
Abstract
Background:
Brain metastases (BM) from differentiated thyroid cancer are rare. Stereotactic radiosurgery (SRS) is commonly used for the treatment of BMs; however, the experience with SRS for thyroid cancer BMs remains limited. The goal of this international, multi-centered study was to evaluate the efficacy and safety of SRS for thyroid cancer BMs.
Methods:
From 10 institutions participating in the International Radiosurgery Research Foundation, we pooled patients with established papillary or follicular thyroid cancer diagnosis who underwent SRS for histologically confirmed or radiologically suspected BMs. We investigated patient overall survival (OS), local tumor control, and adverse radiation events (AREs).
Results:
We studied 42 (52% men) patients who underwent SRS for 122 papillary (83%) or follicular (17%) thyroid cancer BMs. The mean age at SRS was 59.86 ± 12.69 years. The mean latency from thyroid cancer diagnosis to SRS for BMs was 89.05 ± 105.49 months. The median number of BMs per patient was 2 (range: 1–10 BMs). The median SRS treatment volume was 0.79 cm3 (range: 0.003–38.18 cm3), and the median SRS prescription dose was 20 Gy (range: 8–24 Gy). The median survival after SRS for BMs was 14 months (range: 3–58 months). The OS was significantly shorter in patients harboring ≥2 BMs, when compared with patients with one BM (Log-rank = 5.452, p = 0.02). Two or more BMs (odds ratio [OR] = 3.688; confidence interval [CI]: 1.143–11.904; p = 0.03) and lower Karnofsky performance score at the time of SRS (OR = 0.807; CI: 0.689–0.945; p = 0.008) were associated with shorter OS. During post-SRS imaging follow-up of 25.21 ± 30.49 months, local failure (progression and/or radiation necrosis) of BMs treated with SRS was documented in five (4%) BMs at 7.2 ± 7.3 months after the SRS. At the last imaging follow-up, the majority of patients with available imaging data had stable intracranial disease (33%) or achieved complete (26%) or partial (24%) response. There were no clinical AREs. Post-SRS peritumoral T2/fluid attenuated inversion recovery signal hyperintensity was noted in 7% BMs.
Conclusion:
The SRS allows durable local control of papillary and follicular thyroid cancer BMs in the vast majority of patients. Higher number of BMs and worse functional status at the time of SRS are associated with shorter OS in patients with thyroid cancer BMs. The SRS is safe and is associated with a low risk of AREs.
Introduction
Thyroid cancer is the most common endocrine malignancy that accounts for ∼3% of new cancer cases in the United States (1). The incidence of thyroid cancer is rising worldwide, in part, because of increased cancer incidence and early detection (2 –5). Papillary and follicular cancers are epithelial-derived differentiated types of thyroid cancer that account for the vast majority (>95%) of all thyroid cancers (6). Other thyroid cancer types, such as anaplastic (undifferentiated) thyroid cancer and medullary thyroid cancer, are far less common. Brain metastases (BM) of thyroid cancer are extremely rare and can occur in less than 2% of all differentiated thyroid cancer cases (7 –10). However, the discovery rate of asymptomatic thyroid cancer BMs is expected to increase due to increasing utilization of surveillance brain imaging and improving survival of patients with thyroid cancer (11 –13).
Differentiated thyroid cancer is associated with a favorable prognosis, with overall 5-year survival exceeding 90% for localized disease (14,15). The prognosis of advanced-stage thyroid cancers and anaplastic thyroid cancer is worse (14). The presence of BMs from thyroid cancer is associated with grim prognosis and short survival (8,12,16,17). Surgical resection and/or radiation therapy are recommend for the management of differentiated thyroid cancer BMs (12,18). However, the published experience with radiation therapy for the management of thyroid cancer BMs is limited to single-institution series with small sample sizes (8,16,17). There are also some concerns regarding resistance of thyroid cancer cells to radiation therapy, which can have implications for radiation treatment planning and local disease control (19 –21).
Stereotactic radiosurgery (SRS) allows spatially precise high-dose irradiation of intracranial tumors in a single fraction. The SRS is considered a standard of care of BMs of various primary cancer sites either in upfront settings or in combination with surgical resection and/or whole brain radiation therapy (WBRT) that is low-dose multi-fractionated irradiation of the whole brain (22 –25). For more common cancer histologies such as lung and breast, SRS typically achieves a high rate of local disease control of BMs that typically exceeds 70–90% (depending on tumor histology, volume of BM, and duration of follow-up), and it can be repeated in case of local or distant failure (26 –28). The SRS is associated with better cognitive function preservation rates when compared with other radiation therapy techniques, such as WBRT, that use larger radiation fields (27). Preservation of cognitive function can be of particular importance for cancers carrying favorable prognosis, such as a thyroid cancer. Published experience with SRS for thyroid cancer BMs remains limited to single-institution series with small sample sizes (8,10,29,30). Larger studies exploring the efficacy and safety of SRS for the management of differentiated thyroid cancer BMs are warranted. The goal of this international, multi-centered study was to evaluate the efficacy and safety of SRS for differentiated thyroid cancer BMs.
Methods
Patients
Patients were identified from 10 centers in five countries (USA, Canada, Czech Republic, Taiwan, and Spain) affiliated with the International Radiosurgery Research Foundation (protocol R-16-10). Data collection was approved by institutional review boards at each of the participating centers. The database with variables of interest was established by the coordinating investigators at the University of Virginia and sent to all participating centers. Individual patient-level data were de-identified and pooled for the analyses. We included only patients who had an established histological diagnosis of papillary or follicular thyroid cancer and the absence of any other active cancer who were treated with single-fraction SRS for histologically confirmed and/or magnetic resonance imaging (MRI) defined BMs and had at least one clinical or imaging follow-up visit after the index SRS procedure. Patients diagnosed with other non-thyroid cancer were allowed to enter the study only if other cancers were deemed as well controlled, and/or diagnosis of thyroid cancer BMs was established based on histological examination. Patients were treated with the SRS from May 2006 until March 2020. Patients who underwent fractionated (i.e., multi-sessions SRS) and those with other types of thyroid cancer (anaplastic or medullary) were excluded.
Clinical assessment
We collected data about patient sex, age (at diagnosis of thyroid cancer and SRS for BMs), presenting symptoms of BMs, presence of noncentral nervous system (CNS) thyroid cancer metastases, previous therapies for thyroid cancer and BMs, functional status (Karnofsky Performance Status [KPS] score), and number, location, and volume of BMs. We also used the American Thyroid Association (ATA) risk stratification system to stratify patients for risk of recurrence (12). Information regarding thyroid cancer type, presence of BRAFV600E and TERT promoter mutations, and nuclear atypia was also recorded.
SRS technique
The SRS was performed by using standard techniques using Gamma Knife units (Elekta AB, Stockholm, Sweden) with a frame-based approach. The frameless approach was used for hypo-fractionated SRS or when stereotactic frame application was not technically possible. The SRS treatment was typically planned by using thin-sliced contrast-enhanced T1-weighted brain MRIs for stereotactic planning. Treatment plans were made at the discretion of the treating team at each of the participating centers, and they were tailored for individual patient needs.
Clinical and radiographic follow-up
Imaging and clinical follow-up after the SRS was typically performed every 3 months at the discretion of the treating team. We recorded the tumor response by using BMs response assessment in neuro-oncology (RANO) criteria (31), local failure, distant failure, leptomeningeal progression, and new of worsening T2/fluid attenuated inversion recovery (FLAIR) signal change surrounding BMs treated with SRS. Newly diagnosed or recurrent BMs were treated at the discretion of the primary team. The SRS-related adverse events were categorized according to the Radiation Therapy Oncology Group CNS toxicity criteria (32). The use of other treatments after an index SRS was captured. Tumor response at the last imaging follow-up was evaluated according to RANO criteria (31). Date and cause of death was also documented.
Statistical analysis
Overall survival (OS) was defined as interval (in months) from SRS to time or death or the last clinical follow-up, whichever occurred first. The CNS progression-free survival (PFS) was defined as interval from SRS to MRI-documented progression of SRS-treated lesion or the last MRI follow-up, whichever occurred first. Patients who did not achieve an endpoint for OS or CNS-PFS were censored at the last follow-up. The association of clinical indexes and SRS treatment characteristics with OS and CNS-PFS was evaluated by using the Kaplan–Meier method (Log-rank test) and Cox regression analyses. Results of Cox-regression analysis are presented as hazard ratio, confidence interval [CI], and p-value.
All hypothesis tests were two-sided, and a p < 0.05 was considered statistically significant. Statistical analyses were performed with the IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA).
Results
Baseline characteristics
Forty-two patients (52% male) underwent SRS for 122 thyroid cancer BMs (Table 1). The mean age at SRS for thyroid cancer BMs was 59.86 ± 12.69 years. Two patients (5%) had BMs at presentation, and nine (21%) patients were diagnosed with BMs within 6 months of thyroid cancer diagnosis. The mean latency period between diagnosis of thyroid cancer to SRS for BMs was 89.05 ± 105.49 months (median: 59 months; range from 0 to 588 months). Fourteen percent of patients were also diagnosed with non-thyroidal cancer. There were 83% of patients with papillary and 17% of patients with follicular thyroid cancer BMs. The majority of patients were previously treated with radioactive iodine therapy and thyroid hormone for thyrotropin suppression. Ten (24%) patients had a prior resection of thyroid cancer BMs. Functional status at the time of SRS was good in the majority of patients with a median KPS of 90 (range from 80 to 100).
Baseline and Demographic Characteristics of the Study Patients
Some patients had >1 presenting symptom, therefore the total number does add up to 42.
The majority of patients had >1 therapy.
BM, brain metastases; CNS, central nervous system; SRS, stereotactic radiosurgery; TSH, thyrotropin.
The median number of BMs per patient was 2 (range from 1 to 10 BMs). The most common locations of BMs were frontal (40%), parietal (16%), and temporal (15%) lobes. The BMs were asymptomatic and discovered incidentally in the majority of patients, 36% of patients, and the most common presenting symptom was headaches (26% of patients). The majority of patients (83%) also had other non-CNS metastases of their thyroid cancer. According to the ATA risk stratification system at presentation, the majority of thyroid cancers were classified as high-risk (79%).
Radiosurgery
The mean total intracranial BM treatment volume at each SRS session was 3.62 ± 5.99 cm3 (median: 0.79 cm3; range from 0.003 to 38.18 cm3). The mean margin dose was 18.30 ± 3.55 Gy, and the mean maximal dose was 29.83 ± 7.58 Gy (Table 2).
Stereotactic Radiosurgery Treatment Characteristics (n = 122)
Gy, gray.
Clinical outcomes
The mean clinical follow-up duration after the initial SRS was 27.77 ± 28.04 months (median: 15.7 months; range from 1 to 125 months) (Table 3). Sixteen (38%) patients died during the observation period (Fig. 1A). Causes of death were available for 8 patients and included infection (n = 3), systemic (n = 2) and CNS (n = 1) cancer progression, congestive heart failure (n = 1), and sudden death (n = 1). The mean time from SRS for BMs to death was 18.03 ± 16.18 months (median: 14 months; range from 3 to 58 months). Additional BM care after SRS included surgical resection (12%) and repeated SRS (17%) for progression of intracranial disease. Nineteen (45%) patients received chemotherapy/immunotherapy. As expected, there was a significant decrease of KPS scores at the last follow-up visit when compared with pre-SRS score (p = 0.03).
Treatment Outcomes
Five patients received combination therapy.
Alectinib, cobimetinib, etoposide phosphate, carboplatine, cyclophosphamide, melphalan, doxorubicin, and denosumab were administered once for each patient.
Tumor progression (n = 2) and tumor progression versus radiation necrosis (n = 3).
FLAIR, fluid attenuated inversion recovery; KPS, Karnofsky Performance Status; RANO, response assessment in neuro-oncology
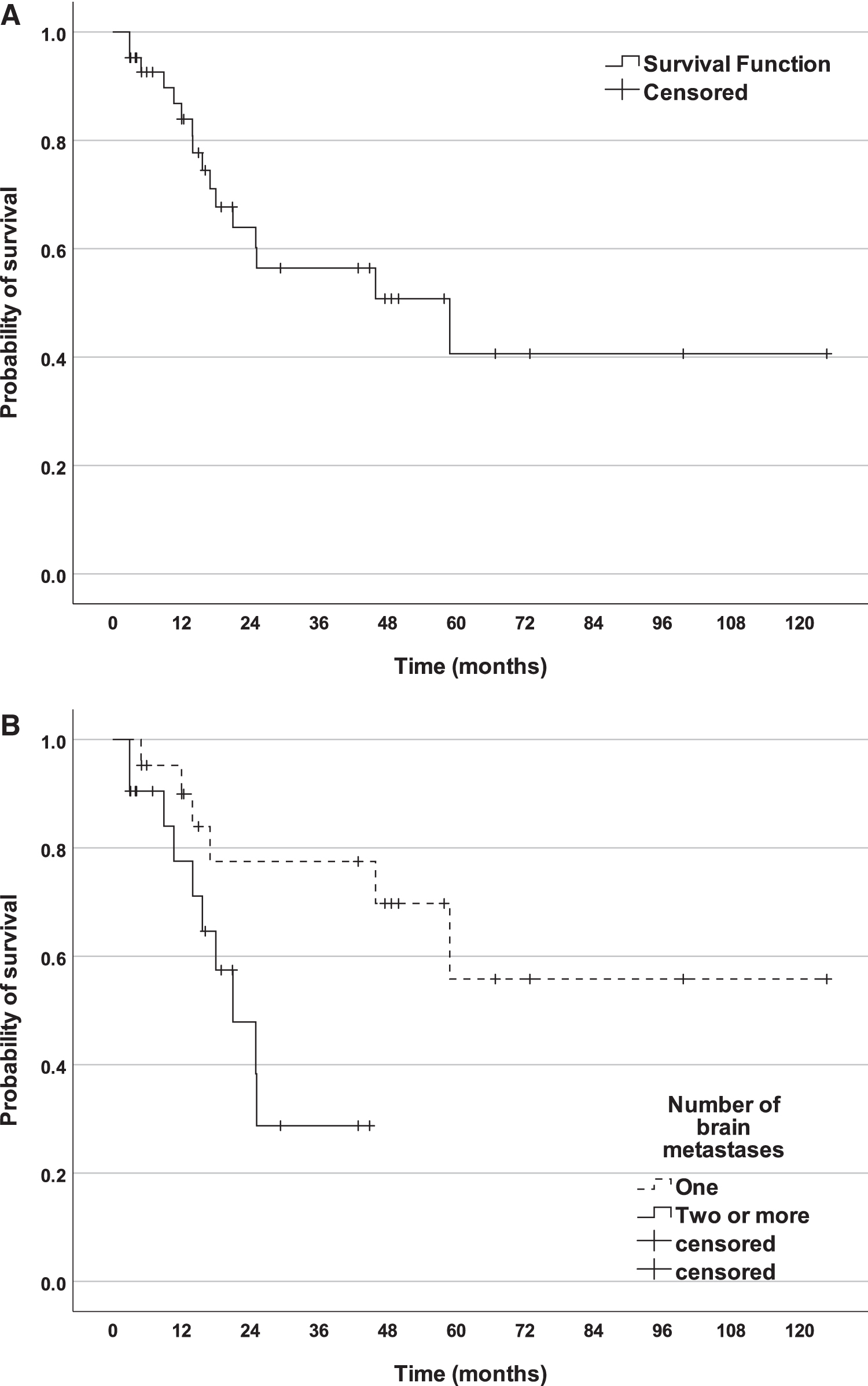
In Kaplan–Meier analyses, OS was significantly shorter in patients with two or more BMs, when compared with patients with one BM at the time of index SRS procedure (Log-rank = 5.452, p = 0.02; Fig. 1B). In univariate Cox-regression analyses, two or more BMs (odds ratio [OR] = 3.688 [CI: 1.143–11.904], p = 0.03) and lower KPS score at SRS (OR = 0.807 [CI: 0.689–0.945], p = 0.008) were associated with shorter OS after SRS for BMs. The OS was not associated with age at diagnosis (p = 0.913), latency period of BMs after thyroid cancer diagnosis (p = 0.2), presence of three of more BMs (p = 0.530), BM volume of 3 or more cm3 (p = 0.455), prior resection of BMs (p = 0.818), presence of distant non-CNS metastases (p = 0.122), ATA risk score (p = 0.634), TERT (p = 0.419), and BRAF (p = 0.835) mutation status.
Progression-free survival
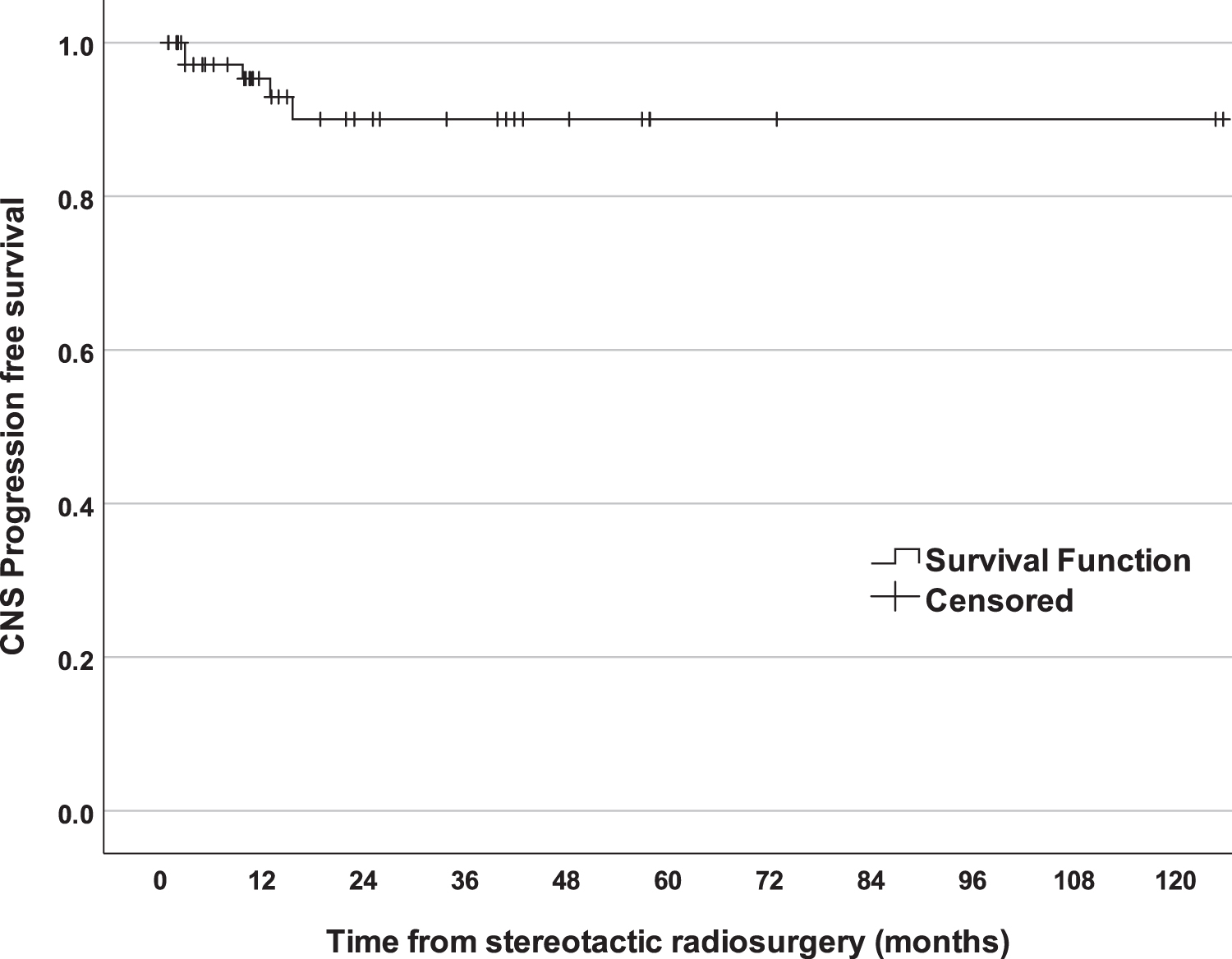
The mean duration of imaging surveillance after SRS was 25.21 ± 30.49 months (median: 11; range: 1–26 months) (Table 3). During this time, local failure was documented in five (4%) BMs treated with SRS (Fig. 2). Local failures included local progression of two BMs and tumor progression versus radiation effects in three BMs. The mean time from SRS to local failure was 7.19 ± 7.34 months (median: 3 months; range from 2 to 16 months). Local failures were observed only in male patients but not in female patients (15% vs. 0%). There were no significant differences between BMs that experienced local failure and those that did not in initial BM volume (3.90 ± 3.12 cm3 vs. 4.82 ± 14.31 cm3, respectively, p = 0.87), margin radiation dose (18.60 ± 0.89 Gy vs. 18.12 ± 3.74 Gy, respectively, p = 0.78), and maximal radiation dose (30.14 ± 1.34 vs. 29.63 ± 7.55, respectively, p = 0.88). According to the RANO criteria, at the last imaging follow-up (data available for 36 patients), the majority of patients were classified as having stable intracranial disease (33%), complete (26%) or partial response (24%), and progressive disease was noted in one (2%) patient.
Safety
There were no adverse radiation events (AREs) in patients included in this study. New or worsening peritumoral T2/FLAIR signal change was noted in 8 patients (7%). The BMs were treated with the SRS at a median interval of 3 months (range: 2–64 months) after the SRS.
Discussion
The SRS was associated with durable local control of papillary and follicular thyroid cancer BMs in the majority of patients. Greater number of BMs and worse functional status at time of SRS were associated with shorter OS after SRS for BMs. The SRS was well tolerated and was associated with a low risk of adverse imaging radiation events.
To the best of our knowledge, this is the largest series to date exploring the efficacy and safety of SRS for differentiated thyroid cancer BMs. Thirty-eight percent of patients died during a mean post-SRS clinical follow-up of 27.77 ± 28.04 months (range: 1–125 months). The median time from SRS to mortality was 18 months. Differentiated thyroid cancer is typically associated with favorable prognosis; however, the presence of BMs carries a grim prognosis and predicts shorter survival time in patients with thyroid cancer (8,12,16,17). Adequate local control of thyroid cancer BMs with either surgical resection or radiation therapy can be associated with improved overall prognosis of patients with thyroid cancer (10,16,31,32). A study of 24 patients with thyroid cancer presenting with BMs found that median survival was longer for patients who received SRS (n = 8) than for those who did not receive SRS (52.5 months vs. 6.7 months) (10). Another study in 23 patients with thyroid cancer BMs also found that median survival was longer in patients who had SRS (n = 15) versus those who did not (37.4 months vs. 12.3 months, respectively). However, this difference did not reach statistical significance (p = 0.28) in this likely under-powered study (33). Intracranial disease control of thyroid cancer BMs via either surgical resection or radiation therapy is important for optimized OS. Surgical resection remains a primary treatment option for good surgical candidates harboring large and surgically accessible BMs, causing brain compression. The SRS should be considered for patients who are not good surgical candidates due to severe comorbidities, present with advanced intracranial disease, or are unwilling to undergo surgery. The SRS has the benefits of being minimally invasive and allowing for easy integration into other adjuvant therapies secondary to the short recovery time.
We found that a greater number of BM and worse functional status at the time of SRS were associated with shorter OS after SRS for differentiated thyroid cancer BMs. These results are congruent with prior studies showing that a greater number of thyroid cancer BMs (34,35) and worse functional status (8,33,34,) are important predictors of shorter survival of patients with thyroid cancer presenting with BMs. Other previously identified unfavorable prognostic factors of patients with thyroid cancer BM include longer latency from thyroid cancer diagnosis to BM (35) and greater patient age (34). Surgical resection of BMs is often identified as a favorable prognostic factor of thyroid cancer BMs (10,16,29,34,35). The lack of the association between histories of resection of BMs and OS in the present study can be explained by patient selection procedures, because we considered only those patients who underwent SRS for BMs and did not include a comparison group of patients treated only with surgical resection. Local recurrence rates of surgically resected BM remain high (36,37), and adjuvant SRS or WBRT can significantly improve local control rates of surgically resected BM (37,38).
During mean imaging follow-up of 25.21 ± 30.49 months (range: 1–126 months), local control of BMs was achieved in the majority of patients. Local failure was documented (or suspected) in only 4% of all BMs treated with SRS, and intracranial disease was deemed as progressive in one patient at the last imaging follow-up visit. High-local control rate (96%) of differentiated thyroid cancer BMs treated with SRS was previously reported in a study that included 9 patients with thyroid cancer treated with Gamma Knife radiosurgery (GKRS) for 26 BMs (30). Local disease control rates were not reported by other groups that used SRS for thyroid cancer BMs (10,35).
In our experience, the majority of patients were treated by using single-session SRS delivering a median radiation dose of 20 Gy (range: 8–24 Gy). There is some concern regarding the radioresistance of thyroid cancer (20,39). Heterogeneity in the radioresistance of anaplastic thyroid cancer cells was previously documented in cell cultures and animal models. Radioresistance was associated with higher levels of CXCR4 compared with radiosensitive cell lines, and hypo-fractionated therapy was associated with superior tumor control and animal survival (21). Radiosurgery with its high dose per fraction approach tends to overcome inherent radioresistance of most cancer histologies (40). Thus, SRS may offer a benefit to BMs from thyroid cancer, particularly if the cancer in the brain proves to be more radioresistant to conventional dose and fractionation schemes of standard whole-brain radiotherapy. Careful planning and an adequate radiation dose are required to achieve local control of thyroid cancer BMs.
In our experience, SRS was associated with low toxicity. Asymptomatic peri-tumoral inflammation/edema was identified in 7% of all BMs and post-SRS radiation necrosis was suspected in three BMs. Others also reported a low risk of transient AREs after SRS for thyroid cancer BMs (30). Transient peritumoral T2/FLAIR signal changes in surroundings occur in a minority of patients after SRS for BM, are often self-limiting, or can be managed with a short course of steroids (41). Radiation necrosis and other AREs can occur in ∼10% of BMs treated with SRS (42 –44) with larger tumor volume, prior WBRT and immunotherapy, predisposing to a higher risk (45).
Our study has limitations that should be acknowledged. Histological confirmation of thyroid cancer BMs was available in 24% of patients, hence there remains a distant possibility that patients had other comorbid malignancies with greater predisposition for CNS metastases. All study patients were treated by using GKRS systems, delivering radiation dose in a single fraction; thus, our results should be interpreted with caution when considering other radiotherapy modalities and techniques. The possible impact of the advancements of systemic thyroid cancer therapies as well as technological improvements in GKRS device and planning software and learning curve is limited, because all patients were managed at high-volume SRS centers and according to the prevailing guidelines (46). On the other hand, the large sample size of this rare disease together with long imaging and clinical follow-up are important strengths of our study fortifying the reliability of our results.
The SRS affords a high local control rate of papillary and follicular thyroid cancer BMs in the vast majority of patients. The mortality of patients with thyroid cancer presenting with BMs remains high, with a greater number of BMs and worse functional status being associated with the shorter survival of patients with thyroid cancer treated with SRS for BMs. The SRS for thyroid cancer BMs is safe and associated with a low risk of toxicity. The SRS should be considered for the management of differentiated thyroid cancer BMs. All patients with differentiated thyroid cancer BMs, and a limited number of metastases and good performance status should be assessed by or discussed with a multidisciplinary group.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.