
Abstract
Background:
Near-infrared autofluorescence (NIRAF) imaging is known to reduce the incidence of post-thyroidectomy hypocalcemia. However, there are no studies on how much NIRAF imaging affects the serum parathyroid hormone (PTH) level after surgery. We investigated the changes of the serum PTH level and ionized calcium (iCa.) in patients undergoing total thyroidectomy with central neck dissection (CND).
Materials and Methods:
This retrospective study with historical control enrolled 542 patients who underwent total thyroidectomy with CND. Patients were divided into two groups: the NIRAF group (261 patients) and the control group (281 patients). PTH and iCa. levels were measured at the hospital stay, 1, 3, and 6 months after surgery. In addition, the number of identified parathyroid glands (PGs), autotransplanted PGs, and the inadvertent resection rate of PGs was evaluated.
Results:
The incidence of postoperative hypoparathyroidism (PTH <15 pg/mL) was significantly lower in the NIRAF group during the hospitalization (88 patients: 33.7% vs. 131 patients: 46.6%; p = 0.002) and at 1 month postoperatively (23 patients: 8.8% vs. 53 patients: 18.9%; p = 0.001). There was no difference in the permanent hypoparathyroidism rate (6 months after surgery) between the NIRAF group and the control group (4.2% vs. 4.6%; p = 0.816). There was no difference in the incidence of hypocalcemia (iCa. <1.09 mmol/L) (during hospitalization: 6.5% vs. 10.0%; 1 month: 2.3% vs. 2.5%; 3 months: 0.8% vs. 0.7%; 6 months after surgery: 1.1% vs. 1.1%) between the two groups. The number of inadvertently resected PGs was significantly lower in the NIRAF group (18:6.9% vs. 36:12.8%; p = 0.021).
Conclusions:
These results suggest that NIRAF imaging may reduce temporary hypoparathyroidism and the risk of inadvertent resection of PGs in patients undergoing total thyroidectomy with CND.
Introduction
The incidence of post-thyroidectomy temporary (<6 months) and permanent (>6 months) hypocalcaemia is 15–30% and up to 7%, respectively (1 –7). Hence, one of the most critical elements in thyroidectomy is to preserve the parathyroid glands (PGs) and prevent hypoparathyroidism.
Recently, after the first report by McWade et al. on the feasibility of near-infrared autofluorescence (NIRAF) imaging for the intraoperative identification of the PGs, studies have shown the effectiveness of imaging in intraoperative parathyroid identification to prevent postoperative hypocalcemia (8 –11). Dip et al. demonstrated that the number of PGs detected increased from 2.6 to 3.5 (p < 0.001) while decreasing the incidence of severe postoperative hypocalcemia (calcium levels <7.6 mg/dL) (12). Benmiloud et al. also reported that NIRAF imaging (Fluobeam 800®; Fluoptics, France) could prevent transient hypocalcemia from 21.7% to 9.1% (p = 0.007) and reduce the rate of inadvertently resected PGs (13). However, Papavramidis et al. did not show a reduction in postoperative hypoparathyroidism or hypocalcemia risk, although NIRAF imaging can decrease the unintentional excision of PGs (28.9% vs. 14.4%, p = 0.02) and the rate of parathyroid tissue presence in the specimen (11).
We showed the feasibility of intraoperative identification of PGs with a custom-built NIRAF imaging system with digital single-lens reflex (DSLR) camera (14). Subsequently, we proposed the concept of “PG mapping” which was defined as the early localization of the PGs through localization of PGs, which were initially not visualized by the surgeon's naked eye. In our study, PG mapping was possible in 92.8% of the patients with our NIRAF imaging system (15).
These new NIRAF imaging technologies for parathyroid identification raised the expectation that they would lower the occurrence of hypoparathyroidism or hypocalcemia after total thyroidectomy with or without central neck dissection (CND). Until recently, most studies evaluated the postoperative calcium levels to determine the usefulness of NIRAF imaging in patients who had total thyroidectomy (12,13).
Measuring postoperative calcium level can be more clinically meaningfully than measuring parathyroid hormone (PTH) level; however, calcium level is influenced by various conditions, such as hydration, vitamin D supplementation, as well as PTH (16). Therefore, PTH measurement can be a more direct parameter for evaluating the efficacy of PG preservation than measuring calcium level. Thus, we examined both PTH and ionized calcium (iCa.) levels to assess the clinical utility of our NIRAF imaging system. Furthermore, all the included patients in this study had CND in addition to total thyroidectomy, which has a higher risk of postoperative hypocalcemia than total thyroidectomy alone. We analyzed the number of identified PGs, autotransplanted PGs, and the inadvertent resection rate of PGs.
Materials and Methods
The institutional review board (IRB) of Busan Paik Hospital, Inje University College of Medicine approved this study and waived the need for informed consent based on the retrospective investigation (IRB 2020-01-191-003). This study was a retrospective analysis of a cohort study using a historical control group.
All patients in this study underwent total thyroidectomy with unilateral or bilateral CND by one surgeon (K.D.L.) between November 1, 2013, and December 27, 2018, at the Department of Otolaryngology-Head and Neck Surgery, Kosin University Gospel Hospital. The surgeon had 20 years of experience and more than 3000 cases of thyroid surgery at the start of the study. The number of enrolled patients was 542, and all had thyroid cancers. All patients who had lateral lymph node metastasis were treated by the lateral neck dissection. The patients were divided into two groups: the NIRAF group (261 patients) and the control group (281 patients) based on the use of NIRAF imaging technique. The NIRAF group included patients between June 1, 2015, and December 27, 2018, while the control group was treated between November 1, 2013, and May 29, 2015. All patients were followed at least six months after surgery. Those patients who had surgery for benign tumors, goiters, thyrotoxicosis, or lobectomy cases were excluded.
In patients with severe hypocalcemia (severe carpopedal spasm, laryngospasm, or seizures, etc.) after total thyroidectomy with CND, calcium gluconate (1–2 g diluted to 50 mL of 5% dextrose or normal saline) was administered as a bolus over 10–20 minutes. In mild hypocalcemia cases (perioral numbness, paresthesia of the hands and feet, muscle cramps, mild carpopedal spasm, etc.), continuous infusion of calcium gluconate (4 g diluted to 500 mL of 5% dextrose or normal saline) for 4 hours followed by oral calcium carbonate 500 mg–1 g t.i.d. with calcitriol 0.25–0.5 μg b.i.d. postoperatively were used for the following conditions: (i) when the surgeon was concerned about damage to the PGs due to frequent manipulation during surgery; (ii) when the serum total calcium level was <7.5 mg/dL or the PTH level was <15 pg/mL after surgery; and (iii) when patients had symptomatic hypoparathyroidism regardless of the blood test results.
Equipment for NIRAF imaging
The device consisted of a modified DSLR camera, a light-emitting diode (LED) light source, and remote display system. The DSLR camera (EOS 80D; Canon, Japan) is an imaging detector that is equipped with a macro-lens. The infrared filter was taken off and replaced by an emission filter of 820/12 nm that can mainly pass the PG autofluorescence wavelength and a minimal amount of room light. The light source was a 780-nm collimated LED (M780L3-C1; THORLABS) with a 769/41 nm excitation filter. An articulation joint was installed in an endoscopic system cart commonly used in the operation room. The autofluorescence camera was mounted on the end of the arm. The computer and large remote display were connected to check the image in real time (Fig. 1).
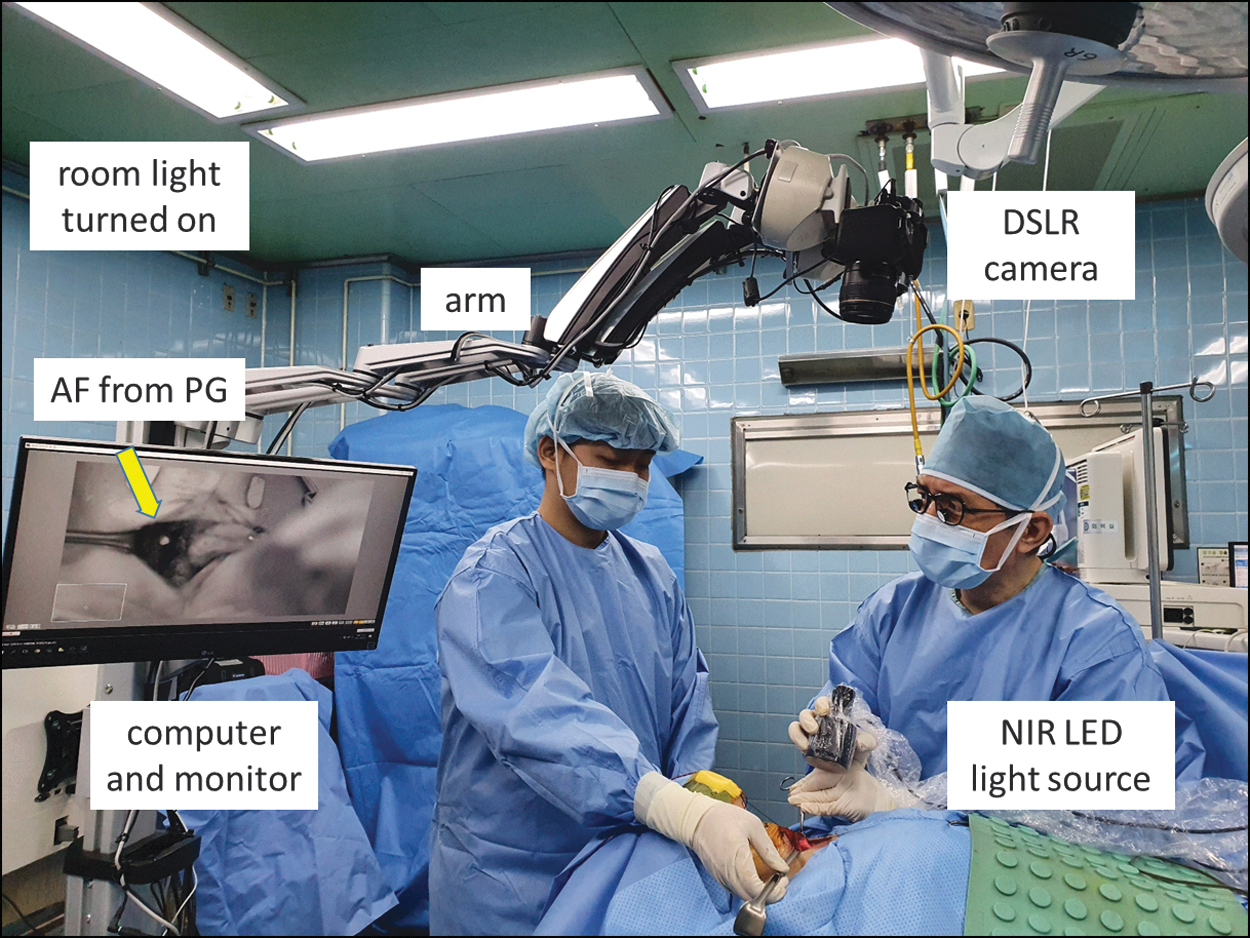
Laboratory-built DSLR camera imaging system used for NIRAF detection to identify PGs. The system consists of an NIR LED light source, DSLR camera with the emission filter, data processing computer, and display monitor. The arrow on the monitor indicates the NIRAF image from the PG. Note this camera system works in the presence of a fluorescent room light turned on during imaging, which makes it possible to maintain the workflow. NIRAF images from PGs with our DSLR camera system cannot be obtained under direct illuminating from operating light. However, when the operating light illuminates outside the surgical field (i.e., under weak indirect operating light), AF image of the PG can be obtained. AF, autofluorescence; DSLR, digital single lens reflex; NIRAF, near-infrared autofluorescence; NIR LED, near-infrared light-emitting diode; PG, parathyroid gland.
Surgical procedure and NIRAF imaging
The authors considered that the inferior PG is the most important structure responsible for hypoparathyroidism after total thyroidectomy and CND. Thus, to avoid the devascularization or inadvertent removal of the gland requiring autotransplantation, we try to routinely identify the inferior PG first before searching for the recurrent laryngeal nerve (RLN) at the paratracheal area during the study period. Before the adoption of our NIRAF imaging system for thyroid surgery, the inferior PG was identified by the naked eye. Once the gland was detected, a meticulous dissection around it was conducted to maintain the vascular pedicle. When the inferior PG was separated from the thyroid gland, it was reflected away laterally with the vascular pedicle to allow easier RLN dissection and wider paratracheal lymph node resection while preserving parathyroid function. Since we came to use the NIRAF imaging system, the first step in the procedure at the paratracheal area has been illuminating with the near-infrared light-emitting diode (NIR LED) light to the paratracheal area that contains the inferior PG. The superior PG was also identified at the thyroid upper pole in a similar way.
To detect and preserve the PGs as early as possible, we tried the PG mapping by step by step imaging as follows. When the lateral lobe of the thyroid gland was mobilized, but still the PGs were not exposed yet, the NIR LED light was illuminated to the expected areas of PGs to localize them before identification with the surgeon's naked eye (Stage P1) (Fig. 2). For PGs that were not identified with NIRAF detection at Stage P1, the imaging procedure was performed again after the dissection of the covering tissues over the PGs as the second step (Stage P2). For the third step (Stage P3), ex vivo NIRAF images were taken from the resected surgical specimens to find PGs that were not detected in stage P1 and P2 (14).
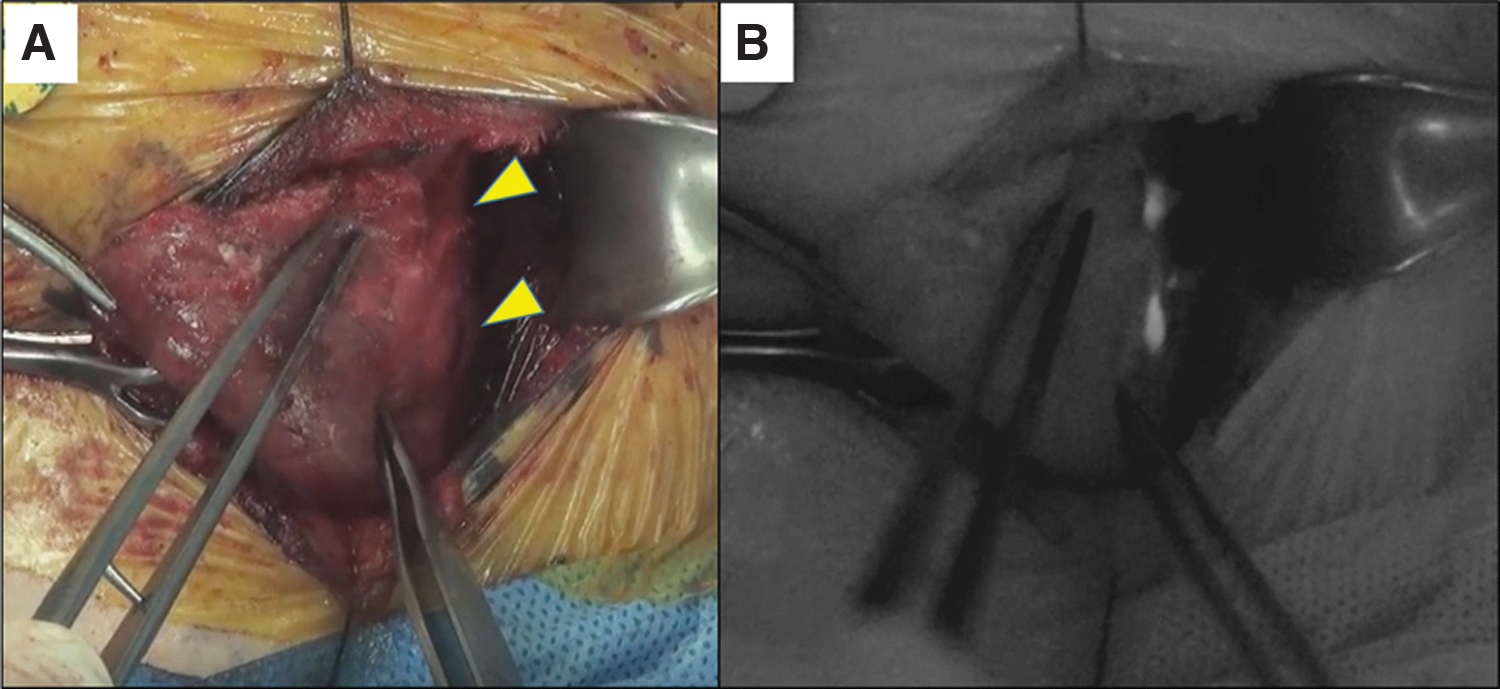
PG mapping by NIRAF imaging using DSLR camera system. Early localization of PGs that are still veiled by fatty connective tissues is possible by illuminating the NIR LED light to the paratracheal area (stage 1). Note the clearly glowing autofluorescence from PGs (
Data collection
The surgeons collected the following data using predefined forms prospectively from the study group and retrospectively from the control group: age, sex, body mass index (BMI), postoperative PTH and iCa. levels during the hospitalization, postoperative 1 month (POD 1 month), 3 months (POD 3 months), and 6 months (POD 6 months). The number of the identified, autotransplanted, and inadvertently resected PGs was also compared between the two groups.
Outcome measures
The primary outcome measure was transient postoperative hypoparathyroidism, defined as a PTH level lower than 15 pg/mL that lasted <6 months, and permanent hypoparathyroidism was defined as PTH level lower than 15 pg/mL at 6 months of follow-up. Temporary and permanent hypocalcemia were defined as an iCa. level (<1.09 mmol/L) at the same time points as the PTH levels that were measured (16). To make sure that the autofluorescent area is parathyroid tissue, histological validation is required. However, as histological validation for healthy PGs may pose ethical problems due to the risk of performing a biopsy, the visual assessment and confidence level of the experienced surgeon, which were suggested by McWade et al., were employed in the NIRAF group (8). The potential of the tissue being PG was rated as high, medium, or low. PGs that were rated as low confidence were not included.
In the NIRAF group, when four PGs could not be found in the surgical field or PGs were intentionally removed due to extensive nodal metastasis or a tissue suspected of being a PG in the specimen, NIRAF imaging was applied to the resected thyroid and CND specimens. Autotransplantation was conducted if the missed or intentionally removed PGs were identified from the removed specimen. The inadvertently resected PGs were defined as those PGs identified in the pathological report after surgery.
Statistical analyses
Continuous data are presented as mean and standard deviation (SD), while categorical data as frequency (%). The χ 2 test was used to assess differences in percentages, and the Student's t-test was used for mean comparisons. Statistical significance was set at p ≤ 0.05. All analyses were conducted using SPSS, version 25.0 (SPSS, Inc.).
Results
The NIRAF group was composed of 261 patients (206 females and 55 males, mean age ± SD: 51.30 ± 12.44 years), while the control group was composed of 281 patients (227 females and 54 males, mean age ± SD: 52.83 ± 10.92 years). The BMI was 24.61 ± 3.93 and 24.25 ± 3.66, respectively. Unilateral and bilateral CND were performed in 163 (62.5%) and 98 (37.5%) in the NIRAF group and 167 (59.4%) and 114 (40.6%) in the control group, respectively. Locally advanced tumors (thyroxine) were present in 23 (8.8%) patients in the NIRAF group and 23 (8.2%) patients in the control group (p = 0.793). There was no difference in sex, age, BMI, extent of the CND, and advanced tumors between the two groups. However, tumor size, central lymph node metastasis, and lateral lymph node metastasis were higher in the NIRAF group (p < 0.05) (Table 1).
Demographics
Chi-square test.
Student's t-test.
BMI, body mass index; CND, central neck dissection; n, number of patients; NIRAF, near-infrared autofluorescence.
The incidence of transient postoperative hypoparathyroidism was significantly lower in the NIRAF group than in the control group during hospitalization (88 patients: 33.7% vs. 131 patients: 46.6%; p = 0.002) and at POD 1 month (23 patients: 8.8% vs. 53 patients: 18.9%; p = 0.001). The mean values of PTH were significantly higher during hospitalization (22.70 vs. 19.17 pg/mL; p = 0.011) and at postoperative 1 month (29.27 vs. 25.37 pg/mL; p = 0.001) in the NIRAF group showing that the NIRAF group had a higher normal parathyroid function than the control group at each period (odds ratio [OR]: 1.71, p = 0.002 in hospital; 2.40, p = 0.001 at 1 month). There was no difference in the incidence of hypoparathyroidism between the two groups at POD 3 and 6 months (Table 2).
Univariate Analysis for the Use of Near-Infrared Autofluorescence Associated with Postoperative Hypoparathyroidism
In hospital, at the time of laboratory test of post-thyroidectomy PTH level during hospital stay; 1 month, at the time of the laboratory test of post-thyroidectomy PTH level 1 month postoperatively; 3 months, at the time of the laboratory test of post-thyroidectomy PTH level 3 months postoperatively; 6 months, at the time of laboratory test of post-thyroidectomy PTH level 6 months postoperatively. OR, univariate analysis for the use of the NIRAF associated with postoperative hypoparathyroidism (PTH <15 pg/mL).
Chi-square test.
CI, 95% confidence interval; OR, odds ratio; PTH, parathyroid hormone.
The incidence of hypocalcemia during hospitalization was 17 patients (6.5%) in the NIRAF group and 28 patients (10.0%) in the control group. The hypocalcemia rate in the two groups was 6 patients (2.3%) versus 7 patients (2.5%) at 1 month; 2 patients (0.8%) versus 2 patients (0.7%) at 3 months; and 3 patients (1.1%) versus 3 patients (1.1%) at 6 months. There was no significant difference in the rate of hypocalcemia between the two groups for all follow-up periods (Table 3). When patients with bilateral CND were compared with patients with unilateral CND in the NIRAF group, the incidence of hypoparathyroidism was significantly higher only at 1 month in the bilateral CND group. When all patients including both the NIRAF and control groups were divided into bilateral versus unilateral CND, the hypoparathyroidism rate was significantly higher in the bilateral CND group during hospitalization and at 1 month. However, there were no significant differences in the hypoparathyroidism or hypocalcemia rate between bilateral versus unilateral CND in the remaining follow-up period (Table 4).
Univariate Analysis for the Use of Near-Infrared Autofluorescence Associated with Postoperative Hypocalcemia
In hospital, at the time of laboratory test of post-thyroidectomy iCa. level during hospital stay; 1 month, at the time of the laboratory test of post-thyroidectomy iCa. level 1 month postoperatively; 3 months, at the time of the laboratory test of post-thyroidectomy iCa. level 3 months postoperatively; 6 months, at the time of laboratory test of post-thyroidectomy iCa. level 6 months postoperatively. OR, univariate analysis for the use of the NIRAF associated with postoperative hypocalcemia (iCa. <1.09 mmol/L).
Chi-square test.
iCa., ionized calcium.
Comparison of the Incidence of Hypoparathyroidism and Hypocalcemia Between Unilateral and Bilateral Central Neck Dissection
In hospital, at the time of laboratory test of post-thyroidectomy PTH level during hospital stay; 1 month, at the time of the laboratory test of post-thyroidectomy PTH level 1 month postoperatively; 3 months, at the time of the laboratory test of post-thyroidectomy PTH level 3 months postoperatively; 6 months, at the time of laboratory test of post-thyroidectomy PTH level 6 months postoperatively.
Chi-square test.
The number of identified PGs during total thyroidectomy with CND showed no difference between the two groups (p = 0.895). PGs were found in 244 cases (93.5%) in the NIRAF group and 260 cases (92.5%) in the control group. The mean count of identified PGs was 3.91 ± 0.36 in the NIRAF group versus 3.90 ± 0.39 in the control group (p = 0.351). There were 10 autotransplanted PGs in the NIRAF group and 10 cases in the control group (p = 0.866). The number of inadvertently resected PGs in the pathological specimen was 18 (6.9%) in the NIRAF group and 36 (12.8%) in the control group, significantly lower in the NIRAF group (p = 0.021) (Table 5). The number of autotransplanted PGs in both groups was similar, but the situation of parathyroid identification was different. In the NIRAF group, 10 autotransplanted PGs were detected by NIRAF imaging. Of these, 5 PGs were found in the central node specimens, which were removed from the surgical field, and 4 were identified in the resected thyroid gland specimens. Only 1 PG was harvested and autotransplanted from the surgical field due to dark color change. However, in the control group, 9 of 10 PGs were autotransplanted from the surgical field due to concern for poor vascularization of the PGs. One PG was found in the resected thyroid gland specimen (Table 6).
Numbers of Identified, Autotransplanted, and Inadvertently Resected Parathyroid Glands
Chi-square test.
Student's t-test.
PG, parathyroid gland.
Individual Analysis of Autotransplanted Parathyroid Glands
n = number of PG.
Discussion
NIR fluorescence imaging technologies have been used in thyroid and parathyroid surgery with exogenous contrast agents or with autofluorescence of PG (9 –11,17 –19). However, as intravenous injection of the contrast dye may lead to neurotoxicity, photobleaching, and pain at the infusion site (20,21), NIRAF imaging technology, which is harmless to the patients, has been developed for PG identification (8,11,22 –25).
Currently, commercially available imaging-based modalities include Fluobeam 800, Fluobeam LX® (Fluoptics), PDE Neo II® (Hamamatsu, Japan), and Karl Storz cameras® (Karl Storz, Germany) (26). We custom-built NIRAF imager that uses a DSLR camera and suggest “PG mapping” for early localization of PGs before identification by the surgeon's naked eye (14,15). Although NIRAF can be helpful to identify PGs during surgery, the clinical utility of imaging to prevent hypoparathyroidism or hypocalcemia still needs further research. Dip et al. evaluated the effectiveness of NIRAF (Fluobeam 800) on the incidence of postoperative hypocalcemia. They suggested that compared with the white light (naked eye), NIRAF imaging during thyroidectomy increases the identification of PGs, enhances their detection ability before the thyroid dissection, and decreases the incidence of severe postoperative transient hypocalcemia (defined as serum calcium <7.6 mg/dL) (12). However, no significant difference was found in the incidence of transient hypocalcemia when hypocalcemia was defined as a serum calcium level of <8.0 mg/dL.
In another study, DiMarco et al. demonstrated that NIRAF imaging might detect inadvertent parathyroidectomy and allow autotransplantation. However, there was no difference between the NIRAF imaging and control groups on inadvertent parathyroidectomy. Furthermore, significant differences were not shown in serum calcium or PTH at one day, two weeks, or thereafter. Thus, they concluded that current NIR imaging technology does not appear to confer a clinical benefit sufficient to justify its use (27). However, Benmiloud et al. conducted a multicenter randomized clinical trial to determine if intraoperative NIRAF imaging system is useful to improve parathyroid preservation and reduce postoperative hypocalcemia (13). They demonstrated that the use of NIRAF could reduce the temporary postoperative hypocalcemia rate from 21.7% (26 of 120 patients, the control group) to 9.1% (11 of 121 patients, the NIRAF group) (p = 0.007). They also showed that fewer patients required parathyroid autotransplantation in the NIRAF (+) group than in the control group: 4 patients versus 16 patients (3.3% vs. 13.3%; p = 0.009), respectively, and the number of inadvertently resected PGs was significantly lower in the NIRAF group than in the control group: 3 patients versus 14 patients (2.5% vs. 11.7%; p = 0.006), respectively.
While most of these studies mainly dealt with the incidence of hypocalcemia in patients with total thyroidectomy (12,13), we investigated if the NIRAF imaging with our custom camera system could reduce hypoparathyroidism in patients who had total thyroidectomy and CND. Although hypocalcemia is a common method for the assessment of parathyroid function after total thyroidectomy and CND, it may occur independent of hypoparathyroidism or can be affected by postoperative fluid infusion or vitamin D or calcium intake, the PTH level is directly measure of PG function, and untreated hypoparathyroidism always leads to hypocalcemia (16,28,29). Thus, in this study, to represent the status of postoperative parathyroid function more precisely, serum PTH level was measured as well as iCa. level. Clinicopathologic differences were observed in tumor size, central lymph node metastasis, and lateral lymph node metastasis between the two groups compared in this study (Table 1). Despite the higher rate of more advanced disease in the NIRAF group, there was a lower incidence of hypoparathyroidism and higher mean levels of serum PTH during hospitalization and 1 month after surgery in the NIRAF group (33.7% vs. 46.6% during hospital stay, 8.8% vs. 18.9% at POD 1 month) (Table 2). The OR of normal PTH function (PTH >15 pg/mL) was higher in the NIRAF group during hospital stay (OR: 1.72) and at postoperative 1 month (OR: 2.40). This suggests that the NIRAF imaging could reduce the incidence of temporary hypoparathyroidism in patients with total thyroidectomy and CND.
Nonetheless, compared with other studies that mainly focus on total thyroidectomy (30 –32), the incidence of immediate hypoparathyroidism (PTH <15 pg/mL) after surgery seems relatively higher in this study (33.7% in the NIRAF group and 46.6% in the control group). It may be due to that our study included patients who had CND, which is a well-known risk factor of postoperative hypoparathyroidism (16,33). The extent of CND (unilateral vs. bilateral) and hypoparathyroidism was also evaluated. The rate of hypoparathyroidism was higher in bilateral CND regardless of the use of the NIRAF imaging during hospitalization and at 1 month. Bilateral CND in the NIRAF group was associated with a higher rate of hypoparathyroidism at postoperative 1 month (Table 4).
When performing CND, it is inevitable to identify and dissect the inferior PG. Thus, to preserve parathyroid function, as described in the surgical technique, we tried to find the inferior PG first during CND. The use of NIRAF imaging may have facilitated the preservation of a high number of in situ PGs in the operation field. Nevertheless, the authors experience that the high number of the preserved PG does not necessarily mean the preservation of parathyroid function. One explanation may be the identification and dissection of PG may often lead to subtle damages or devascularization (34). Consequently, the risk of temporary hypoparathyroidism was higher than expected, even though an average of 3.9 PG was preserved. We believe that the experience of the surgeon for the preservation of parathyroid perfusion is still necessary in addition to NIRAF imaging.
Although our study revealed that NIRAF imaging can reduce temporary hypoparathyroidism, there was no difference in preventing permanent hypoparathyroidism. One of the reasons may be that all the surgeries were performed by a single experienced hand (K.D.L.). This situation seems very similar to intraoperative neural monitoring, which can reduce RLN identification time and decrease the rate of temporary vocal cord paralysis (35).
The incidence of hypocalcemia (6.5% in the NIRAF group and 10.0% in the control group) that occurred immediately after surgery was lower than that of hypoparathyroidism in both groups (PTH <15 pg/mL: NIRAF group [33.7%] and control group [46.6%]) (Table 3). This is likely due to the measured iCa. level being influenced by various factors, such as prophylactic calcium and vitamin D administration, and preoperative hydration status (16,29).
In this study, there was no difference in the number of autotransplanted PGs between the two groups. However, the circumstances of the transplantation were different. Of the 10 transplanted PGs from 10 NIRAF patients, only 1 PG in the surgical field showed low viability (dark color). The 9 transplanted PGs were not from the surgical field. In other words, 4 PGs were found in the resected thyroid gland specimen by NIRAF imaging. These were partially or totally embedded in the thyroid gland (type A2: according to Su et al.) (36). The rest of 5 PGs were detected in the fat tissue of the CND specimen. This means that the 9 transplanted PGs from the specimens in the NIRAF group might have been inadvertently resected. Although all the 9 patients suffered temporary hypoparathyroidism, none of them had permanent hypoparathyroidism. In contrast, in the control group, 9 of 10 transplanted PGs were found in the surgical field with low viability. Only 1 PG was found in the resected thyroid gland ex vivo. When considering autotransplantation of the PGs that were found by NIRAF imaging in the resected specimen, caution is necessary because false positive may occur from metastatic lymph nodes (37). Visual inspection may aid in differentiating metastatic lymph nodes from PGs in this circumstance. However, if in doubt, frozen section analysis may be required before transplantation to rule out metastatic disease. The incidence of inadvertent PGs resection itself was significantly lower in the NIRAF group (18 vs. 36; p = 0.021) (Table 5). We believe that NIRAF imaging can be of great help in minimizing the risk of inadvertent removal of PGs.
Although every patient enrolled in this study underwent surgery by a single experienced surgeon, the attitude of the surgeon to identify and preserve PGs may have been affected by his awareness of the NIRAF device. Due to the nonrandomized retrospective design, such limitation of the study may have led to bias to compare the outcomes between the two groups. To clarify the certainty of PG identification, quantification of NIRAF images might be helpful. However, in this study, the interpretation of NIRAF images for PG identification was based on the surgeon's experience rather than the quantification. This is another limitation of the study. It should be noted that the imaging system utilized is custom-built and needs to be validated in future studies.
In conclusion, this study demonstrates that the NIRAF imaging with a DSLR camera system can reduce temporary hypoparathyroidism and the risk of inadvertent resection of PGs in patients undergoing total thyroidectomy and CND. NIRAF imaging could be considered as an adjunct tool to reduce transient postoperative hypoparathyroidism.
Footnotes
Authors' Contributions
Conception and design: D.H.K. and K.D.L. Administrative support: S.W.K. and Y.-C.A. Provision of study materials or patients: S.W.K., Y.K., and Y.-C.A. Collection and assembly of data: P.K., S.Y.P., H.S.L., and J.C. Data analysis and interpretation: S.W.K. and H.S.L. Article writing: D.H.K. Final approval of article: K.D.L.
Author Disclosure Statement
Pukyong National University and K.D.L. and S.W.K. have a patent on the real-time parathyroid imaging device that has been licensed to U2medteck (Ulsan, South Korea), which encompasses use of the PGImager. This laboratory-built NIRAF imaging device has not been allowed for commercial usage.
Funding Information
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (project no.: 2018R1A2B6005604, 2019M3E5D1A02070860).
Supplementary Material
Supplementary Table S1