
Abstract
Background:
Illness severity in patients infected with COVID-19 is variable.
Methods:
Here, we conducted an observational, longitudinal, and prospective cohort study to investigate serum thyroid hormone (TH) levels in adult COVID-19 patients, admitted between June and August 2020, and to determine whether they reflect the severity or mortality associated with the disease.
Results:
Two hundred forty-five patients [median age: 62 (49–75) years] were stratified into non-critical (181) and critically ill (64) groups. Fifty-eight patients (23.6%) were admitted to the intensive care unit, and 41 (16.7%) died. Sixteen (6.5%) exhibited isolated low levels of free triiodothyronine (fT3). fT3 levels were lower in critically ill compared with non-critical patients [fT3: 2.82 (2.46–3.29) pg/mL vs. 3.09 (2.67–3.63) pg/mL, p = 0.007]. Serum reverse triiodothyronine (rT3) was mostly elevated but less so in critically ill compared with non-critical patients [rT3: 0.36 (0.28–0.56) ng/mL vs. 0.51 (0.31–0.67) ng/mL, p = 0.001]. The univariate logistic regression revealed correlation between in-hospital mortality and serum fT3 levels (odds ratio [OR]: 0.47; 95% confidence interval [CI 0.29–0.74]; p = 0.0019), rT3 levels (OR: 0.09; [CI 0.01–0.49]; p = 0.006) and the product fT3 × rT3 (OR: 0.47; [CI 0.28–0.74]; p = 0.0026). Serum thyrotropin, free thyroxine, and fT3/rT3 values were not significantly associated with mortality and severity of the disease. A serum cutoff level of fT3 (≤2.6 pg/mL) and rT3 (≤0.38 ng/mL) was associated with 3.46 and 5.94 OR of mortality, respectively. We found three COVID-19 mortality predictors using the area under the receiver operating characteristic (ROC) curve (AUC score): serum fT3 (AUC = 0.66), rT3 (AUC = 0.64), and the product of serum fT3 × rT3 (AUC = 0.70). Non-thyroidal illness syndrome (fT3 < 2.0 pg/mL) was associated with a 7.05 OR of mortality ([CI 1.78–28.3], p = 0.005) and the product rT3 × fT3 ≤ 1.29 with an 8.08 OR of mortality ([CI 3.14–24.2], p < 0.0001).
Conclusions:
This prospective study reports data on the largest number of hospitalized moderate-to-severe COVID-19 patients and correlates serum TH levels with illness severity, mortality, and other biomarkers to critical illness. The data revealed the importance of early assessment of thyroid function in hospitalized patients with COVID-19, given the good prognostic value of serum fT3, rT3, and fT3 × rT3 product. Further studies are necessary to confirm these observations.
Introduction
SARS-CoV-2
The SARS-CoV-2 spike protein uses the angiotensin-converting enzyme 2 (ACE-2) as a receptor and thyroid surgical specimens have a high level of ACE-2 mRNA, making it a potential target for the SARS-COV-2 (11). In May 2020, the first SAT case after a SARS-CoV-2 infection was reported (12). A subsequent study that analyzed fifty COVID-19 patients' records found that 56% had low thyrotropin (TSH) serum levels and that the decreases in TSH and total triiodothyronine levels correlated positively with the severity of the disease. These abnormal thyroid function parameters are suggestive of NTIS (13). In another study, 85 COVID-19 patients admitted to the intensive care unit (ICU) had clinical SAT sign, and 15% had suppressed serum TSH and elevated free thyroxine (fT4) levels (14).
Just as with any other severe illness, TH levels may be abnormal in COVID-19 patients, with predominantly a reduction in serum triiodothyronine (T3) (serum thyroxine [T4], may be decreased as well) and an elevation in reverse triiodothyronine (rT3) levels (15 –19). This combination in the setting of a life-threatening disorder that depends on the support of vital organ function is known as NTIS. The reduction in serum T3 levels is due to decreased thyroidal secretion and slower conversion of T4 to T3, whereas the elevation in rT3 levels is usually caused by a slower clearance rate and, in some cases, accelerated inner ring deiodination of T4 (16). These changes in TH economy might have a decisive role in the earliest phase of critical illness and routinely reflect the illness' severity (7,8,10,15). In the case of COVID-19 patients, the drop in serum T3 could also have prognostic function given that T3 modulates lung function and alveolar drainage (20 –22), and cellular immunity (17,23).
In the specific case of COVID-19 patients, the increased levels of cytokines and glucocorticoids, from either endogenous or exogenous sources, are potential mediators of thyroid axis suppression (24). Indeed, it has been reported that in COVID-19 patients there is an association between low free triiodothyronine (fT3) and disease severity, 28-day mortality rate, and hospitalization expenses in ICU (8 –10). However, these studies were limited by the small cohort size, criteria definition for NTIS, for being retrospective analyses, and inconsistency as to when thyroid function tests were obtained (25 –27).
While the COVID-19 epidemic in Brazil grows, details of its clinical characteristics remain poorly understood. Early recognition of patients at a high risk of developing serious illness is essential to improve disease outcomes (28,29). Here, we investigated changes in TH economy and the incidence of NTIS in SARS-CoV-2 patients admitted to a tertiary hospital and whether there is an association between TH levels with serum pro-inflammatory biomarkers and COVID-19 severity and mortality.
Methods
Subjects and data collection
An observational, longitudinal, and prospective cohort study was conducted between June and August 2020, and we enrolled 245 consecutive patients with confirmed COVID-19 admitted to the Metropolitan Hospital Dom José Maria Pires, a tertiary referral hospital in João Pessoa, Paraíba, Brazil (Fig. 1). A written consent form was obtained from the participants or legal representative. The study was approved by the Human Research Ethics Committee of the Lauro Wanderley University Hospital (CAAE:31562720.9.0000.5183).

Flowchart of the study.
Inclusion and exclusion criteria
All patients tested positive for SARS-CoV-2 using the quantitative real-time reverse-transcriptase-polymerase chain reaction (rRT-qPCR) with samples from the respiratory tract and, in cases of negative rRT-qPCR, using clinical, radiological (ground-glass opacities, with or without consolidation, located near visceral pleural surfaces, and multifocal bilateral distribution—CO-RADS 5) (30), and serological (IgG positive for SARS-CoV-2) criteria. The rRT-PCR kit used Biomol OneStep/COVID-19, IBMP, Paraná, Brazil. Patients with a history of thyroid disease, diagnosis of pregnancy, and who used iodinated contrast in the past six months or drugs that interfere with thyroid metabolism were excluded.
Outcomes
The primary goal of the study was to determine the incidence of NTIS (serum fT3 levels <2.0 pg/mL, fT4 and TSH levels within or below the normal reference ranges) in consecutive SARS-CoV-2 patients admitted to a tertiary hospital specialized in COVID-19. Additional exploratory analyses to study the predictive value of NTIS and serum TH levels were collected during the first 48 hours of admission, for disease severity and patient mortality.
Procedures
The detailed clinical information of each patient was obtained by physicians using a standard questionnaire. Two severity scoring systems were used on admission: (i) the quick Sepsis-related Organ Failure Assessment, (ii) the National Early Warning Score 2. Patients underwent chest computed tomography (CT) at hospital admission to investigate a suspected SARS-CoV-2 pneumonia. In all cases, a semi-quantitative CT severity score proposed by Pan et al. (31) was calculated for each of the five lobes, considering the extent of anatomical involvement.
All cases were divided into two clinical classifications: severe and critical. Severe (non-critical) cases were classified for patients who met any of the following criteria: respiratory rate >30 cycles/min, oxygen saturation <93% at rest, partial arterial pressure of oxygen (PaO2)/concentration of oxygen (FiO2) <300 mmHg (1 mmHg = 0.133 kPa), and extent of lung injury (ground-glass opacity) estimated >50%. Critical cases were considered for patients who meet any of the following criteria: manifestation of respiratory failure requiring mechanical ventilation, presence of shock, and other organic failures that need follow-up and treatment in an ICU. For patients who met the inclusion criteria, blood samples were collected before interventions or therapy that could potentially interfere or alter TH or cytokines serum levels, always performed within the first 48 hours of admission.
Serum biochemistry
The complete blood cells count, and measurement of the lymphocyte and neutrophils subpopulations were measured by using a hematological analyzer MEK-7300 (Nihon Kohden®, Tokyo, Japan). Alanine transaminase (ALT), aspartate aminotransferase, creatinine, high-sensitive C-reactive protein (CRP), D-dimer and lactate dehydrogenase (LDH), thyroid function (fT3, fT4, rT3, TSH), thyroglobulin, anti-thyroid peroxidase antibodies, interleukin 6 (IL-6), and ferritin were measured by chemiluminescence immunoassay (MAGLUMI-2000-PLUS; Shenzhen New Industries Biomedical Engineering Co., Shenzhen, China) according to the manufacturer's protocol.
Statistical analyses
A statistical power analysis was performed for sample size estimation. The effect size in this study was conservatively selected at the f2 = 0.10. With an alpha = 0.05 and power = 0.95, the projected sample size needed with this effect size using GPower 3.1.9.7 is approximately N = 158 for a linear regression analysis with two predictors. Thus, our sample size of 245 was more than adequate for the primary outcome of this study and should also allow for expected attrition. The data were expressed as median ± interquartile range. Mann–Whitney, Chi-square, or Fisher's test were used for non-parametric variables. To assess the relative risk of mortality, we used univariate and multivariate logistic regression. We evaluated each variable as a potential biomarker by using receiver operating characteristic (ROC) curves. The significance level of p < 0.05 was accepted as statistically significant. The statistical program GraphPad Prism, v.7.00 (2016), was used to perform statistical tests.
Results
Two hundred seventy-four adult patients consecutively admitted with COVID-19 were considered for potential enrollment in the study, and after assessment of inclusion and exclusion criteria, 245 were enrolled (Fig. 1). The median age was 62 (49–74.5) years, and 145 patients (59.1%) were males. The average hospital stay was 8.3 days. Fifty-eight patients (23.6%) were admitted to the ICU, of whom 41 (16.7%) later died. Table 1 summarizes baseline sociodemographic and clinical characteristics.
Demographic and Clinical Characteristics of the Cohort in Patients Non-Critical and Critical and Their Association with Mortality
Low TSH = TSH <0.4 mIU/L; high fT4 = fT4 > 1.7 ng/dL; high thyroglobulin = thyroglobulin >59.9 ng/mL; NTIS = serum fT3 levels <2.0 pg/mL, fT4, and TSH levels within or lower than the normal ranges at diagnosis; high rT3 = rT3 > 0.35 ng/mL. Mann–Whitney test was performed for continuous variables (age, NEWS2, qSOFA and CT COVID score) while Fisher's exact test was performed for all other variables.
CT, computed tomography; fT3, free triiodothyronine; fT4, free thyroxine; ICU, intensive care unit; IQR, interquartile range; NEWS2, National Early Warning Score 2; NTIS, non-thyroidal illness syndrome; qSOFA, quick Sepsis Related Organ Failure Assessment; rT3, reverse triiodothyronine; TPOAb, thyroperoxidase antibodies; TSH, thyrotropin.
TH levels
On admission (first 48 hours), 54 (22.0%) patients presented with normal serum TSH, fT3, fT4 and rT3 levels. The remaining 191 patients exhibited multiple alterations in TH levels, which could be stratified in two major groups: (i) 154 (62.8%) patients with elevated serum rT3 levels, of whom 31 and 18 also had elevated or reduced serum fT4 levels, respectively; (ii) 18 individuals with isolated high serum fT4 levels (Fig. 2A, B). A smaller number of individuals (n = 16) exhibited low serum fT3 levels associated with fT4 and TSH levels within or lower than normal range, which were in most cases (n = 11) associated with high serum rT3 levels. Lastly, there were 15 individuals with suppressed serum TSH and elevated serum rT3 levels (Fig. 2). None of the patients enrolled exhibited clinical signs of hypothyroidism or thyrotoxicosis.

Venn diagram with the main TH levels alterations distribution observed in 191 COVID-19 hospitalized patients with abnormal results at admission and relationship with disease mortality rate. (
The utilization of clinical and biochemical criteria led us to stratify all 245 patients, within the first 48 hours, into 181 non-critical and 64 critically ill patients (Table 2). Whereas serum TSH and fT4 serum levels were similar in both groups, critically ill patients exhibited lower serum fT3 and high-normal rT3 levels, which, although elevated, were not as high as compared with non-critical patients (Fig. 3 and Table 2).

TH levels, biochemical and hemocromocytometric parameters in 245 critically and non-critically ill COVID-19 hospitalized patients during the first 48 hours of admission. Gray areas in plots represent normal reference ranges. Statistics used: Mann–Whitney test. ALT, alanine transaminase; Anti-TPO, anti-thyroid peroxidase; AST, aspartate transaminase; CRP, C-reactive protein; fT3 × rT3, the product of fT3 and rT3; IL-6, interleukin 6; LDH, lactate dehydrogenase; N/L ratio, neutrophil-lymphocyte ratio.
Variables Measured in Non-Critical and Critical and Their Association with Mortality
ALT, alanine transaminase; AST, aspartate transaminase; 95% CI, confidence interval; CRP, C-reactive protein; IL-6, interleukin 6; N/L ratio, neutrophil-lymphocyte ratio; OR, odds ratio.
Clinical outcome
Of the 245 enrolled patients, 41 patients died of COVID-19 complications about 13 days later. This is in contrast with the group of survivors who were discharged about six days after admission (Table 1). Based on these numbers, we asked how well different clinical and biochemical parameters obtained in the first 48 hours of admission predicted the clinical outcome. The parameters included length-of-stay, ICU admission, CT COVID score, use of vasoactive drugs, and unspecific markers of inflammation (Tables 1 and 2). We used univariate logistic regression analysis and found that among the 11 markers of inflammation, tissue damage, or blood count parameters, 8 were predictors of disease severity and prognosis of mortality: IL-6, D-dimer, LDH, albumin, CRP, neutrophils, neutrophil-lymphocyte ratio, and hemoglobin (p < 0.05) (Fig. 3). The Fisher's exact test confirmed higher mortality risk for all these same markers (Tables 2 and 3).
Variables Analyzed as Potential Biomarkers for Mortality: Receiver Operating Characteristic Curve
AUC, area under the curve; LDH, lactate dehydrogenase; ROC, receiver operating characteristic.
Next, we asked whether TH levels obtained on admission could predict clinical outcomes and, if so, how well they compared with the classical predictors assessed above. Using the univariate logistic regression, serum levels of fT3, rT3 and the product fT3 × rT3 showed strong correlation with disease severity and prognosis of mortality (Table 2). Unexpectedly, the fT3/rT3 ratio did not yield statistically significant predictive power (Table 2). Figure 4A shows TSH, fT4, fT3, rT3, and fT3 × rT3 results among survivor and non-survivor patients. We also plotted an ROC curve, to calculate the mortality predictive power of each parameter. The top parameters based on the area under the curve (AUC >0.65) were the product fT3 × rT3, followed by N/L ratio, CRP, neutrophil count, and serum fT3 (Table 3 and Fig. 4B). Next, using the cutoff value for each parameter we calculated the odds ratio (OR) of mortality using the Fisher's exact test. The parameters with top ORs included the product fT3 × rT3, followed by CRP, neutrophil count, serum fT3 and N/L ratio (Table 3). Notably, some parameters with a low ROC AUC exhibited a significant OR of mortality, that is, serum rT3, IL-6, albumin, and D-dimer (Table 3).
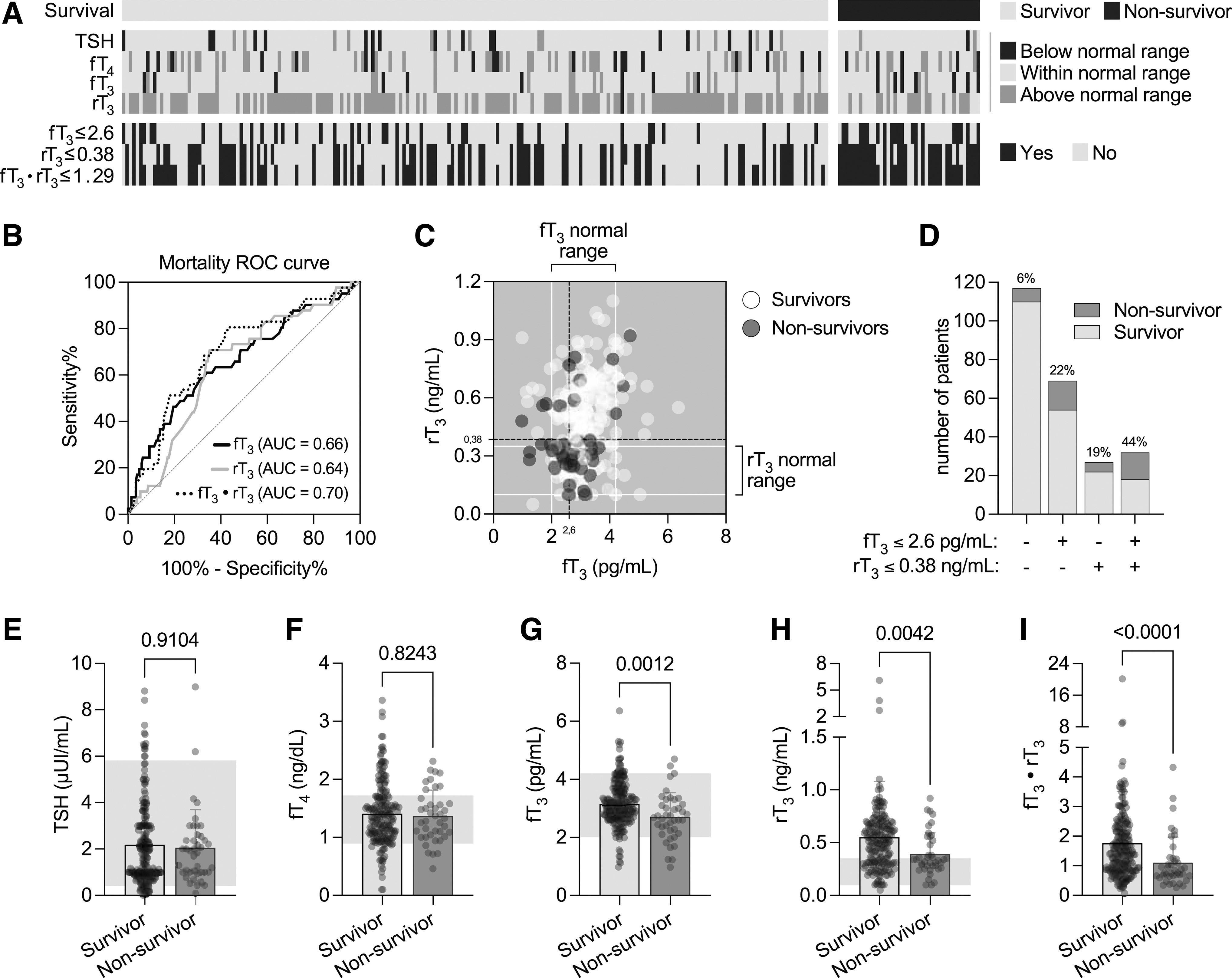
TH levels of 245 COVID-19 hospitalized patients collected during the first 48 hours of admission.
We next used univariate and multivariate regression analysis to calculate the mortality OR by using cutoff values obtained from the ROC curve (Table 4). Whereas serum TSH, fT4, and fT3/rT3 values did not yield a significant OR, we observed that serum fT3, rT3, and fT3 × rT3 yielded highly significant ORs (Table 4). We noticed that the calculated cutoff value for serum fT3—based on the ROC curve—was 2.6 pg/mL, which is within the normal reference range of the method used. Thus, we recalculated the univariate regression analysis by using 2.0 pg/mL (the lower limit of normal), and we obtained an even higher OR for mortality. These analyses were followed by a multivariate logistic regression analysis, which corrects the OR based on eight co-variates (Table 4). The resulting ORs were higher and followed the same pattern observed for the univariate analysis.
Univariate and Multivariable Regression Analyses Between Thyroid Function and Variables
Adjusted for age, neutrophil ( × 103 cells/μL), N/L ratio, albumin, high-sensitivity CRP, LDH, D-dimer and IL-6.
Next, the mortality rates was bubble plotted considering the rT3 and fT3 serum levels. It is notable that survival and shorter length of stay segregated with normal serum T3 and rT3 levels, whereas mortality and longer length of stay segregated with high serum rT3 levels (Fig. 4C). A bar graph of the same data also illustrates these points (Fig. 4D). In addition, Figure 4E–I show differences in TSH, fT4, fT3, rT3, and fT3 × rT3 values among survivor and non-survivor patients.
Discussion
To our knowledge, this is the largest prospective study of hospitalized patients with COVID-19 whose TH serum levels were assessed, including serum TSH, fT4, fT3, rT3, and Tg levels. An elevation in serum rT3 levels was the most frequent alteration observed in these patients (∼63%), followed by high serum fT4 (∼21%) and low serum TSH levels (∼7.3%). Unexpectedly, NTIS were only observed in ∼6.5% patients. No patients exhibited clinical signs or symptoms of SAT, despite that 5.3% of patients exhibited an elevation in serum Tg levels. Remarkably, serum fT3, rT3 and the product fT3 × rT3 exhibited substantial predictive value for disease severity and mortality, with the product fT3 × rT3 performing slightly better than classical parameters such as D-dimer, LDH, albumin, CRP, ALT, neutrophil count, neutrophil/lymphocyte (N/L) ratio, and hemoglobin levels.
Only two studies (total of 482 patients) (10,32) prospectively investigated the hypothesis that serum TH levels in COVID-19 patients could serve as biomarkers of maladaptive response and unfavorable outcomes. In one study, a cohort of 367 Chinese mild-to-moderate COVID-19 patients revealed that 16.9% of patients had abnormal thyroid function test. Serum rT3 was not evaluated, but serum fT3 was obtained in 367 patients and NTIS was identified in 27 (7.4%) patients, although 75.2% had mild disease (10). More recently, an Italian longitudinal prospective observation study of severely ill COVID-19 patients found that 20 of 115 patients (9%) had low serum fT3 levels (32). Notably, both studies concluded that reduced fT3 serum levels are associated with adverse outcomes, for example, inflammatory response, but the impact of the studies was limited by the small sample size, the lack of statistical power, the predominance of mild or severe-illness, and the presence of confounders such as treatment drugs (Table 5) (10,32).
Prospective Studies in COVID-19 Patients Analyzing Association Between Thyroid Function Tests Measured at Admission and Disease Severity or Fatality
↓, reduced serum levels; ↑, elevated serum levels.
Univariate analysis.
Multivariate analysis.
Tg, thyroglobulin; TgAb, thyroglobulin antibodies; TRAb, thyrotropin receptor antibodies.
Indeed, Chen et al. retrospectively observed that COVID-19 patients who died had lower serum fT3 levels on admission (33). Guo et al. recently reported fT3 serum levels as a possible prognostic marker of mortality with AUC = 0.863 in 121 critically ill patients with COVID-19 (27). Another retrospective study of 287 patients identified a 20.2% prevalence of TSH below the reference range (<0.33 mU/L) and an inverse correlation between TSH and IL-6 (r = −0.41; p < 0.001). However, fT3 and fT4 levels were measured only in 73 patients among the 287 included (34). Recently, in a retrospective study, Lang et al. (35) evaluated 127 hospitalized patients and low T3 levels (<3.1 pmol/L) in the univariate Cox regression analysis, showing a strong association with in-hospital mortality (Hazard Ratio [HR] 14,607, 95% confidence interval [CI] [3873–55,081], p < 0.001).
NTIS is considered an adaptive response of the hypothalamus-pituitary-thyroid axis to severe illness, including in patients with COVID-19 (8,10,15,27,28,36). Previous studies have demonstrated that blood levels of pro-inflammatory and anti-inflammatory cytokines correlate with disease's severity and mortality (32). The release of high levels of pro-inflammatory cytokines during the acute response of critical illness could contribute to TH alterations, including the reported drop in serum fT3 (15,25). In our study, the rapid decline in the circulating fT3 serum levels (below the lower limit of the reference range) was observed in only a small percentage of patients, whereas an elevation in serum rT3 levels was frequent; it was the most common alteration in serum TH levels among hospitalized COVID-19 patients.
We found that both, the combination of low fT3 and elevated rT3 serum levels, were robustly associated with inflammatory response, disease severity, and mortality. Serum fT3 levels had good specificity reflecting low false-positive rates, indicating that it might be of practical predictive value once it can be obtained up to two to three hours after hospital entrance. Notwithstanding, the usefulness of fT3 serum levels as a biomarker needs to be further explored given that its alteration might be affected by the degree and phase of inflammatory response, by reduced levels of TH binding proteins and accelerated hormone clearance caused on SARS-COV-2 infection (8,10,27,36,37).
Progressive defect in the T4 to T3 conversion and increment in T4-binding globulin have been previously associated with low levels of serum T3 at admission and disease severity related to human immunodeficiency virus infection. Indeed, rT3 decline was associated with in-hospital mortality (38,39). To our knowledge, the prognostic value of rT3 serum levels in COVID-19 patients has not been investigated in previous studies. Although frequently elevated, patients who ultimately did not survive presented with not as high serum rT3 levels when compared with patients who survived. Consequently, here we made the novel observation that the fT3 × rT3 product exhibited the highest prognostic value of all parameters examined, including inflammation biomarkers, with a sensitivity of 80% and specificity of 57%. The mortality predictive values for serum fT3, rT3, and the fT3 × rT3 product exhibited strong agreement among univariate, multivariate, and sensitivity analyses (Chi-square, Fisher's exact and Mann-Whitney test). However, the predictive capacity of these variables was still modest (area under the ROC curve between 0.6 and 0.7), probably secondary to the homogeneity of the studied population, mainly composed of moderate-to-severe COVID-19 cases referred to a specialized COVID-19 center.
The fact that TSH serum levels remained within normal range in most patients suggests that thyroidal T4 and T3 production might not have been greatly reduced. Whereas the changes in TH serum levels have been interpreted as largely adaptive, it is conceivable that in this situation they might play an expanded role. For example, TH has multiple effects on lung physiology, including alveolar type II cells function and control of in vivo alveolar fluid clearance (AFC) (20,40). It has been proposed that T3 directly instilled into lungs could raise AFC, supporting oxygenation and dribbling the exigency for expanded mechanical ventilation (20,21). Therefore, lower T3 availability in the acute respiratory distress syndrome context could have a negative impact in the diaphragm muscle contraction physiology and impair ventilation (41).
Pos-mortem examination in ICU patients has found that serum rT3 values correlate with reduced liver D1 and increased D3 activities (42). Notably, D3 is inducible by hypoxia-inducible factor (HIF1a), but little is known about the role of HIF in COVID-19 (43). Whereas the elevation in serum rT3 typically noted in NTIS patients is generally interpreted as the result of impaired D1-mediate clearance of rT3, D3 reactivation could be playing a role as well. The worse outcomes observed in patients with less robust elevation in rT3 levels are puzzling and could indicate a failure of D3 reactivation and/or normal D1 activity.
The limitations of this study include, first, that the analysis was limited to a hospitalized moderate-to-severe COVID-19 patients and these results may not apply to individuals with COVID-19 who are not hospitalized. Second, it is unclear whether a decrease in caloric intake, a weight loss, or a combination of these factors are the cause of decreased fT3 levels in COVID-19 critically ill patients.
In summary, this prospective study reports data on the largest number of hospitalized moderate-to-severe COVID-19 patients and correlates serum TH levels with illness severity, mortality, and other biomarkers to critical illness. The data revealed the importance of early assessment of thyroid function in hospitalized patients with COVID-19, given the good prognostic value of serum fT3, rT3, and fT3 × rT3 product. Further studies are necessary to confirm these observations.
Footnotes
Author Disclosure Statement
A.C.B. is a consultant for Synthonics, BLA technology, and Allergan. The other authors declare no conflicts of interest.
Funding Information
No funding was received.