
Abstract
Background:
Sri Lanka introduced universal salt iodization (USI) in 1995 after which we demonstrated a high thyroglobulin antibody (TgAb) prevalence in 1998. However, it is unclear whether thyroid autoimmunity persists in the long term in populations exposed to sustained USI and whether such populations have an excess of thyroid dysfunction. We evaluated the prevalence of thyroid autoantibodies and dysfunction in Sri Lankan children and adolescents after more than two decades of sustained USI.
Methods:
We selected 10- to 18-year-old subjects of both sexes (randomized cluster sampling) from all 9 provinces of Sri Lanka in this cross-sectional study. Blood, urine, and anthropometric data were collected and thyroid ultrasound scans were performed. Validated statistical methods were used to derive local population-specific reference ranges for all thyroid parameters. We also measured urine iodine concentration (UIC), salt, and water iodine concentrations.
Results:
Blood and urine samples from 2507 and 2473 subjects respectively, and ultrasound scans from 882 subjects were analyzed. Population-derived upper limits for thyroid peroxidase antibody (TPOAb) and TgAb, and reference ranges for triiodothyronine, thyroxine, and thyrotropin (total and age-year-related groups) were significantly different from manufacturer's reference ranges. Using these derived ranges, the prevalence of TPOAb was 10.3% and TgAb was 6.4%. Of the TPOAb-positive subjects, TPOAb were of low concentration in 66.2% (1–3 times the upper limit of the reference range [ULRR]) and showed the strongest association with subclinical hypothyroidism (SCH) at the highest concentrations (>4 ULRR). The prevalence of SCH was 3%. Median UIC (interquartile range) was 138.5 μg/L (79.4–219.0) with regional variability, and median thyroglobulin was 8.3 ng/mL (4.1–13.5). Goiter prevalence was 0.6% and 1.93% (thyroid volume compared to age and body surface area, respectively). Salt and water iodine concentrations were satisfactory.
Conclusions:
Sri Lanka has safely and effectively implemented USI with good sources of iodine, leading to sustained iodine sufficiency over more than two decades. The early postiodization TgAb surge (42.1%) has settled (6.4%), and despite a persistently high TPOAb prevalence (10.3%), SCH prevalence remains low (3%). Further studies should be undertaken to monitor thyroid autoimmune dysfunction in Sri Lankan children, using age-specific, population-derived reference ranges.
Introduction
Autoimmune thyroid disease (AITD) affects 5% of the population in iodine-sufficient countries and may cause significant morbidity (1 –3). In children, thyroid dysfunction may delay educational milestones and impair growth and development (4). AITD is usually precipitated by an environmental trigger (e.g., iodine) in genetically predisposed individuals and is characterized by lymphocytic infiltration of the thyroid gland and the development of autoantibodies to the thyroglobulin antibody (TgAb), thyroid peroxidase antibody (TPOAb), and the thyrotropin receptor antibody (5 –7). Although iodine deficiency remains an important problem (8 –10), universal salt iodization (USI) has helped reduce it significantly (9,11), while occasionally increasing thyroid autoantibody prevalence in iodine-supplemented communities (12 –17).
Sri Lanka implemented USI in 1995 and has been consistently iodine sufficient (18). We observed a high prevalence of TgAb (42.1%) in schoolgirls in our study soon after, in 1998 (12). These TgAb were low titer, recognized nonautoimmune epitopes, and reduced with time, suggesting a transient response to iodization (19,20). Postiodization studies from other countries have also reported this phenomenon. However, these studies were relatively small, done at variable times after USI, and defined thyroid autoimmunity using assay reference ranges derived mainly from adult European populations (21 –24).
Currently, it is uncertain whether increased thyroid autoimmunity persists in the long term during sustained USI, and if so, whether these autoantibodies have any functional significance. In this study we use local population derived thresholds to evaluate thyroid autoimmunity and function in children and adolescents after 22 years of sustained USI in Sri Lanka. Our report complies with STROBE guidelines (25).
We hypothesized that long-term sustained USI changes thyroid autoantibody prevalence without causing significant thyroid dysfunction. Thus, the primary study aims were to assess the prevalence of (a) TPOAb and TgAb; and (b) thyroid dysfunction in 10- to 18-year-old subjects in Sri Lanka, using local population-derived reference ranges to determine the relationship between thyroid antibodies and thyroid dysfunction in this population. The secondary study aims were to assess (a) community iodine nutrition; and (b) thyroid volume (TV) relative to age and body surface area (BSA) in this population.
Methods
Participants
This cross-sectional study was undertaken between July and November 2017. The sample size was calculated using the formula “n = (z 2 × p × q/d 2) × D,” and a sample size of 2700 was chosen allowing for a 5% nonresponder rate (S1).
Inclusion criteria—All males and females aged 10–18 years were included. Exclusion criteria—Subjects with chronic disorders requiring long-term treatment were excluded.
Subjects were recruited using a random, multistage, stratified cluster sampling technique using a probability proportional to size model (S2). Fifteen schools were selected randomly from each of the 9 provinces of Sri Lanka (Supplementary Fig. S1) from the Ministry of Education Schools Census for 2017, and a single class chosen from each school by drawing lots. Ten males and 10 females were randomly selected from each class (Fig. 1). Informed consent was obtained from parents or guardians. The Regional Director of Education, individual heads of schools, and the local Research Ethics Committee (MRI, Sri Lanka, 18/2015) approved the study.

Flow diagram showing participant recruitment. Children aged 10–18 years of both sexes were recruited using a random stratified cluster sampling technique and a probability proportional to size model from all nine provinces of Sri Lanka. Twenty children were selected randomly from each of 15 schools in the nine provinces. *Children unavailable because of ill health, being away on school duty, involvement elsewhere in sports and other educational activities. fT3, free triiodothyronine; fT4, free thyroxine; Tg, thyroglobulin; TgAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin; TV/BSA, thyroid volume/body surface area; UIC, urine iodine concentration; US TV, ultrasound thyroid volume.
Processing of samples
Trained field investigators visited schools to collect anthropometric data, and blood and urine samples. Following venipuncture, serum was separated and stored in aliquots at −20°C and a sample of fresh urine collected and stored between 4°C and 8°C, both until transport to the Central Laboratory in Colombo. Each subject brought drinking water from home in investigator-provided bottles. Samples were transported to the Central Laboratory twice weekly and stored at −80°C pending analysis. Commercial salt samples from two manufacturers were collected from retailers within the localities where study subjects lived.
Ultrasound TV
Scanner operators were qualified doctors trained by a U.K. Radiologist specializing in soft tissue imaging and were blinded to all subject-related data. Scans were performed with subjects seated with neck hyperextended, using a 7.5 MHz transducer (LOGIQ V2, GE Ltd. China). The volume (mL) of each lobe was calculated using the following formula: “width × length × thickness (all cm) × 0.479.” The two lobes were added (isthmus disregarded) to give a final volume. TV in these subjects was compared with TV from 15,986 Indian children aged 5–17 years from iodine-sufficient regions—goiter was defined as TV >97th percentile for age, and BSA (26). These standards were more appropriate because of closer geographic, age, and ethnic identity compared with standards derived from European reference populations.
Agreement between scanner operators was calculated using the Bland–Altman method (27). The mean percentage bias was 0.72 (95% confidence interval [CI −6.54% to 5.09%]) for scanner 1 versus 2, −1.42% [CI −7.43 to 4] for scanner 2 versus 3, and −2.14% for scanner 1 versus 3 [CI −7.03 to 2.74%].
Anthropometric measurements
Heights and weights were measured using standardized stadiometers and UNICEF-approved electronic scales (Seca GmbH, Model 869 1321004, Germany), respectively. Information about personal, family history, and medications was documented. BSA was calculated as “weight (kg)0.425 × height (cm)0.725 × 71.84 × 10–41.”
Assay methods
Thyrotropin (TSH), TgAb, TPOAb, and thyroglobulin (Tg) were measured with a sandwich chemiluminescence immunoassay, and free triiodothyronine (fT3) and free thyroxine (fT4) were measured using a solid-phase antigen-linked assay with isoluminol and magnetic particles (all DiaSorin, Saluggia, Italy). All assays were done on a Liaison Immunoassay Analyzer (DiaSorin). The reference Medical Research Council standard 80/558 was used for calibration. Internal quality control samples were used to determine between-batch coefficient of variation, which were all within the manufacturer's recommendations—TSH, 9.7% at 5.6 mIU/L; TgAb, 9.3% at 78.1 IU/mL; TPOAb, 7.9% at 15.2 IU/mL; and Tg, 5.7% at 10.9 ng/mL.
The manufacturer's reference ranges were as follows: fT3 2.2–4.2 pg/mL, fT4 0.8–1.7 ng/dL, TSH 0.3–3.6 mIU/L, Tg 0.2–70 ng/mL, TPOAb 1–16 IU/mL, and TgAb 5–100 IU/mL.
Urine iodine concentration (UIC) and water iodine concentration were measured using ammonium persulfate digestion with spectrophotometric detection of the Sandell–Kolthoff reaction (S3). Samples with known iodine values were used for internal quality control with duplicate testing of low- and high-value samples. External quality control was assured through the EQUIP program of the CDC, Atlanta, GA (S4).
Salt iodine content was measured using the “titration method” (S5).
Population-derived reference ranges
We derived local population-specific reference ranges (2.5th–97.5th percentiles) for TSH, fT4, and fT3 according to the National Association of Clinical Biochemistry (NACB) criteria (28). The reference population was defined by excluding subjects with a personal or family history of thyroid disease, goiter, autoantibodies, and abnormalities on ultrasound scans where available (n = 1437). For TPOAb and TgAb, we determined the 97.5th percentile using a reference population of males with TSH 0.5–2.0 mU/L, with no personal or family history of thyroid disease, no goiter, and no ultrasound scan abnormalities where available (n = 436) (28).
Statistical methods
Data are summarized as median (interquartile range [IQR]) for non-Gaussian or mean (±standard deviation) for Gaussian data (the Shapiro–Wilks test was used to determine normality). The Mann–Whitney test was used for comparison between two groups of continuous variables. The Kruskal–Wallis test was used to compare more than two groups of continuous variables. Categorical variables were analyzed using the chi-squared test for trend, all using AnalyseIt (AnalyseIt, Yorkshire, United Kingdom).
Because of significant differences between manufacturer-recommended and reference population-derived autoantibody cutoffs, we determined an optimal autoantibody cutoff that best identified individuals with subclinical hypothyroidism (SCH), that is, a functional cutoff (29). For this, we explored a nonlinear relationship between TPOAb and TgAb concentrations and SCH, using restricted cubic splines to allow flexible smooth transformation of the relationship. We used the mkspline command in Stata (Stata Corp LLC, TX) to set 3 equally spaced knots at 10, 50, and 90 percentiles (30). Results were obtained from logistic regression models adjusted for age, sex, and body mass index (BMI) with reference values for the splines set at 12 and 10 IU/L for TPOAb and TgAb, respectively (Supplementary Methods Section S1).
Restricted spline regression models were also used to investigate the relationship between antibody concentration and other continuous variables: TSH, fT4, fT3, Tg, and UIC. These relationships were modeled using ordinary least squares linear regression models corrected for age, sex, and BMI (Supplementary Methods Section S1).
To understand the risk factors for SCH, we derived odds ratios (ORs) and CI using multivariate binary logistic regression models. Independent variables included in the model were age, sex, body mass index, as well as variables that attained a significance of p < 0.1 in univariate analysis. The Hosmer–Lemeshow statistic was used to test goodness of fit (31).
Results
Participant characteristics
Participant recruitment is shown in Figure 1. The final sample was 2507 participants from whom 2507 blood and 2473 urine samples were available for analysis. Thyroid ultrasound scans were available in 882. There was no difference in UIC, thyroid hormones, TSH, and autoantibodies between subjects who did and did not have thyroid ultrasound scans.
Participant characteristics are shown in Table 1. Females (53%) had higher TV, goiter and TgAb prevalence, and fT4, while males (47%) had higher fT3 concentrations.
Characteristics of Study Subjects and the Prevalence of Thyroid-Related Parameters in Males and Females
There was a significant difference in the prevalence of goiter and TgAb, and in TV/BSA and fT4 between females and males (p < 0.001). p-Values are for trends between males and females. Figures are numbers (%) or median (IQR).
TPOAb cutoff 28 IU/L.
TgAb cutoff 50 IU/L from local population-based cutoff points.
BSA, body surface area; fT3, free triiodothyronine; fT4, free thyroxine; IQR, interquartile range; Tg, thyroglobulin; TgAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin; TV, thyroid volume; UIC, urinary iodine concentration.
Population-derived reference ranges
Thyroid hormones
Reference ranges were derived for TSH, fT4, and fT3 (n = 1437) for (a) the total group: TSH 0.75–5.88 mU/L, fT4 0.85–1.80 ng/dL, and fT3 2.21–5.22 pg/mL, and (b) for each age-year group. The reference limits for TSH and fT3 decreased progressively with increasing age, whereas fT4 showed an age-related increase. All derived reference ranges had a higher upper limit compared with the manufacturer's reference ranges (Supplementary Table S1).
TPOAb and TgAb
We found significant discrepancies between the reference upper limits derived according to the NACB criteria and that recommended by the manufacturer. For TPOAb, the derived upper limit was 53.7 IU/mL (NACB) compared with the manufacturer's upper limit of 16.0 IU/mL, while for TgAb, the derived upper limit was 53.8 IU/mL (NACB) compared with the manufacturer's upper limit of 100 IU/mL. To address this inconsistency, we determined the functional antibody cutoff as an optimal cutoff that best identified individuals with SCH. A nonlinear relationship was seen between antibody concentrations and SCH risk (Fig. 2). For TPOAb, SCH risk started at 28 IU/L corresponding to the 92nd percentile of the antibody reference population. The manufacturer's upper limit 16 IU/L (82nd percentile) was too low and nondiscriminatory for SCH. For TgAb, SCH risk started at 50 IU/L (97th percentile), while the manufacturer's upper limit of 100 IU/L corresponded to the 98th percentile (Fig. 2).

The relationship between TPOAb and TgAb concentrations and the risk of subclinical hypothyroidism. This figure shows the relationship between TPOAb and TgAb concentrations and the risk of SCH defined as TSH >5.88 mU/L and fT4 within the local population-derived reference range. Curves in (
Thyroid autoantibodies, hormones, and iodine nutrition
TPOAb showed a positive relationship with TSH, and an inverse relationship was seen with fT4 and fT3. There was no consistent relationship for Tg or UIC. TgAb was also positively associated with TSH but negatively associated with fT3, with no significant relationship with fT4, Tg, or UIC (Supplementary Fig. S2).
Prevalence of thyroid autoantibodies
TPOAb prevalence was 10.3% using the population-based functional limit of 28 IU/L and 21% with the manufacturer's upper limit of 16 IU/L. TgAb prevalence was 6.4% using the population-based functional limit of 50 IU/L and 4.2% with the manufacturer's upper limit of 100 IU/L.
Prevalence of thyroid dysfunction
The prevalence of SCH was determined using the (a) manufacturer-recommended, (b) total group-derived, and (c) age-year group-derived upper limits for TSH (Fig. 3). The prevalence of SCH was significantly lower using the total group-derived (3%) compared with the manufacturer's upper limit (16.8%). Similarly, the age-year-derived upper limits were also significantly lower and most marked in the younger age groups. The prevalence using the age-year-specific upper limit increased progressively from 1.8% to 3.3% from the youngest to the oldest age group, while the prevalence using the total group-derived upper limit decreased from 4.5% to 2.4%. The manufacturer-recommended TSH upper limit overestimated SCH at all age groups, while the total group-derived upper limit overestimated the prevalence in the youngest age ranges (Fig. 3). In binary logistic regression, SCH was associated with BMI (OR 1.10, [CI 1.03–1.17], p = 0.004), TPOAb (OR 2.15, [CI 1.17–3.95], p = 0.014), TgAb (OR 5.96, [CI 3.3–10.79], p < 0.001), and Tg (OR 1.17, [CI 1.08–1.27], p < 0.001). There was a significant difference in the prevalence of SCH between TPOAb-positive and TPOAb-negative subjects, and the prevalence of SCH increased with rising TPOAb concentrations (Supplementary Table S2).
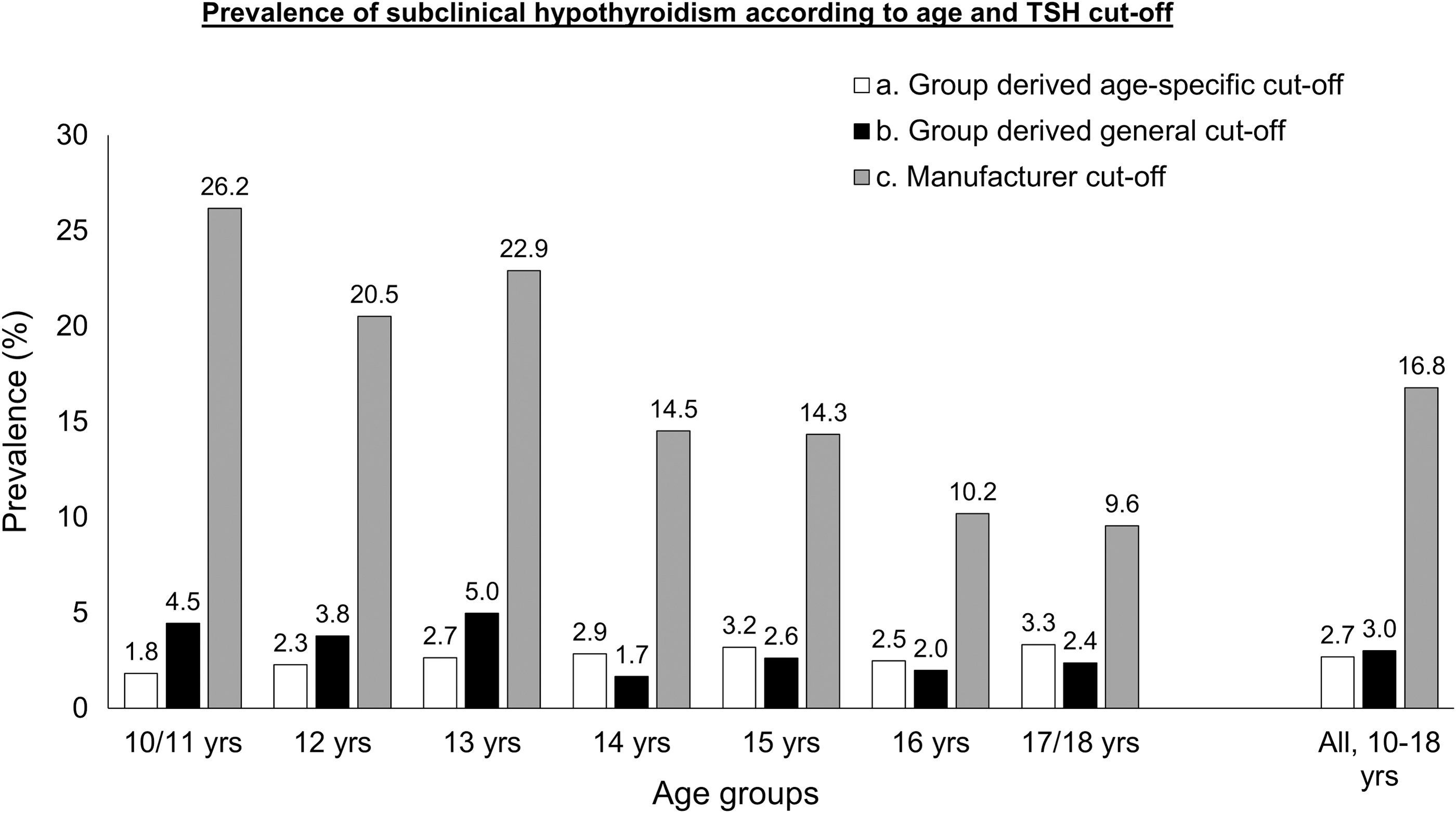
The prevalence of subclinical hypothyroidism according to the upper TSH reference limits using manufacturer's, total group-derived, and age-year group-derived reference ranges. The prevalence of subclinical hypothyroidism varied depending on the reference range utilized—the manufacturer-recommended, total group-derived, or age-year group-derived TSH upper limit. Manufacturer-recommended reference ranges consistently overestimated SCH prevalence compared with the other two ranges. Even when utilizing population-derived reference ranges, the total group-derived reference range consistently overestimated the prevalence of SCH in the younger age groups (10–13 years) compared with age-year-specific reference ranges.
The prevalence of overt hypothyroidism was 0.36%, 0.2% for overt hyperthyroidism, 0.6% for subclinical hyperthyroidism, and 0.52% for isolated hypothyroxinemia.
Urine, water, and salt iodine, and Tg concentration
The median UIC was 138.5 μg/L (79.4–219.0) and median Tg was 8.3 ng/mL (4.1–13.5) and similar for both sexes (p = 0.76, 0.20, respectively). UIC was adequate (100–299.9 μg/L) in 54%, excessive (≧300 μg/L) in 13%, and less than adequate (<100 μg/L) in 33%, although based on a single urine sample. UIC was significantly higher in the Northern compared with the Southern provinces (Supplementary Table S3).
The median (IQR) iodine content in drinking water was 10.1 μg/L (3.1–24) (n = 2007), and the median (IQR) iodine content in commercially available salt samples was 17.5 ppm (11.1–22.8) (n = 200) with regional variability.
Discussion
We have demonstrated in this cross-sectional study of 10- to 18-year-old Sri Lankan children and adolescents (n = 2507) that after 22 years of sustained USI, the prevalence of TPOAb was 10.3%, TgAb 6.3%, and SCH 3%. We have also highlighted the importance of using population-specific and age-year group-derived reference standards when studying children of non-European origin.
The relatively high prevalence of TPOAb (10.3% currently, 8.7% previously) in these Sri Lankan subjects is noteworthy (Fig. 4). These TPOAb were of low concentration, that is, between 1 and 3 times the manufacturer's upper limit of the reference range (ULRR) in 66.2% of TPOAb-positive subjects, were associated with a higher SCH prevalence at higher concentrations (above >3–4 × ULRR), and were not influenced by UIC. The prevalence of TPOAb in children from other parts of the world varied between 2.1% and 6.9%, but local population-derived reference ranges were used only in one such study (S6–S9). A study from Sri Lanka showed a TPOAb prevalence of 41.8% in a group of individuals (median age of 38 years) selected for the presence of a goiter (S10).
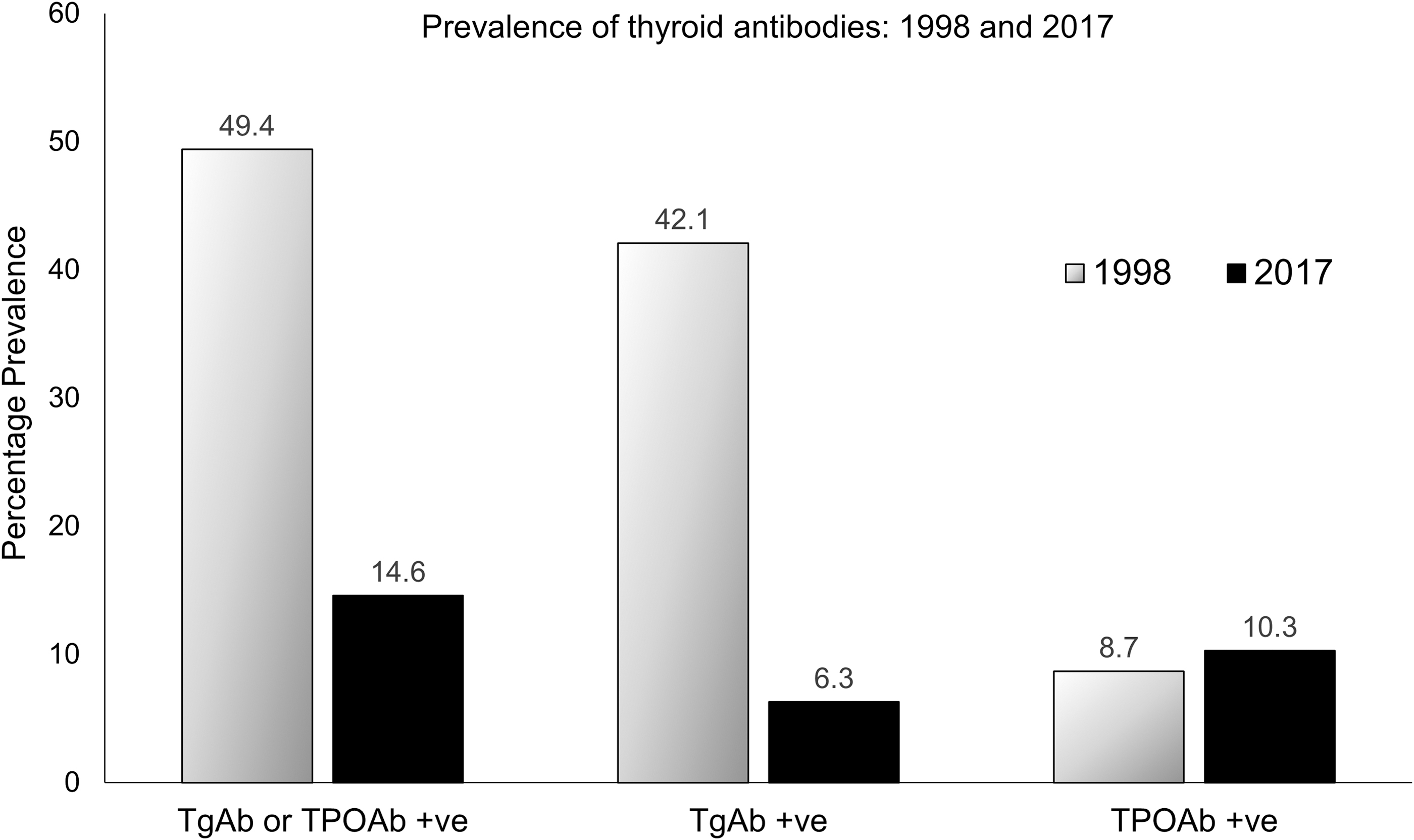
The prevalence of thyroid antibodies in 1998 and 2017. The significant change in the prevalence of total antibody (Total Ab+ve), anti-TgAb, and anti-TPOAb in Sri Lankan schoolchildren over two decades of continuous universal salt iodization is shown here. It should be noted that only schoolgirls aged between 6 and 12 years were studied in 1998 and both girls and boys aged between 10 and 18 years were studied in the current study, and the cross-sectional design of the studies precludes direct comparisons.
We have previously shown an increase in thyroid antibody prevalence in Sri Lanka (20). In 1998, 3 years after USI was first introduced, we reported a high prevalence of TgAb (42.1%) in schoolgirls (Fig. 4). These TgAb, likely caused by iodine-induced Tg epitope reconfiguration (32), were low in concentration and recognized nonimmunodominant epitopes similar to healthy U.K. children (i.e., were “nonpathogenic”) (33). The low TgAb prevalence (6.3%) after more than 2 decades of sustained USI is therefore reassuring, as the initial surge of TgAb did not signal the onset of more widespread AITD. This phenomenon of an early increase of TgAb after USI has been reported elsewhere (21 –24). We note that an increase of both TgAb and TPOAb after long-term USI has also been reported previously, although mainly in adults (34 –38).
Despite the current pattern of autoantibody prevalence, the overall low prevalence of SCH (3%) is reassuring and provides further evidence for the “nonpathogenic” nature of the current antibody profile. The prevalence of SCH in children worldwide is highly variable, but in iodine-sufficient regions varies between 1.7% and 18.4%. These studies were either small (between 270 and 600 in children from India and Nepal), involved children living in areas with high UIC (Korea), or used assay reference ranges derived from Western populations in the majority (S11–S16). Despite the low SCH prevalence in Sri Lanka, the persistent high TPOAb prevalence requires regular monitoring.
Our study highlights the importance of deriving population-specific reference ranges particularly in studies involving children and adolescents. Most European assay manufacturers use reference ranges based on adult European subjects. These ranges are inappropriate for use in these subjects, particularly of non-European origin. In our study, when local population-derived ranges were used, the upper reference limit for TSH was strikingly higher and as a result the prevalence of SCH was 3.0% compared with 16.8% with manufacturer's ranges. For thyroid antibodies, a population-derived functional cutoff represented a more pragmatic threshold for stratifying SCH risk. With this cutoff, TPOAb and TgAb prevalence rates changed from 21% to 10.3%, and from 4.2% to 6.4%, respectively. We have also demonstrated that when children and adolescents of different age groups are studied, defining age-year group-specific reference ranges is important because total group-derived reference ranges may be inappropriate particularly in the youngest age groups where the group reference range overestimated SCH prevalence rates (Fig. 3). We recommend that all future studies involving these subjects should be done using local population-derived reference ranges.
Sri Lanka continues to be iodine sufficient after 22 years of USI (median UIC 138.5 μg/L and median Tg 8.3 ng/mL) with low goiter rates, and good and safe sources of iodine—commercial iodized salt and drinking water. We previously reported the results of iodine surveys between 2000 and 2016, which corroborate the iodine nutrition aspects of our study (18). However, the higher median UIC of 232.5 μg/L (159.3–315.8) in the 2016 national iodine survey (NIS) compared with the median UIC in the current study requires explanation. We believe no single factor explains this difference, but the following may contribute—(a) the difference in the age groups studied with minimal overlap between the 2 (6–12 years in the NIS; 10–18 years in the current study)—the higher UIC in the younger age group is consistent with previous studies elsewhere; (b) dynamic changes over time in local environmental factors or dietary determinants of iodine nutrition (e.g., the introduction of the government salt reduction strategy in 2016); and (c) regional variability of median UIC. However, it is reassuring that both studies showed an overall iodine-sufficient state. The importance of regular review using appropriate techniques should continue to be emphasized.
Our study has several strengths—(a) a large sample size with rigorous selection methodology and analysis; (b) measurement of multiple thyroid-related parameters using population-derived reference ranges more appropriate to a local population of children and adolescents, and (c) the availability of data to evaluate developments over 22 years of USI. However, we are also aware of its limitations—(a) the cross-sectional methodology does not allow direct comparisons with previous studies and (b) TV was measured only in a subset of subjects.
In conclusion, we have shown in this study that the prevalence of SCH has remained low despite a current high TPOAb prevalence (compared with other iodine-sufficient childhood populations). We have also shown the importance of using population-derived reference ranges in studies involving these age groups, as adult-derived assay manufacturer reference ranges may overestimate thyroid-related parameters (e.g., SCH prevalence). This is particularly important when studying non-European childhood populations. Finally, we have also demonstrated that during a period of more than 22 years, Sri Lanka has safely implemented USI and the country has remained consistently iodine sufficient (18).
Footnotes
Acknowledgments
We thank the following for their contributions: (a) Dr. Amila Perera, Dr. Chinthana Sampath, and Dr. Sunil Viraj who carried out thyroid ultrasound scans in the field; (b) the medical laboratory technologists and field technicians who conducted the survey and carried out anthropometric measurements, and sample and data collection.
Authors' Contributions
L.D.P., J.H.L., and R.J. conceived and designed the study. R.J., S.R., and I.P.G. supervised the study. I.P.G. analyzed the ultrasound scans. L.D.P., J.L.C., and O.E.O. performed all statistical analyses. L.D.P., J.H.L., R.J., and O.E.O. drafted the initial article and all authors approved the final version before submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The World Bank, Colombo, Sri Lanka, and the Ministry of Health, Colombo, Sri Lanka, funded this study under the Health Sector Development Projects funding scheme (Grant No. SHSDP/PROJ/CJ/2015/50).
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Figure S1
Supplementary Figure S2