
Abstract
Background:
Papillary thyroid carcinoma (PTC) is a rare malignancy in children and young adults (CAYA). It often presents with aggressive disease patterns and advanced stages, which are clinically distinct from those in adult patients. In this study, we sought to characterize and better understand the clinical variants of PTC in CAYA and explore the underlying mechanisms.
Methods:
CAYA patients (age ≤18 years) diagnosed with PTC between June 2006 and June 2018 were retrospectively recruited from five hospitals. Demographic information, pathological data, and follow-up status were recorded. Tumor samples obtained from 20 children (mean age 15.15 years) and 10 adults (mean age 38.80 years) underwent comprehensive whole transcriptome sequencing. Differentially expressed genes (DEGs), mutational landscape, and immune infiltration were analyzed.
Results:
A total of 217 CAYA-PTC patients (162 females and 55 males) with an average age of 14.38 ± 3.53 years (range 2–18) were included. Lymph node metastasis (LNM) was observed in 85.71%, of which 57.60% were in the lateral cervical compartment. Disease recurred in 28 of 217 (12.90%) patients with a median follow-up of 4.76 years. Multivariate logistic regression analysis revealed that age, bilateral disease, extrathyroidal extension, and coexisting Hashimoto's thyroiditis (co-HT) were independent risk factors for LNM, while co-HT was the only risk factor for recurrence. Using whole transcriptome sequencing of PTC tissues, we identified 301 DEGs. Gene Ontology and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analyses showed that differences in immune mediators played important roles, based on the distributions of mutation frequencies, types, and expression levels between CAYA and adult patients. Based on the integrated data sets, we identified significantly mutated immune genes, cluster of differentiation 24 (CD24), coagulation factor 12 (F12), coagulation factor 5 (F5), integrin subunit alpha 3 (ITGA3), and retinoic acid early transcript 1L (RAET1L), which were then verified by immunohistochemistry. Furthermore, resting mast cells, resting natural killer cells, plasma cells, and regulatory T cells were different in the CAYA-PTC group and correlated with the expression of immune checkpoints.
Conclusions:
There are considerable variabilities that may contribute to the different clinical presentations between CAYA and adult PTC patients, among which the decrease in protective immune cells may be a factor. Collectively, our results add to the possible biological mechanisms involved in CAYA-PTC.
Introduction
Thyroid carcinoma (TC) represents only 0.5–3% of all pediatric malignancies, which is lower as compared with that in adults (1,2), but it still ranks as the third most common solid malignancy and is the most common type of endocrine cancer in children and young adults (CAYA, papillary thyroid cancer [PTC]) (3). For the past two decades, its incidence has increased significantly in both adults (Adult-PTC) and CAYA (CAYA-PTC), and the majority are treated by thyroid surgery (4 –6). In addition, the clinical presentation and tumor behavior differ dramatically in children; for instance, larger tumor size, involvement of the capsule, and more extensive lymph node metastasis (LNM) (7 –9).
The American Thyroid Association (ATA) defined the age limit for CAYA-PTC as ≤18 years (10,11). Thyroid nodules are less common in children than in adults, but are more likely to be malignant in children referred for evaluation of nodular thyroid disease (22–26% vs. ∼5%) (12). Recent data from an Italian multicenter case series of 125 pediatric patients with benign and malignant thyroid nodules indicated thyrotropin (TSH) >2.8 mU/L can serve as a predictor of thyroid cancer in CAYA patients with thyroid nodules (13).
In CAYA-PTC, up to 90% of cases present with palpable lymph nodes in the neck at the time of diagnosis (14), and regional LNM is frequently observed. Furthermore, a high rate of recurrence in cervical lymph nodes has also been reported, resulting in low recurrence-free survival; the 20- and 30-year disease-free survival (DFS) rates are 70.7% and 64.0%, respectively. However, CAYA-PTC has an overall good prognosis, and the 30-year disease-specific survival rate is >95% (15 –17). The contradiction in advanced disease stages with better long-term prognosis makes it difficult for clinicians and researchers to reach an agreement on an optimal treatment pattern (4,6).
In this study, we tried to identify the risk factors for LNM and recurrence in CAYA-PTC, which might support the choice and design of appropriate intervention plans. In particular, we attempted to identify the core genes and immune infiltration that drive the unique clinical presentations in young patients and provide more insights into a better understanding of CAYA-PTC.
Materials and Methods
Study population
We retrospectively reviewed 217 CAYA-PTC patients (≤18 years of age) with a well-documented histological diagnosis of PTC from five tertiary medical institutions in Renji Hospital, Fudan University Shanghai Cancer Center, Children's Hospital of Fudan University, Shanghai Children's Medical Center, and Children's Hospital of Shanghai Jiao Tong University between June 2006 and June 2018. Patients' characteristics are shown in Table 1. The data were retrospectively collected, including demographic information, thyroperoxidase antibody (TPOAb), thyroglobulin antibody [TGAb], and thyroglobulin [Tg], imaging procedures (cervical ultrasound [US], chest radiograph, computed tomography [CT] scan), surgical methods, and pathology reports.
Baseline Characteristics of Study Cohort
Variants of papillary thyroid carcinoma according to WHO New Classification 2017.
T classification from AJCC eighth edition was used.
AJCC, American Joint Committee on Cancer; co-HT, coexisting Hashimoto's thyroiditis; ETE, extrathyroidal extension; LNM, lymph node metastasis; N, no; SD, standard deviation; TT, total thyroidectomy; WHO, World Health Organization; Y, yes.
Surgical approach and pathology
Total thyroidectomy (TT) was performed in patients with suspected bilateral or large isthmus TC. US-guided fine needle aspiration was performed routinely, and cytological findings were classified according to the Bethesda system (18). The presence of distant metastasis (DM) was detected by chest X-ray or CT.
Primary tumor characteristics were recorded, including histological subtype, extrathyroidal extension (ETE), defined as neoplastic infiltration beyond the thyroid capsule, infiltration of the thyroid fibrous capsule, defined as complete capsular transgression by the tumor (19), multifocality (either unilateral or bilateral involving both lobes or one lobe plus isthmus), vascular invasion, and LNM. The diameter of the largest tumor was taken as the tumor size (20). Patients with a hypoechogenic gland pattern in US compatible with autoimmune thyroid diseases and positive TPOAb and/or TGAb were considered to have coexisting Hashimoto's thyroiditis (co-HT) (21).
Postoperative follow-up and recurrence
The management of PTC patients consisted of TT and evaluation for radioactive iodine (RAI) treatment. Criteria for RAI were tumor size >1 cm, LNM, ETE, macroscopic postoperative residual lesions in the neck, and/or DM (22). After primary treatment, all patients received TSH suppression therapy with thyroid hormone. Follow-up were conducted every three months in the first year after the operation, every six months during the next two years, and then yearly. US and thyroid function tests were routinely performed during each follow-up, and a chest X-ray or CT examination was performed once a year.
Tissue specimens
Twenty CAYA and 10 Adult-PTC surgical tissues were obtained with signed informed consent. The characteristics of the 30 patients are summarized in Supplementary Table S1. The comparison of baseline characteristics between 20 CAYA-PTC samples that were subjected to RNA-sequencing and other 197 CAYA-PTC samples are listed in Supplementary Table S2. Most of the baseline characteristics had a p-value >0.05, while multifocal lesions and lateral neck metastasis were more commonly seen in the RNA-seq group.
After complete resection of the affected thyroid gland, the tumor (colored white or gray) was distinguished from normal tissues and dissected in the middle with a scalpel by an experienced surgeon. Samples were obtained from the tumor and collected in sterile freezing tubes. These processes were repeated with each acquired tissue to maintain homogeneity between sample qualities. The primary tumors were immediately frozen at −80°C. The diagnosis was confirmed by pathological examination. Protocols for investigations involving human tissues used in this project were approved by the Ethics Committee of Renji Hospital. The cellularity of the tumor sections was determined microscopically by a pathologist. Sections from 30 patients with cellularity >80% and no necrosis or calcification were selected for RNA sequencing.
RNA sequencing
Total RNA was isolated from frozen tissue blocks containing ∼50–100 mg of tissue using TRIzol Reagent (Life Technologies, Carlsbad, CA) following the manufacturer's instructions. The quality, quantity, and integrity of the total RNA were evaluated using a SmartSpec Plus spectrophotometer (Bio-Rad, Hercules, CA). Whole transcriptome libraries were prepared, and deep sequencing was performed by Sangon Biotech Co., Ltd. (Shanghai, China).
Sequencing libraries were generated on an Illumina HiSeq 2000 platform (San Diego, CA). The quality of the sequencing data was analyzed using FastQC (0.11.2). The reads were aligned to the human genome (hg38) using HISAT2 (2.1.0) and RSeQC (2.6.1). Poorly expressed genes were eliminated based on the criteria of a maximum read count of <20 for all samples. BCFtools (1.5) was used for gene mutation (GM) analyses of each sample.
Then, SnpEff (2.36) was used to calculate the distribution of variation sites in the genome structure, which were filtered according to the following conditions: (i) mass value >20; (ii) coverage >8. The landscape of the mutation was illustrated by ComplexHeatmap (2.4.3). The fusion transcript signatures were identified by EricScript, which is a computational framework that uses a combination of four alignments. It comprises the following steps: (i) mapping of the reads against the transcriptome; (ii) identification of discordant alignments and building of the exon junction reference; (iii) recalibration of the exon junction reference; and (iv) scoring and filtering the candidate gene fusions. Gene expression levels in each sample were quantified and normalized using the Transcripts Per Million (TPM) algorithm.
The differential expression between conditions was statistically assessed using the R/Bioconductor package edgeR (3.14.0). A paired design model was used, as suggested in the edgeR user's guide. The heatmaps were produced using heatmap.2 in the gplots package (2.17.0).
Gene Ontology and pathway enrichment analyses
Based on evidence-supported annotations, Gene Ontology (GO) analyses provided descriptions of the species-specific biological roles of genes, consisting of molecular functions, biological processes, and cellular components (23). Kyoto Encyclopedia of Genes and Genomes (KEGG) analyses were adopted to systematically analyze gene functions and link genomic information with up-to-date gene annotations and possible pathways (24). GO and pathway enrichment analyses were performed using clusterProfiler (3.0.5) and topGO (2.24.0). The significance of enrichment was determined by a hypergeometric test and was adjusted for multiple testing with the Benjamini–Hochberg false discovery rate (FDR). FDR <0.05, between two samples, was adopted to identify differentially enriched GO or KEGG terms.
Immunohistochemistry staining
Surgical samples from patients with PTC (Supplementary Table S3) were fixed in 4% paraformaldehyde, followed by paraffin embedding. After deparaffinization of the sections, antigen retrieval was conducted with heat-induced epitope retrieval in 10 mM citrate buffer for five minutes. Next, the sections were incubated with 3% hydrogen peroxide for 30 minutes and blocked with AquaBlock (PP82; EastCoast Bio) for one hour at room temperature. Primary antibodies against cluster of differentiation 24 (CD24, 10600-1-AP, Proteintech), coagulation factor 5 (F5, 20963-1-AP; Proteintech), coagulation factor 12 (F12, 12551-1-AP; Proteintech), integrin subunit alpha 3 (ITGA3, 66070-1-Ig; Proteintech), mast cell (MC) tryptase (ab134931; Abcam), NCAM1/CD56 (14255-1-AP; Proteintech), CD138/Syndecan-1 (10593-1-AP; Proteintech), FOXP3 (22228-1-AP; Proteintech), and goat anti-rabbit/mouse IgG secondary antibody were used for tissue staining.
Sections were visualized using an Olympus microscope equipped with an Olympus camera and Vision 4.1 software at 200 × and 400 × magnification for each sample. Immunohistochemistry (IHC) quantification and automated scoring were conducted using “ImageJ” (version 2.1.0) and an open-source plug-in “IHC Profile” (25). IHC images were classified into cytoplasmic- or nuclear-predominant staining and imported into the software. Scores were assigned as high positive (3+), positive (2+), low positive (1+), and negative (0). Whether the samples were from CAYA or adult patients was blinded to the experimenters and researchers who interpreted the staining results.
Immunoprofiling and correlation with immune checkpoint
We used an analytical R tool, CIBERSORT (1.03), to estimate the abundance of 22 immune cell types in individual specimens, using gene expression data. CIBERSORT derived a p-value for the deconvolution for each sample using Monte Carlo sampling, providing a measure of confidence in the results. The abundance of infiltrating immune cells was represented by a rainbow column using a barplot (4.0.2). The correlation between differential infiltration of immune cells and immune checkpoints was presented by a scatter matrix by STATA.
Statistical analyses
Continuous variables are displayed as median and standard deviation, and categorical variables are presented as numbers and percentages. Kaplan–Meier (K–M) survival curves were used to evaluate differences in RFS between the two groups. The prognostic significance of various factors for remission was assessed using Cox regression analysis. To compare the mean difference between groups, logistic regression was applied. All statistical analyses were performed using STATA version 12.0 (Stata Corp, College Station, TX). Statistical significance was set at p < 0.05.
Results
Baseline characteristics of study cohort
Two hundred and seventeen CAYA-PTC patients received initial treatment at five tertiary medical institutions in Shanghai from 2006 to 2018. The mean age at diagnosis was 14.38 years (range 2–18 years). There were 162 females (74.65%) and 55 (25.35%) males (female-to-male ratio, 3:1). The mean tumor size was 25.1 mm in the maximum diameter (range 3.0–100.0), and the majority were classic papillary variants. Only 5.1% of all cancers were identified as follicular or other subtypes (26). Clinicopathological characteristics of the 217 patients are presented in Table 1.
Central lymph node metastasis (CLNM) and lateral lymph node metastasis (LLNM) were detected in 186 (85.71%) and 125 (57.60%) patients, respectively. The number of patients with co-HT was 96 (44.23%), and ETE was found in 84 patients (38.71%). During the mean follow-up period of 4.76 (range 0.38–13.01) years, the disease relapsed in 28 (12.90%) patients (Table 1).
Univariate and multivariate logistic regression for LNM and recurrence
We found no significant difference in sex, size, or pathological subtype with LNM, but a noticeably increased risk of LNM among patients with young age at diagnosis (p = 0.000), bilateral involvement (p = 0.003), ETE (p = 0.008), presence of HT (p = 0.000), and multifocal lesions (p = 0.006) in univariate analysis. In multivariate analysis, multifocal lesions were found to be not independent risk factor (p = 0.365) (Table 2).
Univariate and Multivariate Logistic Regression for Lymph Node Metastasis
CI, 95% confidence interval; N, no; OR, odds ratio; Y, yes.
Univariate analysis showed that the recurrence rate was higher in patients with larger tumor size (p = 0.023), bilateral disease (p = 0.009), co-HT (p = 0.000), and lateral neck metastasis (p = 0.021). The only independent risk factor identified in the multivariate analysis was co-HT (p = 0.001). In the average five-year follow-up after the initial surgery, there was a significantly higher risk of recurrence in CAYA-PTC patients with coexisting HT than in those without HT (p = 0.001, odds ratio = 5.942, 95% confidence interval, 2.119–16.659) (Table 3). Furthermore, the log-rank analysis demonstrated that bilateral disease (p = 0.026), LLNM (p = 0.044), co-HT (p = 0.004), and TT operation (p = 0.043) were significantly associated with DFS according to the K–M survival estimates (Fig. 1).
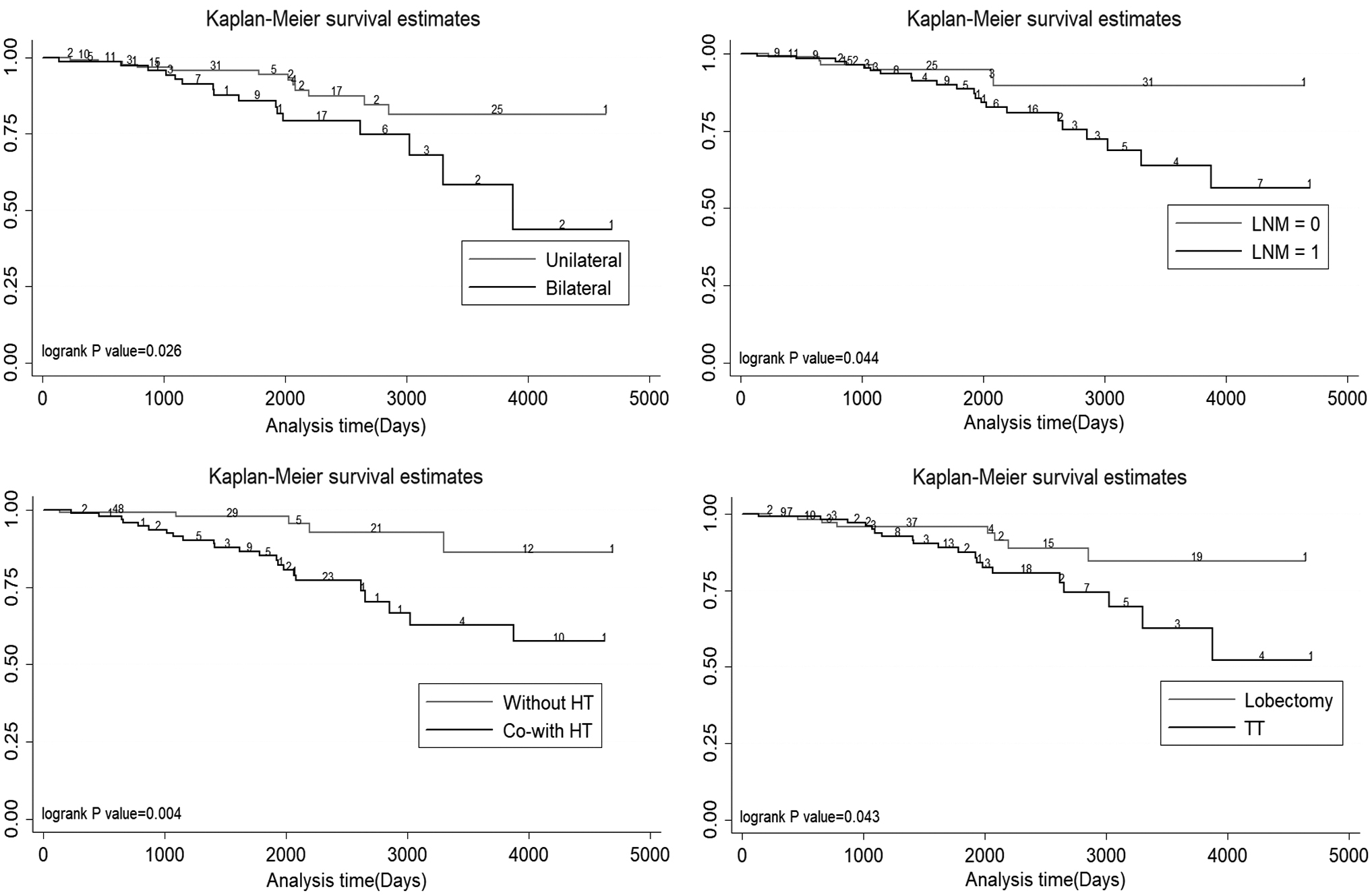
Recurrent disease-free survival of CAYA-PTC patients. CAYA, children and young adult; HT, Hashimoto's thyroiditis; LNM, lymph node metastasis; PTC, papillary thyroid carcinoma; TT, total thyroidectomy.
Univariate and Multivariate Logistic Regression for Recurrence
N, no; Y, yes.
Identification of differentially expressed genes and enrichment in GO and KEGG
To further elucidate the molecular mechanism, we identified protein-coding genes by performing whole-transcriptional sequencing that exhibited expression changes between CAYA-PTC and adult-PTC patients. The basic clinicopathological characteristics of the selected patients are shown in Supplementary Table S1. An overview of the RNA-seq reads was derived from the ENSEMBLE library using the Illumina NOVAseq platform. The clean reads ranged from 71,318,000 to 271,413,822, and the total read counts ranged from 72,756,690 to 275,292,266. The proportion of clean reads ranged from 64.64% to 97.84% in the mapping library. Correspondingly, 10,366,005,772 to 38,812,526,775 total base pairs were generated.
The hierarchical clustering heatmap and differentially expressed genes (DEGs) analysis showed the top 301 genes up- or downregulated by age (Fig. 2A). Among them, 167 genes were downregulated, and 134 genes were upregulated in the CAYA-PTC cases (Fig. 2B). GO category analysis revealed 67 items with differential expression between CAYA-PTC and Adult-PTC patients. These genes with significant differential expression mainly functioned in biological processes of the immune system (GO:0002376) (Fig. 2C, D). Pathway analysis revealed 41 processes affected by DEGs, among which immune diseases and immune system were significant (Fig. 2E, F).

Differential expressed genes in CAYA-PTC and Adult-PTC patients. (
The genetic characterization of pediatric and adult patients was illustrated using a simple schematic diagram, including DEGs, GMs, and fusion genes (Fig. 3). These genes are related to numerous cancer-related processes, such as environmental information processes, genetic information processes, metabolism, and organismal systems.
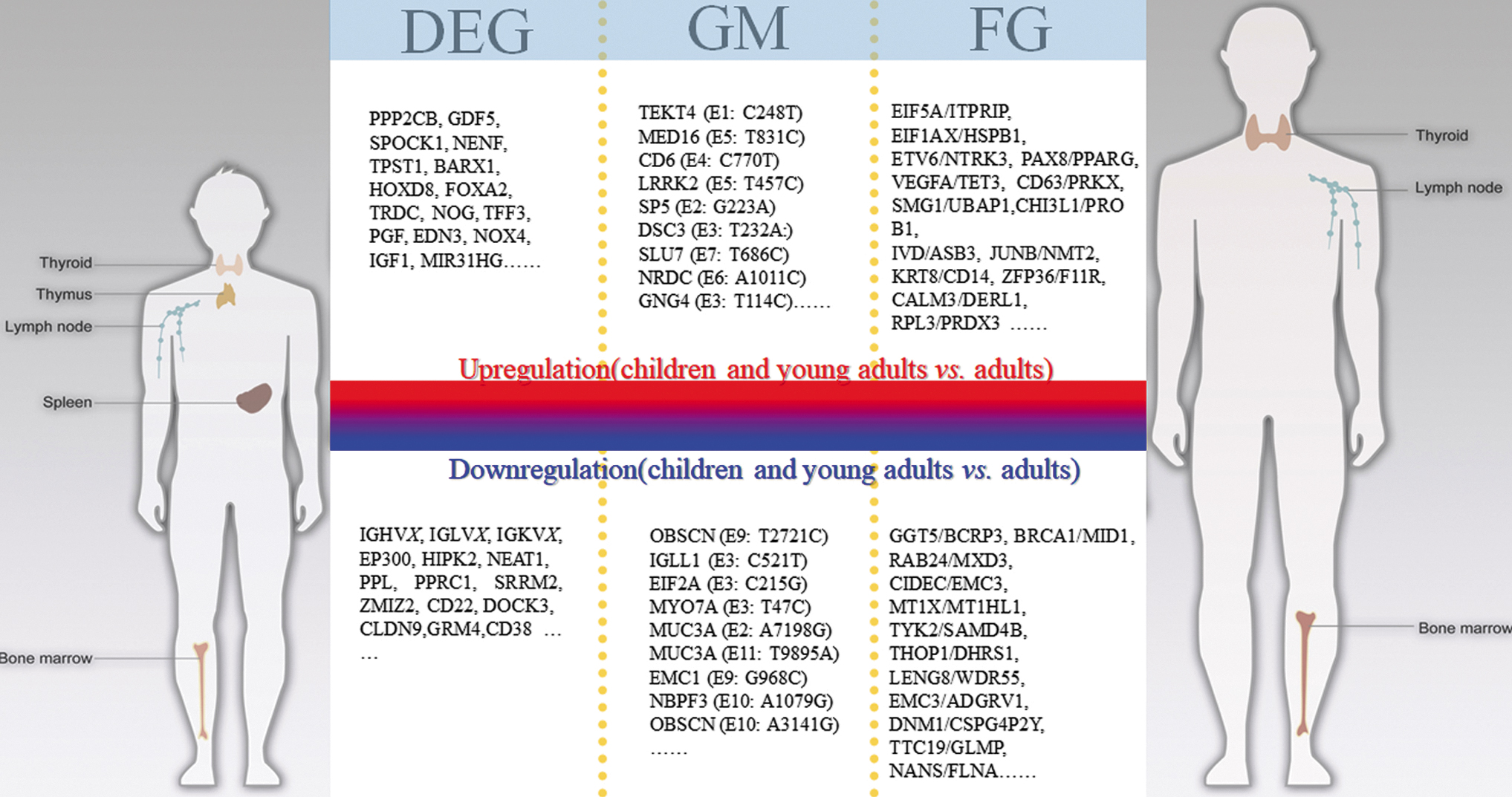
The different molecular genetic characterizations between CAYA-PTC and Adult-PTC patients. DEGs in the upper row were upregulated, and that in the lower row were downregulated. GM and FG in the upper row were occurred only in CAYA patients, and that in the lower row were only occurred in adult patients. FG, fusion gene; GM, gene mutation. Color images are available online.
Mutational landscape of PTC and validation using IHC staining
To achieve a systemic understanding of these genetic variations, we analyzed a total of 546 genes in 18 cancer-related pathways on the cBioPortal website of TCGA (
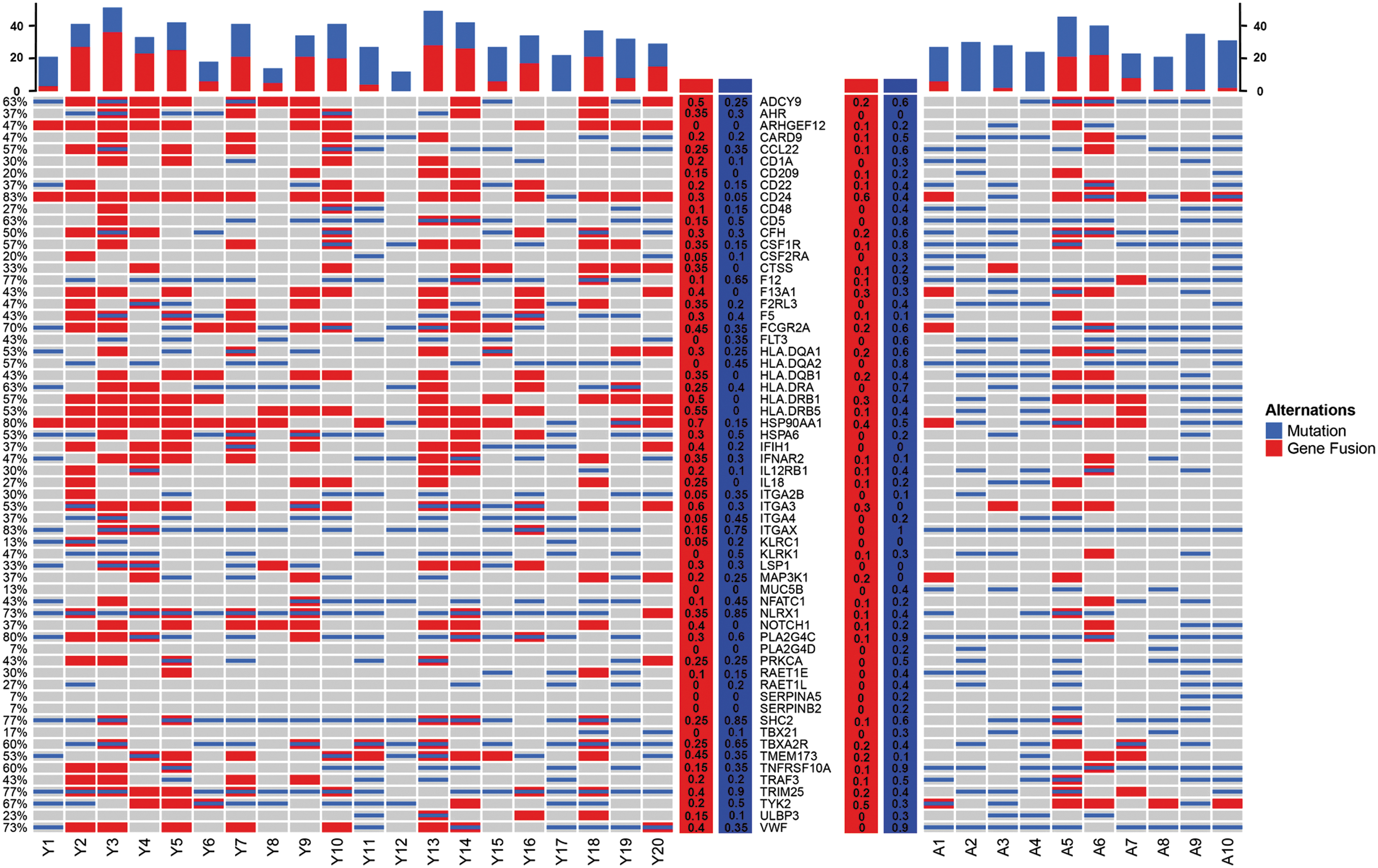
Mutational landscape of DEGs among CAYA-PTC and Adult-PTC patients. Percent mutated samples for each gene are presented in the right panel for CAYA-PTC patient and in the left for adults; rate of mutations per sample is presented in the top panel. The percentage with red background is the presentation of gene mutation, the blue is gene fusion. A, adult-PTC; Y, CAYA-PTC. Color images are available online.
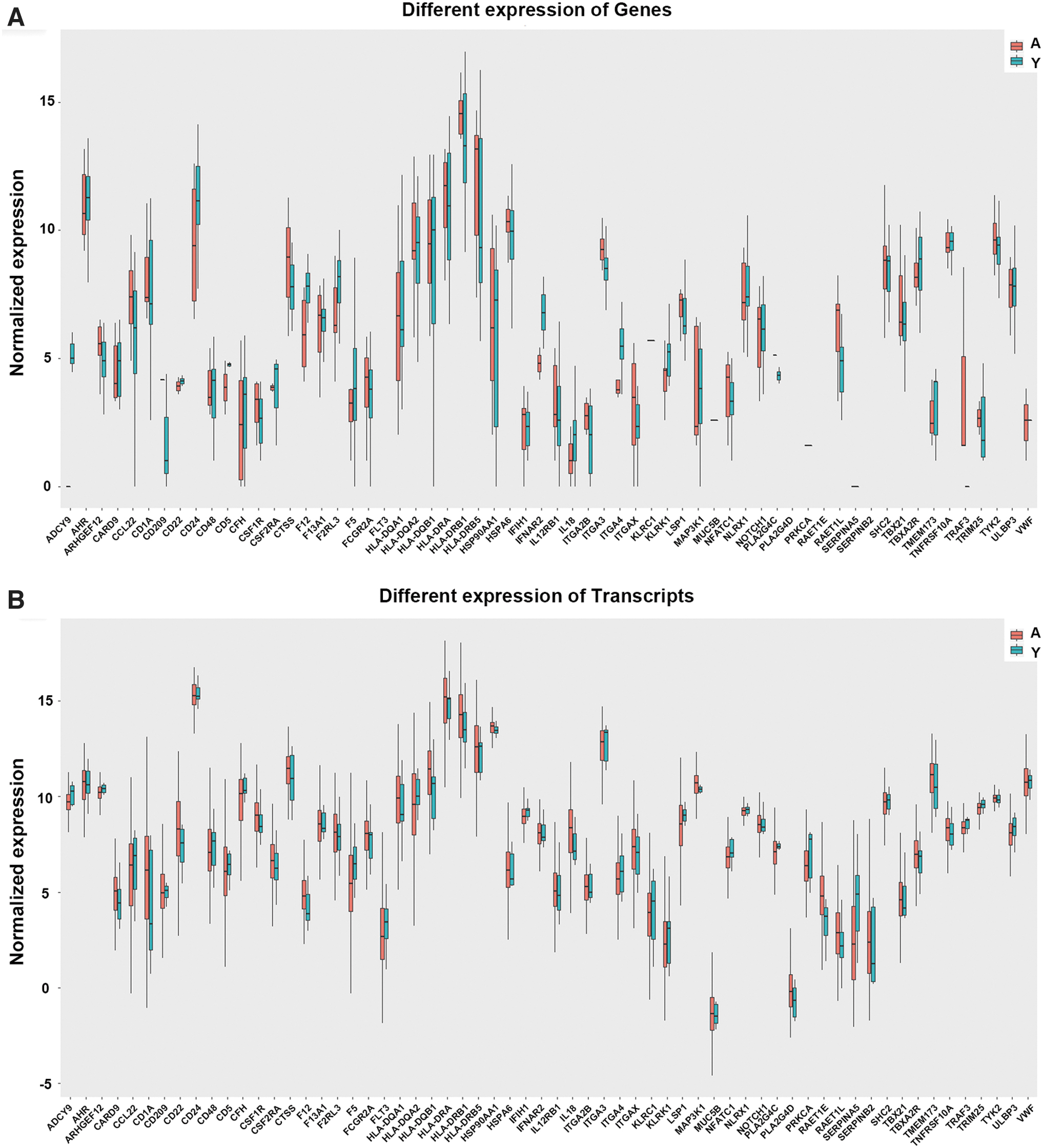
The boxplot of 57 DEGs in gene (
Next, the validation IHC staining also confirmed these four genes. These results are consistent with the sequencing analysis (Fig. 6A, B). IHC staining of CD24, F12, F5, and ITGA3 in para-cancer tissues as normalized comparison are shown in Supplementary Figure S1.
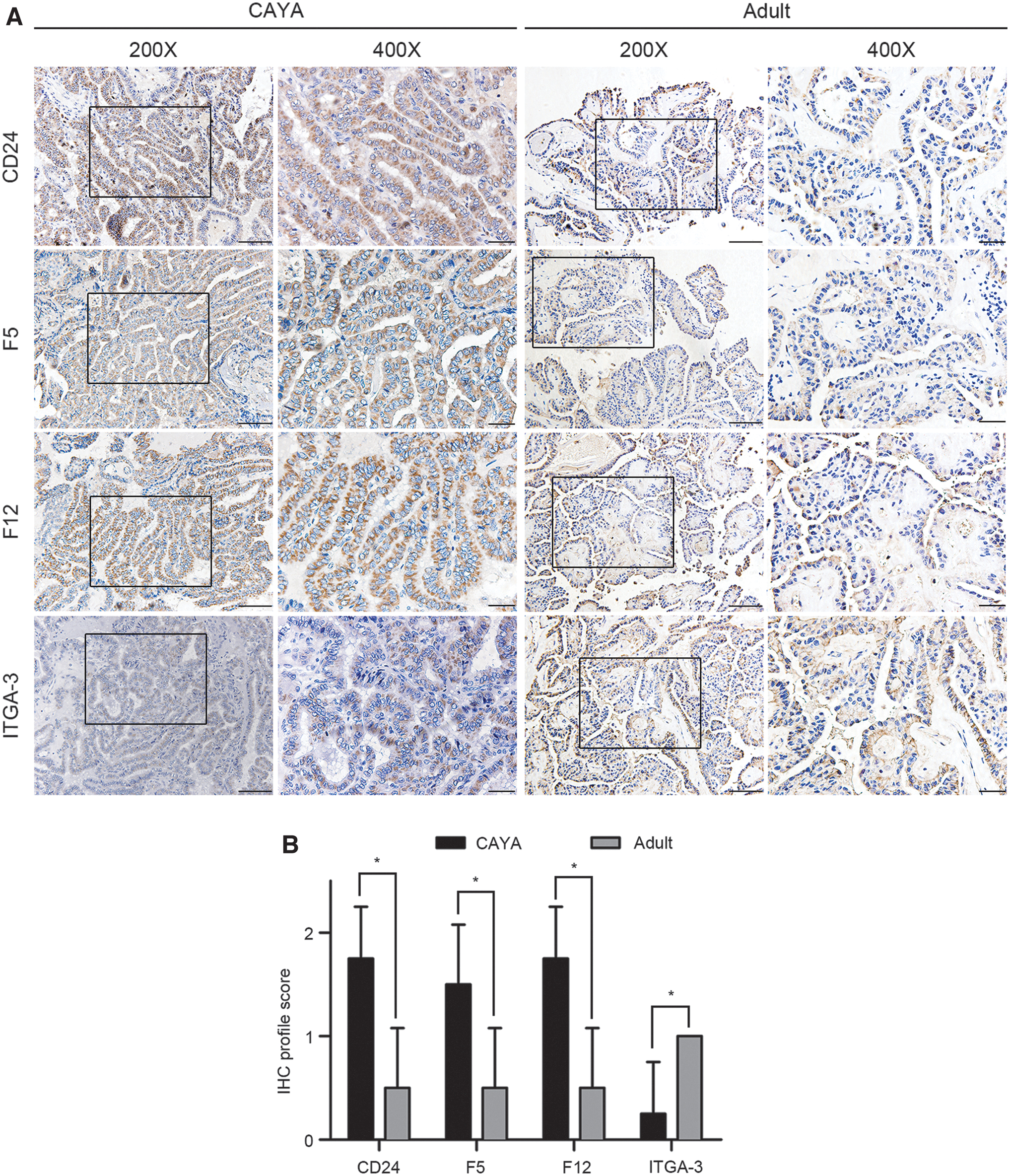
IHC staining of CAYA and Adult-PTC tissue. (
Immune cell infiltration and association with DEGs
Among the total samples, 20 CAYA and 10 adult PTC samples were eligible for analysis with the CIBERSORT database (Fig. 7). As shown in Figure 7A, the fractions of immune cells varied significantly between CAYA and adult PTC tissues. The plasma cells (p = 0.013), T regulatory cells (Tregs) (p = 0.001), and resting natural killer cells (NKs) (p = 0.001) were significantly decreased in CAYA tumor tissues. Likewise, resting MCs were significantly lower in adult tissues than in CAYA tissues (p = 0.049). Based on the aforementioned results, we considered that the proportion of plasma cells, Tregs, resting NKs, and resting MCs significantly differed between CAYA and adult TPC tissues (Fig. 7B).

Infiltration of immune cell proportions in PTC samples and its correlation with immune checkpoints. (
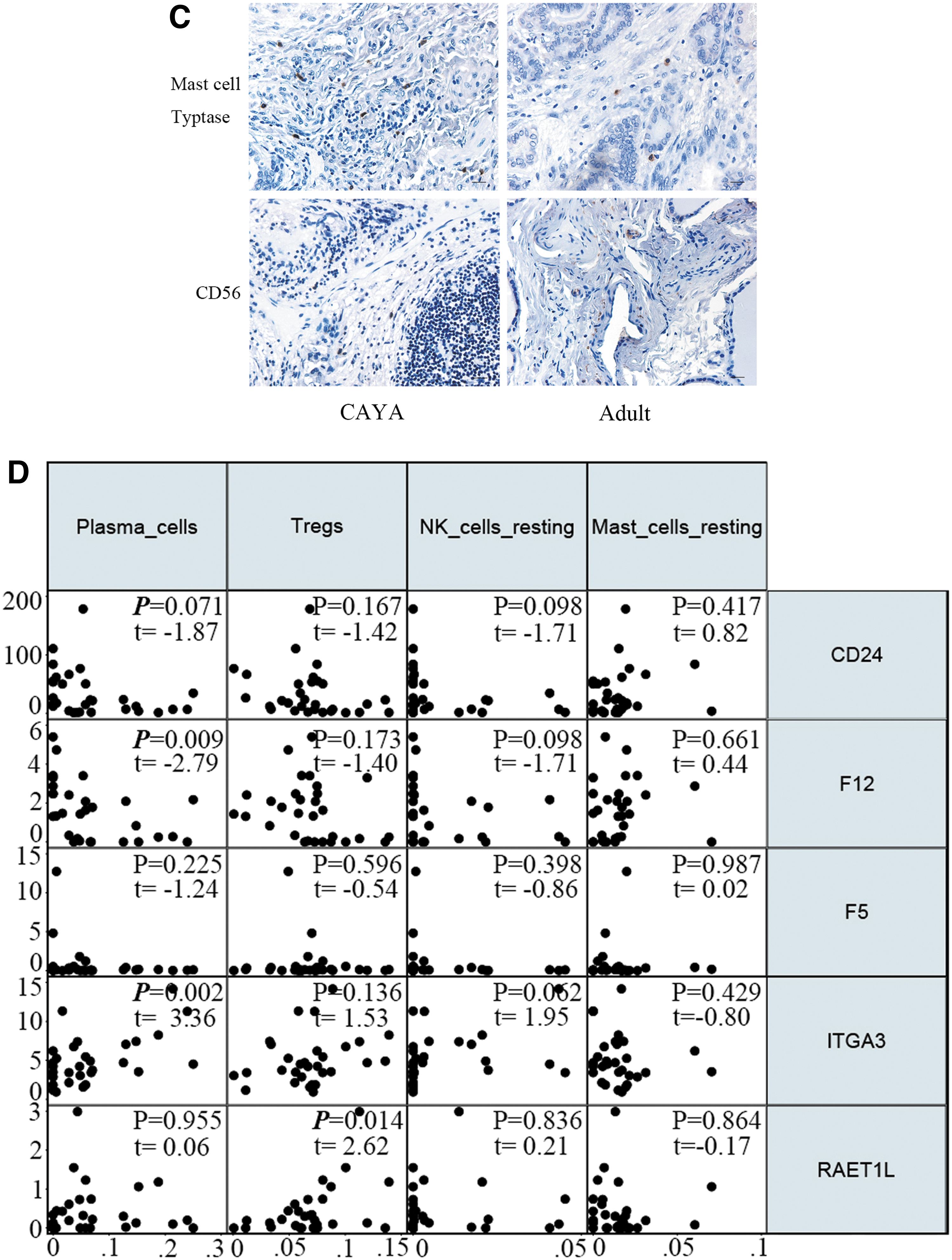
For IHC validation, we used primary antibodies against MC tryptase for MCs, NCAM1/CD56 for NKs, CD138/Syndecan-1 for plasma cells, and FOXP3 for Tregs. As shown in Figure 7C, MCs were upregulated in CAYA-PTC tissues, while percentages of CD56/CD138/FOXP3-positive cells showed no significant difference (the results of plasma cells and Tregs are not shown). Therefore, they were chosen for further analyses. We then determined the correlation between immune cells in CAYA-PTC and adult-PTC tissues (Fig. 7D). Plasma cells were negatively correlated with F12 (t = −2.79, p = 0.009) and positive with ITGA3 (t = 3.36, p = 0.002). Tregs were positively correlated with RAET1L levels (t = 2.62, p = 0.014).
Discussion
In this study, we examined the features and treatment of CAYA-PTC from multiple tertiary hospitals. Thyroid cancer in young patients showed higher rates of LNM and recurrent disease than those in adults. In CAYA-PTC, tumor size >1 cm, multifocality, ETE, diffuse sclerosing variant, and distant metastasis are associated with more aggressive disease. Patients with bilateral disease, LNM, and co-HT have a relatively poor prognosis.
PTC with RET/PTC rearrangements tended to have higher rates of capsule extension and lymph node metastases. DFS is also shorter than that with other mutations (27). In contrast, m6A-related signatures were associated with DFS in patients with PTC. IGF2BP2, one of the genes in the m6A-related module, was strongly expressed in tumor tissues and significantly correlated with clinical phenotypes of stage and ETE (28), while METTL3 plays a tumor suppressive role in PTC carcinogenesis (29).
Some studies have found that the rate of metastases in the lateral neck lymph nodes in patients >18 years of age was only 23.6%, but was 77% in CAYA-PTC patients. The lateral LNM rate in this study was 57.6%, which is concordant with previous reports (30). We found that the risk of LNM and recurrence in pediatric patients with HT increased by 9.3 and 7.3 times, respectively, compared with those without HT. Ren et al. and Zirilli et al. reported that the prevalence of chronic autoimmune thyroiditis in children peaks in early to mid-puberty, and there is a significantly higher rate of co-HT in CAYA-PTC patients. The high prevalence of thyroid nodules and cancer (mostly PTC) in juvenile autoimmune thyroiditis has also been reported (31).
Indeed, some researchers believe that thyroid autoimmunity is closely related to PTC. They hypothesize that HT could exert a promoting effect on PTC. Molecules such as chemokines, cytokines, and probably growth factors may induce secondary elevations in serum TSH levels and thyroid autoantibodies. Especially, since HT is characterized by lymphocytic infiltration, the tumor microenvironment exerted by pediatric HT patients could be an explanation for their aggressive behaviors through which cancer cells escape the immune system to facilitate their own spread.
To explore the underlying molecular mechanisms related to these differences, we constructed a whole transcriptome sequence between CAYA and adult PTC patients. GO and KEGG analysis of DEGs revealed enrichment in functional processes and critical modules related to growth development, and as expected, the immune system. In studies of pancreatic cancer, ZIP4 increased the level of the transcription factor ZEB1, which activated the expression of ITGA3 (32). In PTC, ITGA3 is increased and significantly correlates with tumor development and progression. ITGA3 is a direct target of miR-524-5p, which could inhibit PTC cell viability and migration (33).
In addition, CD24 interacts with the inhibitory receptor Siglec-10 on innate immune cells to dampen inflammatory versus host disease (34 –37). It can be a dominant innate immune checkpoint, which is a promising target for cancer immunotherapy. In our study, CD24 expression was 11 times higher in CAYA-PTC than in adults. This may be the reason why TCs are more likely to spread in children.
However, PTC development is accompanied by immune cell recruitment and infiltration by a large number of innate and adaptive immune cells (38). Our results indicated significant elevations in resting MCs and lower resting NKs, plasma cells, and Tregs in CAYA-PTC tissues, consistent with previous studies.
MCs are tissue-resident immune cells that play a protumorigenic role in the majority of solid tumors, and their effects on PTC vary with stages of tumorigenesis and their localization (39 –42). The extent of peri-, intra-, and peri-tumoral MC infiltration is associated with ETE and LNM in patients with PTC. MCs promote tumor invasiveness in poorly-differentiated TC, which may be related to the recruitment of chemokine factors such as CXCL1/GRO-α and CXCL10/IP10 (43,44). We confirmed that resting MCs were significantly enriched in the CAYA patient group, which may lead to more aggressive biological patterns.
NKs are innate immune cells that are highly involved in cancer immunosurveillance. The low cytotoxic activity of NK is associated with increased cancer risk, which could herald a protective role of NKs during carcinogenesis (45 –48). In PTC, the extent of NK cell infiltration decreases with an increase in the tumor stage (49). Besides, anaplastic thyroid cancer is responsive to NK cell-mediated lysis, leading to the hypothesis that patients can benefit from immunotherapies that incorporate the recruitment of activated NK cells in the tumor microenvironment (50). In addition, the number of plasma cells is higher in patients with PTC without metastases, reflecting the positive impact of adaptive immune activation on PTC prognosis.
In our study, resting NK cells and plasma cells were significantly elevated in adult PTC patients, which indicated that the decrease in protective immune cells and the increase in protumorigenic immune cells may be non-negligible factors in explaining the aggressiveness of CAYA-PTC.
Tregs were more frequently observed within lymphocytic aggregations in co-HT PTC than in PTC alone, and the elevation of Treg cells in primary tumors is associated with metastasis and poor prognosis (51,52). However, in our study, the methodology used to define cell subtypes, such as Treg, may result in false positives due to overlapping gene expression. This may explain why Tregs were paradoxically infiltrated in the CAYA and adult groups.
There are some limitations to our study. First, the risk stratifications of RNA-seq cases were not perfectly matched between CAYA and adults. However, given that most diagnoses of CAYA-PTC were made based on the presence of enlarged cervical lymph nodes or incidental imaging findings, the overall clinical characteristics of young patients were generally more advanced than those of adults. To eliminate extreme sample imbalance, we excluded those with distant metastases. These issues will need additional cell subset analyses, particularly for immune cell infiltration, to confirm the results of the computational analyses.
In conclusion, the decrease in protective immune cells may be an important factor in explaining the more aggressive disease in CAYA-PTC patients. Our results add to the knowledge concerning CAYA-PTC, with new insights into the pathogenesis and potential implications for prognosis prediction.
Footnotes
Acknowledgments
We gratefully acknowledge WX Liu and QQ Shi (State Key Laboratory of Oncogenes and Related Genes & Renji-Med X Clinical Stem Cell Research Center, Ren Ji Hospital, School of Medicine, Shanghai Jiao Tong University) for offering advices on compounds and antibodies and invaluable contributions during this study.
Authors' Contributions
K.G. and K.Q. analyzed and interpreted the data and wrote the article including the figures and tables; Y.S. prepared the materials and performed the experiment; LC.C. and DY.M. collected the data; TQ.S., KR.D., S.G., JB.L. and ZB.L. critical revised the manuscript for important intellectual content; ZY.W. supervised the entire work. All authors read and approved the final manuscript.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by National Natural Science Foundation of China (81772852 and 81972496), the Science and Technology Commission of Shanghai Municipality (16ZR1406600).
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Figure S1