
Abstract
Background:
Levothyroxine (LT4) as a medication is used by up to 5.3% of the adult population. For optimal efficacy, the traditional tablet formulation (LT4tab) requires that patients avoid concomitant ingestion with food, drinks, and certain medications, as well as excellent patient compliance. Some comorbidities influence bioavailability of LT4 and may mandate repeated dose adjustments.
Summary:
New LT4 formulations (soft gel [LT4soft] and liquid [LT4liq]) containing predissolved LT4 are claimed to improve bioavailability, presumably by facilitating absorption. Thus, these formulations may well be more suitable than LT4tab for patients whose daily requirements are subjected to variations in bioavailability. Here, we review the evidence and indications for use of new LT4 formulations and highlight areas of uncertainty that are worthy of further investigation. While bioequivalence is established for LT4soft and LT4liq administered to healthy volunteers compared with LT4tab in pharmacokinetic (PK) studies, therapeutic equivalence of the new formulations seems to be different in several clinical settings. Some evidence suggests that new formulations of LT4 may mitigate against the strict requirements relating to concomitant ingestion with food, drinks, and certain medications, which apply to traditional LT4 tablets. The principal indication is in selected patients with disease fluctuations and intermittent therapies with interfering medications, where the need for frequent dose adjustments and office visits may be diminished. Whether the use of LT4soft or LT4liq in patients with impaired gastric acid secretion results in better control of hypothyroidism than LT4tab remains unclear.
Conclusions:
The evidence in favor of using LT4soft and LT4liq in clinical practice over LT4tab is weak, and the underlying putative PK mechanisms unclear. Additional studies to investigate these potential benefits, define the cost-effectiveness, and understand the PK mechanisms involved with new LT4 formulations are needed.
Introduction
Hypothyroidism affects 5.3%
Dose adjustments may be triggered by patient nonadherence, concomitant medications, gastrointestinal comorbidities, switching between generic and branded LT4 products, diet, and alterations in body weight (10).
The most common cause of therapeutic failure is poor patient adherence (11). Compared with other medications, optimal administration of LT4 is more demanding: it requires fasting, to be taken with plain water, and abstinence from eating or drinking for 30 minutes postingestion. “Refractory” hypothyroidism may be caused by gastrointestinal diseases and interfering medications (12,13).
In addition to LT4 in tablet form (LT4tab), two new formulations, liquid (LT4liq) and soft gel capsules (LT4soft), are approved by the European Medicines Agency and the American Food and Drug Administration. Unlike LT4tab, LT4liq and LT4soft contain predissolved thyroxine (14 –16). Although LT4tab remains the treatment of choice, LT4liq and LT4soft may have therapeutic advantages in some circumstances.
Methods
A PubMed literature search was carried out using combinations of keywords “levothyroxine,” “absorption,” “tablet,” “liquid,” “solution,” “soft gel” up to October 15, 2019.
The Journey of LT4
LT4tab contain LT4 sodium salt compressed into a tablet with several different excipients (lactose monohydrate, cornstarch, carboxymethyl starch, gelatin, croscarmellose sodium, magnesium stearate, citric acid, microcrystalline cellulose, talc, calcium phosphate dibasic dihydrate, Na-laureth sulfate, and tartrazine yellow). Before absorption, the LT4 sodium salt must be released from LT4tab (tablet disintegration) and then go into solution. Excipients are major determinants of disintegration and dissolution (12,17,18). Disintegration of LT4tab may be facilitated by mechanically pulverizing the tablet (19). Solubility of LT4 sodium salt decreases with increase of low pH toward neutral (20). Decreased dissolution may result from raised gastric pH due to antacids, proton pump inhibitors (PPIs), atrophic gastritis, Helicobacter pylori infection (21), delayed gastric emptying (22), food, and drinks other than plain water (23,24).
The principal difference between LT4tab and LT4liq and LT4soft rests with the physicochemical processes that occur in the gastrointestinal tract before absorption (Fig. 1). LT4soft has a gelatin shell, which melts in gastric fluid, thus enabling its LT4 content, predissolved in glycerol, to release into the gastrointestinal fluid and remain in solution regardless of pH (25).
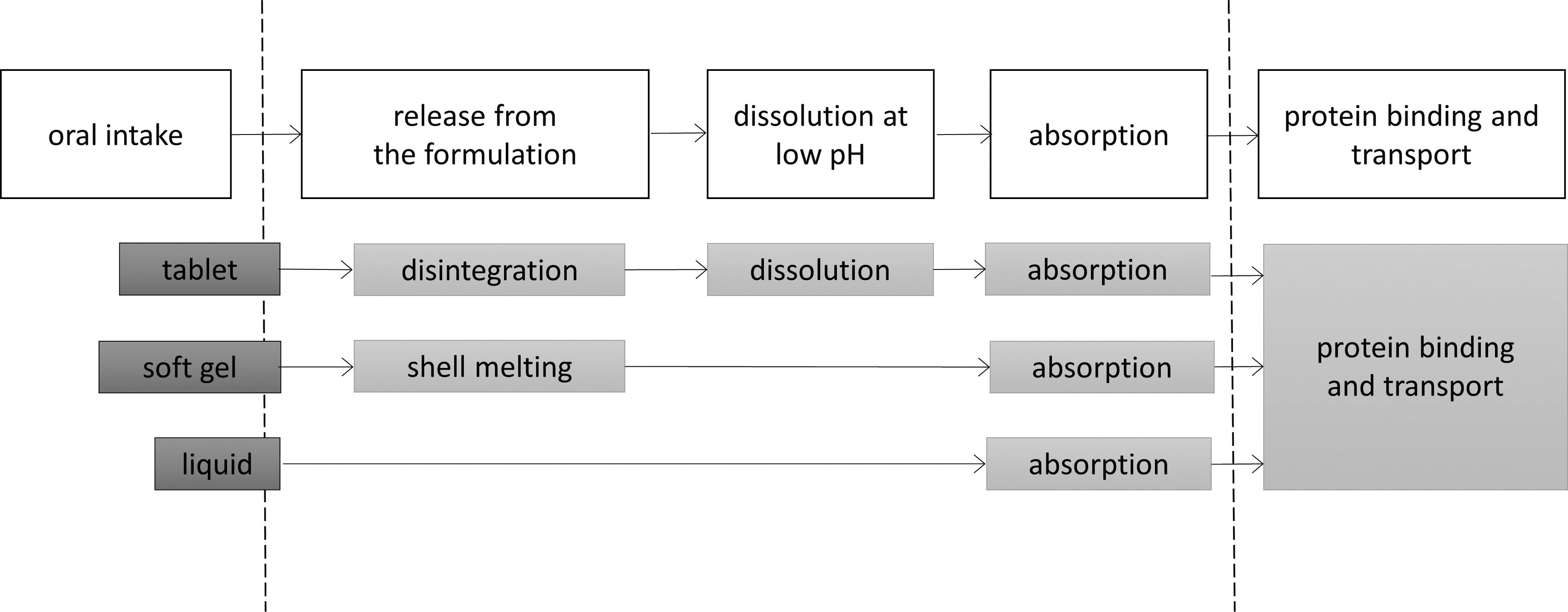
The destiny of swallowed LT4. Three oral formulations are compared. LT4 rapidly passes through the esophagus and arrives in the stomach. The section between the dotted lines is the major determinants of bioavailability. After disintegration (tablet) or melting (soft gel), LT4 is released into the gastric fluid. Absorption percentage is dependent on gastric pH (tablet) and the condition of the intestinal wall (tablet, soft gel, liquid); soft gel and liquid skip the pH-dependent dissolution step. After being absorbed, oral and endogenous thyroxine share the same fate. Disintegration refers to separation of the sodium salt of LT4 from excipients. Dissolution is the process by which the LT4 sodium salt goes into aqueous solution. Melting is the change of physical state from gel to fluid. LT4, levothyroxine.
The principal sites of LT4 absorption are duodenum and jejunum (26), while ileum is important following bariatric surgery (27). Absorption of dissolved LT4 is dependent on the structural integrity and function of the intestinal wall, as well as food and some medications in the intestinal lumen. Bariatric surgery (excluding sleeve gastrectomy) (28), short bowel syndrome (29), and small intestinal diseases can impair absorption of LT4. In addition, calcium salts, iron, sucralfate, orlistat, bile acid sequestrants, soybean, and dietary fiber prevent absorption of LT4 by chelation, complex formation, or surface binding (12,13) (Table 1). Vitamin C facilitates LT4 bioavailability (30).
Factors That Have Been Shown to Impair Levothyroxine Intestinal Absorption
Those factors that interfere primarily with the dissolution step by interfering with gastric pH are in italics. For hepatic cirrhosis, both higher and lower LT4 absorption fractions have been described. The only known facilitator of LT4 absorption is vitamin C. The mechanism of the nongastric interferences is less understood. See text for details.
LT4, levothyroxine.
Once absorbed, orally taken LT4 is handled in the same manner as endogenous LT4.
Pharmacokinetic Considerations
Given the narrow therapeutic index of LT4 (31), bioequivalence and therapeutic equivalence between batches and products are important. Current guidelines recommend that brand and formulation of LT4 should not be altered, unless there is a clinical indication (32,33). The pharmacokinetic (PK) protocol for bioequivalence developed by the regulatory authorities requires a single oral dose of 600 μg of LT4 to be administered to healthy volunteers (34,35) and measurement of the area under the curve (AUC)(0–t) and Cmax for free thyroxine (fT4). Bioequivalence is achieved when the 90% confidence interval for the ratio of the test and reference products is 90.00–111.11% (34). This protocol has been criticized for administering supraphysiological doses of LT4 to healthy volunteers who produce endogenous thyroid hormones.
One notable bioequivalence study found no fT4 change after switching from LT4tab to LT4liq, thus demonstrating apparent bioequivalence. However, LT4liq had a greater TSH-lowering effect compared with the reference product (36). Unlike most bioequivalence studies, both fT4 and TSH were measured while all patients were on the same mcg/kg/day regimen. At 6 and 12 weeks, fT4 and free triiodothyronine did not differ between the two groups, while TSH was substantially lower in patients on LT4liq compared with LT4tab, indicating nontherapeutic equivalence with PK-based studies.
The explanation may be the linear-logarithmic relationship (37,38) between fT4 and TSH, although the curve is not strictly linear (39). Elevation of fT4 within the reference range may result in substantial drop of serum TSH. This is illustrated in an idealized example in Figure 2 and supported by a 72 hour PK equivalence study (40); the serum fT4 curve of LT4soft, which had a more pronounced TSH-lowering effect in the Fallahi study (36), ran somewhat above that of the reference formulation for the full 72 hours (AUC 0–72, 109.1% of the reference product), which may indicate that LT4soft is 109.1% more bioavailable than LT4tab. Although the difference between the two fT4 curves failed to reach the limit of nonequivalence, it may have been enough to evoke a TSH-lowering effect, which is probably indicative of the insensitivity of T4-based PK bioequivalence studies. Furthermore, the early dissolution and hence absorption of the test formulation in the first 60 minutes after ingestion was steeper and resulted in a spike at 60–180 minutes, which substantially exceeded that of the reference product (Cmax 114.8% of reference). Both factors may have contributed to the TSH-lowering effect. Athyreotic patients are more susceptible to this effect than patients with a partially functioning thyroid remnant that may provide a buffer action (41), as the hypothalamic–pituitary thyrostat compensates by altering endogenous thyroid hormone secretion. One may conclude that bioequivalence (by definition) in serum level may not uniformly translate to therapeutic equivalence in biological systems, where linear-logarithmic relationships between parameters may exaggerate the end effect. Comparative PK studies, in euthyroid individuals not receiving other medications, found that LT4tab, LT4liq, and LT4soft meet regulatory criteria for bioequivalence (15,40,42 –44); however, they may not be interchangeable in all clinical scenarios.
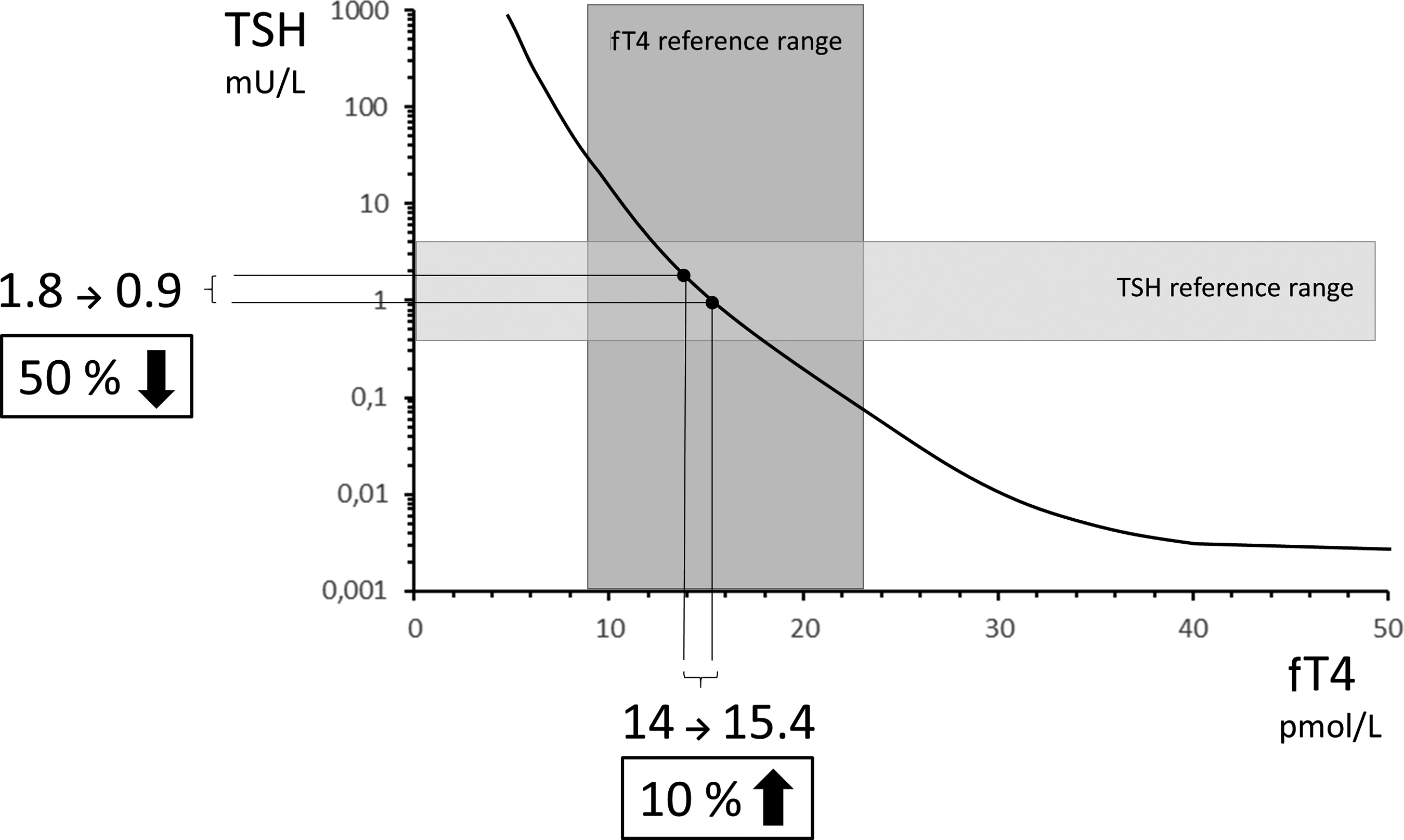
The TSH-fT4 feedback regulation within the reference range. With intact hypothalamic–pituitary regulation, fT4 change evokes a more marked TSH response due to the inverse logarithmic-linear relationship between these parameters. In this idealized example, 10% rise in serum fT4 results in a 50% drop of serum TSH. [Based on the conclusions of Reichlin and Utiger (37) and Benhadi et al. (38)]. fT4, free thyroxine; TSH, thyrotropin.
LT4 and PPIs are widely used medications (45). Reports on the effects of coadministration of LT4 and PPIs are contradictory. Faster and better absorption of LT4soft compared with LT4tab was reported in a patient on a PPI (46). In a randomized comparative study, acute increase in gastric pH induced by intravenous PPI resulted in impaired LT4tab bioavailability compared with LT4soft (47). Another study showed that oral PPI therapy had no such effect by the end of the seventh day of treatment (48). PPI potency, dosage, and routes of administration as well as the different LT4tabs containing different excipients may account for these disparate findings. Other noncomparative PK studies found that a series of conditions and medications can interfere with LT4 kinetics (24,49 –57). One may assume that this interference can be overcome by increasing the LT4 dose, although hard evidence is lacking.
Some data (58,59) suggest that better absorption can be achieved by LT4liq and LT4soft in patients with small intestinal disease. The mechanism for this is unclear.
Clinical Trials and Observations Comparing LT4 Formulations
Several comparative studies focused on formulations of LT4. They include patients with different causes of hypothyroidism (58,60 –78) with (58,59,67,68,71,72,79,80) or without (36,60 –63,73,74,81 –86) comorbidities. In the majority of these studies, patients receiving medications known to interfere with LT4 absorption were excluded, while others lack information on comorbidities and/or concomitant medications. Fifty-five clinical studies (36,58 –74,79 –88) compared LT4tab with LT4liq or LT4soft, while 16 (21,30,75 –78,89 –98) examined the effects of comorbidities, concomitant medications, and timing of ingestion in relation to meals in patients treated with LT4tab.
Clinical studies showed reduced efficacy of LT4tab when taken with PPIs (21,74,90), calcium (63,86), iron (63), sevelamer (99), and espresso coffee (50,73,98). With the exception of sevelamer, these drug interferences were shown, by at least one publication for each category, to be avoidable by switching to LT4liq or LT4soft. However, these studies (63,73,74,86) were small (n = 8–40), retrospective (74), open-label (63,73,74,86), and better compliance with LT4liq/LT4soft cannot be excluded (63,73,74,86), and the clinical significance of the LT4soft impact was doubtful (86).
Similar benefits were claimed upon switching from LT4tab to LT4liq or LT4soft in patients with autoimmune gastritis (67), lactose intolerance (58), following certain types of bariatric surgery (68), H. pylori infection (80), esophageal complications of systemic sclerosis (79), diabetic gastroparesis (71), and giardiasis (59).
All these studies, however, had limitations. Three studies (59,71,79) were single-patient case reports, three (58,67,68) were small (n = 6–17 patients), unblinded observational studies, and patient nonadherence before switching to LT4liq cannot be ruled out for all of them. One study (80) was larger (n = 43), but was unblinded, the two groups were not matched for age and sex, and the differences between LT4liq and LT4tab were subtle and of doubtful clinical importance. The mechanism for improved control of hypothyroidism associated with LT4liq/LT4soft where achlorhydria was absent, is unclear, but improved adherence with these novel preparations may have contributed.
It is widely accepted that food and drink may interfere with LT4tab absorption (23), although this finding has not been confirmed by another study (87). Concomitant food intake does not interfere with the absorption of LT4liq and LT4soft (65,66,88).
Remaining Uncertainty, Lack of Evidence, and Open Questions
While these studies showed potential superiority of LT4liq and LT4soft over LT4tab in the presence of certain comorbidities and concomitant medications, many uncertainties remain (14,100) (Table 2). A growing list of unresolved questions has surfaced with regard to LT4liq and LT4soft (Table 3). Potential absorption sites outside the gastrointestinal tract would be of special importance; buccal or sublingual routes (101) may avoid the need for parenteral administration. Of the least studied drug interactions, the intestinal transporter OATP2b1 was shown to transport T4 and was inhibited by atorvastatin (102). The majority of these questions have to be addressed for both the traditional and the new formulations.
Common Weaknesses of Available Studies Investigating Levothyroxine Formulations
fT4, free thyroxine; TSH, thyrotropin; TT4, total thyroxine.
Open Research Questions for Future Studies on Levothyroxine Bioavailability
The limited number of excipients (gelatin and/or glycerin) in LT4liq and LT4soft compared with LT4tab is promoted (103) as an advantage. PK differences between formulations may impact on biochemical control of hypothyroidism. Patients frequently blame excipients for “allergies,” “intolerances,” and other symptoms, which impact on satisfaction with their treatment, which are unlikely to have an organic basis. There is therefore a need for robust studies that explore the etiology of these symptoms.
Clinical Indications for LT4liq and LT4soft
LT4liq and LT4soft are considerably more expensive than LT4tab, and in the absence of cost-effectiveness data, clinicians ought to be prudent about their use. Patients with stable comorbidities can be managed with higher than average doses of LT4tab (21,104). However, in some patients, gastrointestinal disease fluctuations and intermittent therapies with interfering medications demand frequent LT4tab dose adjustments (105), and such patients may benefit the most from LT4liq or LT4soft. Less frequent biochemical monitoring and dose adjustments may lead to enhanced patient satisfaction (106); however, a recent study did not find improved patient adherence with LT4soft (107).
A significant number of hypothyroid patients are unable to consistently avoid food and beverages for 30 minutes after the ingestion of LT4tab, which can be a considerable burden. In many cases, this can be addressed by moving the timing of LT4tab administration to bedtime (92). If this is not possible, then switching to LT4liq and LT4soft may be an option.
Conclusions
Theoretically, LT4liq and LT4soft may be expected to outperform LT4tab in bioavailability in patients who intermittently are treated with interfering medications or who have fluctuating severity of gastrointestinal disease. A long list of unanswered questions remains. In view of the considerable number of patients dissatisfied with LT4tab treatment, and the increasing demand for combined LT4 and LT3 preparations, there is an urgent need to clarify whether new LT4 formulations may benefit such patients. The burden of separating tablets from breakfast and coffee may also be reduced. Should this be the case, this may prove to be a safer and more efficacious strategy than the use of various combinations of LT4 and LT3 (108). Further robust studies with sufficient power are needed to address these questions to provide evidence-based guidelines.
Footnotes
Authors' Contribution
E.V.N. and M.K. initially analyzed and interpreted the literature. All authors drafted the article, critically revised it, and approved the submitted version. E.V.N. is the guarantor of this work and takes responsibility for the integrity of its accuracy.
Author Disclosure Statement
L.H., E.V.N., E.P., and P.P. are consultants for IBSA Group Pharmaceuticals, Switzerland. However, IBSA has had no influence on the design, interpretation, or decision to publish this article and have not supported this work economically.
Funding Information
No funding was received for this article.