
Abstract
Background:
Survivors of pediatric differentiated thyroid carcinoma (DTC) receive thyrotropin-suppressive therapy to minimize disease recurrence. However, knowledge about long-term effects of subclinical hyperthyroidism on bone mineral density (BMD) in pediatric DTC survivors is scarce, as is the information regarding long-term consequences of permanent hypoparathyroidism on BMD. We evaluated BMD in pediatric DTC survivors and investigated if BMD was affected by subclinical hyperthyroidism and/or permanent hypoparathyroidism during long-term follow-up.
Methods:
In this nationwide longitudinal study, we determined BMD in the lumbar spine and femur by dual energy X-ray absorptiometry in 65 pediatric DTC survivors. Measurements were repeated after minimal 5 years of follow-up in 46 pediatric DTC survivors. BMD results were evaluated according to the recommendations of the International Society for Clinical Densitometry (ISCD) and WHO. At both visits, we determined biochemical parameters and markers of bone resorption (C-terminal telopeptide of type I collagen [β-CTX]) and formation (N-propeptide of type I collagen [PINP] and osteocalcin).
Results:
First and second BMD measurements were done after a median follow-up of 17.0 (interquartile range [IQR] 8.0–25.0) and 23.5 (IQR 14.0–30.0) years after diagnosis, respectively. Median age at diagnosis was 15 years (IQR 13.0–17.0). Twenty-nine percent of the survivors had subclinical hyperthyroidism. In most survivors, BMD T- and Z-scores were within the reference range during both BMD evaluations. However, after 23.5 years of follow-up, a low BMD was found in 13.0%. In the 13 survivors with permanent hypoparathyroidism, BMD values did not differ after 5 years of follow-up compared with baseline values or in comparison with the 33 survivors without permanent hypoparathyroidism. During follow-up, turnover markers β-CTX and PINP remained stable.
Conclusions:
This longitudinal study of pediatric DTC survivors demonstrated normal and stable median lumbar spine and femur BMD values after a median time of 17 and 23.5 years after diagnosis. However, compared with controls, a lower BMD was still found in 13.0% after prolonged follow-up despite intensive follow-up. Based on the studied follow-up period, these data do not provide convincing evidence in support of standard monitoring of bone mass among DTC survivors, but may be restricted to individual cases at low frequency.
Trial Registration:
This follow-up study was registered in The Netherlands Trial Register under no. NL3280 (
Introduction
Differentiated thyroid carcinoma (DTC) during childhood is a rare disease. It has an excellent prognosis, with 15-year survival rates exceeding 95% (1). Nevertheless, the morbidity caused by initial treatment remains considerable. Permanent hypoparathyroidism as postoperative complication was found in up to 23.8% of patients; salivary gland dysfunction as an effect of radioactive iodine treatment was found in 47.6% of patients; and cardiovascular morbidity was reported, in adults, as a possible consequence of thyrotropin (TSH)-suppressive therapy (2 –5).
Mainly in high-risk patients, TSH-suppressive therapy with supraphysiological doses of thyroid hormone is recommended to prevent the growth of any remaining neoplastic tissue (6,7). Overt hyperthyroidism has been shown to affect bone metabolism, causing high bone turnover, increased bone resorption and shortening of the bone remodeling cycle, leading to decreased bone mineral density (BMD) of all skeletal sites and osteoporosis (8). In the adult DTC population, the association between endogenous forms of subclinical hyperthyroidism and bone loss at the hip is well established (9,10). The effects of TSH-suppressive therapy due to exogenous thyroid hormones on BMD are less certain; however, in postmenopausal women TSH-suppressive therapy has been considered a risk factor for osteoporosis, but in men and premenopausal women BMD is probably not affected (11 –16).
In the pediatric DTC population, TSH-suppressive therapy is usually administrated as standard practice and treatment during the period of linear growth and bone acquisition, and may result in detrimental effects on BMD and accrual of bone mass (6,7). Only two cross-sectional studies have assessed the long-term effects of TSH-suppressive therapy on BMD in childhood DTC survivors (17,18). The first study, a cross-sectional evaluation of 124 female pediatric DTC survivors with a mean age of 25 years after a mean follow-up of 10 years, showed no relationship between TSH suppression and lumbar spine and femoral BMD (17). In pediatric DTC survivors receiving calcium and vitamin D supplements for postsurgical hypoparathyroidism, higher lumbar spine and femur BMD values were reported. This association was attributed to reduced resorptive activity of endogenous vitamin D in the presence of parathyroid hormone (PTH) deficiency that was corrected by calcium and vitamin D treatment (17). The second cross-sectional study of 17 pediatric DTC survivors, with a mean age of 27 years and mean follow-up of 14 years, found no relationship between TSH suppression and lumbar spine and femoral BMD or bone microarchitecture compared with 34 healthy controls (18).
Importantly, individual changes in BMD over time during growth and in response to prolonged TSH-suppressive therapy have not been studied and require prospective longitudinal studies. Thus, we primarily determined the changes in lumbar spine and femoral BMD in pediatric DTC survivors treated with TSH-suppressive therapy, initially at a median interval of 17 years after diagnosis and subsequently after 5 years of prospective follow-up. A secondary outcome was to determine the long-term effect of permanent hypoparathyroidism on BMD in pediatric DTC survivors with and without this complication after surgery.
Methods
Study design and population
This study is part of a nationwide long-term follow-up study on pediatric DTC survivors in The Netherlands, as previously described in detail (2). All patients ≤18 years old diagnosed with DTC between 1970 and 2013 and treated in The Netherlands were eligible for inclusion. Exclusion criteria were age <18 years at the start of the study, a follow-up <5 years at first evaluation, DTC as a second malignancy, and thyroid hormone withdrawal or recombinant human TSH (rhTSH) ˂3 months before evaluation. For this study we performed two evaluations, with an interval of ±5 years, consisting of an assessment of the medical history, an evaluation of risk factors for osteoporosis, a physical examination, BMD measurements, and blood sampling (5).
Data collection
The Institutional Review Board of the University Medical Center Groningen (UMCG) approved the study on behalf of all six participating institutions (NL40572.042.12, Netherlands Trial Registry 3280). We obtained written informed consent from all subjects before their participation, performed analyses on anonymized data sets, and consulted patient records to obtain medical history, diagnosis, and treatment details (2). We collected all available historical TSH values and sampling data from hospital laboratory reports or general practitioners.
Study definitions
We have previously provided detailed study definitions and used the definitions below for this specific study (2,3). We calculated follow-up time from date of diagnosis until both evaluations. We defined transient and permanent hypoparathyroidism based on the use of prescribed calcium and active vitamin D for less than six months, and for more than six months after thyroidectomy, respectively. No pediatric DTC survivor who developed permanent hypoparathyroidism has been treated with parathyroid hormone. Pediatric DTC survivors reported their history of fractures (including age and cause of event). To calculate body mass index (BMI) we used the standard formula (BMI = mass [kg]/height [m]2). We defined as postmenopausal women those who had experienced no menstrual bleeding for 12 or more consecutive months (except women who were pregnant, using contraception, or underwent a hysterectomy). No pediatric DTC survivor used steroids or estrogen due to premenopausal estrogen deficiency during long-term follow-up.
The mean TSH level represents the area under the curve for pediatric DTC survivors with at least one available TSH measurement per year from diagnosis to second evaluation of this study. We calculated the mean TSH level during the following three periods: entire follow-up period (diagnosis—second evaluation), first follow-up period (diagnosis—first evaluation), and period between first and second evaluations. We excluded TSH values obtained prior 131I therapy, and during periods of thyroid hormone withdrawal or after stimulation with rhTSH. If a reported value was below the relevant assay detection limit, we used the TSH value of the detection limit for analysis. In addition, we separately determined TSH on the day of the BMD measurements. Subclinical hyperthyroidism was defined as a TSH value between 0.1 and <0.5 mIU/L.
Bone mineral density
To perform BMD measurements of the lumbar spine (vertebrae L1–L4) and femoral neck/proximal femur, we used dual energy X-ray absorptiometry. Two centers used the Lunar system (Lunar DPX-L densitometer; Lunar, Inc., Madison, WI), and four the Hologic system (Hologic QDR Discovery; Hologic, Inc., Waltham, MA). To correct for this difference, we cross-calibrated the systems using phantom data. BMD results were expressed as T- and Z-scores according to the National Health and Nutrition Examination Survey III (NHANES III) (19). The Z-score represents comparison with an age-matched adult (adjusted for sex and race/ethnicity); the T-score represents comparison with a healthy 30-year-old adult (adjusted for sex and race/ethnicity). For premenopausal women and men aged <50 years Z-scores were used with low BMD defined as a Z-score of the lumbar spine or hip ≤−2.0 SD, according to the recommendations of the International Society for Clinical Densitometry (ISCD) (20). A Z-score of >−2.0 SD was considered within the expected range for age. For postmenopausal women and men aged ≥50 years T-scores were used with osteoporosis and osteopenia defined as a T-score of the lumbar spine or hip ≤−2.5 SD and between −2.5 and −1.0 SD, respectively, according to WHO criteria (20,21). A T-score of ≥−1.0 SD was considered normal. Survivors with low BMD, osteopenia, or osteoporosis were considered as having a lower BMD compared with controls.
Laboratory measurements
We asked the pediatric DTC survivors to provide fasting morning blood samples on the same day as BMD measurements. Blood samples were stored at a temperature of −80°C until central analysis (UMCG). The following bone turnover markers were determined: C-terminal telopeptide of type I collagen (β-CTX), N-propeptide of type I collagen (PINP), and osteocalcin (OC). To analyze TSH, PTH, and β-CTX, an electrochemiluminescent immunoassay on the Cobas 6000 immunoanalyzer (Roche Diagnostics, Almere, The Netherlands) was used. 25-Hydroxy vitamin D (25OHD) was analyzed by liquid chromatography tandem-mass spectrometry. PINP was determined by a radioimmunoassay (AIDIAN OY, Espoo, Finland) and OC by using an immunoradiometric assay (DiaSource Immunoassays S.A. Louvain-La-Neuve, Belgium). Alkaline phosphatase (ALP) was analyzed using a colorimetric assay on the Cobas 6000 chemistry analyzer. β-CTX, PINP, and OC values were expressed as absolute values and Z-scores using local reference values of the UMCG (adjusted for age and sex) (22). During follow-up, as recommended by the guidelines, target TSH levels were below the limit of normal (6,7). β-CTX and PINP were analyzed at both evaluations, whereas OC, ALP, PTH, and 25OHD were measured only during the second evaluation.
Statistical analyses
Not normally distributed data were expressed as median and interquartile range (IQR). BMD values of survivors participating in one or both evaluations, BMD values of survivors with and without permanent hypoparathyroidism and bone turnover markers in survivors with declining and stable/increasing T-/Z-scores, were compared using a Mann–Whitney U test or chi-square test/Fisher's exact test. BMD values and bone turnover markers of both evaluations were compared using the Wilcoxon signed-rank test. Two-sided p-values <0.05 were considered statistically significant. IBM SPSS Statistics for Windows, version 23.0 (IBM Corp, Armonk, NY) was used for statistical analysis of the data.
Results
Participants
This nationwide follow-up study originally consisted of 105 pediatric DTC survivors, of whom 65 (61.9%) were eligible for the first evaluation (November 2012–September 2014, Fig. 1). The 65 eligible pediatric DTC survivors did not differ significantly in clinical or treatment characteristics from the 40 noneligible survivors. All 65 participants seen in the first evaluation were asked to participate in the second evaluation (November 2018–January 2020); 46 pediatric DTC survivors (70.8%) agreed to participate (Fig. 1).
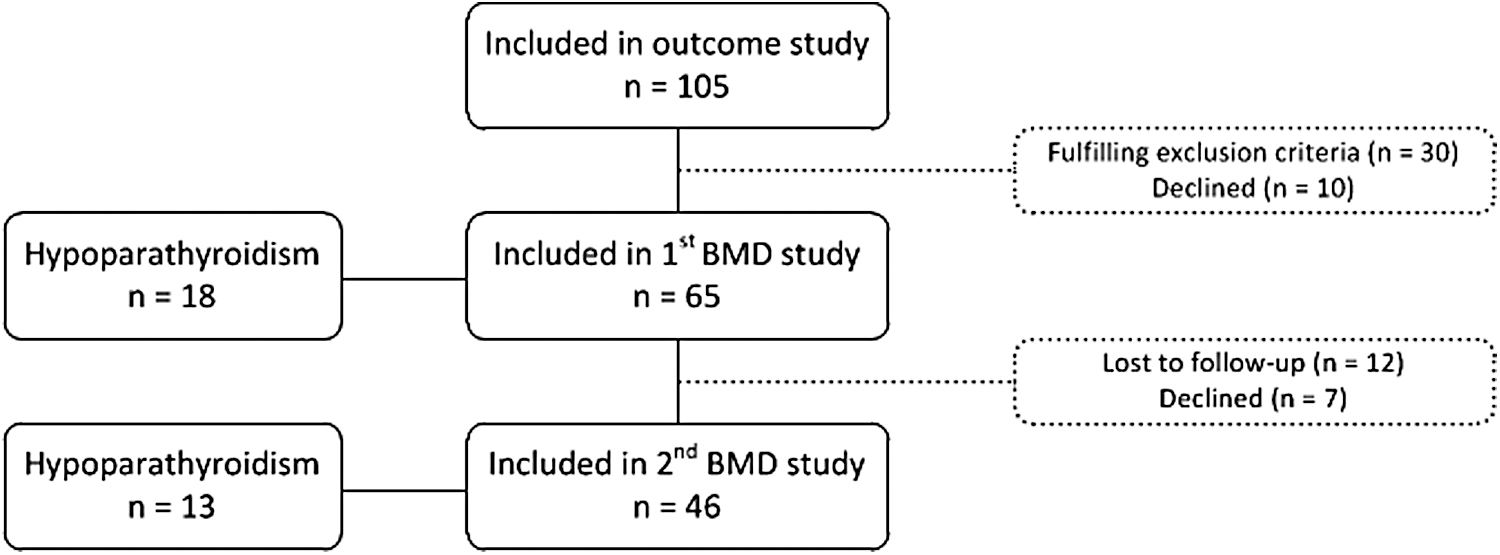
Study flowchart with number of participating pediatric DTC survivors and reasons for noneligibility in first and second BMD evaluations (2). BMD, bone mineral density; DTC, differentiated thyroid carcinoma.
The 65 participants of the first evaluation had a median age at diagnosis of 15 years (IQR 13.0–17.0) and a median age of 32 years (IQR 24.0–40.0) at the first evaluation (Table 1). All had undergone a total thyroidectomy, and 95.7% had received 131I therapy. Median follow-up time was 17.0 years (IQR 8.0–25.0) after diagnosis. Eighteen pediatric DTC survivors (27.7%) had been diagnosed with permanent hypoparathyroidism. Of the pediatric DTC survivors with available TSH values, 29% had a subclinical hyperthyroidism. The median BMI of the 65 participants of the first evaluation was 23.6 kg/m2 (IQR 21.3–26.1), 8 pediatric DTC survivors had a BMI >30 kg/m2.
Clinical and Treatment Characteristics of Study Population
Data represent median (IQR) or number (percent).
In 24 survivors, available TSH values insufficient for analyses, hence n = 41.
In 24 survivors, available TSH values insufficient for analyses, hence n = 22.
In 36 survivors, available TSH values insufficient for analyses, hence n = 10.
P-values represent comparison of survivors with only one evaluation (N = 19) and survivors participating in both evaluations (N = 46) during the first evaluation.
P-values represent comparison of the first (N = 46) and second (N = 46) evaluation of survivors participating in both evaluations.
AUC, area under the curve; BMI, body mass index; FTC, follicular thyroid carcinoma; IQR, interquartile range; PTC, papillary thyroid carcinoma; TSH, thyrotropin.
No statistically significant differences in clinical or treatment characteristics and BMD values were found between the 19 pediatric DTC survivors with only one evaluation and the 46 survivors participating in both evaluations (Table 1). Of the 46 pediatric DTC survivors participating in both evaluations, 40 were female (87%) with a median age at diagnosis of 16 years (IQR 12.8–17.0), and a median age of 34 years (IQR 25.0–41.5) at the time of first evaluation (Table 1). In the 46 pediatric DTC survivors participating in both evaluations, the TSH levels at the time of BMD measurement did not differ (Supplementary Table S1).
BMD measurements
The median BMD values of 65 pediatric DTC survivors participating in the first evaluation are presented in Table 1 and were in most survivors within the reference range. The Z- and T-scores of the 12 pediatric DTC survivors with subclinical hyperthyroidism did not differ from the 29 pediatric DTC survivors without subclinical hyperthyroidism till first evaluation.
In the 46 pediatric DTC survivors participating in both evaluations, there were no differences between the median T- and Z-scores between the first and second evaluation (Table 1). An analysis of men and women separately, and of women, who were pre- or postmenarche during treatment for DTC (34 of 40 women were postmenarche), respectively, showed no statistically significant differences in BMD parameters between both evaluations (data not shown).
Of the 65 participants of the first evaluation, 9 participants were men (1 man ≥50 years) and 56 participants were women (4 postmenopausal women). Of the 46 participants participating in both evaluations, 6 participants were men (1 man ≥50 years) and 40 participants were women (6 postmenopausal women). During the first and second evaluation, one pediatric DTC survivor (premenopausal woman) had a low BMD (Z-score ≤ −2.0). During the first evaluation, three pediatric DTC survivors (three postmenopausal women) were diagnosed with osteopenia of the lumbar spine and/or hip. After 5 years of follow-up, 5 pediatric DTC survivors (4 postmenopausal women and 1 man ≥50 years) were diagnosed with osteopenia of the lumbar spine and/or hip. A T-score ≤−2.5 (osteoporosis) was not reported. After DTC diagnosis, 11 out of 46 pediatric DTC survivors experienced fractures after appropriate trauma.
Figure 2A and B indicates the pediatric DTC survivors with a significant decline (p < 0.05) in the T-/Z-scores of the lumbar spine (22 and 16 survivors, respectively), and Figure 2C and D in the T/Z-scores of the proximal femur (21 and 17 survivors, respectively) over the 5 years of follow-up. During the total follow-up period we found no differences between the groups with declining T-/Z-scores and the pediatric DTC survivors with stable or increasing T-/Z-scores, with regard to the presence of transient or permanent hypoparathyroidism, cumulative 131I dose, postmenopausal status, or extent of TSH suppression.
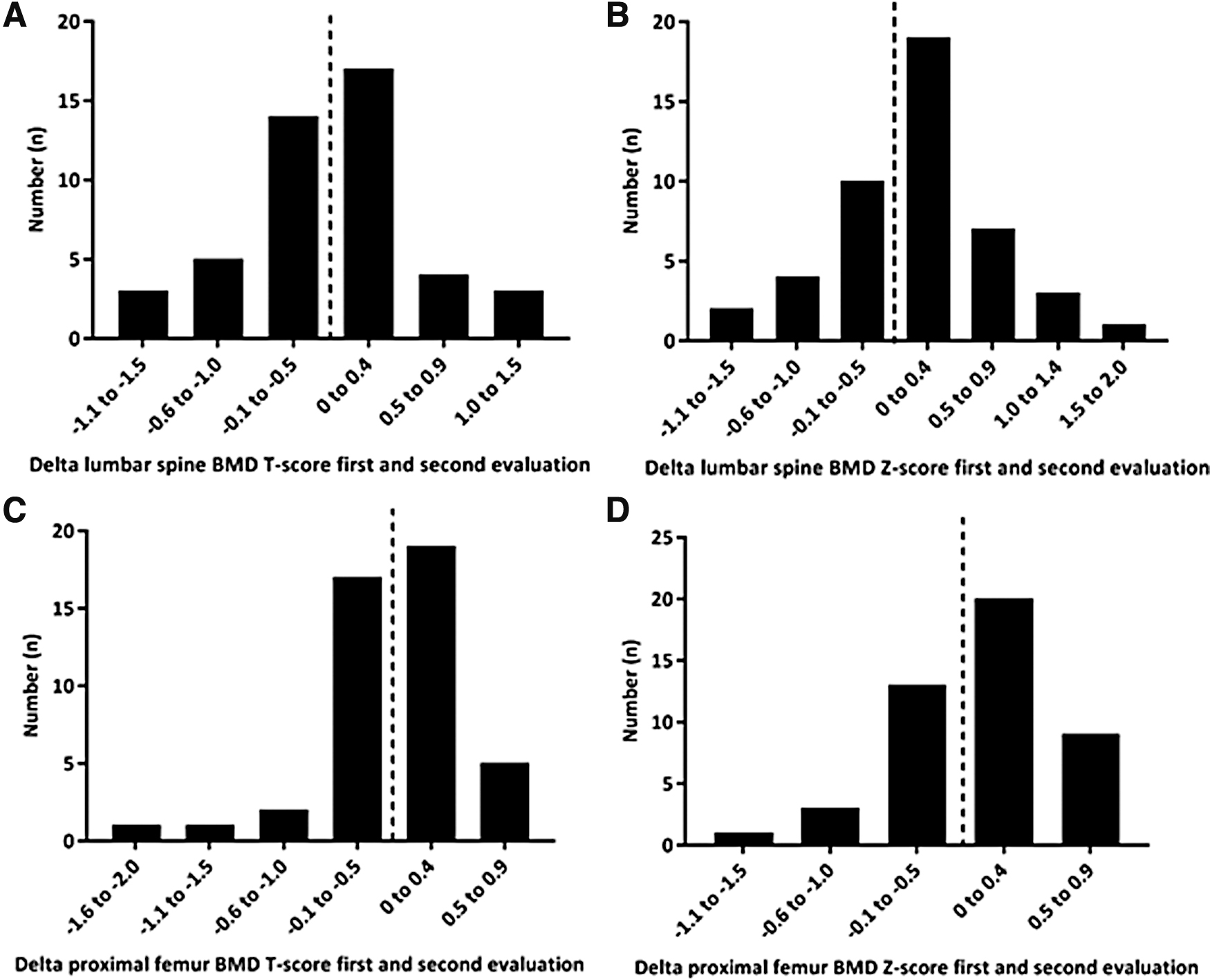
Difference (delta) in T-/Z-scores of lumbar spine (
Of the 65 pediatric DTC survivors participating in the first evaluation, 18 had been diagnosed with permanent hypoparathyroidism. The BMD values at the first evaluation of these 18 survivors did not differ from those of the 47 survivors without permanent hypoparathyroidism (Supplementary Table S2). During the second evaluation, BMD parameters also did not significantly differ between pediatric DTC survivors with or without hypoparathyroidism (Supplementary Table S3). Moreover, of the 46 pediatric DTC survivors participating in both evaluations, 13 survivors were diagnosed with permanent hypoparathyroidism. Their BMD values did not change over time (Supplementary Table S4).
Bone turnover markers
In the 46 pediatric DTC survivors participating in both evaluations, the bone turnover markers β-CTX and PINP did not change during follow-up (Table 2).
Bone Turnover Markers During First and Second Evaluation of 46 Pediatric Differentiated Thyroid Carcinoma Survivors Participating in Both Evaluations
Data represent median (IQR).
ALP, alkaline phosphatase; β-CTX, c-terminal telopeptide of type I collagen; OC, osteocalcin; PINP, n-propeptide of type I collagen.
Comparing the pediatric DTC survivors with declining T-/Z-scores of the lumbar spine with survivors with stable or increasing scores, no differences in bone turnover markers were found (Supplementary Table S5). In addition, focusing on the proximal femur, pediatric DTC survivors with declining T-scores had significantly higher values of β-CTX and OC, whereas the survivors with declining Z-scores showed no differences.
Bone turnover markers in pediatric DTC survivors with and without permanent hypoparathyroidism showed significant differences only during the first evaluation, the PINP Z-score was significantly lower (p = 0.03; Supplementary Table S2), but not during the second evaluation (Supplementary Table S3).
Discussion
In this longitudinal study of pediatric DTC survivors, normal and stable median lumbar spine and femur BMD values were found when determined at a median time of 17 years after diagnosis, and after minimal 5 years prospective follow-up. However, a lower BMD was found in 13.0% after 23.5 years of follow-up compared with controls.
The fact that median BMD values were found to be normal is reassuring, since pediatric DTC patients, diagnosed and treated in a period of bone acquisition, are exposed to plural factors influencing peak bone mass, including TSH-suppressive therapy and hypoparathyroidism (23). Our prospective data are consistent with two previous cross-sectional studies reporting no differences in BMD among pediatric DTC survivors (17,18) and with data in adults with DTC, in which it has been suggested that exogenous subclinical hyperthyroidism may not affect BMD in men and premenopausal women (16).
When using T-scores for the total study population, we found a comparable prevalence of osteopenia in our study population compared with a healthy population of the same sex and age (24,25). However, calcium and vitamin D concentrations in pediatric DTC survivors are routinely measured and supplementation is started when indicated. In this light, the percentage of osteopenia could be considered quite high. It will be interesting to follow this cohort for another five years to monitor prevalence of osteopenia in due time.
Knowledge about the disadvantages of TSH suppression therapy in the pediatric population is increasing; however, studies comparing the outcome and risk of several TSH suppression strategies is needed, especially in perspective of the excellent survival rates of pediatric DTC patients.
Permanent hypoparathyroidism was diagnosed in 27.7% of our subjects. Pediatric DTC survivors with and without hypoparathyroidism showed no significant differences in BMD during both evaluations. All median T-/Z-scores of pediatric DTC survivors with permanent hypoparathyroidism were higher than the scores of subjects without this condition. A finding reported before in pediatric DTC survivors and adult DTC patients (especially in postmenopausal women). This could be explained by a lower bone turnover as a result of lower PTH values and, therefore, a reduced resorptive activity (17,26 –28). A second explanation could be found in the treatment of hypoparathyroidism with a PTH-independent stimulating effect of active vitamin D on osteoblasts. Higher BMD values with lower bone turnover will lead to stiffer bones with lack of microdamage repair and loss of heterogeneous mineral distribution (29). It is still unclear whether hypoparathyroidism results in higher fracture risk (28,30). In our population, only few survivors reported fractures during follow-up, all of them after an adequate trauma. Of note, few if any low BMD-related fractures would a priori be expected to occur in this comparatively young population.
Bone turnover markers are helpful in monitoring antiresorptive and anabolic treatment, but not useful individually to classify bone loss or predict fracture risk (31). During TSH suppression, conflicting effects regarding bone turnover markers have been reported (23). In our study, during follow-up, β-CTX and PINP were stable in all 46 pediatric DTC survivors, including the subgroup of survivors with hypoparathyroidism. During the first evaluation, we found lower levels of bone turnover markers in pediatric DTC survivors with hypoparathyroidism than in survivors without hypoparathyroidism, but not during the second evaluation. This finding was also reported by others in the adult population (27,28).
This is the first study to investigate BMD changes over time by performing repeated evaluations in pediatric DTC survivors after long-term prospective follow-up. Data on height before and after DTC diagnosis were not available, though, major influences of DTC on height outcomes were not expected because of the median age of the survivors at DTC diagnosis (15 years), and most female survivors would already have reached their(near)-final height by passing their menarche before diagnosis. As a result of the low sample size of pediatric DTC survivors with permanent hypoparathyroidism and postmenopausal status, conclusions for these groups could not be made. Finally, TSH data were limited, which makes an association with TSH levels not clearly substantiated.
Conclusion
To conclude, this longitudinal study demonstrated stable median lumbar spine and femur BMD values in pediatric DTC survivors after a median time of 17 years after diagnosis, and after minimal another 5 years of prospective follow-up. After 23.5 years of follow-up, a lower BMD was found in 13.0% compared with controls. Based on the studied follow-up period, these data do not provide convincing evidence in support of standard monitoring of bone mass among DTC survivors, but may be restricted to individual cases at low frequency.
Footnotes
Acknowledgments
We thank J.R. de Jong, PhD, for providing the calculations on the phantom data and J. van Seventer, MA, for providing editorial comments on the article.
Authors' Contributions
Study concept and design by Dekker, Muller Kobold, Brouwers, Williams, Nies, Tissing, Burgerhof, Bocca, and Links. Acquisition, analysis, or interpretation of data by Dekker, Muller Kobold, Williams, Nies, Tissing, Bocca, and Links. Drafting of the article by Dekker, Muller Kobold, Williams, Tissing, Bocca, and Links. Critical revision of the article for important intellectual content by Brouwers, Nies, Klein Hesselink, van der Horst-Schrivers, Havekes, van den Heuvel-Eibrink, van der Pal, Plukker, Ronckers, van Santen, Corssmit, Netea-Maier, Peeters, van Dam, and Boot. Funding obtained by Nies, Klein Hesselink, Tissing, Bocca, and Links. Administrative, technical, or material support by Dekker, Muller Kobold, Brouwers, Williams, Nies, Klein Hesselink, Tissing, Burgerhof, Corssmit, Netea-Maier, Peeters, van Dam, Bocca, and Links. Study supervision by Tissing, Bocca, and Links. Final approval of the version to be published by all authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by Stichting Kinderen Kankervrij (Foundation Children Cancer-Free, The Netherlands, project no. 81) and the Junior Scientific Masterclass Groningen.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5