
Abstract
Background:
Low serum thyrotropin (TSH) has been associated with an increased risk of cognitive impairment in observational studies of older individuals, but the mechanism underlying this is unclear. We investigated the association between changes in thyroid status and cognitive impairment in very old adults, using prospective data from the Newcastle 85+ study.
Method:
A cohort of 85-year-old individuals was assessed for health status and thyroid function. Complete data from a comprehensive multidimensional measure of health and repeat thyroid function were available for 642 participants with normal free thyroid hormones and TSH levels ranging between 0.1 and 10 mU/L. Cognitive performance, assessed using Mini-Mental State Examination (MMSE) and Cognitive Drug Research battery was examined by using linear mixed, logistic regression, and Cox proportional hazard models in relation to baseline and 3-year changes in serum TSH, free thyroxine (fT4), and free triiodothyronine (fT3).
Results:
Over 3 years, declining serum TSH was associated with reductions in fT4 and fT3, and an increased risk of incident cognitive impairment by 5 years (odds ratio1.77 [95% confidence interval: 1.19–2.61]; p = 0.004). A greater reduction in MMSE score was associated with larger TSH decline, at 3 (p = 0.001) and 5 years (p < 0.001), respectively. Steady fT4 concentrations were found in participants with rising TSH.
Conclusions:
In contrast to physiological expectation, in this group of 85-year-olds, a declining serum TSH was associated with reductions in free thyroid hormones over time. A decreasing serum TSH trajectory over time anticipated cognitive decline in later life. Declining TSH concentrations are a biomarker for cognitive impairment in later life.
Introduction
Perturbations in thyroid function are common in older people, with up to 3% of older individuals having a serum thyrotropin (TSH) concentration below the healthy reference interval for younger people, and normal free thyroid hormone levels (referred to as subclinical hyperthyroidism) (1). Although overt hyper- or hypothyroidism have long been recognized to adversely affect cognition, the effects of subclinical thyroid diseases are less clear.
There is increasing evidence of an association between low TSH and adverse cognitive outcomes in older people. At least 15 epidemiological studies have shown that low serum TSH concentration is associated with lower Mini-Mental State Examination (MMSE) scores, a diagnosis of Alzheimer's disease or dementia (2 –6). A meta-analysis involving five prospective cohort studies also suggested increased dementia risk with low TSH (7).
In contrast, serum TSH concentrations above the reference interval (subclinical hypothyroidism) were found to be associated with preserved cognitive function in people aged 65 years and older (7). In fact, some studies suggest that higher serum TSH in older people confers a survival advantage and is associated with protection from dementia (8 –11).
Although both the prevalence and incidence of dementia have decreased over the past decades (12), the projected increases in the population aged 85 years and older, the very old, where both prevalence and incidence are highest, will mean greater numbers of older people with dementia. A better understanding of the mechanism by which parameters of thyroid function influence the risk of cognitive decline and dementia is, therefore, necessary to try to reduce the future disease burden. A few previous studies of thyroid function and cognitive decline have included substantial numbers of the very old, and none have prospectively measured changes in thyroid function over time.
We sought to investigate whether changes in thyroid function could predict future risk of cognitive impairment in this age group. In this study, we examine the relationship between serum thyroid hormones measured at 85 and 88 years of age and subsequent cognitive outcome in the Newcastle 85+ Study cohort.
Methods
Study population
The Newcastle 85+ Study is a population-based longitudinal study of health and aging in a single-year birth cohort (1921) recruited at age 85 from general practices in Newcastle and North Tyneside, UK, regardless of health status and place of residence. Full methodological details of the study have been previously published (13).
A total of 845 participants underwent a comprehensive multidimensional measure of health comprising questionnaires, anthropometric measurements, and physical and cognitive function tests. Fasting blood samples were carried out in the participant's usual residence by a research nurse. All interviewed participants agreed to a review of their general practice medical records to extract data on diagnosed diseases and prescribed medication. Seven hundred sixty participants had venipuncture for thyroid function. Follow-up took place at 3 and 5 years. Figure 1 shows the number of participants included in the analysis at each stage. The study was approved by the Newcastle and North Tyneside 1 Research Ethics Committee (ref: 06/Q0905/2).
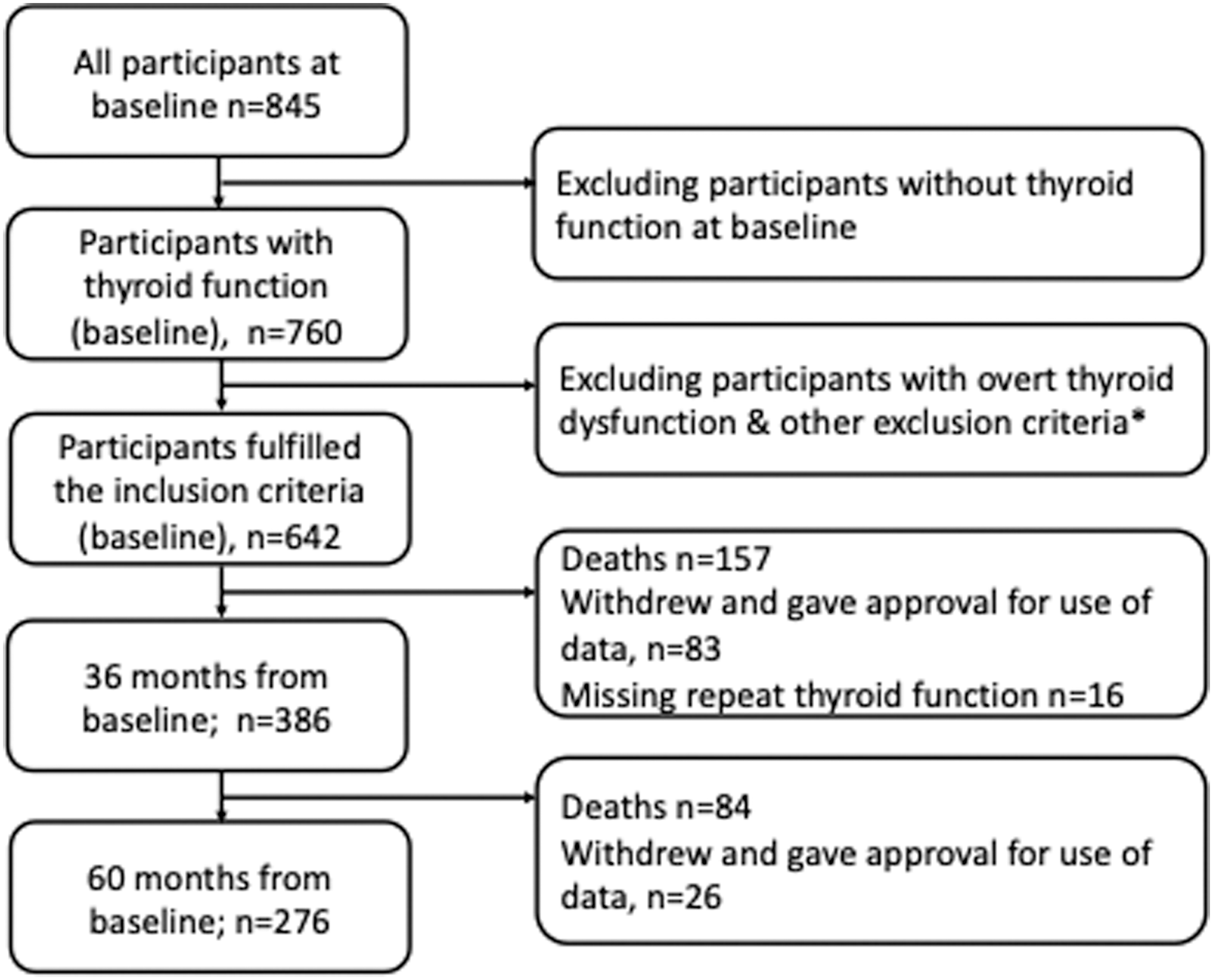
The flowchart of participants analyzed at each phase of the study. *Participants who had overt hyper- or hypothyroidism, were on medications interfering with thyroid function (antithyroid drugs, levothyroxine, amiodarone, lithium), or had TSH <0.1 or >10 mU/L were excluded from analysis.
Blood samples and thyroid hormone assays
Fasting blood samples were obtained between 07:00 and 10:30 hours. Measurement of TSH, free thyroxine (fT4), and free triiodothyronine (fT3) was performed by using a Centaur platform (Seimens) at two time points: baseline (2006–2007) and year-3 (2009–2010). Intra-assay coefficients of variation were serum TSH, 3.8% (at 5.3 mU/L); fT4, 7.9% (at 13.5 pmol/L); and fT3, 3.1% (at 10.5 pmol/L). The following reference ranges were used: TSH, 0.4–4.0 mU/L; fT4, 9.5–22.0 pmol/L; and fT3, 3.5–6.5 pmol/L. Serum reverse T3 (rT3) was assayed in duplicate by radioimmunoassay, using antiserum at a final dilution of 1:600,000 and sample volumes of 25 μL. Thyroid peroxidase antibodies were assayed by Advia chemiluminescent assay on the Centaur platform with an intra-assay coefficient of variation of 17.7% at a concentration of 87.2 U/L. The mean (standard deviation) time between cognitive testing and blood sampling was 8.4 (17.7) days.
On serial measurements, an increasing or decreasing serum TSH trajectory was defined by a change of ≥0.1 mU/L from baseline. This is an arbitrary set point to capture as many participants into the increasing and falling group accordingly, to improve the power for data analysis. Participants who had overt hyper- or hypothyroidism, or on medications interfering with thyroid function (antithyroid drugs, levothyroxine, amiodarone, lithium) were excluded. The final analytic sample comprised the 642 participants who had TSH between 0.1 and 10 mU/L with normal fT4 and fT3 concentrations. The TSH levels below 0.1 or above 10 mU/L are more likely to be caused by endogenous thyroid disorders and, hence, were excluded from the analysis. The TSH was also analyzed according to tertile groups, with the upper tertile defined as 2.56–9.52 mU/L and lower tertile as 0.13–1.54 mU/L.
Assessment of cognitive function
Global cognitive function was available at baseline, 3 and 5 years (relating to participant ages 85, 88, and 90 years) using the standardized MMSE, with a scale ranging from 0 to 30. Cognitive status was defined as normal when MMSE scores were ≥26, whereas incident cognitive impairment was defined as an MMSE score crossing the 25 points threshold (14). A decline in MMSE score ≥3 points is considered to be a clinically meaningful change in cognitive function (15), and it was also used to assess the odds of cognitive decline in one model.
Episodic memory and attention were assessed by using the Cognitive Drug Research computerized assessment system, at baseline and 3 years. Episodic memory was measured with a word recognition sensitivity index (SI) and delayed word recall score. Three main attention tasks measuring response time were used to examine the core aspects of attention: simple reaction time, choice reaction time (CRT), and digit vigilance task (DVT). Power of attention (PoA) was derived from the sum of these three core attention scores, measuring the focused attention and information processing speed. Continuity of attention (CoA) combines the accuracy and error measures from the CRT and DVT to measure sustained attention over the testing period. Details of how each composite measure was constructed and validated have been previously published (16).
Transformation of cognitive test scores
The MMSE and word recognition sensitivity scores were moderately negatively skewed and were corrected with the formula NEWX = SQRT(K − X), where K is the maximum score and X is the participant's score. CoA was substantially negatively skewed and was transformed with the formula NEWX = Log10(K − X), in which K is the maximum score +1 and X is the participant's score. The PoA score was positively skewed and was logarithmically (Log10) transformed. Delayed word recall was substantially positively skewed and was, therefore, Log10 transformed with the formula NEWX = Log10(X + 1), where X is the participant's score. Lower scores in transformed MMSE, word recognition sensitivity, delayed word recall, PoA, and CoA indicate better cognitive function.
Other measures and confounding factors
All multivariable models were adjusted for potential confounders. These include sociodemographic factors (age, sex, and years of education), lifestyle factors (smoking and physical activity), as well as health and morbidities (C-reactive protein [CRP], geriatric depression score, waist-hip ratio, and disease group count). Education was categorized into three groups: 0–9 years (basic education), 10–11 years, and older than 11 years. Physical activity score was derived from a subjective physical activity measure by using a self-reported questionnaire. The physical activity questionnaire categorized participants into low (scores 0–1), moderate (scores 2–6), and high (scores 7–18) physical activity categories, according to the frequency and intensity of physical activity in a week (17). The disease group count variables were derived from a sum of eight disease groups with selective chronic diseases, and participants could score a maximum of 8 (18).
Statistical analyses
Baseline characteristics of participants (n = 642) were compared across the three TSH tertile groups by using the Kruskal-Wallis test for non-normally distributed continuous variables and Chi-square test for categorical variables. Non-normally distributed data were presented as medians and interquartile range. All reported p-values are two-tailed.
Logistic regression models were fitted to explore the association between thyroid changes over 3 years and the odds of incident cognitive impairment (MMSE <26), as well as cognitive decline (reduction in MMSE score ≥3) (odds ratio [OR], 95% confidence interval [CI]). Models are adjusted for all confounders and baseline MMSE.
Changes in global cognition (MMSE), attention, and episodic memory over time were analyzed by linear mixed models; first assessing the cross-sectional effect of baseline thyroid function (including TSH tertile groups) and various cognitive domains (model 1), followed by linear growth curve models with random intercept. Model 2 included an interaction of thyroid function groups and time. Lower transformed MMSE, word recognition SI, delayed word recall, and PoA and CoA scores reflect better cognitive performance. The parameter estimates for model 2 showed the changes in cognition over time that can be attributed to baseline thyroid function. Models were adjusted for all confounders. Linear mixed models with a restricted maximum likelihood method using a first-order autoregressive covariance matrix were used to generate parameter estimates (β) for effects.
The extent of missing values was low at 1% or less for all the covariates, except geriatric depression score at 1.1% Multiple imputations with the automatic method (monotone or fully conditional specification with Monte Carlo Markov chain) were performed for all covariates with missing data. Analyses were performed by using SPSS Statistics 22.0 (IBM Corp. Armonk, NY) apart from the Cox modeling with restricted cubic splines, which used SAS version 9.4 (SAS Institute).
To investigate the effect of the three baseline thyroid measures (TSH, fT4, fT3) as continuous measures on the incidence of cognitive impairment, we used Cox proportional hazard models fully adjusted for all confounders in the subset of participants who were cognitively intact (MMSE ≥26) at baseline (n = 464). Cognitive impairment onset was assumed as being halfway between the last interview with normal cognitive function (MMSE ≥26) and the first interview with cognitive impairment (MMSE <26). The time to onset of cognitive impairment was censored if death occurred before cognitive impairment being observed or at 5 years if still cognitively intact. Forty-four participants were excluded because of censoring (death) before the first observed time of cognitive impairment onset in the analytic sample. Potential nonlinear relationships between each of the thyroid measures and time to onset of cognitive impairment were examined by fitting restricted cubic splines (19).
Sensitivity analysis
Sensitivity analyses were performed to test the robustness of our findings. First, to account for the potential influence of baseline cognition on prospective cognitive changes, analyses were repeated, excluding participants with cognitive impairment (MMSE <26) at baseline. In addition, for models exploring the effect of changes in thyroid function on the odds of cognitive impairment over time, we adjusted analyses by baseline MMSE. Analyses were also repeated redefining cognitive impairment as MMSE <24, because this threshold has been used to define dementia in the very old (20). To explore the association between thyroid changes (baseline vs. 3 years) and the odds of cognitive decline (reduction in ≥3 points), we analyzed the change in MMSE score over the same period versus the subsequent 2 years (3 vs. 5 years).
Results
The median age of the 642 eligible participants was 85.5 years, and 58.1% were women (Table 1). As compared with the original study population (n = 760), the selection criteria in this study resulted in a higher mean physical activity score and hence a fitter study group (Supplementary Table S1). Participants in the lower TSH tertile (0.13–1.54 mU/L) were more likely to have higher levels of CRP, a higher disease group count, and to live in a care home. Those in the lower TSH tertile also had higher fT4 and rT3 levels, compared with the middle and upper TSH tertiles (p < 0.001).
Baseline Characteristics of Participants by Thyrotropin Tertile Groups
TSH tertile was defined as upper (2.56–9.52 mU/L), middle (1.55–2.55 mU/L), and lower (0.13–1.54 mU/L).
For PoA, lower scores indicate better performance.
ApoE4, apolipoprotein E4; BMI, body mass index; CoA, continuity of attention; fT3, free triiodothyronine; fT4, free thyroxine; hsCRP, higher levels of C-reactive protein; IQR, interquartile range; MMSE, Mini-Mental State Examination; PoA, power of attention; SI, sensitivity index; TPO, thyroid peroxidase antibody; TSH, thyrotropin.
Changes in thyroid hormones over time
Of the 642 participants who had baseline thyroid function measured, 54.2% (n = 348) were alive to have their thyroid function tests repeated at 36 months, of whom 221 (63.5%) showed a decreasing TSH trajectory with time, defined by a reduction in serum TSH of ≥0.1 mU/L (Table 2). The mean percentage changes at 3 years for falling and rising TSH trajectory are −32.6% and +52.4%, respectively. The mean serum TSH concentration for those with a falling trajectory declined from 2.67 to 1.80 mU/L, whereas the mean serum TSH level for the rising group increased from 1.85 to 2.82 mU/L. In contrast to expectation, subjects with a falling TSH also showed a reduction in serum fT4 over time, whereas steady fT4 concentrations were found in participants with rising TSH. Over time, fT3 decreased in all participants (Table 2).
Changes in Thyroid Hormones Over Time (Baseline vs. Year 3) as Stratified by Serum Thyrotropin Trend
Table 2 depicted the changes in free thyroid hormones over 3 years according to TSH trend. A falling TSH trajectory is defined by a reduction in serum TSH of ≥0.1 MU/L over time. An increase in serum TSH of ≥0.1 MU/L over time indicates a rising TSH trend. The TSH value at baseline and 3 years was represented by mean and 2.5–97.5 percentile. The mean difference between free thyroid hormone at baseline versus 3 years was compared with Wilcox-sign and paired t tests, for free T4 and free T3, respectively.
Falling TSH group mean (2.5–97.5 percentile) at baseline = 2.67 (0.79–5.67), year 3 = 1.80 (0.50–3.74), % change −32.6.
Steady TSH group mean (2.5–97.5 percentile) at baseline = 1.66 (0.31–4.32), year 3 = 1.67 (0.31–4.36), % change +0.6.
Rising TSH group mean (2.5–97.5 percentile) at baseline = 1.85 (0.42–4.51), year 3 = 2.82 (0.76–7.30), % change +52.4.
All cohort TSH group mean (2.5–97.5 percentile) at baseline = 2.33 (0/41–6.48), year 3 = 2.04 (0.39–6.27), % change −12.4.
TSH trajectory, baseline to year 3, predicted future cognitive function
Of the participants whom had repeated thyroid function tests at 36 months, 99.4% (n = 346) and 79.3% (n = 276) were reassessed on the MMSE at 3 and 5 years, respectively. General linear modeling showed that change in serum TSH concentration over 3 years was positively associated with change in MMSE score at 3 (β 0.31; CI 0.01–0.611; p = 0.045) and 5 years (β 0.52; CI 0.08–0.95; p = 0.020). Subgroup analysis, stratifying serum TSH according to the direction of change, showed that only those who had a falling TSH concentration at 3 years exhibited a positive association with a change in MMSE. Falling TSH concentration was associated with a reduction in global cognition. Greater reduction in MMSE score was associated with larger TSH decline, at 3 (β 1.15; CI 0.47–1.83; p = 0.001) and 5 years (β 2.12; CI 1.01–3.23; p < 0.001), respectively.
Using logistic regression modeling, a reduction in serum TSH from baseline to 3 years was associated with increased odds of incident cognitive impairment (MMSE <26) at 5 years in those surviving 5 years; OR 1.77 (CI 1.19–2.61); p = 0.004), but not at 3 years (Fig. 2). These associations also held for fully adjusted models when incident cognitive impairment was redefined as MMSE <24. Apart from incident cognitive impairment (MMSE <26), a reduction in TSH concentrations over time was also associated with cognitive decline, defined as falling MMSE scores ≥3 points over 5 years (OR 1.45 (CI (1.01–2.09), p-value 0.049) (Fig. 2). This relationship was stronger among those who had normal cognition at baseline (OR1.73 [CI (1.06–2.80]; p = 0.027).
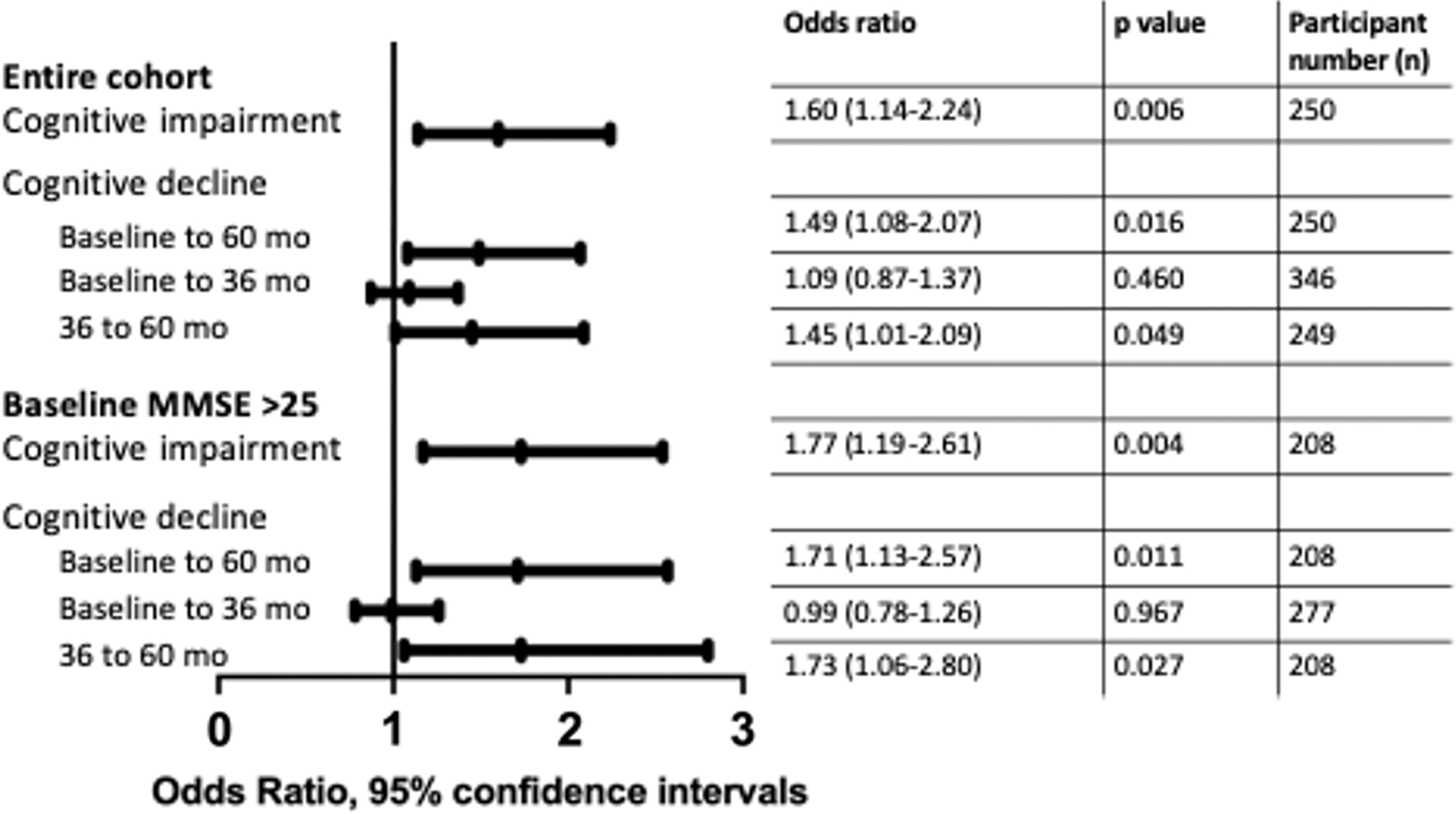
Decreasing TSH trajectory and the odds of incident cognitive impairment (MMSE <26) at 60 months, and cognitive decline (reduced MMSE score ≥3) over 5 years. MMSE, Mini-Mental State Examination.
Relationship between baseline TSH and cognitive performance
At baseline, participants in the lower TSH tertile had a greater prevalence of cognitive impairment (p = 0.002), worse performance in word recognition sensitivity (p = 0.001), PoA (p = 0.036), and CoA (p = 0.034), compared with those in the upper TSH tertile (Table 1). The associations between baseline thyroid function and cognitive performance over 3- and 5 years of follow-up were examined with linear mixed models (Table 3). Lower baseline serum TSH was found to be associated with worsening sustained attention (CoA) over 3 years in individuals both with (p = 0.03) and without (p = 0.012) baseline cognitive impairment. There was no significant relationship between baseline serum TSH and global cognition (MMSE score) over time.
Effects of Baseline Thyroid Function on Global Cognition Over 60 Months and Episodic Memory and Attention Over 36 Months
Model 1, assesses the cross-sectional effect of baseline thyroid function on each cognitive domain.
Model 2, an interaction of baseline thyroid function and time, indicating the changes in cognition over time that can be attributed to a variation in baseline thyroid function.
Lower scores in transformed MMSE, word recognition sensitivity, delayed word recall, PoA, and CoA indicate better cognitive function.
The sections highlighted in bold indicate results which were statistically significant.
Categorical TSH analysis with middle TSH tertile as referent; the effects of upper TSH tertile on all cognitive domains were all nonsignificant (results not shown).
SE, standard error.
Relationship between serum free thyroid hormones and cognitive state
In the whole cohort, lower fT3 at baseline was found to correlate with worse initial MMSE performance (p = 0.002) (Table 3; model 1). Among individuals who were cognitively intact at initial assessment, lower baseline fT3 was associated with worse global cognition over time (p = 0.031) (Table 3; model 2). Contrastingly, lower baseline fT4 correlated with better MMSE performance over time (p = 0.005) (Table 3; model 2). There was no evidence that prospective changes in fT3 and fT4 from baseline to year 3 were associated with changes in cognitive status over time.
To account for censoring due to death or withdrawal, Cox Proportional Hazards regression models were fitted to further examine the relationship between baseline thyroid function and risk of developing cognitive impairment (MMSE <26). Thyroid function was modeled in two ways. First, the baseline values of each thyroid parameter were fitted in separate models with age and sex included as covariates in Model 1, and all covariates in Model 2. These models assumed a linear relationship between the thyroid parameter and the hazard for cognitive impairment. There was no evidence of a significant relationship between any of the baseline thyroid parameters and the incidence of cognitive impairment as defined by MMSE <26 (Table 4). Cubic spline models suggested that the linear relationship was satisfactory (Fig. 3). We repeated all analyses with the assumption of cognitive impairment as MMSE <24 and found evidence that higher fT3 was protective of cognitive impairment after adjustment for all covariates (Hazard ratio = 0.77, CI = 0.60–0.99, p = 0.04).

Restricted cubic spline curves of the relationship between TSH, fT4, fT3, and hazard ratio for cognitive impairment (MMSE <26), adjusted for age, sex, education, smoking, physical activity score, disease count, Geriatric Depression Score, CRP, and waist/hip ratio. CRP, C-reactive protein; fT3, free triiodothyronine; fT4, free thyroxine.
Relationship Between Baseline Thyroid Hormones and Time to Onset of Cognitive Impairment (MMSE <26); Hazard Ratios (per Unit Increase) and 95% Confidence Intervals
The section in bold indicates result which was statistically significant.
Adjusted for age and sex.
Adjusted for age, sex, education, smoking, physical activity score, disease count, Geriatric Depression Score, waist/hip ratio, and CRP.
HR per SD increase of: 1.539 mU/L TSH, 0.434 pmol/L fT3, 2.223 pmol/L fT4.
CI, 95% confidence interval; HR, Hazard ratio; SD, standard deviation.
Discussion
No previous study has looked at serial change in thyroid function over time in very old individuals. In health, there is a reciprocal relationship between serum TSH and free thyroid hormones, around a notional set-point for the hypothalamo-pituitary-thyroid axis: low TSH being associated with higher free thyroid hormones and vice versa. In contrast, in this cohort of 85-year-old individuals, we found that a reduction in serum TSH concentration over time was associated with the falling fT4 and fT3. This suggests for the first time that falling serum TSH in advanced old age may reflect a pattern of central hypothyroidism, possible owing to changes in hypothalamo-pituitary state or an increasing burden of non-thyroidal illness with age, rather than mild thyroid hormone excess. Interestingly, parallel observations have been made in aged rodents, with lower peripheral thyroid hormone concentrations but the minimal change is TSH (21,22).
On the other hand, we observed a trend of rising TSH without associated falling in fT4 levels. This suggests potential thyroid resistance or reduced thyroid sensitivity to TSH action and that a compensatory rise in TSH is needed to maintain serum T4. These findings have profound implications for the interpretation of low serum TSH concentrations in very old people and for the management of “subclinical hyperthyroidism,” a condition defined solely by abnormal TSH concentrations, which increases in prevalence with advancing age (23).
The main focus of our study was cognition. We found that lower baseline TSH and fT3, and higher fT4 were associated with worse cognitive outcomes. This is in keeping with other prospective epidemiological studies in younger patient cohorts (2 –6), and it confirms that this association holds in the very old. A wide variety of intercurrent illnesses may transiently affect serum thyroid hormone concentrations (24), and 30–75% of individuals with a one-off low serum TSH will show recovery to the reference range with a year (25,26). This means that observational studies where subjects are stratified on the basis of a single measurement of thyroid function are prone to confounding by misclassification (27). This study shows for the first time that a decreasing TSH trajectory between the ages of 85 and 88 years predicted the development of cognitive decline and incident dementia by the age of 90 years. This suggests that a common factor(s) could underlie both decreasing serum TSH concentration and the development of dementia.
Although low serum TSH has been reproducibly associated with dementia and cognitive impairment in observational studies (2,6), the pathophysiological mechanisms underlying this finding are unclear. Reducing serum TSH in younger individuals would be suggestive of the development of primary thyroid autonomy or mild hyperthyroidism. However, in this very elderly population, individuals with falling serum TSH between the ages of 85 and 88 also had decreasing serum fT4 and fT3 concentrations, which contradicts our usual understanding of the TSH/free thyroid hormone relationship.
Changes in thyroid function with age are complex. Older individuals have a high disease burden, with transient infection, chronic inflammatory or degenerative conditions that tend to cause a central downregulation of the thyroid axis, termed “sick euthyroid syndrome,” that can lead to reduced serum TSH and fT3. There is also a reduced conversion of T4 to T3 during “non-thyroidal illness,” and decreased hepatic clearance of thyroid hormones and reduced type 1 deiodinase activity in older individuals. However, aging is also associated with pathophysiological changes in the central hypothalamo-pituitary-thyroid axis (28,29). A blunted pituitary response to thyrotropin releasing hormone (TRH) and a lesser degree of TSH elevation in response to hypothyroidism have been observed in older individuals, with or without dementia (30 –32). Older people with hypothyroidism also require less levothyroxine replacement to maintain the same TSH (33). Hence, aging may modify the hypothalamic TRH or the pituitary TSH secretory response.
Another explanation for our findings might be that the underlying brain involution and pathological changes preceding dementia could result in lower circulating TSH levels, before the clinical manifestation of cognitive impairment. Pseudodementia is a well-recognized manifestation of overt hypothyroidism, and a contrasting hypothesis is that lower TSH levels reflect relative central hypothyroidism that could be driving the cognitive impairment. The latter would mean that therapeutic manipulation of thyroid hormone status could be worthwhile in cognitive impairment and dementia.
Our prospective observational study has some limitations. A relatively small number of individuals were studied, and with progressively lower numbers of repeated thyroid function and cognitive assessment at follow-up visits (owing to mortality), there was less power to detect a significant difference in cognitive performance, particularly using the MMSE as this was not administered at every interview. We have included various confounders, including comorbidity and medication use, but there may be other less common yet important conditions that have not been included.
There was also a change in the study population after incorporating the selection criteria for thyroid function. A better physical activity score means a healthier cohort remained for analysis. This potentially improves the sensitivity of the analysis, as the confounders from non-thyroidal illness or co-morbidities were excluded, but the drawback is that the analytic sample is less representative of the general population of the very old. Nevertheless, this is the first prospective study of thyroid changes on cognitive performance over time in this age group and we included participants with advanced frailty and those living in care or nursing homes, as well as those with cognitive impairment or dementia. Hence, our results should be relatively representative of an age-matched population.
In summary, in this cohort of 85-year-olds, declining TSH concentrations over time were associated with falling serum free thyroid hormones, a pattern consistent with relative central hypothyroidism not hyperthyroidism. We show, for the first time, that a decreasing TSH trajectory anticipates cognitive decline in later life. Further studies are now required to better understand the significance of changes in thyroid function in this age group and their relationship to cognitive outcome.
Footnotes
Acknowledgments
This work was supported by the NIHR Biomedical Research Centre at Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle Hospitals Healthcare Charity and Newcastle University. The authors acknowledge the operational support of NHS North of Tyne, the local general practitioners and their staff, the research nurses, laboratory technicians, data management, and clerical team.
Authors' Contributions
E.H.G.: conception and design of the work, analysis and interpretation of data, and article writing. C.J.: design of the work, analysis and interpretation of data, and revising the article. M.E.Y.: analysis and interpretation of data, revising the article. R.D.: analysis and interpretation of data, revising the article. S.H.P.: conception and design of the work, article writing, and revising the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Newcastle 85+ Study was funded by the Medical Research Council (grant no. G0500997), the Biotechnology and Biological Sciences Research Council, Newcastle Healthcare Charity, and the Dunhill Medical Trust. E.H.G. was supported by NIHR Academic Clinical Lectureship.
Supplementary Material
Supplementary Table S1