
Abstract
Background:
Childhood cancer survivors and bone marrow transplant recipients treated with radiation therapy (RT) are at increased risk for subsequent thyroid cancer. However, the genetic landscape of pediatric thyroid cancer, both primary and RT-induced, remains poorly defined, as pediatric papillary thyroid carcinoma (PTC) has been understudied compared with adults and data on pediatric follicular thyroid carcinoma (FTC) are virtually nonexistent. The objective of this study was to characterize and compare the molecular profiles of pediatric RT-induced PTC and FTC cases with primary pediatric thyroid cancers.
Methods:
A total of 41 differentiated thyroid carcinomas (11 RT cases and 30 primary cases) from 37 patients seen at Phoenix Children's Hospital between January 1, 2010 and December 31, 2019 were evaluated by targeted next-generation sequencing and/or BRAF immunohistochemistry.
Results:
Eighty-six percent (6/7) of RT-PTC harbored a gene fusion (GF) compared with 56% (14/25) of primary PTC; 14% (1/7) of RT-PTC had a single-nucleotide variant (SNV; specifically, a point mutation in the DICER1 gene) compared with 44% (11/25) of primary PTC (all of the latter had the BRAFV600E mutation). An exceedingly rare ROS1 fusion was identified in a child with RT-PTC. With respect to FTC, copy number alterations (CNAs) were seen in 75% (3/4) of RT cases compared with 40% (2/5) of primary cases. None of the RT-FTC had SNVs compared with 100% (5/5) of primary FTC.
Conclusions:
In children, the molecular profile of subsequent RT-induced thyroid cancers appears to differ from primary (sporadic and syndromic) cases, with a high prevalence of GFs in RT-PTC (similar to PTC occurring after the Chernobyl nuclear reactor accident) and CNAs in RT-FTC. A better understanding of the molecular mechanisms underlying these cancers may lead to more accurate diagnosis, prognosis, and treatment, as some of the genomic alterations are potentially targetable.
Introduction
Treatment advances in childhood cancer have resulted in five-year overall survival approaching 85% in the United States (1). Similarly, there is an 85% chance that children who undergo bone marrow transplant (BMT) will be alive 10 years later (2). However, with increased survival has come the recognition of serious late health effects as an unintended consequence of therapy. These include subsequent malignant neoplasms, which account for nearly one-half of nonrelapse mortality at five years (3). Radiation therapy (RT) is a major risk factor (4 –6).
RT-induced malignancies also affect adults, though children are more susceptible. Genotoxic injury to stem cells, which are generally more active in children compared with adults, may explain this difference (4). Further, the young thyroid appears particularly sensitive to RT-induced DNA damage, and children who have received RT to the head, neck, or upper thorax for a nonthyroid malignancy are at significant risk for differentiated thyroid carcinoma (DTC) (4,7 –9).
Standard incidence ratios in this population range from 5- to 69-fold relative to baseline, depending on radiation dose (10). The risk of RT-induced cancer is dose-dependent although plateauing at about 20–29 Gy (10) and strongly inversely correlated with age at exposure (5). This elevated risk persists for decades after exposure (11 –13). Tumorigenesis is driven by genomic alterations, and genomic injury is a known mechanism for radiation effects on normal tissues (4); however, the genetic landscape of RT-induced DTC in children has not yet been well defined.
Large adult studies have elucidated the main oncogenic drivers of primary DTC (14). Previous studies involving children, though limited, have shown similar genomic alterations as in adults; however, the frequency of particular alterations is quite different, as gene fusion (GF) events are much more common in children, whereas in adults, point mutations predominate (9).
Much of what we know regarding the role of radiation exposure in the development of DTC, including during childhood, comes from studies following the Chernobyl nuclear reactor accident in 1986. In these studies, GF emerged as the genetic drivers in RT-induced DTC (15).
Molecular mechanisms underlying the development of both primary and RT-induced DTC involve deregulation of the mitogen-activated protein kinase signaling pathway, and to a lesser degree, the phosphatidylinositol-3-kinase (PI3K)/AKT-pathway (16). Point mutations and GF function as key driver events for tumorigenesis in the thyroid follicular cell (9,16). The result is one of two subtypes of DTC: the more common papillary thyroid carcinoma (PTC), representing 80–90% of cases, or follicular thyroid carcinoma (FTC) (17).
Next-generation sequencing (NGS) is a tool that allows for simultaneous high-throughput sequencing analysis of genomic alterations. It has been used to study adult DTC to provide a comprehensive understanding of tumor biology (18). In this study, we used NGS to characterize the genetic landscape of RT-induced DTC developing in our childhood cancer and BMT survivors, and secondarily to compare these findings with the molecular profile of a cohort of other children from our institution with primary DTC.
Materials and Methods
Following approval by the Institutional Review Board (IRB), we retrospectively reviewed the electronic medical records of patients seen during a 10-year period (January 1, 2010 to December 31, 2019) in longitudinal childhood cancer and BMT survivor clinics, to identify those patients who received RT to the head, neck, or upper thorax, or total body irradiation, for a primary nonthyroid malignancy or as part of a BMT conditioning regimen at ≤18 years and subsequently developed a secondary DTC. There were 11 RT-induced tumors from 10 patients with adequate remaining tissue for genomic testing. All patients were contacted to obtain informed consent. If they could not be contacted, consent was waived per IRB approval.
Because the low number of RT cases precluded precise age/sex-matched control selection, the comparison group comprised all pediatric (aged ≤18 years) primary (i.e., no history of RT) FTC patients from the study period, the consecutive most recent PTC patients, and those whose tumors had been already characterized by clinical (i.e., not research) genomic testing by using NGS and/or positive immunohistochemistry (IHC) for mutant BRAF protein. There were 30 tumors from 27 pediatric primary DTC patients.
All 11 RT tumors and the majority (77%, 23/30) of primary tumors were sent for the ThyroSeq v3 assay. Thirty-three of these 34 tumors were resection specimens with formalin-fixed, paraffin-embedded (FFPE) tissue, and 1 was fine-needle aspirate (FNA) rinsing in ThyroSeqPreserve solution. For the resection specimens, we typically submitted one hematoxylin and eosin (H&E) and six unstained slides freshly cut at 5 μm and refrigerated until shipped. For the FNA case, frozen needle rinsings from two passes were submitted (one pass for rapid on-site evaluation plus an additional dedicated pass for possible molecular testing given the cytologic atypia that was observed).
Briefly, nucleic acids (DNA/mRNA) were isolated (in resection cases, the relative amount of tumor tissue was enriched by manual microdissection from the unstained slides, with H&E guidance) and NGS analysis was applied to detect single-nucleotide variants (SNVs)/indels, GF, gene expression alterations (GEA), and copy number alterations (CNAs) in targeted regions of 112 thyroid cancer-related genes. It should be noted that three of these cases (two FNA and one specimen with core needle biopsies) were initially reported as negative but subsequently were positive on quality assurance retesting performed on the resection specimens.
Two of the primary tumors had been sent for ThyroSeq v2, a 56-gene panel to evaluate for SNV/indels in targeted regions of 14 genes, more than 42 types of GF involving 9 genes, and GEA in 8 genes. One tumor had FFPE tissue (one H&E and five unstained sections were freshly cut at 5 μm from each of two core needle biopsies), while the other tumor had needle rinsings from four FNA passes (slides were prepared for three rapid on-site evaluation episodes).
One of the primary tumors had been sent to the City of Hope National Medical Center for their HopeSeq Thyroid FFPE NGS-based assay comprising hotspot mutation analysis of 87 genes, entire coding region mutation analysis of 48 genes, fusion analysis of 51 genes, copy number analysis of 47 genes, and microsatellite instability.
One primary tumor was sent for the FoundationOne NGS-based assay interrogating the entire coding sequence of 314 genes and the promoter of TERT for SNV/indels and CNA, as well as the introns of 28 genes involved in rearrangements, in addition to determining microsatellite status and tumor mutation burden. Another primary tumor was sent at a later date for the FoundationOne®CDx assay, which assesses the full coding exonic regions of 310 genes for SNV/indels and CNA and select intronic regions of 36 genes including TERC, a noncoding RNA gene, and the promoter region only of TERT.
Finally, BRAF IHC (but not NGS) was performed for clinical purposes on two resection specimens in the primary DTC group. Subsequently, BRAF IHC was performed for research purposes on all 11 RT tumors and interpreted by the study pathologist (K.T.S.).
The diagnosis of DTC was based on histopathological criteria put forth by the World Health Organization (19), and tumor classification was based on the seventh edition of the tumor-node-metastasis (TNM) system of the American Joint Committee on Cancer (20).
Statistical analyses
Descriptive statistics were prepared. Student's t and Fisher's exact tests were conducted to compare differences between RT- and primary (P)-DTC. A p-value <0.05 was considered statistically significant for analyses.
Results
Patients' demographic and clinical characteristics are summarized in Table 1. Clinicopathological and molecular features for each individual tumor can be found in Table 2. Figures 1 and 2 depict representative RT-induced and primary cases, respectively; Figure 3 shows genomic alterations identified by group.
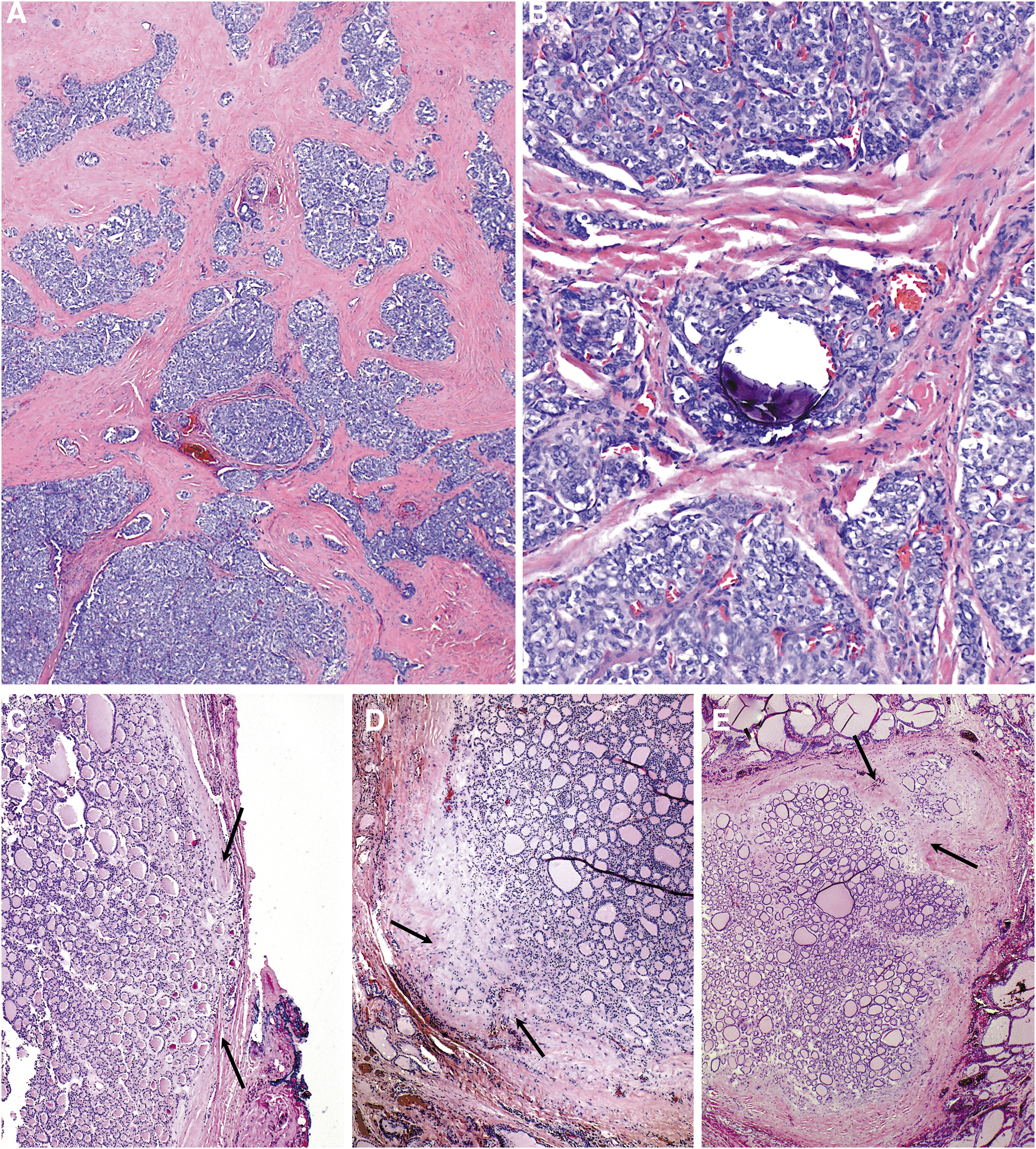
Representative RT-DTC cases (H&E stain). (

Representative P-DTC cases. (
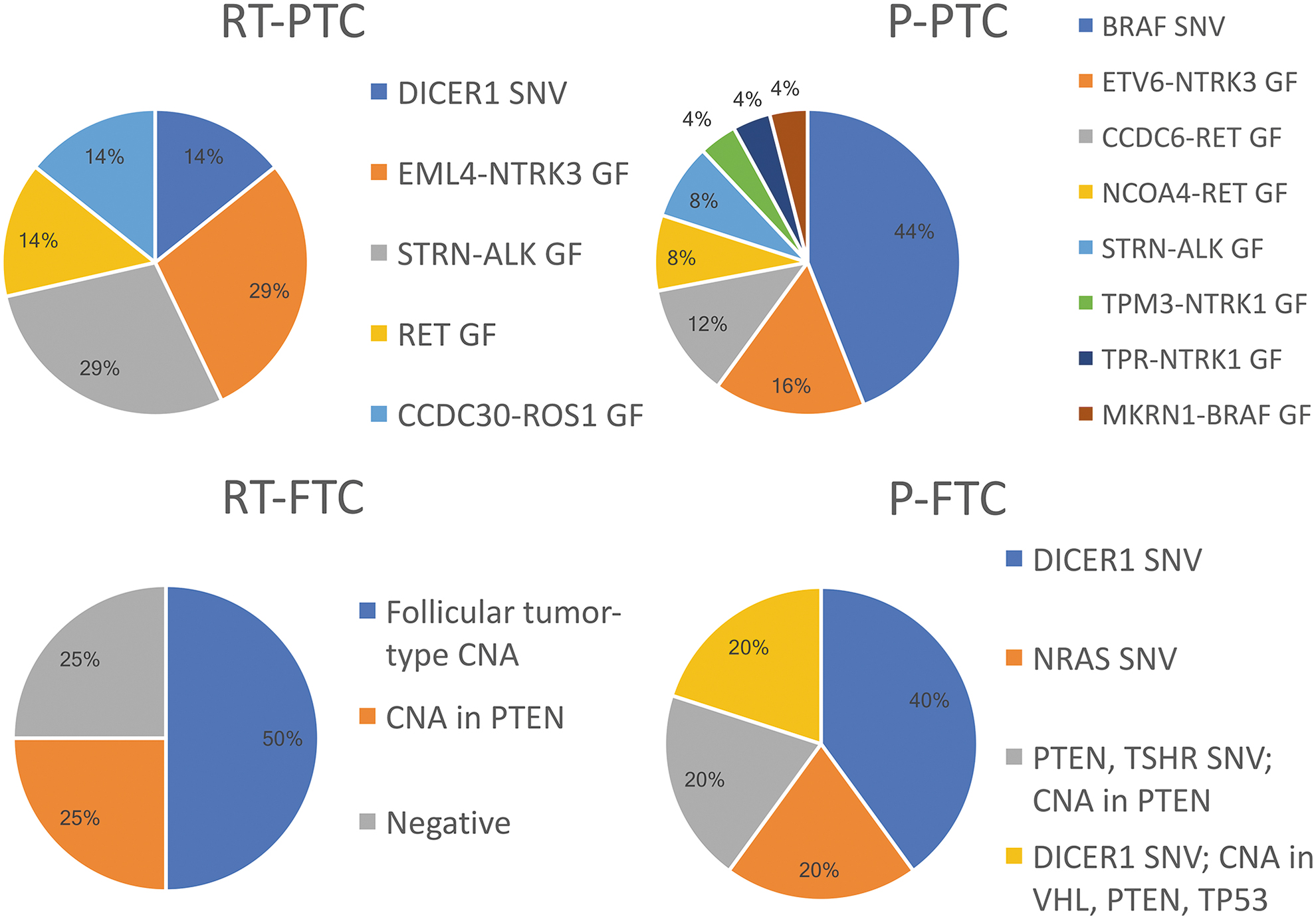
Pie charts depicting the frequency of the various SNV, GF, and CNA in our RT-induced and primary PTC and FTC. CNA, copy number alteration; GF, gene fusion; SNV, single-nucleotide variants. Color images are available online.
Demographic and Clinical Characteristics by Type of Differentiated Thyroid Carcinoma
Values are shown as n (%) or mean ± standard error.
FTC, follicular thyroid carcinoma; PTC, papillary thyroid carcinoma; RT, radiation therapy.
Clinicopathological and Molecular Features
SNV variant allele frequency listed as a percentage.
ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; ARMS, alveolar rhabdomyosarcoma; B-thal, beta-thalassemia; CHL, classic Hodgkin lymphoma; CNA, copy number alteration; DTC, differentiated thyroid carcinoma; e, exon; F, female; FHx, family history; FV, follicular variant; IHC, immunohistochemistry; infil, infiltrative; JMML, juvenile myelomonocytic leukemia; L, left; M, male; MDS, myelodysplastic syndrome; onco, oncocytic; P, primary; R, right; RAI, radioactive iodine; SNV, single-nucleotide variant; Warhtin, Warthin-like.
There were 11 RT-induced DTC cases from 10 patients (1 had 2 tumors tested) and 30 primary DTC cases from 27 patients (1 had 3 tumors tested, and another had 2 tumors tested).
The 10 patients in the RT group (6 female, 4 male) received RT for the following diagnoses: acute myeloid leukemia (3 patients), myelodysplastic syndrome, acute lymphoblastic leukemia, juvenile myelomonocytic leukemia, beta-thalassemia, classic Hodgkin lymphoma, alveolar rhabdomyosarcoma, and Wilms tumor with pulmonary metastases. The mean age at RT was 6.5 years (range 0.9–17.4). The mean latency period from RT to DTC diagnosis was 10.1 years (5.4–19.1), while the mean age at diagnosis of RT-DTC was 16.6 years (11.7–22.7).
Seven of the RT-DTCs were PTC coming from six patients (four female, two male). The mean age at RT was 8.6 years (3.2–17.4). The mean latency period from RT to PTC diagnosis was 8.5 years (5.4–18.2), while the mean age at PTC diagnosis was 17.1 years (11.7–22.7). The mean RT dose was 49.4 Gy; doses ranged from 4 to 187.2 Gy. The mean lesion size was 1.7 cm. Six of the seven RT-PTC (85.7%) demonstrated GF: two EML4-NTRK3, two STRN-ALK, one RET (partner gene not specified), and one with an exceedingly rare CCDC30-ROS1 fusion. A single RT-PTC (14.3%) harbored a DICER1 SNV (c.5438A>C p.E1813A). Interestingly, the patient who had multifocal PTC had a DICER1 mutation in one tumor and an EML4-NTRK3 GF in the other.
We examined four RT-induced FTC from four patients (three male, one female). The mean age at RT was 3.2 years (0.9–8.1). The mean latency period from RT to FTC diagnosis was 12.6 years (8.0–19.1); the mean age at diagnosis of FTC was 15.9 years (12.8–20). The mean RT dose was 24.5 Gy (8 –42). The mean lesion size was 2.2 cm. In terms of genomic alterations, three of four (75%) of RT-FTC had CNA: Two had multiple chromosome CNA of follicular tumor-type (common in both the follicular variant [FV] of PTC as well as FTC) (21), while the other had CNA (specifically, loss) involving the PTEN gene locus. There was one case in which no SNV/indels, GF, or CNA were detected. All 11 RT-DTC were negative for mutant BRAF protein by IHC.
The P-DTC group comprised 30 tumors from 27 patients, 1 of whom had PTEN hamartoma tumor syndrome, which is associated with FV-PTC, FTC, follicular adenoma, and hyperplastic nodule formation (21). The mean age at diagnosis of P-DTC was 14.4 years (7.3–18.7).
Most (83.3%) of the tumors in the P-DTC group were PTC, including 25 PTC from 22 patients (19 female, 3 male); 1 had 3 PTC analyzed, and 1 had 2 PTC analyzed. The mean age at diagnosis of P-PTC was 14.6 years (7.3–18.7). The mean lesion size was 2.5 cm. Fourteen (56%) of 25 P-PTC had a GF: 4 ETV6-NTRK3, 3 CCDC6 (a.k.a. PTC1)-RET, 2 NCOA4 (a.k.a. PTC3 or ELE1)-RET, 2 STRN-ALK, 1 TPM3-NTRK1, 1 TPR-NTRK1, and 1 MKRN1-BRAF. The 11 other P-PTC (44%) had the BRAFV600E SNV.
The remaining five tumors (16.7%) in the P-DTC group were FTC from five patients (four female, one male). The mean age at diagnosis of P-FTC was 13.3 years (9.3–16.3). The mean lesion size was 3.5 cm. Two patients had one DICER1 SNV each (c.5113G>A p.E1705K or c.5425G>T p.G1809W); one patient had two different DICER1 SNVs (c.5441C>T p.S1814L at 60.5% variant allele frequency, and c.5113G>A p.1705K at 30.7% variant allele frequency) accompanied by CNA involving the VHL, PTEN, and TP53 gene loci; one patient had an NRAS SNV (c.181C>A p.Q61K); and one patient had a PTEN SNV (c.697C>T p.R233*) as well as CNA involving PTEN and a TSHR SNV (c.1897G>T p.D633Y).
Four of five (80%) of these cases were minimally invasive; the case that was widely invasive was the one with two different DICER1 mutations and the VHL, PTEN and TP53 CNA. Since molecular testing was performed on a research basis, we do not know whether any of the DICER1 mutations in our study were somatic or in the germline and thus syndromic.
Ten tumors in the P-PTC group came from 10 patients with autoimmune thyroid disease. Seven (all female) had Hashimoto thyroiditis and six had GF [three with ETV6-NTRK3, two with STRN-ALK, and one with CCDC6(PTC1)-RET], while the other patient with Hashimoto's had a BRAFV600E SNV. Three patients had Graves' disease (two female, one male). One received radioactive iodine (RAI) five years earlier as definitive therapy for the treatment of Graves' disease. This patient was one of the two who had BRAFV600E SNVs. In comparison, only a single patient in the RT-induced group had a prior diagnosis of hypothyroidism.
Discussion
In this retrospective study, we characterized and compared the molecular profiles of pediatric RT-induced DTC in childhood cancer or BMT survivors, with pediatric primary DTC. We identified an increased frequency of GF in RT-induced PTC cases compared with P-PTC cases. We also observed an increased frequency of CNA in RT-induced FTC compared with P-FTC, which uniformly carried SNV. Lastly, we identified an exceedingly rare ROS1 fusion in a child with RT-induced PTC.
The majority of what we know about the molecular genetics of DTC has come from adult studies given the relative rarity of pediatric DTC. In general, about 70% of adult P-PTC harbor point mutations, while GF are identified in ∼15% of cases (10% RET, 2–3% BRAF, 2% NTRK1/3, 2% ALK, 5% THADA, 1% PPARG) (21). In contrast, we know that childhood DTC are more likely to harbor GF than adults, with frequencies of >50% reported in multiple studies (22).
In this study, 86% (6/7) of RT-induced PTC cases harbored a GF as compared with 56% (14/25) of P-PTC. Consistent with our findings, GF were observed in 84% of PTC in children living in the vicinity of Chernobyl at the time of the nuclear accident (15). GF were also noted to be the most common genetic alteration, although less prevalent, in a recent, cohort of primarily pediatric P-PTC, occurring in 56% of cases (52/93) (23), similar to our observations. Therefore, our findings further support the conclusion that pediatric PTC are more likely to demonstrate GF than PTC in adults, but interestingly they also suggest that RT-PTC in children may be more likely to harbor GF than pediatric primary (sporadic or syndromic) cases.
One explanation for the higher prevalence of GF in pediatric RT-PTC may be related to the promotion of proximity-dependent oncogenic fusion events. Radiation is a well-established inducer of DNA double-stranded breaks, which introduces the potential for aberrant chromosomal recombination, including GF (24). The propensity for this to occur is believed to increase in the thyroid follicular cell, as the gene loci participating in fusion events lie in close proximity spatially during the interphase promoting intra- and interchromosomal rearrangements (25).
Genes on the same chromosome (intrachromosomal) have a greater chance of fusing together, which has been suggested to govern RET-PTC rearrangements in PTC (26,27), but spatial proximity may also play a role in certain interchromosomal NTRK rearrangements (28). Conversely, given that thyroid cancers began to manifest in children four to five years after Chernobyl, it may be that these GF had already spontaneously occurred in the thyroid follicular cells but radiation induced those cells to proliferate (24).
Although we hypothesized that intrachromosomal rearrangements would have been more common than interchromosomal rearrangements in our RT-induced tumors, that was not the case, as 3 (60%) of the 5 GFs in our RT patients were interchromosomal [involving 2 different chromosomes: t(2;15)(p21;q25.3) for the 2 EML4-NTRK3 GFs, and t(1;6)(p34.2;q22.1) for CCDC30-ROS1] while the 2 STRN-ALK GFs (40%) were intrachromosomal (fusing ALK at 2p23.2 with STRN at 2p22.2), whereas 10 (71.4%) of the 14 GFs in the primary PTCs actually had intrachromsomal rearrangements (CCDC6 a.k.a. PTC1 or H4 at 10q21.2 or NCOA4 a.k.a. PTC3 or ELE1 at 10q11.22 were fused with RET at 10q11.21 in a total of 5 cases, plus the 2 cases of STRN-ALK GFs, and 1 case each fusing either TPM3 at 1q21.3 or TPR at 1q31.1 with NTRK1 at 1q23.1, and 1 case fusing MKRN1 at 7q34 with BRAF at 7q34); only the 4 ETV6-NTRK3 GF resulting from t(12;15)(p13.2;q25.3) were interchromosomal.
The most common GF detected in our study included known oncogenes NTRK1/3, ALK, and RET. NTRK fusions have been reported in both RT-induced and sporadic forms of pediatric PTC (22). ETV6-NTRK3 was observed at a frequency of 14.5% (9/62) in a cohort of post-Chernobyl radiation-induced PTC compared with only 2% in a comparative cohort of sporadic cases (29). Further, the authors of this study were able to induce ETV6-NTRK3 in thyrocytes exposed to ionizing radiation in vitro, suggesting that this GF may be a mechanism of radiation-induced carcinogenesis (26). In contrast, ETV6-NTRK3 was only observed in P-PTC in our study and was not identified in any RT-induced cases.
We also identified a much higher frequency of NTRK fusions in P-PTC cases at 24% (6/25), a figure consistent with frequencies of 18% and 26% reported in recent pediatric cohorts of sporadic PTC (23,30). While we identified NTRK fusions in 29% (2/7) of RT-PTC, both were EML4/NTRK3: one in a FV-PTC, the other in a classic PTC. EML4/NTRK3 has been reported in adult FV-PTC as well (31).
ALK fusions were detected in 29% (2/7) of RT-PTC and 4% of P-PTC (all STRN-ALK) in our cohort. STRN-ALK was previously reported in childhood PTC related to the Chernobyl accident (24). While rarely reported in adult PTC (14), STRN-ALK fusions were also reported with a frequency of 6.5% in a large cohort of pediatric patients with sporadic PTC (23).
Similarly, a reported frequency of 7% occurred in a cohort of children and young adults, as compared with a frequency of <1% in adults (32), suggesting that ALK fusions may be more prevalent in pediatric PTC. Reports in adults have historically been associated with radiation exposure (33); however, this does not seem to be the case in children.
The RET fusions are well-established drivers in radiation-induced PTC in children, with reported frequencies of 36–87% in various studies (30). The RET fusions have been associated with more extensive disease, including spread to lymph nodes, extra-thyroidal extension, and metastasis (30,34). Consistent with these finding, the single RET fusion identified in the RT-exposed group in our study was a stage 4 tumor with extensive nodal disease.
Notably, NTRK, ALK, ROS1, and RET fusions are potential therapeutic targets in the case of recurrent or metastatic disease (35 –38). For patients who are refractory to RAI, tyrosine kinase inhibitors have been shown to improve progression-free survival in adults (39).
We also evaluated four RT-induced and five primary cases of FTC. Interestingly, 75% of RT-FTC demonstrated CNA and no SNV were detected. In contrast, all five (100%) of P-FTC had SNV. Two (40%) of the P-FTC additionally had CNA. The CNA gains occur via genetic amplification or chromosomal instability and aneuploidy (extra chromosome) with the potential for increased protein expression and activation of downstream signaling (40), while losses arise from deletions of chromosomal material.
Specifically, gains of genes encoding receptor tyrosine kinases ultimately increase phosphorylation and activation of the PI3K/Akt pathway in FTC (41). The CNA occur in about 60% of adult FTC (21), and a higher frequency of CNA is observed in FTC compared with PTC (42). The frequency of CNA in pediatric FTC is not clear as FTC are rare and understudied, with less than 100 characterized cases (9). Further, the vast majority of radiation-induced DTC are PTC (43), making it difficult to elucidate the genetic landscape specific to RT-FTC.
An association between radiation exposure and FTC is also less clear than in PTC, despite both arising from the same thyroid follicular cell. Therefore, the significance of the high frequency of CNA in a small number of RT-induced FTC compared with a small number of P-FTC observed in this study is not entirely clear and warrants further study. However, our observations provide an important addition to the significantly limited literature.
Worthy of additional comment is the finding of an exceptionally rare CCDC30-ROS1 fusion in an RT-induced PTC. The sequence on each side of the CCDC30-ROS1 fusion junction joining exon 10 of CCDC30 with exon 36 of ROS1 is shown in Figure 4. This patient was diagnosed with PTC at age 11. She had a history of Wilms tumor involving the left kidney, with metastasis to the left lung at age 4 for which she was treated with dactinomycin, vincristine, and doxorubicin and RT to the whole lung, left flank, and partial liver (19.5 Gy) followed by focal liver boost (26.4 Gy). Seven years from the completion of RT, a 1 cm right thyroid nodule was palpated on physical exam. Post-total thyroidectomy with central and right lateral lymph node dissections revealed a 2.4 cm PTC (pT2N1b).
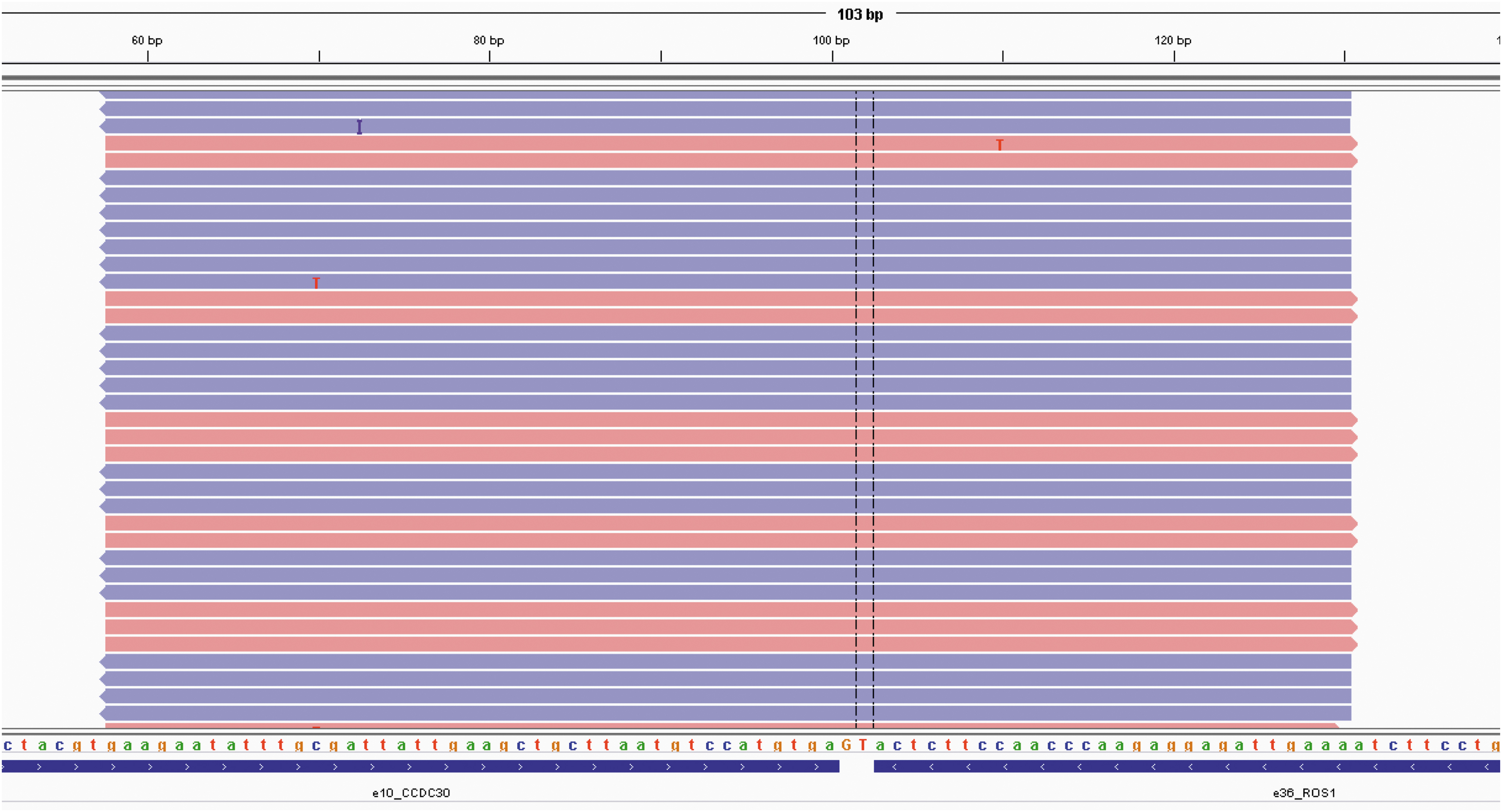
IGV screenshot showing the sequence on each side of the CCDC30-ROS1 fusion junction joining exon 10 of CCDC30 with exon 36 of ROS1. Because fusion breakpoints are typically intronic, we look for fusions at the RNA (cDNA) level, which shows the expressed result of the product. Color images are available online.
The ROS1 fusions are not uncommon in lung cancer but to our knowledge have only been reported twice in DTC: once in a 24-year-old female with a locally aggressive (pT4aN1b) solid variant PTC, with CCDC30-ROS1 fusion (44), and the other, a 50-year-old female with a 2.2 cm classic PTC with invasive disease (pT3bN1a) and EZR (exon 10)-ROS1 (exon 34) fusion (45).
In regard to clinical characteristics, DTC occurred ∼1 year later in the RT-induced group compared with the primary tumor group. This may reflect the long latency period seen in those with RT-induced DTC. In contrast to the sporadic forms and background cancer rates that demonstrate a female predominance (9), the sex distribution in the subsequent malignant neoplasm group was 50% female. Interestingly, thyroid lesions detected in the RT group were smaller in size, emphasizing the need for a high index of suspicion for a subsequent DTC in this patient population no matter the size of a thyroid nodule.
Also, the RT-induced tumors were not more advanced than those in the primary tumor group, which may also reflect the more aggressive surveillance practices, particularly screening ultrasounds, for childhood cancer and BMT survivors with a history of RT. Ultrasound surveillance in this group likely detects cancer earlier than sporadic cases that are diagnosed once a nodule/mass is detected on exam or on imaging for autoimmune thyroid disease or an unrelated other reason.
The strength of this study is the molecular profile of a cohort of pediatric patients with subsequent DTC after therapeutic radiation, which adds significantly to the current literature, particularly with respect to RT-induced FTC.
However, this study has limitations. First, the primary tumor group consisted mostly of the most recent patients diagnosed at our institution with DTC; therefore, there may be a selection bias, although the distribution of genomic alterations we identified were similar to previous reports on pediatric DTC. Our study is further limited by the small sample sizes, which prohibited adequate power to identify statistically significant differences between groups. Larger cohorts are needed to better characterize the genetic landscape of subsequent RT-induced DTC in childhood cancer survivors.
In conclusion, we identified a high prevalence of GF in RT-induced PTC and a high prevalence of CNA in RT-induced FTC compared with sporadic cases in pediatric patients, indicating that this late effect of childhood cancer treatment may be characterized by specific genomic signatures. These findings may lead to an improved understanding of patients most at risk for this late effect and identify important diagnostic, prognostic, and therapeutic factors in pediatric DTC.
Footnotes
Authors' Contributions
J.H., D.N., K.B., A.W., and K.S. participated in writing the article; reviewed it; and revised its intellectual and technical content.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a Learner's Research Fund grant at Phoenix Children's Hospital awarded to Jennifer Hess.