
Abstract
Introduction:
Serum thyrotropin (TSH) receptor antibodies (TRAbs) are occasionally found in patients with amiodarone-induced thyrotoxicosis (AIT), and usually point to a diagnosis of type 1 AIT (AIT1) due to Graves' disease (GD). However, the TRAb role and function in AIT have not been clarified.
Methods:
A retrospective cohort study of 309 AIT patients followed at a single academic center over a 30-year period. AIT TRAb-positive patients (n = 21, 7% of all cases) constituted the study group; control groups consisted of type 2 AIT (AIT2) TRAb-negative patients (n = 233), and 100 non-AIT patients with GD. Clinical and biochemical data at diagnosis and during the course of disease were compared. Histological samples of patients who had total thyroidectomy were reviewed. Stored serum samples were used for a functional assay of TRAb class G immunoglobulins (IgGs) in Chinese hamster ovary (CHO) cells stably transfected with complementary DNA encoding for the TSH receptor.
Results:
TRAb-positive patients were grouped according to color flow Doppler sonography, radioactive iodine thyroid uptake, and duration of amiodarone therapy before thyrotoxicosis in type 1 (n = 9, 43%; TRAb1) or type 2 (n = 12, 57%; TRAb2) AIT. TRAb1 patients had clinical and biochemical features indistinguishable from GD controls, and were responsive to methimazole. Conversely, TRAb2 patients had clinical features similar to AIT2 controls, and were responsive to glucocorticoids, but not to methimazole. The CHO cell functional assay demonstrated that TRAb1 IgGs had a stimulatory effect on cyclic AMP production, which was absent in TRAb2 IgGs. Pathology in TRAb1 showed hyperplastic thyroid follicles and mild lymphocyte infiltration, reflecting thyroid stimulation. On the contrary, TRAb2 samples revealed follicle destruction, macrophage infiltration, and sometimes fibrosis, consistent with a destructive process.
Conclusions:
Almost 60% of TRAb-positive AIT patients had a destructive thyroiditis. TRAb-positive tests in AIT patients do thus not necessarily imply a diagnosis of GD and AIT1, and should be evaluated in the clinical and biochemical setting of each AIT patient and confirmed by measuring thyroid-stimulating immunoglobulins.
Introduction
Amiodarone is a widely used and very effective class III antiarrhythmic drug, which may, however, have multiple side effects, including thyroid dysfunction (1). Both amiodarone-induced hypothyroidism and amiodarone-induced thyrotoxicosis (AIT) may develop. There are two major types of AIT: type 1 AIT (AIT1), which is a form of iodine-induced hyperthyroidism usually developing in a gland with underlying functional autonomy (either nodular goiter or Graves' disease [GD]), and the more frequent type 2 AIT (AIT2), a destructive thyroiditis more often occurring in a normal thyroid (2). A correct diagnosis is mandatory, because thionamide antithyroid drugs (ATDs) are the treatment of choice for AIT1, while AIT2 is unresponsive to ATDs and is treated with glucocorticoids (3). However, indeterminate forms exist, in which both pathogenic mechanisms coexist, and diagnosis is not straightforward because diagnostic criteria are not entirely specific. For example, the presence of a small goiter and/or positive tests for antibodies to thyroglobulin (TgAb) or thyroperoxidase (TPOAb) does not rule out AIT2 (4). Refining criteria for the differential diagnosis between the AIT subtypes is thus key for an effective therapeutic strategy and for promptly restoring euthyroidism in patients whose cardiac function is often compromised (5 –7). Thyrotropin (TSH) receptor antibodies (TRAbs) are the cause of Graves' hyperthyroidism (8,9). Therefore, positive TRAb tests in patients with AIT usually point to a diagnosis of AIT1 (3). However, studies systematically analyzing the presence and function of TRAbs in the context of AIT are lacking.
The aim of our retrospective study was to analyze the clinical records of our large population of AIT patients gathered over a 30-year period, to assess TRAb prevalence, their possible pathogenic role, and therefore their usefulness in the diagnostic workup of AIT.
Materials and Methods
Study design
This was a retrospective cohort study of patients referred to the Endocrinology Unit of the University of Pisa for AIT over a 30-year period (January 1990–December 2019), with the primary goal of identifying patients with positive TRAb tests (Study Group). Two control groups were defined: (i) TRAb-negative AIT2 patients treated within the same time period; and (ii) one hundred consecutive patients referred for GD from August 2019 to December 2019. Clinical and biochemical data at diagnosis were collected. Some patients had total thyroidectomy for AIT (n = 49, six of whom were TRAb-positive) or GD (n = 19), and their histological samples were reviewed. Finally, for a subset of patients, serum samples collected at diagnosis and stored at −20°C for scientific purposes at our department were retrieved.
It is our usual practice to obtain written informed consent for the recording and use of anonymous data for research purposes during the first clinical visit at our clinic, and all the patients involved in the study had provided their consent. The study was approved by the Review Board of the Department of Clinical and Experimental Medicine of the University of Pisa.
Patients, diagnosis of AIT, and clinical management
Throughout the study period, 309 AIT patients had the appropriate complete clinical records for the purposes of this study. Of these, 21 patients (7%) with TRAb levels that were at least 1.5-fold higher than the upper normal limits for our laboratory were identified. They were labeled in chronological order, according to the date of referral (PT1 to PT21). Among the remaining patients, 233 TRAb-negative AIT2 patients constituted the AIT2 control group. One hundred consecutive GD patients made up the non-AIT control group.
AIT was diagnosed on clinical grounds (signs and symptoms of thyrotoxicosis) and biochemical data (increased serum thyroid hormone concentrations, reduced/undetectable serum TSH concentration, increased urinary iodine excretion [UIE] on amiodarone therapy) (3,10). After diagnosis of AIT types, ATD treatment for AIT1 or glucocorticoid therapy for AIT2 was initiated (3). Briefly, preexisting thyroid disease (e.g., diffuse or multinodular goiter), thyroid vascularity at color flow Doppler sonography (CFDS), thyroidal radioactive iodine uptake (RAIU), and duration of amiodarone therapy before thyrotoxicosis were used to differentiate between AIT1 and AIT2, as previously reported (2,10,11). AIT patients treated surgically had a total thyroidectomy either to treat thyrotoxicosis or, after restoration of euthyroidism, to treat the underlying thyroid disease (5). GD patients were treated according to currently available guidelines (12,13).
Thyroid evaluation
Serum TRAbs were measured at our university hospital laboratory with a second-generation radioimmunoassay up to 2014 (TRAK TRAb, BRAHMS, Berlin, Germany), and with a third-generation enzyme-linked immunosorbent assay (ELISA) (ElisaRSR TRAb; RSR Limited, Cardiff, UK) thereafter. Both kits measured thyrotropin binding inhibitory immunoglobulins (TBII), thus not distinguishing between stimulatory and nonstimulatory antibodies. Sensitivity and specificity reported by the manufacturer for the ElisaRSR TRAb assay are 95% and 100%, respectively. The same data were unavailable for the TRAK TRAb assay, due to the manufacturer's refusal to provide such information when contacted for this specific purpose. It is the practice of our laboratory to test for discrepancies in the diagnostic accuracy for every assay to be replaced: the two TRAb assays demonstrated a similar diagnostic accuracy (unpublished internal data available upon request), in line with the data published by other authors (14,15). The diagnostic cutoffs provided by the laboratory were <2 U/L with the former assay and <2.5 U/L with the latter assay. Patients were considered to be TRAb-positive if they had serum TRAb concentrations repeatedly (i.e., at least twice during the course of the disease) higher than 1.5 times the diagnostic cutoff provided by the laboratory. Recent exposure to biotin was investigated in all patients after the first reports of misdiagnosis of GD (16), and all the clinical charts were checked for previous biotin assumption.
Details about the commercial kits used for free thyroxine (fT4), free triiodothyronine (fT3), TSH, TgAb, and TPOAb during the 30-year period of the study are available upon request. Normal values in our laboratory are as follows: fT4, 7–17 pg/mL; fT3, 2.7–4.5 pg/mL; TSH, 0.4–4.0 mU/L; TgAb <30 U/mL; and TPOAb <10 U/mL. UIE was measured in random morning urinary samples; median UIE in our area is 110 μg/L. Thyroid volume was measured by ultrasonography and calculated by the ellipsoid model (width × length × thickness × 0.52 for each lobe). CFDS was performed as previously reported (11), which identified a qualitative sonographic pattern ranging from pattern 0 (i.e., absent vascularity or minimal intrathyroidal spots) to pattern III (diffuse hypervascularity) (17). Thyroidal RAIU was measured 3 and 24 hours after the administration of a tracer dose (50 μCi) of radioactive iodine (131I). The normal 3- and 24-hour RAIU values in our area are 10–20% and 30–45%, respectively. Patients with GD were submitted to joint endocrine/ophthalmic evaluation to assess the presence, activity, and severity of Graves' orbitopathy (GO) according to standardized criteria (18). For the purposes of this study, we used the Clinical Activity Score (19) to assess GO activity.
Functional TRAb assay
A functional TRAb assay was performed using an in-house assay. Class G immunoglobulins (IgGs) were extracted from available sera of TRAb-positive AIT patients and used for a cyclic AMP (cAMP) production assay. IgGs were prepared using a commercial kit according to the manufacturer's instructions (Mab Trap G II; Pharmacia Biotech). IgGs prepared from a healthy subject were used as the control.
Chinese hamster ovary cells, stably transfected with the human TSH receptor (JPO9), were used (20). JPO9 cell lines were cultured in Petri dishes in Roswell Park Memorial Institute 1640 medium (Sigma-Aldrich).
Cells were seeded at a concentration of 25,000 cells/well in 96-well plates with medium and used for the assay the following day. Cells were washed with Hanks' balanced salt solution and stimulated with 1 mU/mL bovine TSH (bTSH; Sigma-Aldrich), or IgGs (alone or with bTSH) at a concentration of 1 mg/mL. A commercial cAMP competitive ELISA Kit (Thermo Fisher Scientific) was used to measure extracellular cAMP in the medium collected from each well after a 1-hour incubation.
All experiments were performed in triplicate, and the results (pmol/well) were expressed as the mean value. To evaluate the effects of IgGs, an index of inhibition of TSH-dependent cAMP production was calculated according to the following formula (21):

Pathology
Six out of 21 TRAb-positive AIT patients underwent total thyroidectomy. Their histological samples were analyzed by two expert pathologists, who were blinded to the clinical features of the patients, for five different items: (i) hyperplasia, that is, crowding of the thyroid epithelium with the formation of pseudopapillary structures (0 absent, 1 present); (ii) lymphocytic infiltration, varying from scattered lymphocytes within stroma surrounding follicles to prominent lymphoid aggregates with germinal centers (0 absent, 1 mild, 2 significant); (iii) macrophage infiltration, usually associated with follicular disruption with histiocytes infiltrating the follicular epithelium or scattered within the colloid (0 absent, 1 mild, 2 significant); (iv) fibrosis, that is, acellular, keloid-like with irregular broad bands intercepting the parenchyma (0 absent, 1 mild, 2 significant); and (v) thyroid follicle disruption, evident when the contour of the thyroid follicle appears interrupted and associated with macrophagic infiltrate (0 absent, 1 mild, 2 significant) (22,23).
Statistical analyses
Data were expressed as median and interquartile range or mean for continuous variables, and as frequency and percentage for categorical variables. Groups were compared using the Mann–Whitney test for continuous variables and by the chi-squared test for categorical variables. The paired t-test was used to evaluate variations in thyroid hormone concentrations following medical therapies. A p-value <0.05 was considered statistically significant. All computations were performed using SPSS v.25 (SPSS, Chicago, IL).
Results
Identification of AIT patients with TRAbs
Serum TRAbs were detected in a subset of AIT patients (21/309, 6.8%): 15 patients (71.4%) were diagnosed before 2014, with the TRAK TRAb assay, and the remaining 6 patients (28.6%) thereafter with the ElisaRSR TRAb assay. The proportion of TRAb-positive AIT patients did not change after introducing the new TRAb assay (7.4% vs. 6.5%, respectively). The TRAb titer was between 1- and 1.5-fold the upper normal limits only in two AIT patients. This finding was not confirmed at subsequent examinations, and hence, these patients were not included in the study population. No patient was exposed to biotin.
The clinical and biochemical features of TRAb-positive AIT patients are shown in Table 1. Nine out of 21 TRAb-positive AIT patients (42.9%) had clinical and biochemical features of type 1 AIT and were indicated as TRAb1. The remaining 12 patients (57.1%) had typical AIT2 features and were indicated as TRAb2. While no difference was found in the prevalence or serum levels of TgAb, TRAb1 patients had a markedly higher serum TPOAb concentration than TRAb2 patients (Tables 1 and 2). GO was present in 3 out of 21 TRAb-positive AIT patients (2 with mild GO and 1 with moderate GO), all belonging to the TRAb1 subgroup.
Comparisons of Various Variables Between the Different Groups
The subset of AIT patients presenting TRAbs with clinical and biochemical features typical of GD is identified as the TRAb1 group. The subset of AIT patients presenting TRAbs without the clinical and biochemical features typical of GD is identified as the TRAb2 group. The control group of patients affected by TRAb-negative AIT2 is identified as the AIT2 group. The control group of patients affected by GD is identified as the GD group. Graves' orbitopathy and CAS were not evaluated in the setting of AIT2.
Baseline Clinical and Biochemical Features of the Study Group of Thyrotropin-Receptor Antibody-Positive Patients with Amiodarone-Induced Thyrotoxicosis and Control Groups
The whole study population includes patients affected by AIT who present serum TRAb above the upper limit of normality. The subset of AIT patients presenting TRAbs with clinical and biochemical features typical of GD is identified as the TRAb1 group. The subset of AIT patients presenting TRAb without the clinical and biochemical features typical of GD is identified as the TRAb2 group. The control group of patients affected by TRAb-negative AIT2 is identified as the AIT2 group. The control group of patients affected by GD is identified as the GD group. Data are expressed as number (%) for categorical variables, and as median (IQR) for continuous variables. “p” refers to the comparison between TRAb1 and TRAb2 patients. To convert pg/mL to pmol/L multiply by 1.54 (fT3) or by 1.29 (fT4).
AIT, amiodarone-induced thyrotoxicosis; AIT2, type 2 AIT; BMI, body mass index; CAS, Clinical Activity Score; CFDS, color flow Doppler sonography; fT3, free triiodothyronine; fT4, free thyroxine; GD, Graves' disease; RAIU, radioactive iodine uptake; TgAb, thyroglobulin antibodies; TgAb+ patients, patients with detectable TgAb concentrations; TgAb+ and TPOAb+ patients, patients with detectable TgAb and TPOAb concentrations; TPOAb, thyroperoxidase antibodies; TPOAb+ patients, patients with detectable TPOAb concentrations; TRAb, TSH receptor antibodies; TRAb1, type 1 TRAb; TRAb2, type 2 TRAb; TSH, thyrotropin; UIE, urinary iodine excretion.
Comparison of TRAb-positive AIT patients with the control groups
As shown in Tables 1 and 2, TRAb-positive AIT patients were older and more frequently male than the GD control group and, as expected, had higher UIE levels. While features of TRAb1 patients were very similar to those of the GD controls, except for a lower serum fT3 concentration and RAIU values, TRAb2 patients had higher serum fT4 concentrations and fT4/fT3 ratio, lower prevalence of TPOAb, lower RAIU values, lower thyroid volume, and markedly different CFDS patterns compared with GD controls.
Compared with TRAb-negative AIT2 patients, TRAb1 AIT patients had higher RAIU values, CFDS pattern, TgAb and TPOAb prevalence and concentration, and a shorter exposure to amiodarone (Table 2) (p = 0.001). Conversely, TRAb2 patients were similar to TRAb-negative AIT2, with the exception of a higher prevalence and concentration of TgAb and TPOAb.
Management of TRAb-positive AIT patients and restoration of euthyroidism
All TRAb1 AIT patients were initially treated with ATDs (methimazole, starting daily dose of 10–40 mg, based on severity of thyrotoxicosis), with restoration of euthyroidism after a median of 38 days (range, 28–132 days). No patient belonging to this study population received perchlorate. While one TRAb1 patient remained in long-term remission after a 16-month course of ATDs, seven patients subsequently required a definitive therapy for thyrotoxicosis (five 131I, and two total thyroidectomy), One TRAb1 patient died during ATD treatment due to acute myocardial infarction.
Six out of 12 TRAb2 AIT patients were given ATDs before referral to our center, with no significant effect on serum thyroid hormone concentrations after a median time of 43 days (range, 22–76 days). Conversely, glucocorticoids restored euthyroidism in all TRAb2 patients, except for three patients who were referred for thyroidectomy while still thyrotoxic due to sudden decompensation of cardiac function. Combination therapies (i.e., the association between glucocorticoids and ATDs), used in three TRAb2 patients, provided no benefit in the duration of exposure to thyrotoxicosis compared with glucocorticoids alone (p = 0.275). Four out of 12 TRAb2 patients underwent total thyroidectomy.
Data on serum TRAb concentrations after restoration of euthyroidism were available in 13 patients (5 TRAb1, and 8 TRAb2). All patients (n = 6) referred for total thyroidectomy had undetectable serum TRAb concentrations: after 10 and 24 months, in two TRAb1 patients, and after a median of 8 months, IQR 4.8–12.8 in four TRAb2 patients, respectively. Three TRAb1 patients were treated with 131I therapy and developed permanent hypothyroidism: TRAbs were undetectable in two and persistently high in one patient (>5 U/L for 5 years). The remaining four TRAb2 AIT patients had undetectable TRAbs after a median of 13 months (IQR 9.8–17) after restoration of euthyroidism with glucocorticoid treatment.
The TRAb functional assay
Sera from six TRAb-positive patients were prepared for the cAMP production assay, one from the TRAb1 group (PT21), and five from the TRAb2 group (PT16–20), as shown in Figure 1. When cells were exposed to PT21 IgGs, there was a threefold increase in cAMP production with respect to basal levels (p = 0.0008), suggesting a stimulatory activity. Conversely, TRAb2 IgGs led to no significant increase in cAMP production. Simultaneous exposure to TRAb2 IgGs and bTSH led to an increase in cAMP production in 4 patients, suggesting a neutral activity, whereas PT16 IgGs incubated with bTSH had a 94% cAMP decrease compared with stimulation with bTSH or with normal IgG (p = 0.002).
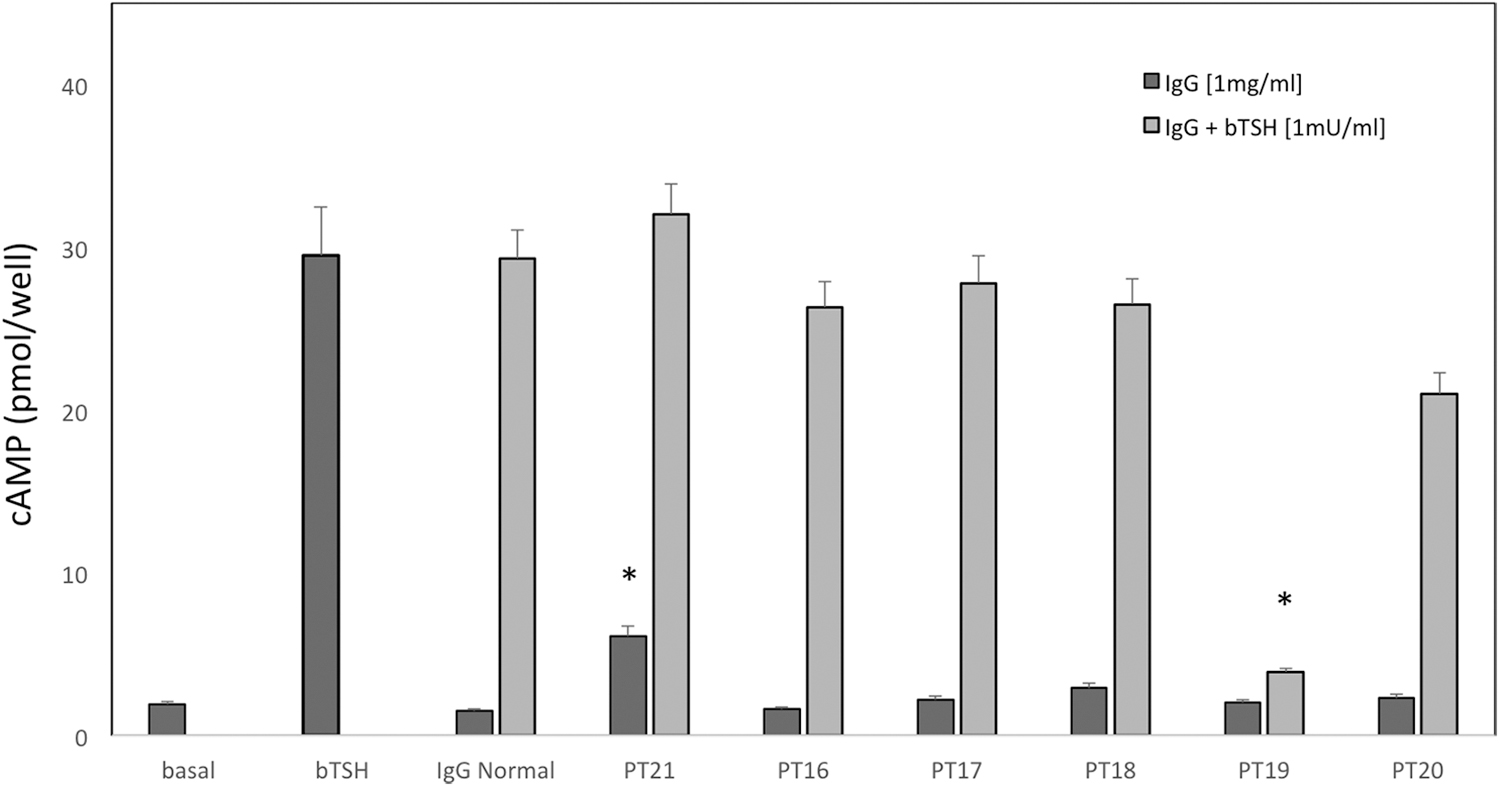
Functional assays. The IgGs were incubated at 1 mg/mL in the absence and presence of bTSH (1 mU/mL). Extracellular cAMP was measured in the medium collected from each well after a 1-hour incubation and the concentrations are expressed as pmol/well. Patients were labeled in chronological order. An IgG from a healthy subject was used as control (labeled as “IgG normal”). Results are expressed in pmol/well. Mean values ± SEM are shown. *Indicates statistical significance (p < 0.05), with a p-value of 0.0008 for PT21 cAMP rise following exposure to IgGs alone, and a p-value of 0.002 for PT19 cAMP decrease following exposure to IgGs and bTSH, as indicated in the text. bTSH, bovine TSH; cAMP, cyclic AMP; IgGs, class G immunoglobulins; SEM, standard error of the mean.
Pathology
In TRAb1 patients, hyperplastic thyroid follicles and mild lymphocytic infiltration were observed, whereas in TRAb2 patients the main features were follicle destruction and macrophage infiltration (Fig. 2, Table 3). Lymphocytic infiltration was also found in two out of four TRAb2 AIT patients, and was associated with the presence of detectable TPOAb and TgAb.
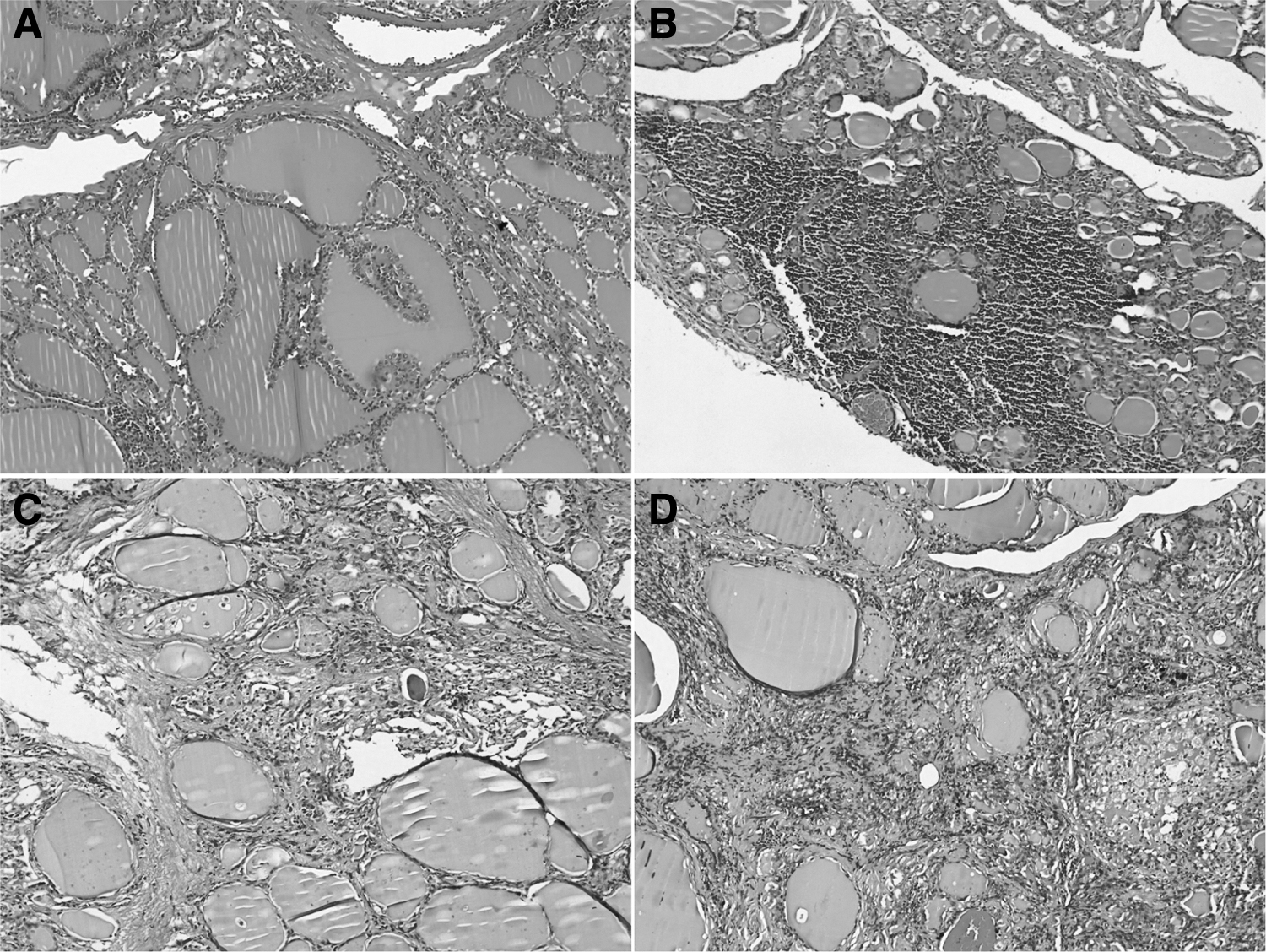
Representative histopathological images from surgical specimens of AIT patients who presented with elevated TRAb concentrations (H&E staining, original magnification × 10). (
Pathological Features of Thyrotropin-Receptor Antibody-Positive Amiodarone-Induced Thyrotoxicosis Patients Who Had Total Thyroidectomy
The TRAb groups were defined as reported in the text. Patients were labeled in chronological order. Hyperplasia was graded as absent (0) or present (1). Lymphocytic infiltration, macrophage infiltration, fibrosis, and thyroid follicle destruction were graded as absent (0), mild (1), and significant (2). See text for details.
Discussion
The effects of the iodine-rich drug, amiodarone, on thyroid autoimmunity are conflicting. Iodine can induce autoimmunity in animal models (24), and rapid iodine repletion may transiently increase the occurrence of GD (8). Excess iodine released from amiodarone might thus be involved in the pathogenesis of thyroid autoimmunity in vivo (1), at least by triggering organ-specific autoimmunity in genetically susceptible individuals (25). Moreover, the toxic (cytolytic) effects of amiodarone (or its metabolite, desethylamiodarone, or iodine itself) on the thyroid (26) might cause the transient release of thyroid autoantigens, thus triggering autoimmune reactions (25,27). However, real-life data from amiodarone-treated patients are conflicting, with only some studies showing an increased incidence of thyroid autoimmune phenomena in AIT-treated patients (27,28). The appearance of thyroid autoantibodies, including TRAb, following a thyroid destructive process, such as subacute (29) and postpartum thyroiditis (30,31), or radioiodine therapy (32,33) is well-known. Interestingly, a previous study reported the appearance of nonstimulatory TRAbs in GD patients who originally presented with only stimulatory TRAbs following radioiodine treatment (34). The appearance of thyroid autoantibodies following a destructive process, including AIT2, could be due to the damage-induced exposure of thyroid autoantigens, which can be implicated in the triggering of autoimmune reactions, at least in predisposed individuals (25).
TRAbs are the cause of hyperthyroidism in GD, because they bind to and stimulate the TSH receptor, thereby inducing excess and uncontrolled thyroid hormone synthesis and secretion (8,9). TRAbs are also associated with GO (35,36). However, nonstimulatory (neutral/blocking) TRAbs have also been detected both in patients with GD and with other thyroid autoimmune disorders (37 –40). The association between AIT and GD seems infrequent (41,42), but has not been systematically evaluated.
In our large series, TRAbs were identified in 6.8% of AIT patients over a 30-year period. The association of TRAb with AIT is thus uncommon. However, the risk of misinterpretation of positive TRAb tests in this clinical setting should not be overlooked because it is potentially detrimental for patients with underlying cardiac compromise. In fact, half of TRAb-positive AIT2 patients were initially treated with ATDs alone, which as expected (3) had no effect on thyrotoxicosis, thus delaying the prompt restoration of euthyroidism, which is a fundamental goal in such patients.
TRAb-positive AIT patients were heterogeneous, and the majority (57.1%) did not have features compatible with GD, but rather with AIT2. Therefore, positive TRAb tests in the AIT setting should not per se be considered sufficient to differentiate AIT types. Compared with control GD patients, TRAb-positive AIT patients differed in age and sex distribution, in keeping with the notion that GD is more frequent in women and in young adults (8), while AIT is more prevalent in men and in older age groups (3). However, while in the elderly GD is often milder with fewer symptoms (43,44), the clinical and biochemical features of TRAb1 patients were similar to those of the younger GD control group, with the exception of lower RAIU and fT3 values. These differences are related to the inhibitory effects of amiodarone (or iodine load) on RAIU and the peripheral deiodination of T4 to T3, respectively (2). At variance, TRAb2 patients differed considerably from GD controls in terms of the higher serum fT4 levels and other biochemical and imaging features. Compared with TRAb-negative AIT patients, TRAb1 patients had substantially different features from AIT2 controls, while those of TRAb2 were very similar to those of the AIT control group, with the exception of a higher prevalence of thyroid autoimmune phenomena. Only a minority (14.3%) of TRAb-positive AIT patients had GO, and were invariably included in the TRAb1 subset.
TRAb1 patients developed AIT following a shorter exposure to amiodarone compared with TRAb2. While this result is in line with a previous study that identified a shorter exposure to amiodarone for AIT1 compared with AIT2 patients (45), it is not possible to ascertain whether this time difference was due to a preexisting subclinical GD, because thyroid function tests were not carried out before starting amiodarone therapy.
The results of the pathology and the functional assay underscored the clinical differences between TRAb1 and TRAb2. Although the small number of histological samples available prevents unequivocal conclusions from being drawn, our results suggest that such conditions are underpinned by different pathological phenomena: TRAb1 patients presented typical features of GD (i.e., follicle hyperplasia and lymphocyte infiltration), whereas TRAb2 patients showed follicle destruction without hyperplasia, macrophage infiltration, and fibrosis, which are typical of destructive thyroiditis (22,23,46). Similarly, the functional assay revealed that only TRAb1 IgGs had a stimulatory effect on the TSH receptor, in line with a diagnosis of GD, whereas TRAb2 IgGs failed to stimulate cAMP production, in line with a previous report (41). Thus, in TRAb2 patients, TRAbs, in line with their nonstimulatory features, do not play any pathogenic role in the occurrence of thyrotoxicosis, which is the result of a thyroid-destructive process.
However, the detection of TRAbs does not necessarily mean that there are immunoglobulins harboring a stimulatory activity, even outside the AIT setting. The commercially available assays used for TRAbs can be divided between those that detect the inhibition of binding to the TSH receptor (TBII), such as those used in our study, and those that detect the stimulatory activity on the TSH receptor (thyroid stimulating immunoglobulins [TSI]) (47,48). While all the AIT patients in our study population were found to be TRAb-positive when assayed with the TBII kits, it is possible that the TRAb2 patients would likely have been TRAb-negative if assayed with kits that detect only TSI. Although additional studies are necessary, these findings suggest that the different assays used for detecting TRAbs may provide different information, which may significantly impact the workup of AIT patients.
Finally, the fact that TRAb1 patients were responsive to ATDs, whereas TRAb2 patients were responsive to glucocorticoids, and that empirical combination therapy (ATDs + glucocorticoids) failed to provide an advantage over glucocorticoid therapy alone, for TRAb-negative AIT2 patients, lends further support to the results of the clinical trials on the treatment of AIT2 (49,50).
The main limitation of the present study is the relatively small number of TRAb-positive AIT patients. However, given the large number of AIT patients initially screened for TRAb positivity, this reflects the low prevalence of TRAb positivity in AIT.
In conclusion, finding TRAbs in AIT patients is relatively rare, but it should not be overlooked, because it may lead to misclassification of AIT and inappropriate treatments, delaying the prompt restoration of euthyroidism required in these patients. In the diagnostic workup, the use of TSI assays may be preferable to the use of TBII assays, since only the former is expected to identify pathogenic TRAbs. In fact, TRAbs may be either stimulatory or nonstimulatory, and only stimulatory TRAbs define a form of AIT1 substantially superimposable to GD. On the contrary, the presence of nonstimulatory TRAbs does not change the best therapeutic approach to AIT2 represented by glucocorticoids.
Footnotes
Authors' Contributions
D.C. was involved in the direct care of the patient, design of the study and data collection, statistical analysis, writing and reviewing of the article, and the approval of its final version. G.D.M., E.F., A.M., P.A., and M.T. were involved in the design of the study, carrying out the laboratory experiments, data collection, writing and reviewing of the article, and the approval of its final version. L.T. and F.B. were responsible for the pathology revision, data collection, writing and reviewing of the article, and the approval of its final version. A.M.D.C., G.C., C.U., G.M., and L.M. were involved in the direct care of the patient, data collection, writing and reviewing of the article, and the approval of its final version. L.B. and F.B. were involved in the direct care of the patient, design of the study, writing and reviewing of the article, and the approval of its final version.
Author Disclosure Statement
All the authors declare no competing financial interests and no conflicts to disclose.
Funding Information
The authors received no specific funding for this work.