
Abstract
Background:
The worldwide incidence of papillary thyroid carcinoma (PTC) has increased. Efforts to reduce overtreatment follow two approaches: limiting diagnostic workup of low-risk thyroid nodules and pursuing active surveillance (AS) after diagnosis of microscopic PTC (mPTC). However, most studies on AS have been performed in countries with a relatively high proportion of overdiagnosis and thus incidental mPTC. The role of AS in a population with a restrictive diagnostic workup protocol for imaging and fine-needle aspiration remains unknown. Therefore, the aim of this study was to describe the proportion and characteristics of patients with mPTC in the Netherlands and to describe the potential candidates for AS in a situation with restrictive diagnostic protocols since 2007.
Methods:
All operated patients with an mPTC in the Netherlands between 2005 and 2015 were identified from the Netherlands Cancer Registry database. Three groups were defined: (Group 1) mPTC with preoperative distant or lymph node metastases, (Group 2) mPTC in pathology report after thyroid surgery for another indication, and (Group 3) patients with a preoperative high suspicious thyroid nodule or proven mPTC (Bethesda 5 or 6). Only patients in Group 3 were considered potential candidates for AS.
Results:
A total of 1018 mPTC patients were identified. Group 1 consisted of 152 patients with preoperatively discovered metastases. Group 2 consisted of 667 patients, of whom 16 (2.4%) had lymph node metastases. There were 199 patients in Group 3, of whom 27 (13.6%) had lymph node metastases. After initial treatment in Group 3, 3.5% (7/199) of the patients had recurrence.
Conclusions:
Restrictive diagnostic workup strategies of patients with small thyroid nodules lead to limited patients eligible for AS and a higher incidence of lymph node metastases. We believe that there is limited additive value for AS in countries with restrictive diagnostic workup guidelines such as in the Netherlands. However, if an mPTC is encountered, AS can be offered on an individual basis.
Introduction
The worldwide incidence of papillary thyroid carcinoma (PTC) has increased (1 –3). This rising incidence is due to a significant increase in the use of diagnostic imaging modalities (e.g., ultrasonography, computed tomography [CT], and magnetic resonance imaging [MRI]) (4 –7) and the improvement of quality of the postoperative pathological examination (8) as prevalence rates of PTC in autopsies over the past 45 years remain stable (9). The rising incidence of PTC alongside a stable or even declining mortality rate (1,10,11) combined with the stable prevalence in autopsies is highly suggestive for overdiagnosis and overtreatment of PTC (12,13). The latter is in line with the observation that particularly the incidence of microscopic PTC (mPTC, PTC with the largest dimension of 1.0 cm or less) is rising. Where in 1990 only 25% of detected thyroid cancers in the United States was an mPTC, this number increased to 40% in 2008 (13). The clinical significance of mPTC still remains unclear. Some suggest that mPTC are indolent tumors and have no impact on survival and morbidity (1). However, a study by Mehanna et al. (14) suggested the existence of at least two different entities of mPTC. They found that incidental mPTC had a lower incidence of lymph node metastases and a lower risk of recurrence than nonincidental mPTC, and they, therefore, proposed less aggressive treatment in patients with incidentally found mPTC.
Currently, worldwide efforts have been made to reduce overtreatment using a parallel approach, in which a limited workup of incidentally found thyroid nodules is combined with active surveillance (AS) after diagnosis of mPTC. Most international guidelines are shifting to a less aggressive treatment approach to reduce overtreatment mostly by advocating the use of AS instead of immediate surgery for patients with unifocal mPTC without lymph node metastasis. AS entails monitoring the patient over time with neck ultrasounds and only operate when progressive disease is encountered. This strategy reduces the number of patients exposed to surgical morbidity and has comparable oncological outcomes to immediate surgery (15 –17). However, most studies on AS have been performed in countries with a relatively high proportion of overdiagnosis and thus incidental mPTC (18).
The 2015 American Thyroid Association (ATA) guidelines recommend AS as an alternative treatment option for patients with low-risk mPTC and also adopted a more restrictive diagnostic workup for thyroid nodules, advocating not to perform fine-needle aspiration (FNA) in nonpalpable nodules (<1.0 cm) (19). However, if no FNA is performed in the vast majority of nodules <1 cm, AS may not have a large additive value in the reduction of overtreatment. Since 2007, Dutch national guidelines advocated, in contrast to various other earlier guidelines (4,20 –22), to only perform FNA in palpable (assuming larger than 1 cm) nodules (23). In addition, thyroid incidentalomas found on ultrasound, CT, and MRI have no strict indication for further follow-up. Only [18F]2-fluoro-2-deoxy-D-glucose (FDG) positron emission tomography (18FDG-PET)(/CT)-positive incidentalomas are evaluated by means of FNA cytology due to the relatively higher risk of malignancy (24). Currently, the role of AS in a population with a highly restrictive diagnostic workup protocol for imaging and performing FNA remains unclear.
Therefore, the aim of this study was to describe the proportion and characteristics of patients with mPTC in the Netherlands. The potential candidates for AS are described in a situation where more restrictive diagnostic protocols have been implemented since 2007.
Methods
Data collection
Data were obtained from the Netherlands Cancer Registry managed by the Netherlands Comprehensive Cancer Organization (IKNL) and from the Dutch registry of histo- and cytopathology reports (PALGA). Adult patients diagnosed and treated for mPTC in the Netherlands from January 2005 to December 2015 were included. They were identified by means of pathology reports in which the tumor had to be ≤1.0 cm in the largest dimension, using the Eighth Edition of the American Joint Committee on Cancer TNM classification (25). Patients with unknown tumor diameter were also included if the report explicitly stated that a microcarcinoma was found in the specimen. All reports that were identified by IKNL as T1a and T1 were reviewed. Baseline characteristics (age, sex, and follow-up time), findings from the pathology reports (tumor diameter, number of localizations, type of mPTC, coexistence of thyroiditis, vascular/capsular invasion, multifocality, bilaterality, extrathyroidal extension, lymph node involvement, BRAF mutation, encapsulating tumor and complete [R0] or less than complete [R1 and R2] resection), follow-up, and recurrence data were collected. Recurrence was defined as local recurrence of disease, the occurrence of lymph node metastases and distant metastases after initial treatment. This study was approved by the Medical Ethics Committee of the Erasmus Medical Center (MEC-2018-1195). The STROBE guideline for reporting observational studies was used.
Patients
Three patient groups were defined: (Group 1) patients with preoperative pathologically proven lymph node or distant metastases of mPTC, (Group 2) patients with mPTC in a pathological specimen after thyroid surgery for another indication (e.g., Graves' disease, Bethesda 3 or 4 nodules, multinodular goiter), and (Group 3) patients with a preoperative high suspicious thyroidal nodule or proven mPTC (Bethesda 5 or 6). Patients in Group 1 are not candidates for AS due to lymph node or distant metastases. As patients in Group 2 underwent surgery for another indication, they are not candidates for AS for mPTC (incidentally) found in the specimen. Patients in Group 3 were classified as potential candidates for AS.
Statistical analyses
Descriptive statistics were used to express continuous variables with normal distribution as mean with standard deviation or abnormal distribution as median with interquartile range (IQR). Distribution was assessed using the Shapiro–Wilk normality test. Categorical variables are described as count (n) and percentage (%). Differences between the groups were analyzed using the Mood's median test for continuous variables and the Pearson chi-square test or Fisher's exact test for nominal variables.
The Kaplan–Meier method was used to estimate recurrence-free survival, and the log-rank test was used to evaluate statistical differences in recurrence between the different groups. IBM SPSS Statistics 25 (IBM Corp., Armonk, NY) and R 3.6.3 were used to perform all statistical analyses. p-Values of <0.05 were considered significant. No data imputation was used for missing data.
Results
Patient and treatment characteristics
From January 2005 to December 2015, a total of 6477 patients were diagnosed with thyroid cancer in the Netherlands (26). A total of 1459 patients were identified as T1a or T1. After review of the pathology reports, 441 patients were excluded (Fig. 1). In 1018 patients, an mPTC diagnosis was confirmed, representing 15.7% of the total number of thyroid cancer cases in the study period in the Netherlands. Patients had a median follow-up time of 68.7 [IQR: 42.8–102.6] months. The median age at time of diagnosis was 50.0 [IQR: 41.0–60.0] years and 75.8% were female. The median tumor diameter in the pathological specimen was 6.0 [IQR: 3.0–8.0] mm. In total, 368 (36.1%) patients underwent a total thyroidectomy, 240 (23.6%) underwent a completion thyroidectomy, and 401 (39.4%) patients underwent a hemithyroidectomy. In total, 397 (39.0%) patients received radioiodine ablation (RAI) treatment after total or completion thyroidectomy, and therapeutic cervical lymph node dissection was performed in 170 (16.7%) patients. Prophylactic cervical lymph node dissections were not performed. Additional baseline characteristics are summarized in Table 1.
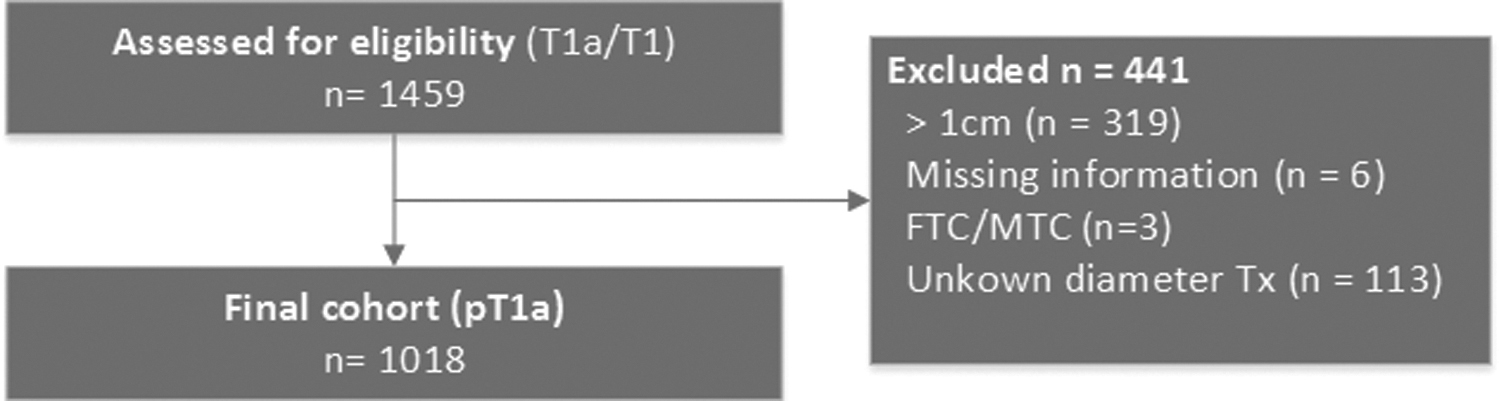
Flowchart of patient enrollment. FTC, follicular thyroid carcinoma; MTC, medullary thyroid carcinoma.
Clinical and Histopathological Characteristics of Microscopic Papillary Thyroid Carcinoma Patients in the Netherlands (N = 1018)
Data are expressed as number (percentage) or as median [IQR]. Missing data are presented in parentheses behind variables.
Certain mPTC but precise diameter unknown.
CLND, concomitant cervical lymph node dissection; CCLND, central CLND (level VI); IQR, interquartile range; LCLND, lateral CLND (levels II–IV) (total number of dissections); mPTC, microscopic papillary thyroid carcinoma; RAI, radioiodine ablation.
AS candidates
Group 1 consisted of 152 patients (14.9%) who were diagnosed with an mPTC and preoperative cytology or pathology-proven lymph node or distant metastases. Group 2 consisted of 667 patients (65.6%) who were incidentally diagnosed after thyroid surgery for another indication. The remaining 199 (19.5%) mPTC patients were treated because of a preoperative Bethesda 5 or 6 result after FNA cytology and categorized into Group 3. Figure 2 shows the yearly distribution of these groups. At highest, 30 patients annually would have been suitable for AS.

mPTC over the period 2005–2015 in the Netherlands. mPTC, microscopic papillary thyroid carcinoma.
Follow-up
Overall, lymph node metastases were found in 19.0% of the total cohort while the percentage of distant metastases was 0.4%. Group 1 showed a lymph node metastases percentage of 98.7% (150/152) preoperatively. Lymph node metastases were found in the surgical specimen in 2.4% (16/667) in Group 2 and in 13.6% (27/199) of the patients in Group 3. The overall recurrence rate in patients was 3.8% (including local recurrence, lymph node metastases, and distant metastases after initial treatment). Recurrence rate was significantly higher in Group 1 compared with Group 2 and Group 3 (19.1% vs. 0.4% vs. 3.5%, p < 0.001) (Fig. 3; Table 2). Tumor diameter in the potential AS group was larger than that in Group 1 and Group 2 (8.0 [IQR: 6.0–9.0] mm vs. 6.0 [IQR: 3.4–8.0] mm and 5.0 [IQR: 2.0–7.0] mm, p < 0.001). Table 2 summarizes additional characteristics.

RFS in the different groups. AS, active surveillance; RFS, recurrence free survival.
Differences in Clinical and Histopathological Characteristics Between the Three Groups
Data are expressed as number (percentage) or as median [IQR].
AS, active surveillance.
Discussion
mPTC of the thyroid accounted for 15.7% of the total amount of thyroid cancers diagnosed in the Netherlands from 2005 to 2015 (26). In this time frame of 11 years, 199 patients were identified as potentially eligible for AS (±3.1% of all thyroid cancers). The burden of mPTC in the Netherlands is strikingly lower than that in other countries. In the United States, nearly half of all identified thyroid cancers were <1.0 cm in 2008 (13). In France, the proportion of mPTC among all operated thyroid cancers was 43.1% (1998–2001) (27). Another study that included data from eight Chinese cancer registries showed that 32.1% of the thyroid cancers between 2000 and 2014 were mPTC (28). The lower incidence of mPTC in the Netherlands is a direct result from a decade long, more restrictive diagnostic workup strategy aiming to reduce the detection of small indolent tumors with no need for treatment at all (23). As expected, more restrictive diagnostic protocol will lead to a population with less frequently diagnosed mPTC and fewer patients who would be eligible for AS. Although the burden of mPTC in the Netherlands is lower than that in other countries, the incidence of mPTC after surgery for another indication has increased over time, which can be attributed to the improved quality of the postoperative pathological examination and reporting (8). Also, an increase in potential candidates for AS can be seen, which could be explained by the increased use of 18FDG-PET(/CT) for the staging and diagnosis of malignancies other than thyroid cancer (29,30).
Patients who could be eligible for AS (Group 3) in the Netherlands have a higher incidence of lymph node metastases (13.6%) when compared with other AS studies. Ito et al. demonstrated that lymph node metastases appeared in only 3.8% of mPTC patients at 10-year follow-up when applying an AS strategy (17). These results are supported by a study from Tuttle et al. (15), in which they closely observed 291 patients with PTC <1.5 cm as an alternative to immediate surgery. They observed tumor growth in 3.8% of the patients and no regional or distant metastases developed during AS. It needs to be noted that median follow-up time was relatively short (25 months, range; 6–166 months) and that they included PTC <1.5 cm (15). More importantly, these studies were performed in a setting where no restrictive diagnostic protocols were applied. The differences in mPTC incidence and the occurrence of lymph node metastases underline the fact that different diagnostic protocols will result in different populations by selection and thereby likely affect the biological behavior of mPTCs in a population. In other words, if a more restrictive diagnostic protocol is being used, less mPTC incidentalomas with indolent behavior are found. This will lead to fewer patients eligible for AS, and when eligible, they may tend to have relatively more lymph node metastases representing a more aggressive selected biological population.
Despite the higher incidence of lymph node metastases in the Dutch population, the Dutch thyroid cancer survival rates were excellent and comparable or even higher than the international survival rates regardless of the more restrictive diagnostic workup. The Dutch age-standardized death rates for men and women are 0.23 and 0.33 per 100,000, respectively. This is lower or comparable to the European and American average death rate for men and women (10,31). The equal survival rates demonstrate that the Dutch workup protocol is an excellent treatment strategy to prevent overdiagnosis and overtreatment of PTC. However, because of the limited number of patients who would be eligible for AS and a higher incidence of lymph node metastases due to patient selection, we believe that a national AS standardized protocol has limited additive value in preventing the overtreatment of PTC. Since the 2015 ATA guideline adopted a more restrictive diagnostic workup strategy, it is expected that if the guideline is followed, AS will not have large additive value in the management of mPTC. However, when an mPTC is incidentally found, despite the restrictive protocol [e.g., by 18FDG-PET(/CT) scan], AS can be offered on an individual basis after discussing the risks and benefits of surgery versus AS with patients. The ideal candidate for AS would be an older patient (>60 years) with a unifocal mPTC without evidence of lymph node metastases, as proposed by the Memorial Sloan Kettering Cancer Center (32). It still remains unclear at which frequency and for how long patients should be followed in an AS protocol. Additional studies are needed to asses these issues, but also the impact on quality of life should be monitored.
This study has several limitations. First, it is a nonrandomized retrospective study. Despite the care of data collection and the use of clear inclusion criteria, some degree of observation bias cannot be ruled out. Second, it should be noted that this study's data are based on histopathological reports and patients who actually underwent AS are therefore not included in this study. However, according to the Dutch guideline, AS was not a treatment option in the study period, and we, therefore, assume that there were few to no patients undergoing AS in this study period. Third, ultrasound data were not available, and therefore, it was not possible to distinguish between Bethesda 5 with or without highly suspicious ultrasound. For this reason, all Bethesda 5 nodules were included in the AS group. Furthermore, the database did not specify the date of RAI treatment. It was therefore not possible to determine the exact number of patients who had cancer-specific RAI treatment or, for example, RAI for Graves' disease preoperatively. Finally, 29 patients with an encapsulated tumor were included. These tumors could potentially be noninvasive follicular tumors with papillary features tumors, which are considered benign in the current era. Unfortunately, it was not possible to reclassify the pathology reports with the present data. However, the number of encapsulated tumors did not differ between the different groups.
Restrictive diagnostic workup strategies of patients with small thyroid nodules results in a low proportion of mPTC and as a consequence a limited number of patients eligible for AS. Furthermore, patients who are eligible for AS in the Netherlands have a higher incidence of lymph node metastasis than in other populations due to patient selection. Based on these data, it can be concluded that in countries with restrictive diagnostic guidelines there is a limited additive value of AS to prevent overtreatment of mPTC. However, if an mPTC is encountered, AS can be offered on an individual basis. We would encourage the collection of follow-up data of patients in AS in national prospective databases.
Footnotes
Authors' Contributions
All the authors contributed to data collection and analysis, drafting of the article, and approved the submitted version.
Author Disclosure Statement
All the authors have no conflicts of interest to declare.
Funding Information
This research did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sector.