
Abstract
Background:
Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) reclassification has significantly influenced the field of thyroidology. However, the extent of this impact depends upon the incidence of NIFTP in a given population. In this meta-analysis, we aimed to obtain robust information about the actual incidence of NIFTP worldwide by reviewing the published data.
Methods:
Comprehensive literature search was performed using electronic databases of PubMed and Web of Science over a five-year period (January 1, 2016, to January 30, 2021). The incidence of NIFTP was calculated by dividing the number of NIFTPs by the number of papillary thyroid carcinomas (PTCs). Meta-analysis of proportion and their 95% confidence interval [CI] were pooled using the random-effect model. Heterogeneity across the included studies was assessed using I 2 statistics. Egger's regression test and funnel plot of estimates were used to evaluate the publication bias. p-Value <0.05 was considered significant.
Results:
From 505 publications, we included 50 studies, all retrospective, with 100,780 PTCs and 3990 NIFTP from 92 institutions worldwide. The overall incidence of NIFTP was 6.0% [CI 4.4–8.2] among PTCs or thyroid malignancies with a high level of heterogeneity among the included studies (I 2 = 98.6%). NIFTP incidence was largely similar in North America and Europe (9.3% vs. 9.6%), with a significantly lower overall rate in Asia (2.1%). There was a significant decline in the reported incidence of NIFTP in non-Asian studies published after 2017 (p = 0.002). On applying our data on global thyroid cancer statistics, this reclassification would affect ∼30,881 patients annually, with a lower impact in Asia compared with North America and Europe.
Conclusions:
This comprehensive meta-analysis confirms that the worldwide NIFTP incidence is much lower than estimated initially. The NIFTP rates are significantly lower in Asian compared with North American and European countries. Apart from geography, NIFTP rates are significantly influenced by the nature of study, type of database used for sample collection, and the diagnostic criteria used. Introduction of NIFTP may potentially spare over 30,000 patients worldwide annually from clinical and psychological consequences of a thyroid cancer diagnosis.
Introduction
The incidence of thyroid cancer has increased threefold during the past 30 years, with papillary thyroid carcinoma (PTC) accounting almost entirely for this increase (1). Despite this significant rise, the disease-specific mortality has remained stable, leading to the speculation of the indolent nature of many of these tumors, especially the noninvasive encapsulated follicular variant of papillary thyroid carcinoma (EFV-PTC) (2,3). In 2016, a working group of the Endocrine Pathology Society critically re-examined EFV-PTC and later reclassified the noninvasive subtype of EFV-PTC as noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) (2). This reclassification was suggested with the primary aim of avoiding the term carcinoma, and the consequent risk of overtreatment for noninvasive tumors that have a benign clinical behavior and are known to have a very low recurrence rate (<1%) (2).
After the latest revision of diagnostic criteria for thyroid tumors in 2018, NIFTP is now defined as an encapsulated or well-demarcated noninvasive neoplasm with a follicular growth pattern, papillary-like nuclear features along with the absence of well-formed papillae or psammoma bodies, without typical findings of the aggressive subtypes of PTC or poorly differentiated carcinoma and lacking BRAF or other high-risk mutations (TP53, TERT promoter) (2,4,5). NIFTP has also been recently introduced in a “borderline” tumor group, along with follicular tumor of uncertain malignant potential (UMP) and well-differentiated tumor of UMP, in the 2017 World Health Organization (WHO) classification of tumors of endocrine organs, recognizing its extremely low risk and standardizing a classification worldwide (6).
The year 2021 marks the fifth anniversary of NIFTP and this new entity still attracts considerable interest. Labeling NIFTP as a nonmalignant neoplasm has not only influenced the patient's psychology in a positive manner (2,7) but has had a significant impact on medical professionals related to different expertise in the field of endocrine cancers. New treatment and management guidelines have been developed by thyroidologists and endocrine surgeons for decision-making in patients in thyroid nodules (8,9). NIFTP reclassification has also been acclaimed as a “practice changer” in endocrine pathology (7). New histological criteria and sampling protocols have been introduced for pathological evaluation of surgical samples (10,11), cytomorphological features have been redefined (12), and new recommendations related to the role of molecular pathology have been developed (5). Altogether, the health care system has been substantially relieved of the financial burden (7,13). Finally, it has also influenced the epidemiologists and medical statisticians by changing the output and statistics of thyroid cancers.
Apparently, the extent of all the changes related to NIFTP reclassification depends on the incidence of NIFTP in a certain population (8). Nikiforov et al. documented an NIFTP rate of 18.6% in their seminal article, which was immediately followed by several other studies from America and European countries suggesting similar rates, ranging from 15% to 28% (2,14 –17).
Since that time, additional studies from all around the world have been published, which allowed us to initiate a meta-analysis on a worldwide scale. Hence, in this context, the focus of this study was to obtain more robust information about the true incidence of NIFTP worldwide by reviewing the published data and conducting a meta-analysis.
Materials and Methods
Search strategy
The meta-analysis was done using “Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guideline” (18), and a comprehensive literature search was conducted. Databases of PubMed and Web of Science were searched and information was collected from the year of NIFTP inception (January 1, 2016) till January 31, 2021. The search terminologies were “(NIFTP OR non-invasive follicular OR noninvasive follicular) AND thyroid.” In addition, a manual search was performed by reviewing citations within the included publications and related references presented in PubMed.
Study selection
All the relevant results were imported to Endnote (Clarivate Analytics, Philadelphia, PA) and duplicate articles were deleted. Two researchers independently reviewed titles and abstracts of the retrieved articles, applying the selection criteria. Studies are included if they satisfied all of the following criteria: (i) studies on NIFTP and (ii) studies providing the incidence of NIFTP OR studies providing the number of NIFTPs, PTCs, and/or thyroid cancers. Studies were excluded if they were (i) case reports/reviews; (ii) focusing on a specific group of thyroid nodules (i.e., indeterminate nodules and pediatric nodules); (iii) not providing or not able to calculate incidence of NIFTP; (iv) theses, books, or conference proceedings; and (v) duplicate studies. Discrepancies between two reviewers were solved by on-site discussion and consensus.
Data extraction
Two reviewers read the full-text of all relevant articles and extracted the information independently, into a standardized worksheet. The following data were extracted from the included studies: year of publication, authors, institution, country, study period, source of NIFTP search (surgical pathology vs. cytology database), study design (retrospective vs. prospective), diagnostic criteria for NIFTP (year 2016 vs. 2018), number of thyroid cancers, number of PTCs, number of follicular variant (FV)-PTCs, and number of NIFTPs. For studies in which the number of NIFTPs was missing and the authors only provided the change in risk of malignancy of cytological categories, NIFTP number was estimated based on the reduction of malignancy risk and the total number of surgically treated cases. Data were cross-checked, and any discrepancies were discussed and mutually solved.
Data analysis
The incidence of NIFTP was calculated by dividing the number of NIFTPs with the number of PTCs. In studies with missing data on PTC cases, the number of thyroid cancer cases was used instead of the number of PTCs, since PTC accounts for the majority of thyroid cancers (19). To avoid overlapping data from the same institution, we only included one study with the highest number of NIFTP cases. For multicenter studies with potentially duplicating data, if those studies provided data for individual institution, we removed data of the suspected institutions and retained the other institutions. Otherwise, all such studies were excluded to avoid selection bias. We used the Comprehensive Meta-Analysis (Englewood, NJ) and JAMOVI for meta-analyses. Meta-analysis of proportion and their 95% confidence interval [CI] were pooled using the random-effect model. Subgroup analysis was also conducted for continents, countries, years of publication, and source databases. To assess heterogeneity across the included studies, the I 2 statistics was utilized, which measures the proportion of variation among the studies (20). We used the Egger's regression test and funnel plot of estimates to evaluate the publication bias. If p-value was <0.05, there was a presence of significant publication bias.
Results
Characteristics of included studies
A total of 505 articles were available for initial title and abstract screening, of which 83 studies were included for full-text reading (Fig. 1). After reading the full-text of these articles, we further excluded 33 of them, and finally, 50 studies qualified for meta-analysis (2,14,16,17,19,21 –65). Table 1 shows all the relevant details related to studies included in this meta-analysis. All included studies were retrospective cohort studies with study duration ranging from 1 to 21 years, with almost half (48%; n = 24) being published in 2017–2018. The highest number of publications was from the North American continent (n = 19) followed by Asia (n = 16) and Europe (n = 12). Altogether, patients were recruited from more than 92 institutions worldwide. The number of participant institutions from Canada and Denmark could not be determined (47,61) since these were population registry-based studies. There were four multi-institutional reports, two from Asian countries (22,43) and two involving American and European institutions (2,44).

Flowchart depicting study selection method for meta-analysis.
Studies Included in Meta-Analysis (Sorted Chronologically)
Number of PTCs was not provided in these studies and we used the number of thyroid cancers instead.
Cyto, cytology; FV, follicular variant; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; n.s., not specified; PTC, papillary thyroid carcinoma; surg path, surgical pathology.
Incidence of NIFTP and subgroup analysis
A total of 100,780 PTC cases from 50 studies and more than 92 institutions worldwide were included for this meta-analysis. Geographically, 61.5% of these patients (n = 61,649) were from the Asian continent alone, with American and European continents constituting 19.8% and 18.9% patients, respectively. Eight independent studies from Korea, altogether, contributed to the highest number of cases subjected to evaluation of diagnosis from a single country followed by China, the United States, and Japan (Fig. 2). The characteristics of all included studies are described in Table 1.
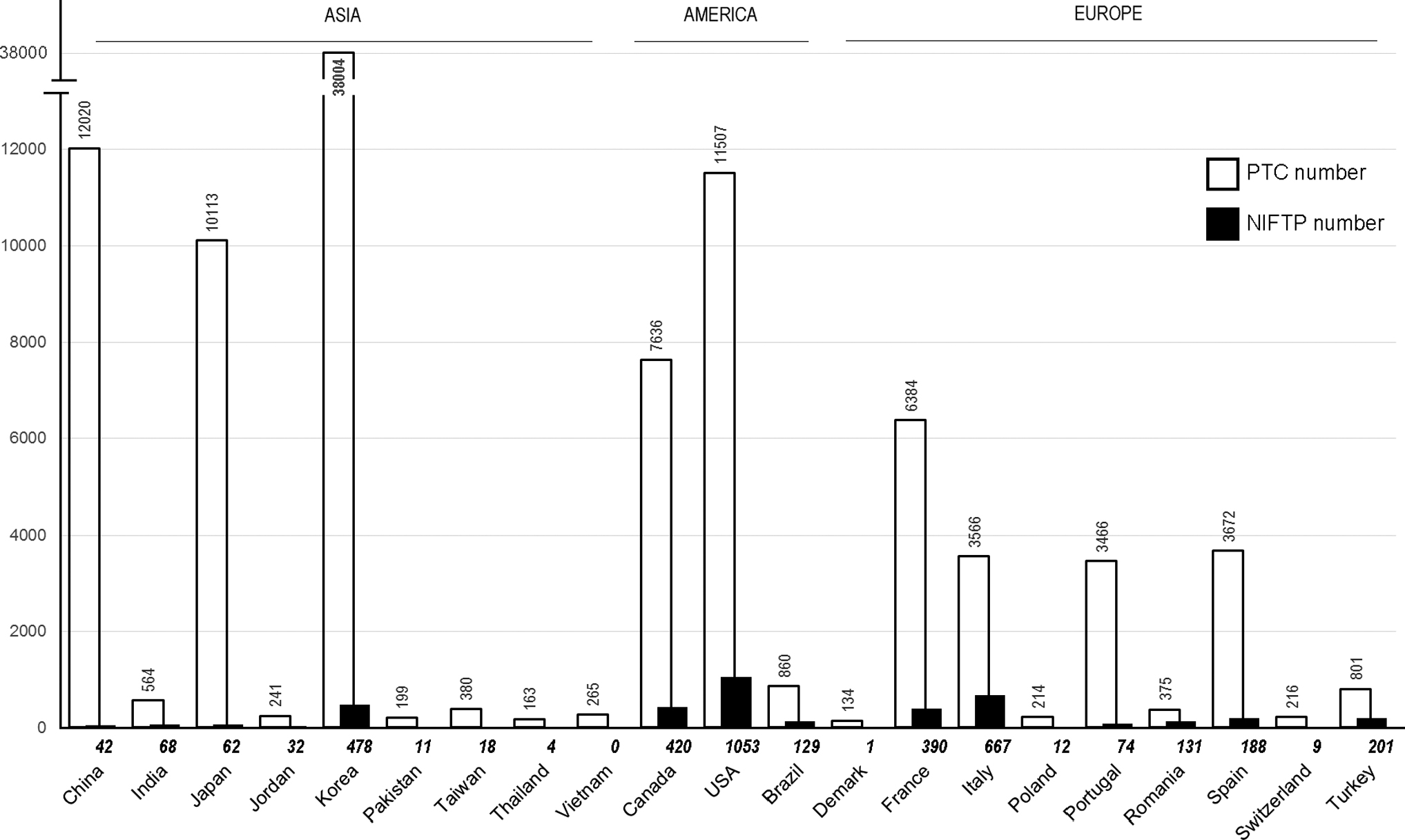
Number of PTC and NIFTP cases included in the study from different countries. Numbers of PTCs and NIFTPs are provided at the top and bottom of the corresponding columns. NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; PTC, papillary thyroid carcinoma.
In total, 3990 cases of NIFTP were identified, with an overall NIFTP incidence of 6.0% [CI 4.4–8.2] among PTCs or thyroid malignancies. There was a high level of heterogeneity among the included studies (I 2 = 98.6%). We performed subgroup analyses to identify the sources of heterogeneity. The NIFTP incidence from North America and Europe was largely similar (9.3% vs. 9.6%). Continent-wise, the highest incidence (15.0%) was documented in South America; however, this was based on a single study from Brazil. Despite recruiting the highest number of patients, the overall incidence in the Asian continent was significantly lower, such that NIFTPs constituted only 2.1% of all thyroid malignancies. However, when analyzed individually, the incidence rate was highly variable among different countries, ranging from 0.15% (Korea) to 34.9% (Romania). Table 2 shows detailed data on the incidence of NIFTPs from different countries (Supplementary Fig. S1).
Incidence of Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features in Various Subgroups
CI, 95% confidence interval.
The incidence of NIFTP also varied depending upon the database used for case inclusion and was ∼1.5 times higher when cytology databases were used, instead of surgical pathology databases (7.5% vs. 5.4%). The majority of the studies used the latter source for case retrieval. Eight studies used the 2018 diagnostic criteria for NIFTP, while the remaining 52 studies used 2016 criteria. When the rates of NIFTP were compared between these studies, it was observed that the overall incidence of NIFTP declined from 4.6% to 1.8% with the use of the revised 2018 diagnostic criteria.
It was also seen that, regardless of geography, the overall reported incidence of NIFTP declined considerably in studies, which were conducted after 2017. This decline in rates was particularly significant in studies from the United States and European countries, where NIFTP rates dropped from 17.4% (reported in 2015–2017) to 6.5% (2018–2021), two-tailed p-value = 0.002 by t-test. At the same time, the Asian series did not produce statistically significant difference between both time periods (p = 0.2). The degrees of heterogeneities following subgroup analyses remained high (I 2 > 75% in all subgroups).
Estimation of worldwide incidence of NIFTPs
The results of the present study were also applied to the data on thyroid cancers and PTCs as provided by GLOBOCAN 2020 (66) and Mao and Xing (67), respectively. Considering the worldwide incidence of NIFTP to be 6.0%, as found in our meta-analysis, this reclassification would have an impact on ∼30,881 patients annually. However, this impact would be lower in Asia compared with Europe and North America, despite the fact that the crude number of thyroid cancers and PTCs diagnosed annually is four to six times higher in the Asian continent. Table 3 shows in detail the estimated number of NIFTPs in relation to the incidence rate documented in the present study.
Estimated Annual Incidence of Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features Based on GLOBOCAN Data
Worldwide estimate used.
Publication bias
No publication bias was found after conducting Egger's regression test (p = 0.271) and visualization of funnel plot (Supplementary Fig. S2).
Discussion
In this meta-analysis, we have collected data from the available publications with reported institutional incidence of NIFTP (Table 2). A total of 50 studies were included, which were conducted in America, Europe, and Asia. We found that the overall incidence of NIFTP was 6.0% [CI 4.4–8.2] of all the PTCs worldwide. Asian studies reported a much lower incidence of NIFTP (2.1% [CI 1.2–3.6]) compared with the European and American counterparts. This incidence also was highly variable among different countries and also significantly reduced in non-Asian studies conducted after 2016.
An international, multidisciplinary, retrospective study published in 2016 proposed reclassification of a type of low-risk thyroid cancer as NIFTP, eliminating the term “cancer/carcinoma” from the tumor name (2). Immediately, NIFTP became a hot topic among the scientific community, such that within a short span of <2 years, there were more than 80 peer-reviewed publications reporting an institutional experience with NIFTP, largely from America and Europe (4). Adoption of the new terminology has significantly influenced the management strategies and guidelines as patients with NIFTP are now no longer labeled as having cancer and hence treated less aggressively, leading to a decrease in the financial burden on the health care system worldwide (2,7,8,68). Another important impact of NIFTP reclassification was to suggest that it likely represents the “benign” counterpart or precursor of invasive EFV-PTC, a concept that had not been accepted and understood in clinical thyroidology until recently (2).
The impact of the changes related to NIFTP reclassification depends on the incidence of NIFTP in a particular population or institution (8). Nikiforov et al. in their seminal article documented NIFTP rates of 18.6% among 3400 PTC cases retrospectively evaluated in a multi-institutional study, including the Italian and American institutions. They further estimated that this reclassification would have an impact on more than 45,000 patients annually worldwide (2). Soon, five independent retrospective studies from the United States, Europe, and Brazil documented a large series of patients with NIFTP (over 70 patients in each series), with rates ranging 15–28% (16,17,23,42,69). These NIFTP rates were further supported by other studies from those regions (14,15).
As per the GLOBOCAN data, the Asian continent contributed 59.7% of all the new worldwide thyroid cancer cases in 2020 (66). Despite this significant load, there was limited literature related to NIFTP and its rate till 2017, when Bychkov et al. reported data from nine Asian tertiary thyroid cancer centers (22). In this study, a total of 1070 cases of FV-PTC were identified after screening of 26,604 cases of PTC, subsequently reclassifying 206 cases of FV-PTC as NIFTP, documenting very low rates of NIFTP ranging from 0% to 4.7%, with an average of 1.5%, which was more than 10 times lower, compared with the Western series. Earlier findings from meta-analysis suggested discrepancies in NIFTP incidence between Asian and Western countries; however, results from that study relied on NIFTP cases searched via the cytology database alone (70). The present meta-analysis contributed by 28 independent institutions from 9 Asian countries has confirmed a low rate of NIFTP (2.1%) from the Asian continent, even a wide variation was noted, such as from 0.4% in China (22,29,48,63) to 14.4% in India (33,58,71). On the contrary, the incidences of NIFTP from European and American countries were much higher (Table 2).
The reasons for discrepancies between the Western and Asian series, as suggested by our meta-analysis, are multifactorial. First, although conventional PTC is the most common type of thyroid carcinoma, there is significant variation in the reported incidence of the FV-PTC between the Asian, American, and European continents (64,66,67). Until the inclusion of NIFTP in the latest histological classification of thyroid tumors, it was seen that EFV-PTC had increased in incidence by an estimated twofold to threefold over the past two to three decades and makes up 10–20% of all thyroid cancers diagnosed in Europe and North America during that era (4,72,73). Nikiforov et al. in their multi-institutional cohort study documented even higher rates of FV-PTC (37.9%) (2). However, these rates are much lower in Asian countries ranging from 2.2% to 9.8% (22,71). Since the majority of studies on NIFTP are retrospective studies where the cases of FV-PTC were reviewed, this difference in rates of NIFTP between Western and Asian countries, as suggested by our meta-analysis, can be well explained. Cancers are also known to exhibit racial and ethnic variations making them more common in one part of the world than another, along with influencing the mutation prolife and molecular mechanism in different populations (74). The prevalence of BRAFV600E mutation is known to be higher in many Asian countries such as Korea, Japan, and China, which could also render a predominance of classic PTC over FV-PTC in the continent (75 –79), therefore decreasing the rate of NIFTP.
Some FV-PTCs are known to have subtle or focally expressed nuclear features, which at times can make it extremely difficult to differentiate them from follicular adenoma or follicular carcinoma. This problem is further compounded by the fact that there is no consensus as to what percentage of a given (encapsulated) follicular lesion must show these characteristic nuclear features to make such a diagnosis. It has been observed that over the period of the last 10–15 years, the threshold to recognize PTC nuclear features (17,72) has decreased among the American pathologists, which could explain the growing incidence of FV-PTC along with the decrease in follicular adenoma cases (5,80 –82). On the contrary, this threshold has been found to be higher among the Japanese and Korean pathologists (83 –85). Hence, the different rates in the Asian and Western series could further be explained by this difference in threshold for interpretation of nuclear features.
Also, several studies emphasized recently that the Western and Asian countries have different approaches in management of indeterminate thyroid nodules where the NIFTP usually resides (86). It has been reported that surgeons in Asian countries encourage active surveillance in this scenario leading to a decreased number of resections, and hence, a lower rate of NIFTP (86 –88).
Apart from the reasons mentioned above, several other factors may contribute to the Western and Asian discordance. The primary source of search for data collection, surgical or cytological, may play a considerable part. The present study also suggests that data of NIFTP collected from the surgical database yielded 1.5 times lower incidence of NIFTP compared with data collected from the cytology database. The FNA database may not be considered an ideal source for data collection due to higher chances of drop out of referral cases as well as less maintained databases in single-institutional settings compared with countries with a comprehensive health care system (19,89). Hence, primary search of NIFTP via a surgical pathology database can provide more precise incidence. Our meta-analysis shows higher use of surgical databases for data collection in studies from Asian countries compared with studies from Europe and America (75% vs. 65%). This further suggests that the studies from Western countries might have overestimated the true incidence of NIFTP.
Asia contributes to more than half of all the new worldwide cases of thyroid cancers annually (66). Hence, many countries such as Korea have more active screening programs for detection of thyroid cancer, leading to higher detection rates of papillary thyroid microcarcinoma, which may further dilute the incidence of NIFTP in these regions (90). We also observed that with time, especially after 2017, there has been a declining trend in NIFTP rates particularly in North American and European studies. The possible reason could be the use of more refined criteria for NIFTP as suggested by Nikiforov in 2018 (<1% papillae substituted with no papilla). This study also observed nearly 2.5 times decline in the incidence of NIFTP when studies using the 2016 versus 2018 diagnostic criteria were compared. Another possible reason for the decrease in NIFTP incidence after 2017 could be related to the fact that in the NIFTP era, submission of the entire capsule of the nodule for microscopic examination is being suggested leading to increased detection of capsular invasion by pathologists. Also, since the introduction of this new entity, pathologists are getting more versed and hence are more vigilant of diagnostic features. For instance, Cho et al. in their study showed that the arbitrary cutoff of 1% misclassified noninvasive classical PTCs with a predominant follicular architecture as NIFTPs. Therefore, they suggested that diagnosis of NIFTP should only be restricted to tumors displaying an exclusive follicular pattern lacking true papillae (23). However, Xu et al. in their recent study of 235 unifocal encapsulated PTCs did not document any nodal metastasis irrespective of the invasive status, suggesting that the initial <1% papillae criterion may still be valid for diagnosis of NIFTP (91). The results of our study showed that the impact of refined criteria is just within 10% decrease, as it was found in the study by Cho et al. (23), which is not sufficient to explain the 2.5-times drop in NIFTP rate reported in non-Asian series after 2017. We speculate that soon after the initial excitement about this new entity, pathologists started using more stringent criteria, therefore the incidence is decreasing. The decrease in the reported prevalence of NIFTP can further be explained by the fact that in cases with borderline nuclear features of PTC and the differential diagnosis of follicular adenoma versus NIFTP, pathologists no longer feel a concern with missing cancer and more often diagnose such nodules as follicular adenoma.
There are some concerns in this study that need to be outlined. First, there was selection bias due to the retrospective nature of all the studies included in the meta-analysis. To our surprise, no prospective study reporting institutional incidence of NIFTP has been published so far. Second, the degree of heterogeneities was very high and could not be explained by subgroup analysis. The only possible explanation could be the institutional variations in diagnostic criteria (i.e., perception threshold for PTC nuclei) and hence different FV-PTC rates. In fact, despite having a long list of factors potentially contributing to the different NIFTP rates among institutions explained above, we believe that observer variation in histological interpretation is the major one. This is best illustrated by a case when three institutions from the same city, Boston, reported markedly variable incidence of NIFTP, namely 28.0% (14), 14.5% (40), and 2.3% (56).
Another limitation is that the number of studies included varied significantly among countries, which could affect the pooled incidence of NIFTP. Using numbers of thyroid carcinoma instead of PTC, which have been provided in several studies, may have led to the overestimation of NIFTP incidence. However, we do not expect that this particular factor could introduce significant bias because the number of such studies/institutions was <10% out of all the studies enrolled. In addition, we cannot exclude publication bias toward institutions with historically high rates of FV-PTC, and hence NIFTP. This could be a reason why a high NIFTP rate was reported in 2016, immediately after the introduction of this new entity. Lastly, we could not find relevant studies from many European countries, including highly populated Germany and the United Kingdom. Similarly, there is a severe lack of data from Latin America and completely missing data from Australia, Africa, and the Middle Eastern countries. While our study revealed an obvious trend of different NIFTP rates among continents, we anticipate more reports from the above countries, which will help fill a geographic map of NIFTP.
Almost all the studies so far have done a retrospective search for NIFTP by reviewing the cases of FV-PTC, which may not be sufficient to document all cases of NIFTP in a given institution. Several recent studies (58,92,93) documented that a substantial number of cases initially diagnosed as follicular adenoma and adenomatoid nodule were reclassified into NIFTP leading to an increase in its rates. Hence, both these encapsulated/circumscribed follicular-patterned lesions should be added in the retrospective search along with FV-PTC to find the true incidence of NIFTP. We admit that our calculated NIFTP rate could be biased by this fact; however, it should be emphasized that this meta-analysis rather sought for clinically meaningful NIFTP cases, that is, those, which could be downgraded from FV-PTC and bring benefits to patients. Reclassification of some benign nodules (adenomas or hyperplastic) into NIFTP has no clinical consequences.
The present study has several strengths, most importantly being able to bring attention to the actual NIFTP rates, which is of importance to a wide audience ranging from pathologists to clinicians to epidemiologists. Strict inclusion and exclusion criteria used in the meta-analysis provide more reliability to our data. Analysis of impact of the type of database used in selection for cases of NIFTP along with variable trends of NIFTP rates with time also makes this meta-analysis more informative. A recent study by Kitahara et al. reported on the influence of nomenclature changes on trends in PTC incidence in the United States. The authors found that recent (2016–2017) declines were observed for all PTCs and, particularly, the incidence of FV-PTC sharply declined from 2015 to 2017. Furthermore, they estimated that observed increases in NIFTP accounted for 10% of the decline in FV-PTC (94). We anticipate, based on our data, that with time, NIFTP will not be included in cancer registries and will have an impact on thyroid cancer statistics.
In conclusion, our meta-analysis confirms that the worldwide NIFTP incidence is much lower (6%) than estimated initially (15–28%). The overall incidence in the Asian continent was significantly lower compared with the Western countries. The reasons for this discrepancy are multifactorial, including geographic variability in the incidence of PTC, different thresholds for identification of nuclear features in the interpretation of follicular patterned thyroid lesions, and different approaches in the management of thyroid nodules in indeterminate categories. Also, there was a considerable decline in NIFTP rates in studies conducted after 2017, particularly those from the United States and European countries. We estimated that over 30,000 patients annually worldwide could be potentially spared from overtreatment following reclassification of noninvasive EFV-PTC to NIFTP. Future prospective studies with a strict adherence to diagnostic criteria may further validate our findings.
Footnotes
Authors' Contributions
C.R.: conceptualization, data curation, formal analysis, investigation, validation, writing—original draft, and editing.
H.G.V.: conceptualization, data curation, formal analysis, investigation, methodology, validation, writing—original draft, and editing.
T.Q.N. and H.C.N.: data curation, formal analysis, investigation, writing—review, and editing.
C.K.J. and K.K.: investigation, methodology, validation, writing—review, and editing.
A.B.: conceptualization, investigation, methodology, software, validation, writing—original draft, and editing.
Statement of Ethics
This study is exempt from ethics committee approval since this is a systematic review and meta-analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by a grant (NRF-2020R1F1A1070028) from the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Science and ICT.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2