
Abstract
Background:
Thermal ablation (TA) has been applied in patients with low-risk papillary thyroid microcarcinoma (PTMC) who refuse surgery or active surveillance (AS). Recently, TA has been proposed as a potential therapeutic option for patients who are suitable for surgery or AS. However, the clinical outcomes of TA versus surgery remains controversial because of a lack of sufficient data. This study aimed to compare the clinical outcomes between radiofrequency ablation (RFA) versus thyroid lobectomy (TL) for low-risk PTMC in a large cohort.
Methods:
This retrospective study evaluated 884 patients with unifocal low-risk PTMC treated with TL or RFA from June 2014 to March 2018. Among them, 460 patients underwent TL (TL group) and 424 patients, who refused surgery or AS, underwent RFA (RFA group). Patients were regularly followed up after treatment. Local tumor progression, recurrence-free survival (RFS), complications, and treatment variables, including procedure time, estimated blood loss, hospitalization, and cost, were compared after propensity score matching (PSM).
Results:
After PSM, a total of 332 patients underwent TL (mean ages 43.8 ± 9.5 years) and 332 underwent RFA (mean ages 44.1 ± 9.5 years). During the follow-up (median [interquartile ranges], 48.3 [23.2] months), no significant differences were observed in local tumor progression (1.8% vs. 3.3%, p = 0.209), lymph node metastasis (0.6% vs. 0.6%, p = 1.000), recurrent PTMC (1.2% vs. 2.4%, p = 0.244), persistent lesion (0% vs. 0.3%, p = 0.317), and 4-year RFS rates (98.2% vs. 97.0%, p = 0.223) between the TL and RFA groups. Distant metastasis was not detected. None of the patients who were treated by RFA underwent delayed surgery. Patients undergoing RFA had shorter procedure time (3.4 [2.5] vs. 86.0 [37.0] minutes, p < 0.001), lower estimated blood loss (0 vs. 20 [10.0] mL, p < 0.001), shorter hospitalization (0 vs. 7.0 [3.0] days, p < 0.001), lower cost ($2035.7 [254.0] vs. $2269.1 [943.4], p < 0.001) and lower complication rate (0% vs. 4.5%, p < 0.001) than those treated by TL. The association between treatment modality and recurrence remained nonsignificant after Cox analysis (p = 0.247).
Conclusions:
This large matched study revealed comparable four-year clinical outcomes between RFA and TL for low-risk PTMC. As a minimally invasive modality, RFA may be a promising alternative to the existing treatment options for low-risk PTMC.
Introduction
The global incidence of papillary thyroid microcarcinoma (PTMC), a papillary thyroid cancer with a maximum diameter of 1 cm in size regardless of the presence or absence of high-risk features (1,2), has been increasing for the past decades (3,4), and the optimal management remains controversial. Most PTMCs have excellent prognosis; however, concerns regarding overdiagnosis and overtreatment are growing.
Active surveillance (AS) is considered a new conservative option for low-risk PTMC, defined as a PTMC without clinically evident metastases or local invasion and no convincing cytological evidence of an aggressive subtype of tumor (5). Although support for AS has been established in Japan (6), the willingness to accept this management in other counties seems to be low and varied (5). Without clinical, imaging, or biomarkers that can accurately distinguish the small percentage of aggressive PTMC from the majority of indolent tumors, patients have to confront the possibility of the tumor being aggressive with metastases and suffer the associated psychological anxiety (7). Patient anxiety is also the most common reason for delayed surgery during AS (8). Moreover, many health care providers are concerned about providing AS in real-world practice (6), such as availability and acceptance of routine ultrasound (US), quality and consistency of longitudinal evaluation, as well as the health care or medical insurance policy (9,10). Therefore, the current standard treatment for PTMC is still surgery (5), and thyroid lobectomy (TL) has been recommended as the first-line option instead of total thyroidectomy (TT) for low-risk PTMC (5). TL for low-risk PTMC effectively removes the primary tumor (11), but may result in scar formation, complications, and poor quality of life (12).
As another treatment approach, US-guided thermal ablation (TA), including radiofrequency ablation (RFA), microwave ablation (MWA) and laser ablation (LA), has been recommended as an alternative to surgery for symptomatic benign thyroid nodules and recurrent thyroid cancers (5,13 –17). Although TA is not considered as a routine treatment for primary PTMC according to published guidelines (5,11,13,17,18), low-risk PTMC patients have undergone this treatment either because surgery was not feasible or AS was refused (19 –23). Recently, in some centers, TA was also proposed as a potential therapeutic option for low-risk PTMC in patients who are suitable for surgery or AS (24). To date, only a few studies have compared TA and surgery in low-risk PTMC, including MWA versus surgery (TT and TL) (25), MWA versus TL with cervical lymph node dissection (CND) (26), LA versus TL+CND (27), RFA versus surgery (TL, TL+CND, TT, and TT+CND) (28), and the results demonstrated no differences in clinical outcomes between different treatment modalities. However, these studies were small series, included different surgeries or lacked matched control groups. Moreover, none have reported the clinical outcomes between the first-line treatment TL versus TA.
Therefore, the aim this study was to perform a propensity-matched cohort analysis of patients with unifocal low-risk PTMC treated with TL or RFA and determine patient outcome.
Materials and Methods
This retrospective study was approved by the Institutional Review Board of China PLA General Hospital. All the patients underwent treatment at China PLA General Hospital and provided written informed consent before treatments. The RFA informed consent emphasized that surgery was the standard treatment procedure recommended by guidelines, and RFA could not prevent recurrent PTMC and undetectable lymph node metastasis (LNM).
The inclusion criteria were (a) unifocal PTMC confirmed by core-needle biopsy (CNB) with maximum diameter no larger than 10 mm; (b) no clinical or imaging evidence of capsular infiltration, extrathyroidal extension (ETE), LNM and distant metastasis on US, and chest computed tomography (CT); (c) no history of neck irradiation; and (d) a follow-up period of ≥24 months. The exclusion criteria were (a) patients with convincing evidence of aggressive PTMC by biopsy (5); (b) ETE or metastasis; (c) other malignant disease; and (d) a follow-up period <24 months or data missing. The electronic medical records of 2411 patients with low-risk PTMC who underwent treatment between June 2014 and March 2018 were reviewed. After the exclusion of patients, 460 patients underwent TL and 424 patients treated by RFA were included in this study (Fig. 1).

Study flow diagram. CND, cervical lymph node dissection; PSM, propensity score matching; PTMC, papillary thyroid microcarcinoma; RFA, radiofrequency ablation; TL, thyroid lobectomy; TT, total thyroidectomy.
Pre-treatment evaluation
All patients underwent thorough examinations before treatment, including complete blood count, thyroid function tests, coagulation tests, and imaging evaluation, including US and chest CT to exclude clinical evidence of ETE, or local/distant metastases (19,20,29). The tumor volume was calculated using the following equation: V = πabc/6 (V is the volume, while a is the largest diameter on US, b and c are the other two perpendicular diameters).
Treatment and follow-up
TL procedures were performed by surgeons with >20 years' experience in thyroid surgery. Patients underwent TL under general anesthesia in the operating room. All the patients underwent TL without prophylactic ipsilateral CND.
The RFA procedures were performed by an experienced US physician with >20 years' experience in thyroid and interventional US. Patients underwent RFA under local anesthesia in an outpatient clinic. A bipolar RFA generator (CelonLabPOWER; Olympus Surgical Technologies Europe) and an 18-gauge bipolar RF applicator with 0.9 cm active tip were used (CelonProSurge micro 100-T09; Olympus Surgical Technologies Europe) in this study (20). RFA was performed using trans-isthmic approach with moving-shot and hydrodissection techniques (13). Normal saline was injected using another needle (23 gauge) to separate the target tumor from critical structures to prevent thermal injury (20) (Fig. 2). We enlarged the ablation area that exceeded the tumor edge (by at least 3–5 mm) to prevent marginal residual tumor and recurrence (30). Contrast-enhance US (CEUS) was performed immediately after RFA to evaluate the ablation area. CEUS was performed after bolus injection of SonoVue (2.4 mL), followed by 5 mL of normal saline flush. Complementary ablation was performed if any enhancement was seen on CEUS (20).
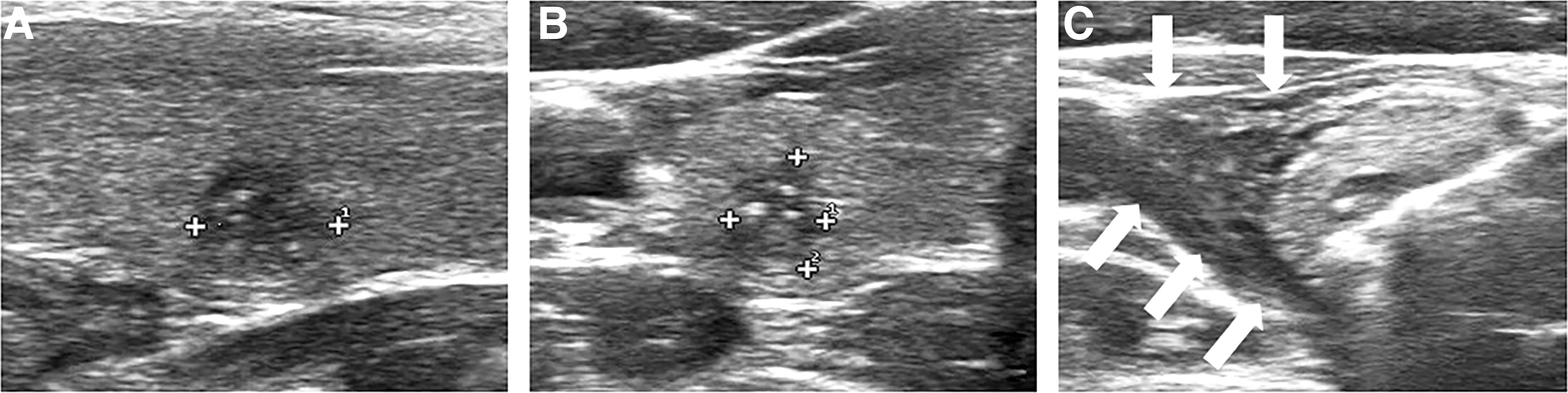
The hydrodissection technique. (
Patients were evaluated by US, CEUS (only the RFA group) and chest CT (annually), and clinical evaluation during the follow-up. In the TL group, patients were regularly followed every 6–12 months. In the RFA group, clinical follow-up was performed at 1, 3, 6, 12 months and every 6–12 months thereafter. At three or six months after RFA, to evaluate the ablation efficacy, CNB was performed of the central zone, the peripheral zone and the surrounding thyroid parenchyma of the ablated area (31). All the patients were advised to have levothyroxine after treatment to maintain thyrotropin levels between 0.5 and 2 mU/L (5).
End points and definitions
The primary outcome measures were local tumor progression, distant metastasis, recurrence-free survival (RFS), and delayed surgery. Local tumor progression was defined as (28): (a) persistently detected lesion at the ablated tumor confirmed by biopsy; (b) new recurrent PTMC that was separated from the treated tumor confirmed by biopsy; and (c) cervical LNM confirmed by biopsy. Distant metastasis detected by CT, positron emission tomography, or bone scan if there were suspicious symptoms. RFS was calculated from treatment initiation to tumor recurrence or the last date of follow-up date. Delayed surgery was defined if a patient in the RFA group underwent surgery due to tumor progression or anxiety during the follow-up period.
Secondary outcome measures were treatment variables (hospitalization, procedure time, estimated blood loss, and cost) and complications. Procedure time was defined from incision to closure time, not including anesthesia time. The cost of RFA included the preoperative examination, surgery, local anesthesia, and RF needle fees. The cost of TL included the preoperative examination, surgery, general anesthesia, and hospitalization (hospital bed, nursing, and postoperative medication fees). Complications were identified. Recurrent laryngeal nerve (RLN) injury was defined as impaired movement of one or both vocal cords on laryngoscopy, and permanent RLN injury was defined as an injury that did not recover within six months (32). Hypoparathyroidism was defined as a parathyroid hormone level <15 pg/mL 24 hours postoperatively, and permanent hypoparathyroidism was defined as no recovery within 6 months (32).
Statistical analyses
Normally distributed continuous variables are expressed as mean ± standard deviation and compared using the independent-sample t-test. Non-normally distributed continuous variables are presented as median with interquartile range (IQR) and compared using Mann–Whitney U test. Categorical variables were presented as numbers with percentages and compared using chi-square or Fisher's exact test. To control for inherent potential biases, 1:1 propensity score matching (PSM) was applied in the two groups based on age, sex, largest diameter, mean diameter, volume, location, follow-up period, and presence of chronic lymphocytic thyroiditis (CLT), which was confirmed by thyroid function test. PSM was performed by using the nearest-neighbor matching method with a caliper distance of 0.05 without replacement. Patient characteristics and outcomes were compared before and after matching. RFS rates were calculated using the Kaplan–Meier method and compared using the log-rank test. Univariable and multivariable analyses were performed using a Cox proportional hazard model to identify variables associated with recurrence. Statistical analyses were performed using SPSS statistical software (version 25.0) and R software version 3.6.2 (MatchIt packages, R Foundation for Statistical Computing). A two-sided p < 0.05 was considered as statistically significant.
Results
Patient characteristics
Baseline characteristics are presented in Table 1. In the unmatched group, patients in the RFA group have smaller tumor size (median [IQR], 65.4 [98.4] vs. 110.0 [142.4] mm3, p < 0.001) and shorter follow-up period (48.1 [18.4] vs. 48.9 [28.4] months, p = 0.026) than those in the TL group. After 1:1 PSM, there were 664 patients with similar features: RFA (n = 332) and TL groups (n = 332).
Baseline Characteristics of Patients Before and After Propensity Score Matching
Data are expressed as mean ± SD or median (IQR) or number of tumors (percentages) patients with percentages in parentheses for categorical variables.
CLT, chronic lymphocytic thyroiditis; IQR, interquartile range; PSM, propensity score matching; RFA, radiofrequency ablation; SD, standard deviation; TL, thyroid lobectomy.
Primary outcomes
Before PSM, the overall incidence of local tumor progression, LNM, recurrent PTMC, and persistent lesion was 2.7% (24/884), 0.8% (7/884), 1.8% (16/884), and 0.1% (1/884), respectively. The comparisons of local tumor progression are summarized in Table 2. No significant differences were found in the local tumor progression (9/460 [2.0%] vs. 15/424 [3.5%], p = 0.148), LNM (3/460 [0.7%] vs. 4/424 [0.9%], p = 0.914), recurrent PTMC (6/460 [1.3%] vs. 10/424 [2.4%], p = 0.240) and persistent lesion (0/460 [0%] vs. 1/424 [0.2%], p = 0.298) between the TL and RFA group. The RFS rates at 1 and 4 years were 99.1% and 98.0% in the TL group, and 99.3% and 96.9% in the RFA group (p = 0.174) (Fig. 3). During the follow-up, no distant metastasis was detected. No cancer-related death or other thyroid cancers were observed. None of the patient in the RFA group underwent delayed surgery.

RFS curves for RFA vs. TL in the treatment of low-risk PTMC before matching. RFS, recurrence-free survival.
The Comparison of Local Tumor Progression Between the Two Groups
Data are expressed as mean ± SD or median (IQR) or number of tumors (percentages).
LNM, lymph node metastasis; PTMC, papillary thyroid microcarcinoma.
In the TL group, six patients developed recurrent PTMCs, which were all located in the contralateral lobe at 16.0 ± 9.8 months after surgery with a mean volume of 119.3 ± 129.2 mm3. One patient received RFA and the tumor disappeared after 12 months. The other five patients underwent TT+CND; one of them had cervical LNM on surgical pathology. A total of three patients developed LNM at 16.0 ± 3.5 months after surgery with a mean volume of 324.1 ± 133.6 mm3. Two patients had a central LNM and underwent TT+CND. The other patient developed multiple central and lateral LNM and underwent TT with lateral neck compartmental LN dissection. In the RFA group, four patients developed LNM at 19.5 ± 5.7 months after treatment with a mean volume of 131.8 ± 44.4 mm3. Three were located in the lateral compartment and one in the central compartment. Ten patients developed recurrent PTMC at 27.6 ± 12.7 months with a mean volume of 54.6 ± 76.1 mm3. Seven of them were in the contralateral lobe and three were in the ipsilateral lobe. One persistent lesion was diagnosed by postablation CNB at six months after RFA. Of the 15 patients with local tumor progression, only 1 with recurrent PTMC chose AS, and the volume was stable during the follow-up. The other 14 patients received additional RFA, and 11 of the lesions disappeared. The remaining three lesions were negative on postablation CNB.
After PSM, there were no significant differences in the rate of local tumor progression (1.8% vs. 3.3%, p = 0.209), LNM (0.6% vs. 0.6%, p = 1.000), recurrent PTMC (1.2% vs. 2.4%, p = 0.244), and persistent lesion (0% vs. 0.3%, p = 0.317) between the TL and RFA group. The RFS rates at 1 and 4 years were 98.8% and 98.2% in the TL group and 99.1% and 97.0% in the RFA group, respectively, (p = 0.223) (Fig. 4). Cox regression analysis revealed that treatment modality was not significantly associated with recurrence after adjusting for age, sex, tumor size and CLT [hazard ratio = 1.888, CI: 0.643–5.542, p = 0.247] (Table 3).

RFS curves for RFA vs. TL in the treatment of low-risk PTMC after matching.
Univariate and Multivariate Analysis Evaluating the Risk Factors for Recurrence
CI, confidence intervals; HR, hazard ratio.
Secondary outcomes
A comparison of treatment variables and complications is present in Table 4. In the matched groups, patients in the TL group had a significantly longer procedure time (86.0 [37.0] vs. 3.4 [2.5] minutes, p < 0.001), more blood loss (20.0 [10.0] vs. 0 [0] mL, p < 0.001), longer hospitalization (7.0 [3.0] vs. 0 [0] days, p < 0.001), and higher cost ($2269.1 [943.4] vs. $2035.7 [254.0], p < 0.001) than those in the RFA group. None of the patients had complications after RFA. In contrast, the complication rate in the TL group was 4.5% (15/332) (p < 0.001). One patient had fever (0.3%), which resolved within 3 days after medication. Twelve patients (3.6%) had transient RLN injury and recovered within 1–3 months after treatment with dexamethasone. Two patients had transient hypoparathyroidism (0.6%), which resolved within 1–3 months after the administration of vitamin D or calcium. No patient developed permanent RLN injury or hypoparathyroidism.
The Comparison of Treatment Variables and Complications of the Two Groups
Data are expressed as mean ± SD or median (IQR) or number of tumors (percentages).
RLN, recurrent laryngeal nerve.
Other outcomes
In the unmatched TL group, the surgical pathology revealed that the incidence of occult PTMC, microscopic ETE, and gross ETE was 13.3% (61/460), 28.3% (130/460), and 0% (0/460), respectively. After PSM, the incidence of occult PTMC, microscopic ETE, and gross ETE was 11.1% (37/332), 27.1% (90/332), and 0% (0/332), respectively.
In the RFA group, 383 tumors disappeared completely during the follow-up (90.33%). The numbers of complete disappearance were 22 (5.19%), 81 (19.10%), 161 (37.97%), 49 (11.56%), 55 (12.97%), 13 (3.07%), and 2 (0.47%) at 3, 6, 12, 18, 24, 36, and 48 months after RFA, respectively (Fig. 5).
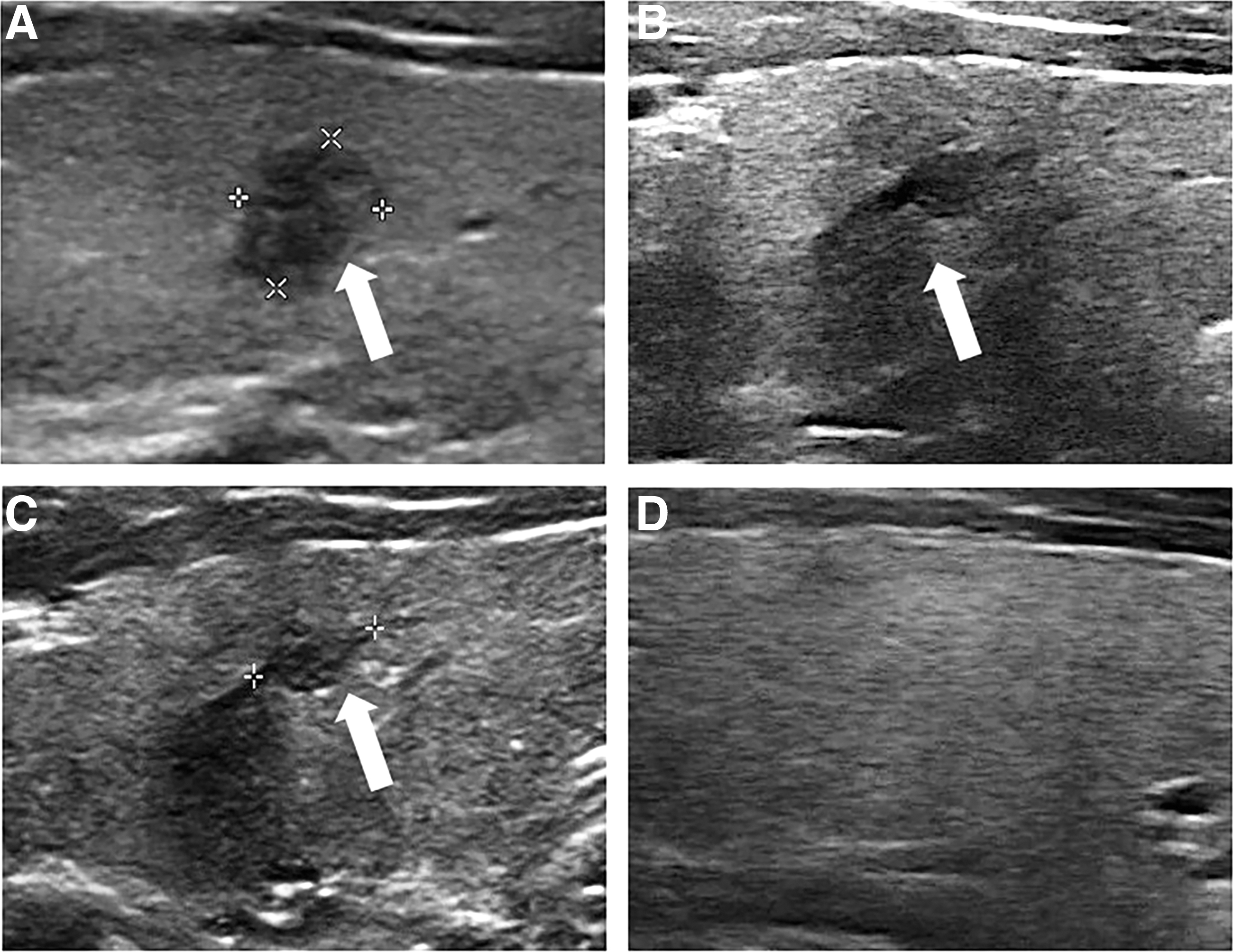
US image of a 40-year-old male with a low-risk PTMC.
Discussion
In this study, comparisons of local tumor progression and RFS in the PSM groups revealed comparable outcomes between RFA and TL for low-risk PTMC. Moreover, RFA was associated with shorter procedure time, lower cost, lower estimated blood loss, shorter hospitalization, and lower complication rates than those treated by TL. To the best of our knowledge, this is the largest study to compare the clinical outcomes of RFA and TL for low-risk PTMC using PSM.
The incidence of low-risk PTMC has grown rapidly (3,4). The current standard treatment for low-risk PTMC is surgery (5). AS is recommended as a conservative option for low-risk PTMC (5) and has favorable results (6 –8,33). A recent meta-analysis reported that during 5 years of AS, the pooled proportion of tumor size enlargement was 5.3% and the pooled proportion of LNM was 1.6% (7). However, patient preference and compliance were important elements in this strategy (34). Because of anxiety, most patients chose immediate surgery instead of AS (35). Anxiety was also the most common reason for the decision to perform delayed surgery during AS (8). Moreover, cultural factors, population mobility, medical liability concerns, and family support could also impact the implementation of AS for low-risk PTMC (9). For low-risk PTMC patients who refused surgery or AS, TA could be considered as effective and safe alternatives (19 –23). In some centers, TA was adopted as a standard alternative together with surgery or AS for patients with low-risk PTMC, and 84.6% of patients evaluated were suitable for this treatment (24). This indicated the potential impact of this technique for patients, which seemed to prefer a treatment over AS and favored a more minimally invasive approach compared with surgery (24). Because patients' perceptions and preferences for available treatments is becoming increasingly important in decision-making in oncology, reliable evidence-based comparison between different treatments for low-risk PTMC is crucial for appropriate clinical decision-making (24,36 –38). Only a few studies have demonstrated comparable outcomes in TA versus surgery for low-risk PTMC (25 –28). Li et al. (25) found that no recurrence in a comparison of 46 patients each who underwent MWA and surgery (9 patients, TT; 37 patients, TL) after 42-month follow-up. Li et al. (26) found no statistical differences in recurrent PTMC (2/168 [1.2%] vs. 1/143 [0.7%], p = 0.659), LNM (5/168 [3.0%] vs. 5/143 [3.5%], p = 0.795), and disease-free survival (95.8% vs. 95.5%, p = 0.974) between 168 patients who had MWA with 143 patients who had TL+CND at 2-year follow-up. Furthermore, Zhou et al. (27) reported that the local recurrence (3/45 [6.5%] vs. 2/36 [5.6%], p > 0.05) and 3-year RFS rate (93.3% vs. 97.2%, p = 0.822) were not significantly different between 45 patients treated with TL+CND and 36 patients who underwent LA. Zhang et al. (28) recently reviewed 94 patients who underwent RFA and 80 patients treated surgically (19 by TL, 39 by TL+CND, 8 by TT, and 14 by TT+CND) over 5-year follow-up and no significant differences in the rate of recurrent PTMC (1/94 [1.1%] vs. 1/80 [1.3%], p = 0.363) and LNM (0/94 [0%] vs. 1/80 [1.3%], p = 0.460) between RFA and surgery were observed. However, these studies were small cohorts with different surgical treatments, and none of them compared the clinical outcomes between TL and TA for low-risk PTMC. In this study, before PSM, patients in the RFA group had a smaller tumor size and shorter follow-up period than those in the TL group. To minimize the effect of potential confounding factors, the clinical variables were adjusted for by PSM. The results revealed that during the four-year follow-up, no significant differences in the local tumor progression and survival outcomes were found between the two groups. Treatment modality was also not associated with the recurrence of low-risk PMTC. The results in this study are consistent with those from previous studies (25 –28) and a recent meta-analysis (39). It indicates that RFA could be a promising alternative to TL for low-risk PTMC.
We found RFA had several advantages over TL. First, RFA led to shorter procedure time, smaller estimated blood loss, and shorter hospitalization, indicating a faster postoperative recovery after treatment. Second, compared with TL, patients undergoing RFA had a lower complication rate. Moreover, several methods, such as trans-isthmic approach, hydrodissection technique, and moving shot technique are also helpful in reducing the complications (39). Third, the RFA cost was significantly lower than that of TL, which is noteworthy considering the high prevalence of PTMC (39). Furthermore, none of the patients in the RFA group underwent delayed surgery because of anxiety. This was consistent with a recent meta-analysis, which reported that only 1.1% patients (5/470) with local tumor progression underwent delayed surgery after TA, with none undergoing delayed surgery because of anxiety (40). In contrast, the numbers of patients who underwent delayed surgery during AS because of anxiety other than size increase or LNM was 32–69% (7), suggesting that RFA may alleviate or even eliminate patient anxiety by treating the primary tumor.
RFA has some disadvantages as compared with TL. First, RFA cannot resolve occult PTMCs. However, for low-risk PTMC, the effect of occult lesions on overall survival was small (5). Second, RFA is inferior to TL in terms of tumors with ETE. Although microscopic ETE identified only on histological examination has no impact on mortality (41), the risk of recurrence of PTMC associated with microscopic ETE ranges from 3% to 9%, which with gross ETE ranges from 23–40% (5). Third, the possibility of persistent lesion is real (42,43), because US evaluation of the ablated area to exclude the presence of residual tumor is difficult. In this study, one tumor was diagnosed as a persistent lesion by postablation CNB, which was similar to the results in previous studies on RFA for recurrent tumors (44,45). Several strategies were used in this study to avoid incomplete ablation and tumor persistence, including an enlarged ablation area during the RFA procedure (19 –22, 28, 46 –50), CEUS evaluation immediately after RFA (20, 22, 28, 29, 46, 48 –51), and biopsy during the follow-up (20, 28, 29, 31, 48, 49). Because insufficient cellularity caused by tumor apoptosis and coagulative necrosis from TA could reduce the diagnostic accuracy of fine needle biopsy of the ablation area (52,53), CNB was performed in the three parts of the ablated tumor to confirm complete ablation after RFA, which have also been used for recurrent thyroid cancer and benign nodules (54 –56). Moreover, because the ablation procedure is operator dependent, it should be performed by high-volume physician in experienced treatment center to maximize the efficacy (13,40). Fourth, lack of histological final diagnosis was another disadvantage of RFA, and the risk of an aggressive histological variant could not be completely excluded.
According to the 2015 American Thyroid Association guideline, a sonographically suspicious subcentimeter thyroid nodule without evidence of ETE or suspicious LNM may be observed with close sonographic follow-up rather than pursuing immediate biopsy (5). However, a size <1 cm does not guarantee indolence, and cultural context, patient age, and preference may modify decision-making (5,9,57). Some patients with suspected subcentimeter nodules underwent biopsy and subsequent treatment even if the lesions were small. In this study, CNB was used for PTMC diagnosis before treatment instead of fine needle aspiration. Different from the developed countries, the use of fine needle aspiration was not yet widespread in China, and there were differences exist in the process of diagnosis and management of thyroid nodules in China and other countries. The application rate of fine needle aspiration was only 52% in tertiary hospital and 12.9% in the nontertiary hospital according to a nationwide questionnaire survey in 2019 (57). Compared with fine needle aspiration, CNB had a higher diagnostic accuracy, a lower nondiagnostic rate, and a lower rate of false-negative results to prevent further biopsy (53,58,59). Moreover, CNB was safe, well-tolerated, and associated with a low incidence of complications when performed by experienced operators (58).
This study has some limitations. First, this was a retrospective study. Although randomized clinical trials could yield the most powerful conclusions, they might be difficult to perform because of patient preference. Accordingly, in the absence of prospective or randomized clinical trials, this PSM analysis suggests comparable outcomes between RFA with TL for low-risk PTMC. Second, the follow-up duration was relatively short. Given the good prognosis of PTMC, a longer follow-up period is needed to confirm the results. Third, the sensitivity of imaging modalities to detect LNM was low, and the presences could not be completely excluded in either group. Fourth, some treatment variables, such as cost and hospitalization in Asian countries might be different from those in other countries. In China, most patients completed preoperative examinations after hospitalization because of the medical insurance, which took several days. Generally, they were discharged two to three days after the surgery. While this is not representative of perioperative surgical treatment in other countries, these practices may result in additional costs compared with RFA. Fifth, this study only compared the clinical outcomes between RFA and TL for low-risk PTMC, further studies comparing RFA, TL, and AS for low-risk PTMC are needed.
In conclusion, this large matched study showed comparable four-year clinical outcomes between RFA and TL for low-risk PTMC. As a minimally invasive modality, RFA may be a promising alternative to the existing management options for low-risk PTMC.
Footnotes
Authors' Contributions
Clinical studies, experimental studies/data analysis, and statistical analysis by L.Y. Literature research, study concepts, and design by M.Z. Article preparation by Q.S. Guarantor of integrity of the entire study, study concepts and design, and article editing by Y.L.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study is supported by Beijing Municipal Science & Technology Commission (No. Z181100001718017) and National Natural Science Foundation of China (No. 81771834).