone levels were not reported. Two studies were randomized controlled interventional trials, where the interventional arm of patients received prophylactic thyrostatic drugs before ICM administration (15,16); for these studies, we considered only the patients in the observational arm. The iodine supply of the study region was reported in some of the articles. Other articles, however, did not contain any information about the local nutritional iodine intake; in this case, information was retrieved and reported according to the literature (Iodine global network) (17 –20). Table 1 summarizes study design and characteristics of the studies included.

Flowchart for the systematic review and meta-analysis.
Study Design and Characteristics of the 30 Articles That Met the Final Inclusion Criteria
“All” means baseline thyroid status euthyroid, (subclinical) hypothyroid or subclinical hyperthyroid.
A, angiography; CA, coronary angiography; CC, case–control study; CCG, cholecystography; CS, cohort study; CT, computed tomogram; ERCP, endoscopic retrograde cholangiopancreatography; HSG, hysterosalpingography; Int, intervention study; IVP, intravenous pyelogram; L, longitudinal study; NR, not reported; PhG, phlebography; PS, prospective study; RCT, randomized control trial; RS, retrospective study; SH, subclinical hyperthyroidism.
The time endpoint to assess thyroid hormone levels after ICM exposure varied between 1 and 541 days between studies. However, 28 out of 30 studies had a time endpoint between 7 and 56 days after ICM exposure to assess thyroid hormone levels.
Meta-analysis
Twenty-nine studies had sufficient data on the prevalence of hyperthyroidism after ICM exposure (15,16,21 –48). The pooled analyses included in Figure 2 show the overall estimated prevalence of overt hyperthyroidism after ICM exposure in the 26 studies that reported it: the rate was extremely low (0.1% [CI 0–0.6%]). The three studies not included in the figure reported the overall rate of thyrotoxicosis, rather than only overt hyperthyroidism. Figure 3 shows the prevalence of overt hyperthyroidism according to thyroid status at baseline (only in euthyroid patients vs. patients with the full spectrum of thyroid function [euthyroidism, hypothyroidism, hyperthyroidism; “all patients”]): the overall estimated prevalence was slightly higher in patients who were euthyroid at baseline (0.3% [CI 0–1.7%]) compared with “all patients” (0% [CI 0–0.5%]). The prevalence of subclinical hyperthyroidism at baseline was reported only in a small subset of studies and was very low; hence, no analysis could be performed on the prevalence of overt hyperthyroidism in patients with subclinical hyperthyroidism at baseline.
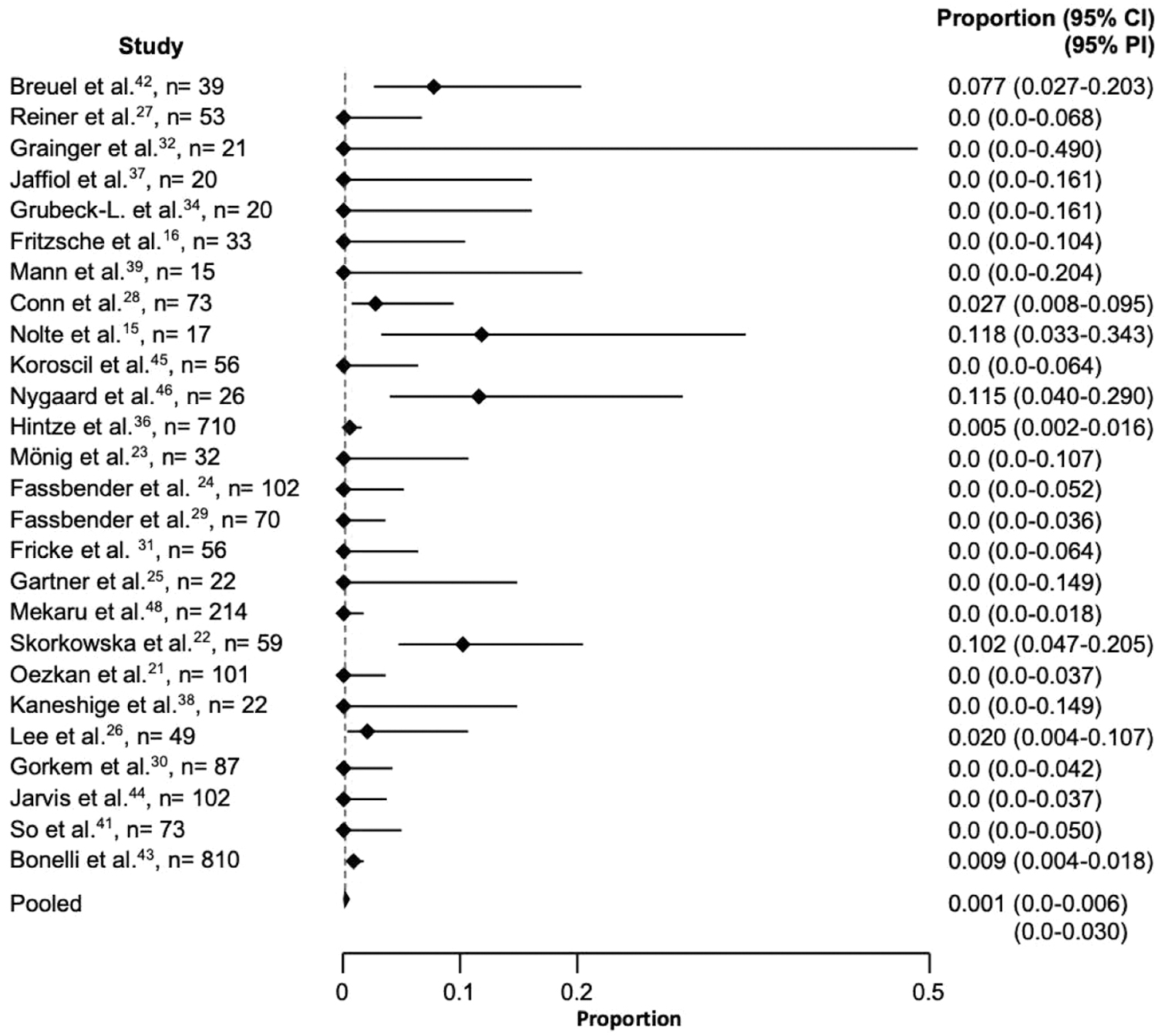
Overt hyperthyroidism at follow-up in all-comers. Between-study heterogeneity tau2 = 0.009 − I 2 = 45%. CI, confidence interval; PI, prediction interval.
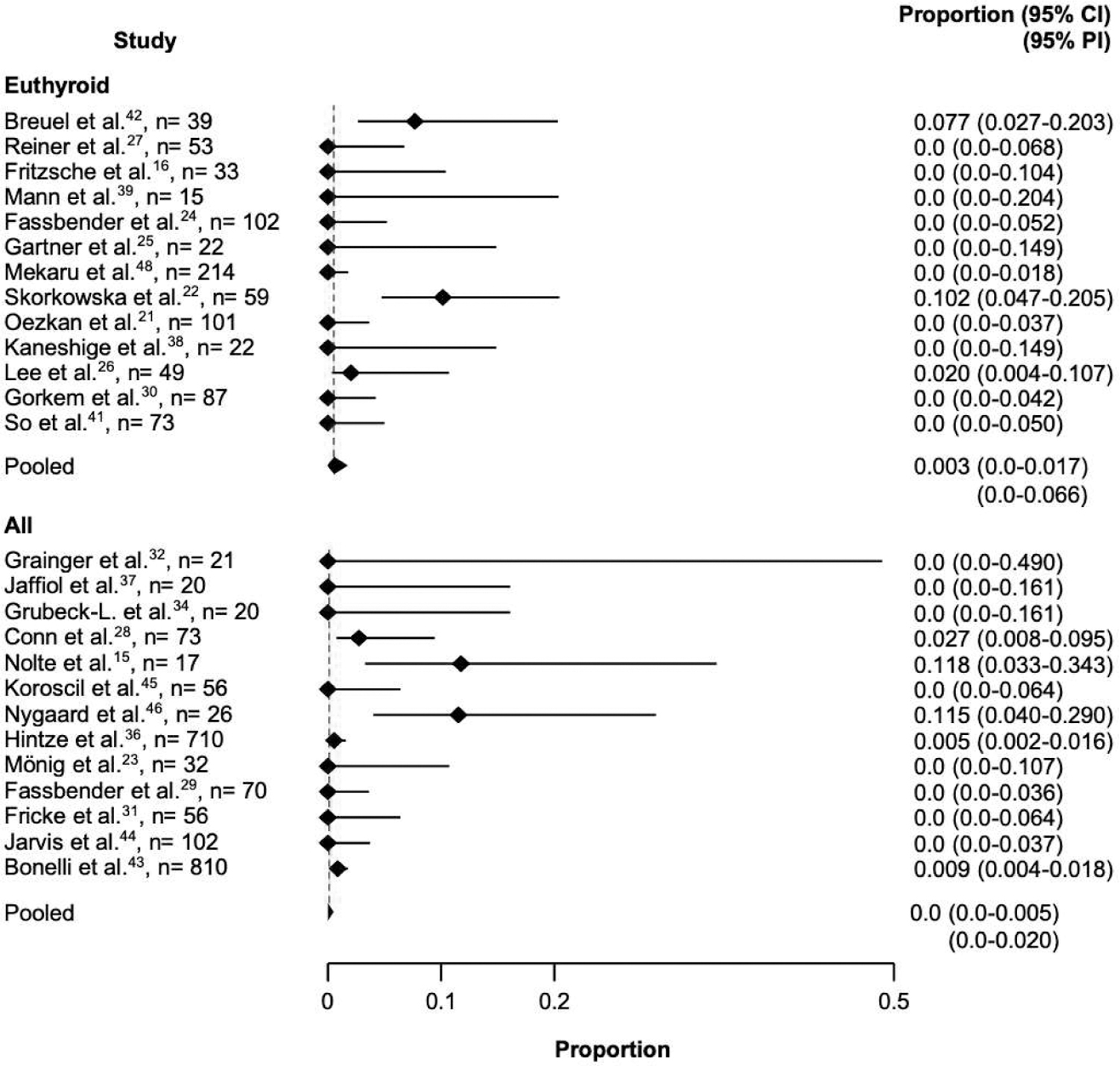
Overt hyperthyroidism at follow-up in all-comers by baseline status. Between-study heterogeneity within stratum euthyroid: tau2 = 0.02 − I 2 = 56%; all: tau2 = 0.01 − I 2 = 36%. Between-stratum heterogeneity: p = 0.82.
Subgroup analysis
To avoid possible bias, a subgroup analysis was performed after exclusion of the studies in which iopanoic acid and ipodate were used as ICM, as these are thyrostatic agents that inhibit type 2 deiodinase, potentially leading to hypothyroidism. The prevalence of overt hyperthyroidism after exclusion of these studies did not change (0.1% [CI 0–0.7%]).
As there were major differences among studies regarding time endpoints at which thyroid function was assessed after ICM exposure, we performed a subgroup analysis for the prevalence of overt hyperthyroidism at 1 week and 30 days after ICM exposure (Fig. 4a, b) because the risk of hyperthyroidism is expected to be higher between one of these timepoints. There were no events at 1 week and the prevalence was very low at 30 days (0.4% [CI 0–0.12%]).
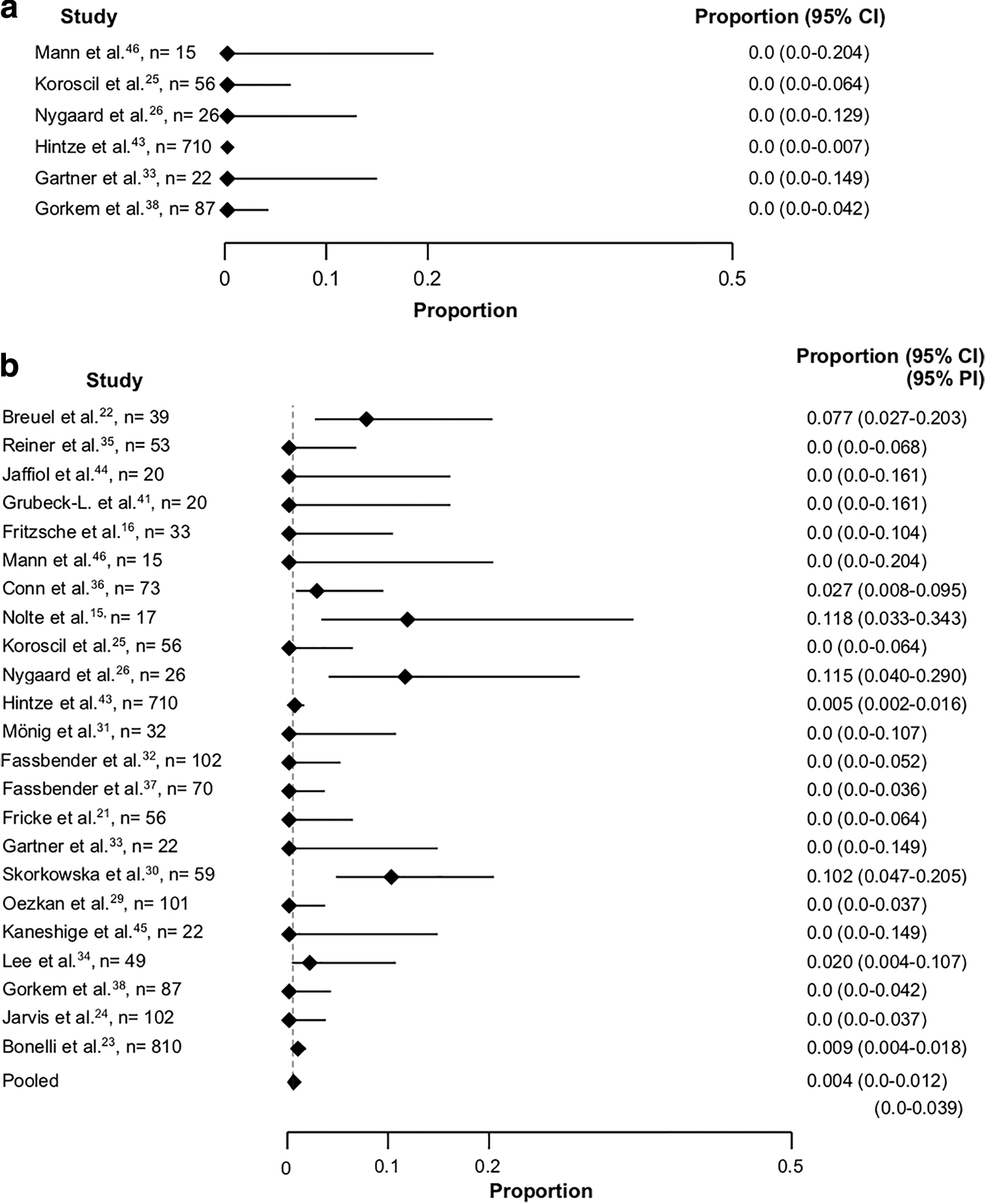
(
Study quality
The methodological quality of the studies is reported according to the GRADE guidelines (Table 2). In the initial assessment, only one study (15) had a high level of evidence due to study type (randomized controlled trial). All other studies initially had a low level of evidence due to their observational study design. No study fulfilled the criteria for uprating (i.e., large effect, dose–response gradient, and direction of plausible confounding), mostly due to their small sample size. After adjusting for the quality of evidence according to GRADE domains (risk of bias, inconsistency, indirectness, imprecision, and publication bias), only one study (15) had a high level of evidence. Three studies (31,36,43) had a low level of evidence. All other studies had a very low level of evidence.
Methodological Quality of the Studies According to the Grading of Recommendations Assessment, Development, and Evaluation Guidelines
Values meaning initial quality/quality of a body of evidence: ++++, moderate. ++, low. +, very low. Risk of bias/inconsistency/indirectness/imprecision: 0, not serious; −1, serious; −2, very serious. Publication bias: 0, not likely; −1, likely; −2, very likely.
Discussion
To the best of our knowledge, this is the first meta-analysis that estimates the prevalence of overt hyperthyroidism after administration of ICM during radiographic procedures. The results demonstrate that the prevalence of IIH after ICM exposure is extremely low. They also suggest that the prevalence of IIH does not depend on the initial thyroid status. Although the number of patients with baseline subclinical hyperthyroidism was too small to perform a subgroup analysis, the few studies that specifically reported these data did not find the prevalence of overt hyperthyroidism to be higher in patients with baseline subclinical hyperthyroidism (15,31).
Interestingly, two of the analyzed studies, both conducted in goitrous regions (Turin, Piemont, and Wroclaw, Lower Silesia) found a considerably higher prevalence of IIH after ICM exposure (22,43) compared with the other studies. Of note, the study by Bonelli et al. reported also higher rates of overt (0.37%) and subclinical (6.8%) hyperthyroidism at baseline. Potential explanations for these observations include that the population studied by Bonelli et al. was older (mean age 67 years), and that about a third (35%) had thyroid nodules and hence a potentially higher prevalence of focal autonomy, which could account for the higher rate of baseline hyperthyroidism. Moreover, only 20% of study patients were consumers of iodized salt; accordingly, median, but not mean urinary iodine concentration was borderline (100 μg/L). In contrast, the study by Hintze et al., which was also conducted in a low iodine intake area with a similar study design and number of patients, found lower baseline rates of subclinical (3.8%) and overt (0.14%) hyperthyroidism. This could be partly explained by the younger study population (mean age 55 years) and the lower prevalence of thyroid nodules (17%). When considering the type of ICM used, only two studies (43,44) reported the use of iodixanol, an iso-osmolar contrast agent, whereas low- or high-osmolar agents were administered in all other studies. Interestingly, rates of IIH were higher in these two studies (10% in the study by Bonelli et al. and 6.2% in the subpopulation of 16 patients reported by Jarvis et al.), with most of the patients having subclinical, and not overt, hyperthyroidism. Further studies are needed to investigate whether the use of iso-osmolar contrast media could be associated with higher rates of IIH.
The second study with a higher rate of IIH is the study by Skórkowska et al. (22). In that study patient age was similar (mean 58 years) to most studies, but there was a considerably higher rate of patients presenting with thyroid nodules at baseline (37%), similar to the study population of Bonelli et al., which could, again, account for a higher rate of autonomy. This hypothesis is further supported by the relatively high iodine uptake on baseline scintigraphy (mean 24%). Hence, the differences in hyperthyroidism rates both at baseline and after 4 weeks compared with other studies is likely explained by differences in the study population.
There were major differences in the type and amount of ICM, in the type of radiographic procedures, as well as in the time endpoint chosen to assess thyroid hormone levels. As the amount of organic iodine that is released from contrast agents clearly exceeds the RDA and hence may result in a Jod-Basedow phenomenon, it is apparent that the type of procedure and/or the amount of the administered ICM do not have a major influence on the prevalence of IIH.
Some of the studies might have been influenced by the use of iopanoic acid and ipodate, two radiographic agents that are well-known inhibitors of type 2 deiodinase and that have, therefore, also been used as thyrostatic agents in severe thyrotoxicosis. For this reason, we performed a subgroup analysis excluding studies where these two agents were used as contrast media; however, no difference was found in the prevalence of IIH, which remained extremely low.
There is considerable heterogeneity in the time endpoint chosen to assess thyroid function after ICM exposure among studies (1–541 days after exposure). In studies that reported multiple timepoints, we selected the timepoint closer to 30 days as the endpoint to compare them with other studies. A 30-day endpoint was the most commonly chosen timepoint in most of the selected studies, as the occurrence of overt hyperthyroidism after ICM exposure is expected around that time and urinary iodine excretion usually normalizes by 40 days (7,49,50). However, one may argue that some patients develop IIH at an earlier timepoint and could, therefore, be missed. To address this question, we performed a subgroup analysis looking at the prevalence of IIH 7 days after ICM administration in the studies reporting data at this timepoint. However, there were again no differences in the prevalence of IIH, which remained very low.
Most of the included studies were performed >25 years ago, when radioimmunoassays (RIAs) were commonly used for measuring thyroid hormone levels. Although these RIAs were, in part, less precise, we do not expect that this would introduce bias because clinically relevant thyroid dysfunction would have been detectable independently from the type of assay used.
An additional limitation is that most of the studies did not assess the presence of potential risk factors for the development of hyperthyroidism (i.e., goiter and focal autonomy of nodules), thereby introducing a potential selection bias. However, one of the biggest and qualitatively best studies included in the analysis presented in this study (36) did not identify any cases of IIH in patients with subclinical hyperthyroidism, goiter, or autonomy at baseline. In this study, only 2 out of 788 patients developed IIH after ICM exposure, and neither of them had any risk factors at baseline.
According to GRADE criteria, we found an overall low quality of the analyzed studies. Only one study had a very high quality (15) and three studies were of low quality (31,36,43). All other studies had a very low quality, and most of them were performed >30 years ago on small patient samples and with very heterogenous study designs. Moreover, since there have been considerable changes in the composition of ICM during the past 20 years, extrapolating data accrued in the 1980s to current clinical practice should be done with caution.
According to current recommendations, prophylactic treatment with thyrostatic drugs and/or perchlorate (where available) to avoid the risk of developing IIH may be considered for high-risk patients with suppressed thyrotropin levels, especially in patients in whom adverse effects of thyrotoxicosis could compromise clinical outcomes, for example, in patients with cardiac disease (51). However, the results presented in this study demonstrate that the prevalence of IIH after ICM exposure is very low. Therefore, it is questionable whether administration of a prophylactic regimen is indeed indicated in patients who are euthyroid or who have subclinical hyperthyroid at baseline. Future studies should specifically address this question.
In summary, our results suggest that the prevalence of IIH after ICM administration during radiographic procedures is extremely low. Therefore, it is questionable whether prophylactic administration of thyrostatic drugs for the prevention of IIH is indicated, even in patients with possible risk factors at baseline.
Footnotes
Author Disclosure Statement
The authors state that no competing financial interest exists.
Funding Information
No funding was received for this study.
Supplementary Material
Supplementary Appendix SA1