
Abstract
Background:
The guideline for managing pediatric thyroid nodules has not been established. We investigated the appropriateness of the Korean Society of Thyroid Radiology (KSThR) guidelines and the need to consider risk factors for managing pediatric thyroid nodules.
Methods:
From August 2007 to February 2020, a database of thyroid nodules in patients younger than 19 years who underwent fine-needle aspiration (FNA) was analyzed. Two radiologists retrospectively reviewed ultrasound images to characterize the nodules according to the Korean Thyroid Imaging Reporting and Data System (K-TIRADS) criteria. Thyroid nodules were divided into benign and malignant nodules. Clinical risk factors were identified, including familial thyroid cancer, history of radiation therapy, and underlying thyroiditis. According to the K-TIRADS categories and the presence of risk factors, malignancy rates were calculated. We compared the diagnostic performance of the original KSThR guidelines and newly suggested criteria for FNA derived by simulation tests with variable size cutoffs in the total study population, a group with risk factors, and a group without risk factors.
Results:
A total of 107 patients (mean age, 13.9 years; range, 4–18 years; 83 females; 50 patients with risk factors) with 133 nodules (71 benign and 62 malignant) were included. The malignancy rate of thyroid nodules was higher in the group with risk factors (64.0%) than in the group without risk factors (43.9%; p = 0.037). Compared with the KSThR guideline (≥1.0 cm for K-TIRADS 4 and 5), the accuracy was higher (62.4% vs. 56.4%) and the unnecessary biopsy rate was lower (44.0% vs. 47.4%) when the new criteria (≥0.6 cm for K-TIRADS 4 and ≥0.5 cm for K-TIRADS 5) were used in the total study population. In particular, in the group with risk factors, the newly suggested size criteria had a much higher accuracy (73.1% vs. 59.7%) and lower unnecessary biopsy rate (30.4% vs. 35.5%) than the KSThR guideline.
Conclusions:
For the management of thyroid nodules in children, it is necessary to consider risk factors and adjust the criteria values for FNA. FNA should be considered in children with risk factors for thyroid cancer even if thyroid nodules are small.
Introduction
Thyroid cancer is the most common malignancy of the endocrine system, and its incidence has been increasing in pediatric populations (1). The prevalence of thyroid nodules in the pediatric population is lower than that in adults and ranges between 0.05% and 5.1%. However, pediatric thyroid nodules are three to five times more likely to be malignant (22–26% vs. 5–10%) (2 –4). In addition, children typically present with more advanced disease at diagnosis and higher recurrence rates (2,5,6).
Ultrasound (US) is the most commonly used imaging modality for screening, diagnosis, and treatment planning of thyroid nodules. Since the Thyroid Imaging Reporting and Data System (TI-RADS) was first proposed in 2009, various TI-RADS systems have been developed. These systems showed a similar performance in the diagnosis of thyroid cancer in adults (7,8) and have been adopted and used in pediatric cases of thyroid nodules with comparable diagnostic performance (9 –11). According to the 2015 guidelines of pediatric thyroid nodules, the criteria for performing fine-needle aspiration (FNA) of thyroid nodules in pediatric patients are consistent with the guidelines for adults (2). However, according to a few recent studies, the TI-RADS system developed for adults is not suitable for children (11,12), and the appropriateness of the Korean Society of Thyroid Radiology (KSThR) guidelines for managing pediatric thyroid nodules has not been assessed.
Although most cases of thyroid cancer occur in populations without risk factors, there are well-known risk factors, including history of radiation therapy (RT), familial history of thyroid cancer, and autoimmune thyroid diseases (4,13). Despite this, there are no specific management plans based on the presence of risk factors for thyroid cancer in pediatric and adult patients using the TI-RADS system.
This study aimed to investigate the appropriateness of the KSThR guideline and to determine the need of considering clinical risk factors for the management of thyroid nodules in children.
Materials and Methods
The institutional review board of our institution approved this retrospective study, and the need for informed consent was waived.
Study population and data set
The clinical data repository system of our institution was used to identify patients aged younger than 19 years who underwent FNA or core needle biopsy (CNB) of thyroid nodules from August 2007 to February 2020. During this time period, 95 patients (122 nodules) underwent FNA, and 25 patients (29 nodules) underwent CNB. Of the 117 patients, 55 underwent thyroid surgery. Final diagnoses were determined from the surgical pathology or the last cytopathological results based on the Bethesda system from FNA or CNB. Indeterminate nodules, including atypia of undetermined significance results (6 nodules in 6 patients), or nondiagnostic results (12 nodules in 10 patients) of the Bethesda system in the cytopathological report without surgical confirmation were excluded. All nodules were divided into benign (Bethesda II or surgically confirmed benign nodule) and malignant (Bethesda VI or surgically confirmed malignancy). Figure 1 illustrates the flowchart of the inclusion and exclusion criteria.
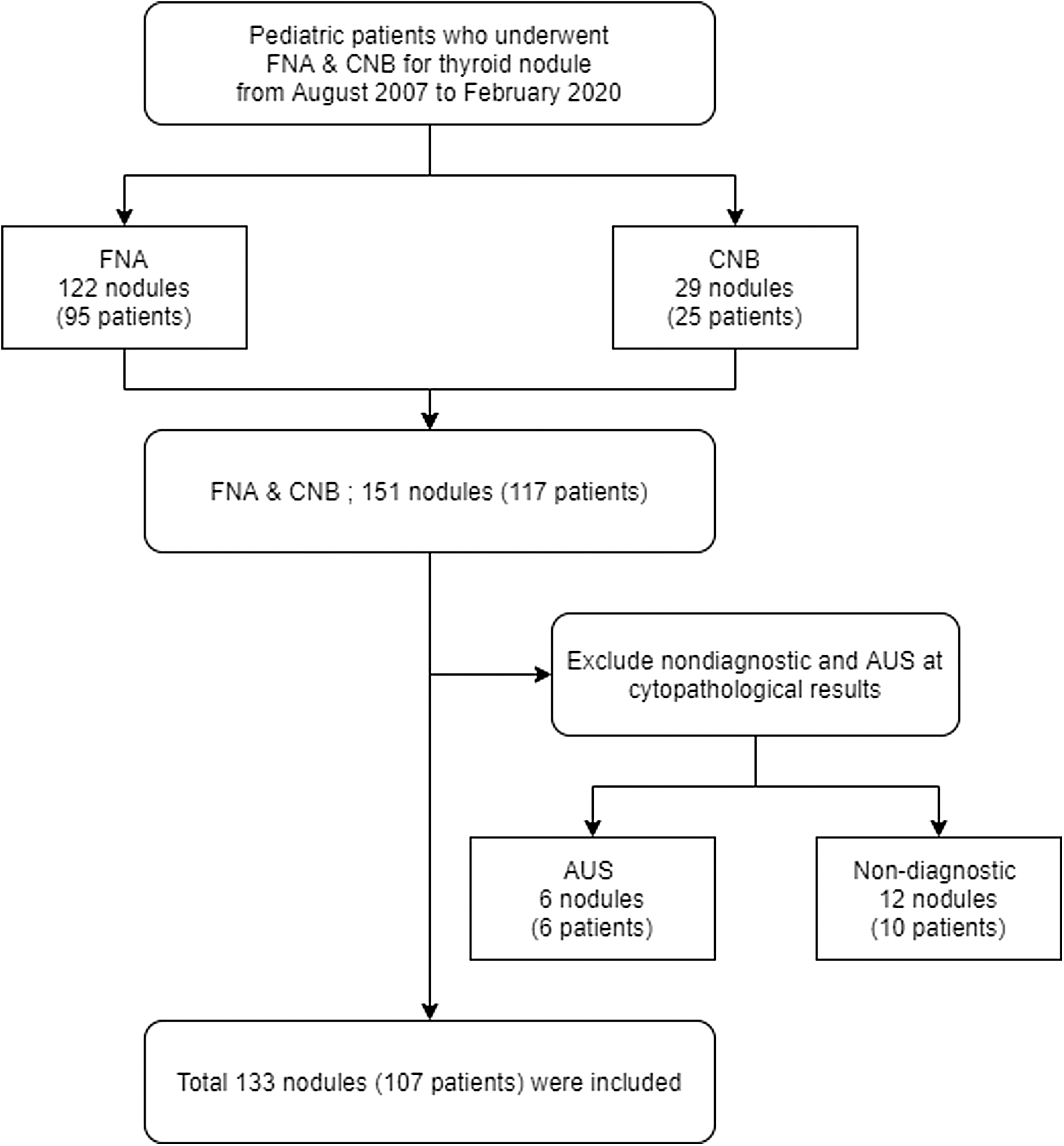
Flowchart of patient inclusion and exclusion. AUS, atypia of undetermined significance; CNB, core needle biopsy; FNA, fine-needle aspiration.
Clinical data
Patients' electronic medical records were reviewed to collect demographic data, clinical risk factor for thyroid cancer, and histopathologic results from the surgical specimen, FNA, or CNB. Risk factors for thyroid cancer include a history of RT, familial thyroid cancer, and underlying thyroiditis (4). Thyroiditis was identified by a pathological examination or a combination of antibody tests and US findings. The history of family thyroid cancer was defined as a patient who had at least one of their first-, second-, or third-degree relatives diagnosed with thyroid cancer (14,15).
US examinations and FNA/CNB
All thyroid US examinations were performed using a high-frequency linear transducer with different US machine (12–5 MHz transducer, Aplio XG, Toshiba, Tokyo, Japan; 12–5 MHz transducer, iU22, Philips Medical Systems, Bothell, WA; 4–15 MHz transducer, Aixplorer, SuperSonic Imagine, Aix-en-Provence, France; 6–15 MHz transducer, Logiq E9, GE Healthcare, Milwaukee, WI). Thyroid US images obtained just before FNA or CNB were analyzed. The average duration between US examination and FNA or CNB was 12.4 ± 30.3 days (range, 0–196 days).
US-guided FNA was performed using a 23-gauge needle with a freehand technique. CNB was performed using an 18-gauge automatic biopsy gun (ACECUT; TSK Laboratory, Tochigi, Japan). In general, FNA was performed if the diameter of a given nodule was 1 cm or larger. Even if the nodule was smaller than 1 cm, the nodule underwent FNA if suspicious US features (microcalcification, nonparallel orientation, and spiculated/microlobulated margin) were present (16). CNB was usually performed in cases of nodules of large size, dense calcification, or prior inconclusive FNA results.
US image analysis
According to the Korean Thyroid Imaging Reporting and Data System (K-TIRADS), the nodules were characterized by consensus between two radiologists (Y.J.C. and S.B.L. with 8 and 6 years of experience in thyroid US, respectively) who retrospectively reviewed the US images without previous radiology or pathology reports. Each nodule was then classified into the K-TIRADS categories (Supplementary Table S1) (16).
Simulation of size cutoff for FNA indication
We evaluated the impact of multiple size cutoffs for FNA of nodules categorized as K-TIRADS 4 and 5, on the diagnostic performance of thyroid cancer. Six size criteria with a difference of 0.1 cm from 0.5 to 1 cm were evaluated. In addition, the patients were divided into three groups (total study population, group with risk factors, and group without risk factors), and each group was evaluated separately.
Moreover, the diagnostic performance of the three FNA simulations was evaluated. Simulation 1 was identical to the KSThR guideline for FNA, and simulation 2 was the same as simulation 1, but only for K-TIRADS 5 nodules using the optional criterion of the KSThR guideline (16). Simulation 3 was a newly suggested size criterion in our study. As the cutoff value for FNA indication, we adopted the size with the highest accuracy for detecting thyroid cancer in diagnostic performance evaluations of multiple size cutoffs for K-TIRADS 4 and 5 nodules.
Statistical analyses
The malignancy risks according to the K-TIRADS categories and the presence of risk factors are calculated as percentages. The association between risk factors and final diagnoses was evaluated using the χ2 test. Subgroup analysis was performed between the groups with each risk factor and the group without risk factors. All thyroid nodules were divided into indicated or not indicated groups according to the FNA indication of the KSThR guidelines, and the missed malignancy rate, defined as the proportion of malignant nodules not included in the FNA indication among all malignant nodules, was calculated.
The diagnostic performance in the detection of thyroid cancer was evaluated (sensitivity, specificity, accuracy, and unnecessary biopsy rates) according to the three guideline simulations. The unnecessary biopsy rate was defined as the proportion of benign nodules among the biopsied nodules (17). The diagnostic performance of the simulations was compared using the binary diagnostic test of clustered samples with the NCSS Statistical Software (Kaysville, UT). This statistical method includes a comparative test and an equivalent test for sensitivity and specificity. This technique is referred to as the ratio estimator approach according to Donner and Klar (18). Other statistical analyses were performed using MedCalc (version 15.2; MedCalc Software, Ostend, Belgium). A p-value <0.05 was considered statistically significant.
Results
Patient and nodule characteristics
In this study, 133 nodules in 107 patients (mean age, 13.9 ± 3.2 years; range, 4–18 years; 83 females) were included. Patient and nodule characteristics based on risk factors are described in Table 1. Among the 107 patients (133 nodules), 50 patients (67 nodules) had risk factor for thyroid cancer: a history of RT (18 patients, 25 nodules), familial thyroid cancer (5 patients, 6 nodules), and underlying thyroiditis (27 patients, 36 nodules). Among patients with risk factor of familial thyroid cancer, three patients (three nodules) had thyroid cancer among their first-degree relatives and two patients (three nodules) had thyroid cancer among their second-degree relatives. There were no significant differences in age or sex between the group without risk factors (mean age, 13.9 ± 3.0 years; 42 females and 15 males) and the group with risk factors (mean age, 13.9 ± 3.5 years; 41 females and 9 males). There were a total of 62 malignant nodules; 58 of them (51 papillary thyroid carcinomas and 7 follicular cancers) were confirmed by histopathology, and the remaining 4 (papillary thyroid carcinomas) had only FNA or CNB results. Among histologically confirmed malignant cases, results of genetic mutation test were available in small number of patients, and the results are represented in Supplementary Table S2. Thyroid nodule size based on the K-TIRADS categories and risk factors is summarized in Supplementary Table S3.
Patient and Nodule Characteristics
Values are mean (standard deviation), expressed in years.
Values were not significantly different between the group without risk factors and the group with risk factors.
CNB, core needle biopsy; FNA, fine-needle aspiration; Hx, history; RT, radiation therapy.
Malignancy rates according to the K-TIRADS categories and risk factors
In the study group, the malignancy rate was 46.6% (62 of 133). Table 2 shows the malignancy rates according to the K-TIRADS categories and risk factors. In the nodule-based analysis, K-TIRADS 4 had a higher malignancy rate (total, 60.0%; group with risk factors, 64.3%; group without risk factors, 50.0%) compared with the malignancy risk from the KSThR guideline (15–50%). The malignancy rates of the other K-TIRADS categories (2, 3, and 5) were similar to the estimated malignancy risk from the KSThR guideline.
Malignancy Rates According to the Korean Thyroid Imaging Reporting and Data System Categories and Risk Factors Based on Nodule Number
Values are malignant/total nodule number and data in parentheses are malignancy rate.
Average risk of malignancy according to the K-TIRADS categories.
K-TIRADS, Korean Thyroid Imaging Reporting and Data System.
In the patient-based analysis, the group with risk factors (malignancy rate, 64.0%, 32 of 50) had a significantly higher malignancy rate (p = 0.037) compared with the group without risk factors (malignancy rate, 43.9%, 25 of 57). Furthermore, the relative risk for the group with risk factors was 1.46 [1.02–2.09] (p = 0.040). In the subgroup analysis for each risk factor, each subgroup had a higher malignancy rate (RT, 66.7%; thyroiditis, 55.6%; familial thyroid cancer, 100%) compared with the group without risk factors (43.9%), but there was no statistically significant difference. The malignancy rates according to the K-TIRADS categories and risk factors based on patient-based analysis are presented in Supplementary Table S4.
Missed malignancy rates with the KSThR guidelines
Missed malignant cases with the KSThR guidelines are summarized in Table 3. According to the KSThR guideline, 21 of 62 (33.9%) malignant nodules (16 in the group with risk factors and 5 in the group without risk factors) were excluded for FNA or CNB, and all missed malignant nodules were in K-TIRADS 4 or 5, except for one K-TIRADS 3 nodule. The group with risk factors had a higher rate of missed malignancies than the group without risk factors (total, 44.4% vs. 19.2%; K-TIRADS 4, 55.6% vs. 16.7%; K-TIRADS 5, 35.3% vs. 18.8%; K-TIRADS 4 and 5, 45.7% vs. 18.2%). Average nodule size of missed malignant nodule based on the K-TIRADS categories and risk factors is presented in Supplementary Table S5.
Missed Malignancy Rates with the Korean Society of Thyroid Radiology Guideline
Values are missed/total malignant nodule number and data in parentheses are missed malignancy rates.
Diagnostic performance in the prediction of thyroid malignancy with the KSThR guideline and simulation
The accuracy in the prediction of thyroid malignancy according to each size cutoff is shown in Figure 2. In K-TIRADS 4, the cutoff value of 0.6 cm showed the highest accuracy for the total study population (60.0%) and the group with risk factors (60.7%), and a value of 0.8 cm showed the highest accuracy for the group without risk factors (66.7%). In K-TIRADS 5, the cutoff value of 0.5 cm showed the highest accuracy for the total study population (73.8%) and the group with risk factors (80.0%), and the 0.8 and 0.9 cm values showed the highest accuracy for the group without risk factors (77.3%). We adopted these cutoff values for each group, and new size criteria for FNA indication were established. The exact cutoff values for each simulation are summarized in Table 4.

Comparison of accuracy for the diagnosis of malignant thyroid nodules according to multiple size cutoff values. This graph shows a comparison of accuracy according to the variable nodule size threshold for K-TIRADS 4 (
Size Cutoff Values for Simulation of Fine-Needle Aspiration
The diagnostic performance of simulations 1, 2, and 3 is represented in Figure 3. For the total study population, the sensitivity of simulation 3 (90.3%) was higher than that of simulation 1 (66.1%, p < 0.001) and simulation 2 (77.4%, p = 0.015), and the specificity of simulation 3 (38.0%) showed equivalent results to those of simulation 1 (47.9%, p = 0.003) and simulation 2 (42.3%, p < 0.001). In addition, for the group with risk factors, simulation 3 showed higher sensitivity (88.9%) than simulation 1 (55.6%, p < 0.001) and simulation 2 (69.4%, p = 0.022), and the specificity of simulation 3 (54.8%) was equivalent to that of simulation 1 (64.5%, p = 0.027) and simulation 2 (61.3%, p = 0.001). For the group without risk factors, simulation 3 showed equivalent sensitivity (88.5%) to simulation 1 (80.8%, p = 0.012) and simulation 2 (88.5%, p < 0.001). In addition, the specificity of simulation 3 (35.0%) was equivalent to that of simulation 2 (27.5%, p = 0.002) and was the same as that of simulation 1 (35.0%). In terms of accuracy, simulation 3 had the highest accuracy (simulation 1 vs. 2 vs. 3; 56.4% vs. 58.6% vs. 62.4% in the total; 59.7% vs. 65.7% vs. 73.1% in the group with risk factors; and 53.0% vs. 51.5% vs. 56.1% in the group without risk factors). In addition, simulation 3 had the lowest unnecessary biopsy rates (simulation 1 vs. 2 vs. 3; 47.4% vs. 46.1% vs. 44.0% in the total; 35.5% vs. 32.4% vs. 30.4% in the group with risk factors; 55.3% vs. 55.8% vs. 53.1% in the group without risk factors). The 2 × 2 tables for each simulation are shown in Supplementary Figure S1.

Comparison of diagnostic performance for malignant thyroid nodules according to three simulations. This graph shows a comparison of diagnostic performance, including sensitivity (
Discussion
Although previous studies have suggested that adult thyroid US guidelines can be extended to pediatric patients (2,9), it is worth taking some factors into consideration. For adults, guidelines for thyroid nodule management are changing in a trend toward taking a conservative approach to minimizing the potential harm from overtreatment. However, thyroid nodules in pediatric patients are more likely to be malignant than those in adult patients (2,3). Moreover, pediatric thyroid cancer is likely to show aggressive features, including early lymph node and distant metastases (2,5). Nevertheless, the prognosis for pediatric thyroid cancer is good, but should be diagnosed early with appropriate treatment (19). In particular, it is important to make appropriate criteria of FNA for children who undergo screening US due to clinical risk factors. Therefore, for children with risk factors, general guideline of thyroid nodule for FNA may need to be modified.
Modifying the guidelines has resulted in improving diagnostic performance without increasing unnecessary biopsy rate in our study. In our study, the malignancy rate of thyroid nodules was high (46.6%) compared with previous reports (19.1–27.0%) (3,10,12). A previous study on pediatric thyroid nodules of more than 1 cm showed a similar malignancy rate (42.0%) (9). Although the overall malignancy rate is high, in our study, the malignancy rate for K-TIRADS 2 (0%) and 3 (10.6%) nodules was similar to that of the KSThR guideline (<3% and 3–15% for K-TIRADS 2 and 3, respectively), but in the case of K-TIRADS 4 in the total study population (60.0%) and the group with risk factors (64.3%), the malignancy rate was higher than the adult guideline estimates (15–50%). This result is consistent with previous studies showing higher malignancy rates in children than in adults in intermediate or highly suspicious nodules using the American Thyroid Association (ATA) guideline and The American College of Radiology (ACR)-TIRADS (9,12).
In addition, in the same study, ACR-TIRADS guidelines showed a high missed malignancy rate (22.1%) in pediatric thyroid nodules (12). In our study, the missed malignancy rate was even higher than that reported in a previous study in the total study population (33.9%) and the group with risk factors (44.4%). Therefore, adult guidelines may be inappropriate for the management of thyroid nodules in children, especially for patients with risk factors.
None of the guidelines considers risk factors for thyroid cancer. The KSThR guideline also does not provide specific FNA indications for patients with risk factors for thyroid cancer and suggests that lower cutoff values can be considered for FNA of nodules with intermediate or low suspicion patterns in patients with clinical risk factors (16). In our study, patients with clinical risk factors showed higher malignancy rates than those without (64.0% vs. 43.9%, p = 0.037). In addition, when FNA was performed according to the KSThR guidelines, the results suggest that it is more likely to miss thyroid cancer in children with clinical risk factors than in children without risk factors (69.2% vs. 16.7% in K-TIRADS 4; 35.3% vs. 18.8% in K-TIRADS 5). Considering this result, the guideline for the management of thyroid nodules in children and adolescents needs to adjust the criteria for performing FNA in patients with clinical risk factors.
As previous studies have shown, the KSThR guideline has high sensitivity and low specificity for the detection of thyroid cancer, compared with other guidelines, including European and ACR guidelines (20 –22). In a study of adult thyroid nodules, the KSThR guideline showed sensitivity between 93.5% and 95.7% and specificity between 23.6% and 28.7% for detecting thyroid cancer (20 –22). When the size cutoff value from the KSThR guideline was applied to children regardless of risk factors, it showed lower sensitivity (66.1%) and higher specificity (47.9%) than the results in adults. In particular, the group with risk factors showed lower sensitivity (55.6%) than the group without risk factors (80.8%) with the KSThR guideline. In pediatric patients without clinical risk factors, the diagnostic performance of the KSThR guideline was similar to that of the new criteria. In comparison with the KSThR guideline, new size criteria had significantly higher sensitivity, comparable to the results of adults, with insignificant decrease of specificity in the total study population and the group with risk factors. In addition, the newly proposed size criteria achieved the highest accuracy, even though it had the lowest unnecessary biopsy rate. Therefore, in the future, the guidelines for the management of pediatric thyroid nodules should consider clinical risk factors.
This study had several limitations. First, in addition to the risk factors identified in this study, there are well-known risk factors such as iodine intake, but due to the inherent limitation of the retrospective study, it was difficult to assess other confounding risk factors. Second, only pathologically confirmed thyroid nodules were studied. The fact that only nodules that had undergone FNA or CNB were included may have caused the overall high malignancy rate in the study. Further prospective studies, including benign nodules identified on US follow-up, might be helpful to evaluate the diagnostic performance of the new criteria for the management of pediatric thyroid nodules. Furthermore, the study population was small, and the simulation could not be performed by dividing the cohort into a training set and validation set. The diagnostic performance was obtained from the identical group that created the cutoff size, which might serve as a bias that increased the diagnostic performance. Furthermore, as our study was conducted in a single tertiary center, the study cohort includes large number of patients with risk factors, such as RT history, and referred cases with thyroid nodules of high K-TIRADS categories from other hospitals. That may have resulted in the overall high malignancy rate and a high missed malignancy rate when applying the KSThR guideline. Thus, the diagnostic performance of the KSThR guideline for this study cohort may not be generalized to pediatric patients. A multicenter study is essential for developing guidelines for the management of general pediatric patients with thyroid nodules.
Considering that pediatric thyroid cancer are aggressive and have a high recurrence rate, the management guidelines for pediatric thyroid nodules may need to be different from adult guidelines. In addition, specific guidelines may be required for patients with risk factors for thyroid cancer. This study revealed that, for pediatric patients, FNA needs to be carried out more actively on smaller thyroid nodules than for adults. In particular, FNA in pediatric patients with clinical risk factors should be strongly considered in the management of thyroid cancer.
Footnotes
Authors' Contributions
S.B.L. carried out the initial analyses, drafted the initial article, and reviewed and revised the article. S.L. collected data, and reviewed and revised the article. Y.H.C. reviewed and revised the article. J.-E.C. and W.S.K. coordinated and supervised data collection and critically reviewed and revised the article for important intellectual content. Y.J.C. conceptualized and designed the study, and reviewed and revised the article. All authors approved the final article as submitted and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Author Disclosure Statement
All authors have no potential conflicts of interest to declare.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5