
Abstract
Background:
High bile acid concentration is associated with adverse perinatal outcomes (i.e., stillbirth and preterm birth) and experimental studies indicate that thyroid hormone regulates bile acid metabolism, but this has not yet been translated to clinical data in pregnant women. We aim to explore the association of thyroid function with bile acid concentrations and the risk of gestational hypercholanemia.
Methods:
This study comprised 68,016 singleton pregnancies without known thyroid or hepatobiliary diseases before pregnancy and thyroid medication based on a prospective cohort. Thyroid function and serum total bile acid (TBA) were routinely screened in both early (9–13 weeks) and late pregnancy (32–36 weeks). Hypercholanemia was defined as serum TBA concentration ≥10 μmol/L. Multiple linear regression models and multiple logistic regression models were performed.
Results:
A higher free thyroxine (fT4) during both early or late pregnancy was associated with a higher TBA concentration and a higher risk of hypercholanemia (all p < 0.01). A higher thyrotropin (TSH) in early pregnancy was associated with a higher TBA concentration in early pregnancy (p = 0.0155), but with a lower TBA concentration during later pregnancy (p < 0.0001), and there was no association of TSH with hypercholanemia. Overt hyperthyroidism in late pregnancy was associated with a 2.12-fold higher risk of hypercholanemia ([confidence interval; CI 1.12–4.03], p = 0.021) and subclinical hyperthyroidism during later pregnancy was associated with a 1.5-fold higher risk of hypercholanemia ([CI 1.14–1.97], p = 0.0034). Sensitivity analyses indicated that a high fT4 throughout pregnancy was associated with a higher risk of hypercholanemia rather than only in early or late pregnancy.
Conclusions:
A higher fT4 concentration during either early or late pregnancy, but not the TSH concentration, is associated with higher TBA and a higher risk of gestational hypercholanemia. Furthermore, hyperthyroidism during pregnancy could be a novel risk factor for hypercholanemia.
Introduction
Intrahepatic cholestasis of pregnancy is a liver disorder characterized by pregnancy-specific maternal pruritus with increased serum bile acid concentrations (also known as hypercholanemia) that affects 0.3–6.1% pregnant women with a marked ethnic difference (1 –4). Bile acids facilitate biliary excretion and intestinal lipid and nutrient uptake, but supraphysiological concentrations may exert cytotoxic effects on multiple organs, for example, the liver, placenta, and fetal heart (5,6). Intrahepatic cholestasis of pregnancy is associated with an increased risk of preterm birth, stillbirth, meconium-stained amniotic fluid, fetal hypoxia, and neonatal unit admission, and the elevated level of serum bile acid reflects the severity of the disease (7,8). The synthesis and excretion of total bile acid (TBA) is tightly regulated by hepatic nuclear receptor-mediated signaling pathways (9). Under the influence of estrogen and sulfated progesterone metabolites, serum TBA concentrations typically increase with advancing gestation (10,11), but the etiology of gestational hypercholanemia as well as intrahepatic cholestasis of pregnancy remains to be fully elucidated. Risk factors for intrahepatic cholestasis of pregnancy include a personal or family history of intrahepatic cholestasis of pregnancy, multiple pregnancy, hepatobiliary pathologies such as cholelithiasis or hepatitis and various genetic mutations (12). Chinese guideline recommends an earlier screening in women with high-risk factors of intrahepatic cholestasis of pregnancy and recommends ursodeoxycholic acid as the first-line therapy for intrahepatic cholestasis of pregnancy, although its effectiveness is disputed (13). Further knowledge of the pathophysiology and clinical risk factors underlying intrahepatic cholestasis of pregnancy are required to optimize clinical risk stratification and treatment strategies.
Thyroid hormone is an important regulator of the increased metabolic demand during pregnancy (14). Experimental studies have shown that thyroid hormone stimulates the hepatic conversion of cholesterol into bile acid by inducing expression of cholesterol 7α-hydroxylase (CYP7A1), a key enzyme involved in bile acid synthesis (15,16). Cases of cholestasis presumably caused by hyperthyroidism have been reported in a neonate (17) and nonpregnant adults (18,19). However, to the best of our knowledge, there is no prospective study investigating the association of thyroid function with gestational hypercholanemia. Therefore, the aim of this study was to explore the association between maternal thyroid function and TBA and hypercholanemia during pregnancy.
Materials and Methods
Study design and participants
This prospective cohort study was performed at the International Peace Maternity and Child Health Hospital (IPMCH), a large public hospital providing secondary and tertiary care in Shanghai, China. Eligible participants were those who underwent first trimester prenatal screenings at this hospital between January 2013 and December 2018. A total of 81,524 pregnancies with antenatal examination were initially enrolled in this study. Subsequently, we excluded twin pregnancies, in vitro fertilization pregnancies, pregnant women with a history of thyroid disease or thyroid interfering drug usage, including levothyroxine, propylthiouracil, and methimazole, pregnant women with a history of any hepatobiliary disease, including history of hepatobiliary surgery, history of fatty liver and viral hepatitis, history of drug-induced liver damage, or other liver disorders during their current pregnancy. There were 68,016 pregnancies left in the final analyses for early pregnancy. After further excluding women who were diagnosed with hypercholanemia in early pregnancy and accepted treatment, and women absent in late pregnancy measurement, 66,360 pregnancies remained in the analyses in late pregnancy. Considering pregnancies of the same women correlated more heavily than pregnancies of different women, we did sensitivity analyses by excluding women (3.7%) with repeated pregnancies, which had no change on the conclusion (data not shown). Ethical approval was obtained from the IPMCH Ethics Committee (GKLW2012-49). This study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the appropriate institutional review committee. All participants provided written informed consent.
Data collection
During hospital visits, all data were prospectively collected by nurses, residents, and gynecologists with use of electronic patient files. Fasting blood samples were drawn from the median cubital vein, and the serum was separated by centrifugation within six hours. Thyrotropin (TSH), free thyroxine (fT4), and thyroid peroxidase antibody (TPOAb) concentrations were measured using the Architect i2000 immunoassay (Abbott, Chicago, USA) according to the protocol of the manufacturer. The intra- and interassay coefficients of variation ranged between 1.6% and 3.6% for TSH, 1.9–4.0% for fT4, and 10.0% for TPOAb. TBA concentrations were measured using the Cobas c702 chemistry analyzer (Roche Diagnostics, Basel, Switzerland) following the manufacturer's instructions. The intra- and interassay coefficients of variation for TBA were ≤5%.
Data on maternal age, parity, maternal education level were collected through interviews at first clinical presentation during which height and weight were also measured to calculate body mass index (BMI). Thyroid function and TBA concentrations were assessed in both early (9–13 weeks) and late pregnancy (32–36 weeks). TPOAb level of >5.6 IU/mL was defined as positive. Hypercholanemia was defined as TBA concentration ≥10 μmol/L, which was diagnosed and managed as intrahepatic cholestasis of pregnancy during clinical practice according to the intrahepatic cholestasis of pregnancy management guideline of the Chinese Medical Association of Obstetrics and Gynecology (13). Less than 0.1% of all women smoked or consumed alcohol.
Statistical analysis
A multiple linear regression model was used to investigate the association of TSH or fT4 with TBA and TBA/cholesterol ratio. To fulfill model assumptions TBA concentrations and ratio of TBA/cholesterol were logarithmically transformed as ln (TBA +1) and ln (TBA/cholesterol ratio), with figures showing back-transformed values for clinical interpretation purposes. Nonlinearity was assessed through restricted cubic splines with three knots at the 10th, 50th, and 90th percentiles. We used multiple logistic regression models to study the association of TSH and fT4 with hypercholanemia. We further divided the population into three tertile groups according to cholesterol levels to explore the relationship between fT4 and hypercholanemia at different cholesterol levels. Euthyroid and thyroid disease entities in early and late pregnancy were defined by trimester-specific and population-based cutoff values using the 2.5th and 97.5th percentile (11.7 and 19.4 pmol/L for fT4 in early pregnancy, 9.0 pmol/L to 14.1 fT4 pmol/L for late pregnancy, 0.016 and 3.53 mU/L for TSH in early pregnancy, 0.39 and 3.67 mU/L for TSH in late pregnancy) in TPOAb negative women. Multiple regression models were adjusted for potential confounders such as maternal age, BMI, parity, education level and pre-eclampsia based on biological plausibility, identification of a variable as a confounder in previous studies (20), change of the effect estimates of interest, and/or reduction in the residual variability of the outcome. For confounders with missing data, multiple imputations according to the Markov chain Monte Carlo method were used (21). Five imputed data sets were created and pooled for analyses. No significant differences in descriptive characteristics were found between the original and imputed data sets. All statistical analyses were performed using R statistical software version 3.6.1 (packages rms, visreg, mice, and mass) (22).
Results
After exclusions, the final study population comprised 68,016 women (Fig. 1), the basic characteristic of which are shown in Table 1. The median (95% range) TSH and fT4 were 1.17 (0.02–3.69) mU/L and 14.5 (11.6–19.4) pmol/L during early pregnancy (9–13 weeks), and were 1.45 (0.39–3.56) mU/L and 11.3 (9.0–14.2) pmol/L during late pregnancy (32–36 weeks), respectively. The median (95% range) serum TBA was 1.9 (0.6–5.7) μmol/L during early pregnancy, and was 3.2 (1.1–9.4) μmol/L during late pregnancy, respectively. There were 1896 (2.8%) pregnant women with hypercholanemia.
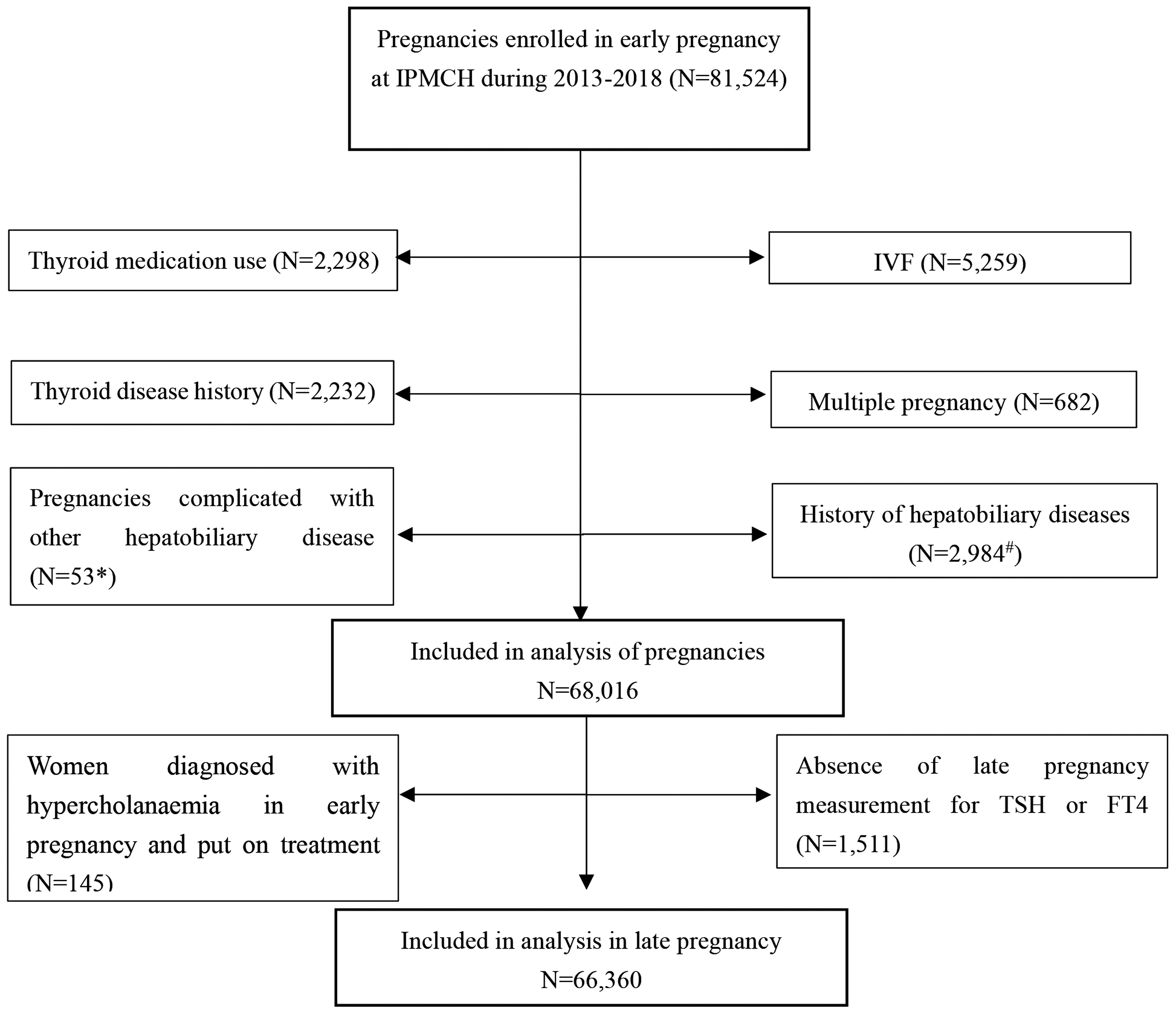
Study population flowchart. *Including gallbladder disease, autoimmune liver disease, acute fatty acid liver disease, and HELLP syndrome. #Including history of hepatobiliary surgery, history of fatty liver and viral hepatitis, and history of drug-induced liver damage. Gestational weeks for TBA/thyroid function screening were 9–13 weeks in early pregnancy and 32–36 weeks in late pregnancy. fT4, free thyroxine; HELLP syndrome, hemolytic anemia, elevated liver function and low platelet count syndrome; IPMCH, International Peace Maternity and Child Health Hospital; TBA, total bile acid; TSH, thyrotropin; IVF, in vitro fertilization.
Population Characteristics
Gestational weeks for TBA/thyroid function screening were 9–13 weeks in early pregnancy and 32–36 weeks in late pregnancy.
BMI, body mass index; fT4, free thyroxine; TBA, total bile acid; TSH, thyrotropin.
Thyroid function and TBA concentrations as well as hypercholanemia
As shown in Figure 2, there was a positive association of fT4 in early and late pregnancy with TBA concentration in late pregnancy (p < 0.0001). There was also a positive association of fT4 in early and late pregnancy with gestational hypercholanemia (Fig. 3; p = 0.0004 for early pregnancy and p = 0.003 for late pregnancy, respectively). Although TSH in late pregnancy was negatively associated with TBA concentration (Fig. 2; p < 0.0001), there was no association of TSH with hypercholanemia (Fig. 3). Subanalyses showed the change in TSH and fT4 concentration was negatively associated with TBA change; a higher fT4 was associated with a higher TBA/cholesterol ratio and the association of late pregnancy fT4 with TBA concentrations was more evident in women with a lower cholesterol (Supplementary Figs. S1–S3).
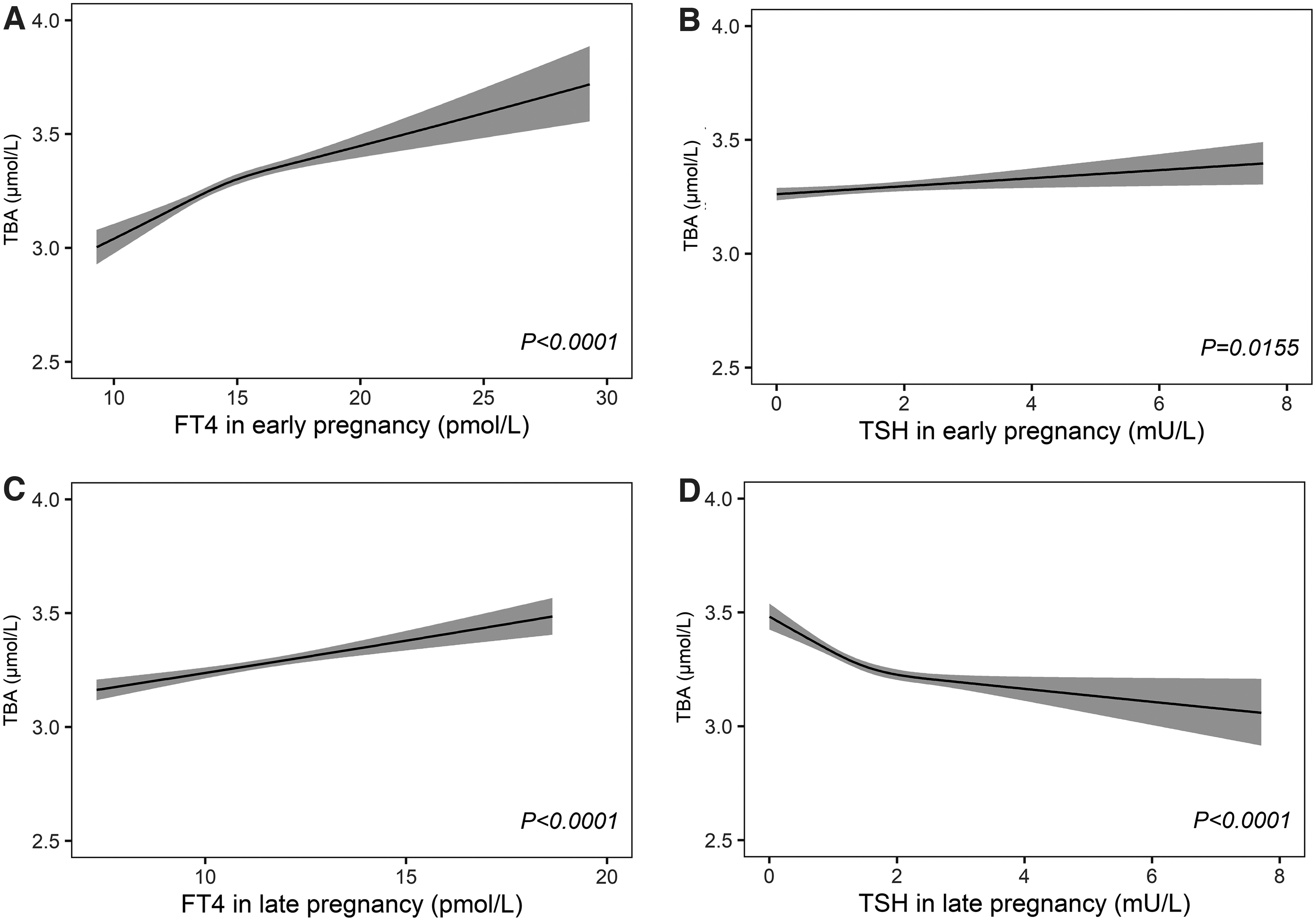
The association between thyroid hormone with TBA. (
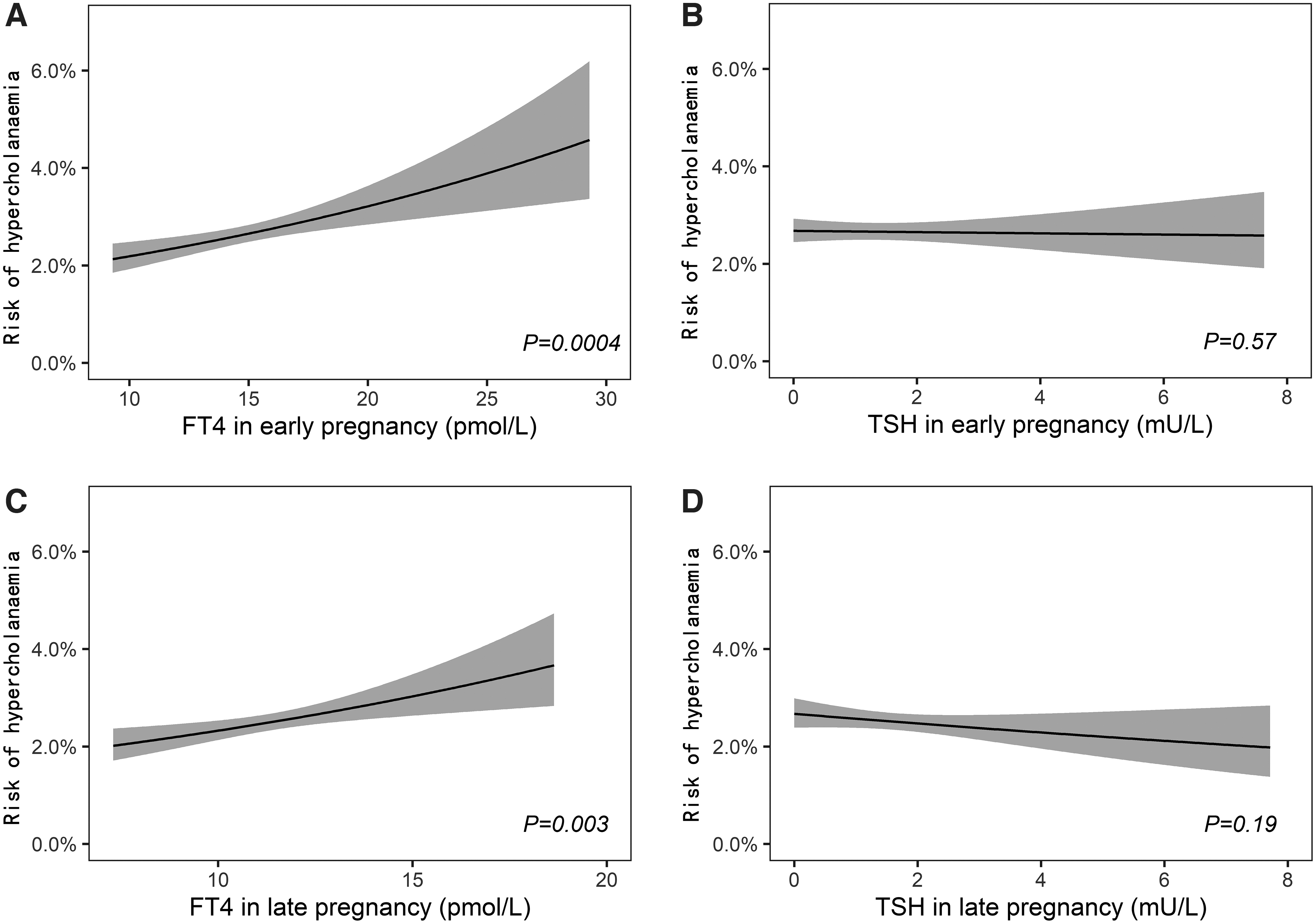
The association between thyroid hormone with risk of gestational hypercholanemia. (
Thyroid entities and hypercholanemia
We further explored whether thyroid entities were associated with hypercholanemia (Table 2). During early pregnancy, hyperthyroidism was associated with a higher risk of hypercholanemia (odds ratio [OR] 1.44 [CI 1.03–2.00], p = 0.0326) and isolated hypothyroxinemia was associated with a lower risk of hypercholanemia (OR 0.64 [CI 0.44–0.93], p = 0.018) in the unadjusted model, but these associations failed to reach statistical significance after adjustments for confounders. During late pregnancy, hyperthyroidism (OR 2.12 [CI 1.12–4.03], p = 0.0212) and subclinical hyperthyroidism (OR 1.50 [CI 1.14–1.97], p = 0.0034) were associated with a higher risk of hypercholanemia before and after adjustment.
Thyroid Entities in Early and Late Pregnancy with the Risk of Hypercholanemia
Gestational weeks for TBA/thyroid function screening were 9–13 weeks in early pregnancy and 32–36 weeks in late pregnancy. Analyses were adjusted for age, BMI, education levels, parity, and pre-eclampsia.
Women diagnosed with hypercholanemia in early pregnancy and put on treatment were excluded.
BMI, body mass index; OR, odds ratio; aOR, adjusted OR.
Persistently high or low fT4 and hypercholanemia
We further explored whether a persistent low or high fT4 concentration during early and late pregnancy was associated with hypercholanemia (Table 3). A persistently high fT4 from early to late pregnancy (fT4 in the highest 10%) was associated with an increased risk of hypercholanemia (OR 1.29 [CI 1.00–1.65], p = 0.0485), compared with fT4 in the reference group (fT4 25th–75th in both early and late pregnancy). Similarly, a persistently low fT4 from early to late pregnancy (fT4 in the lowest 10%) was associated with a lower risk of hypercholanemia when compared with the reference group (OR 0.63 [CI 0.44–0.88], p = 0.01). However, a low or high fT4 only during early or late pregnancy was not significantly associated with hypercholanemia. Similar associations for TBA concentrations are shown in Supplementary Table S1.
Persistent High or Low Free Thyroxine from Early to Late Pregnancy Is Associated with Hypercholanemia
Gestational weeks for TBA/thyroid function screening were 9–13 weeks in early pregnancy and 32–36 weeks in late pregnancy. Analyses were adjusted for age, BMI, education levels, parity, and pre-eclampsia.
Reference group was women with fT4 in 25th–75th percentile in early pregnancy.
Reference group was women with fT4 in 25th–75th percentile in late pregnancy.
Reference group was women with fT4 in 25th–75th percentile in both early and late pregnancy.
Discussion
In this study, we showed that hyperthyroidism during late pregnancy is a risk factor for gestational hypercholanemia, based on the untreated population. In line with this finding, a higher fT4 as well as subclinical hyperthyroidism was also associated with a higher risk of hypercholanemia while isolated hypothyroxinemia was associated with a lower risk of hypercholanemia. Sensitivity analyses indicated that persistently high fT4 concentrations were associated with the increased risk of hypercholanemia.
There are various causes of bile acid disorder, but we focused on pregnancy-specific bile acid disorder; therefore, this study excluded women with the pre-existing hepatobiliary disease, because their bile acid disorders caused by other mechanisms are not pregnancy specific. Similarly, to focus on the association between new-onset thyroid disease with bile acid concentration change during pregnancy, and to avoid the effect of thyroid drug on the association, women with known thyroid diseases or having received thyroid medication during pregnancy were further excluded in this study. In the analyses in late pregnancy, we did not exclude women with hypercholanemia treated in late pregnancy, because these women received treatment after TBA test in late pregnancy and their TBA concentrations were not affected by the treatment.
Intrahepatic cholestasis of pregnancy is a pregnancy-specific disease for which the etiology is not yet fully elucidated but likely to involve multiple endocrine and environmental factors as well as genetic susceptibility (23,24). Our results showed that a higher fT4 concentration or hyperthyroidism was associated with a higher TBA. These findings essentially translate the results from experimental studies and studies in nonpregnant individuals to pregnant women (25). One potential mechanism for this association is that thyroid hormone regulates the conversion of cholesterol to bile acids by enhancing human cholesterol 7 alpha-hydroxylase (CYP7A1) expression and reducing PSCK9 (25). In addition, the concomitant suppression of TSH may add to the increase in TBA as it was shown that higher TSH represses CYP7A1 activity in rats (26). The latter could also partially explain the higher risk seen especially in women with overt and even subclinical hyperthyroidism. We also showed that a higher fT4 was associated with a higher TBA/cholesterol ratio and that the association of late pregnancy fT4 with TBA concentrations was more evident in women with a lower cholesterol. These results could reflect the thyroid hormone-mediated increased activity of CYP7A1. Alternatively, these results could be explained by separate thyroid hormone effects on bile acid production and direct effects on cholesterol homeostasis [i.e., metabolism or reabsorption (25,27)]. As intrahepatic cholestasis of pregnancy and hypercholanemia are also typically associated with dyslipidemia (28), further studies are required to investigate the metabolic profile in women with combined hyperthyroidism and hypercholanemia (25).
Interestingly, sensitivity analyses suggested that it was mainly persistent low or high fT4 that was associated with the risk of hypercholanemia. fT4 concentrations change throughout gestation (14), with higher concentrations in early pregnancy due to the thyroid stimulatory properties of human chorionic gonadotropin and then decreasing toward term (29). This is opposite to the risk of hypercholanemia, which generally increases as pregnancy progresses. Most likely, the association of persistently low or high fT4 with hypercholanemia reflects potential effects of prolonged small alterations in CYP7A1 activity increasing the risk of hypercholanemia. The prolonged time of high fT4 as a risk factor also increases the chance of the occurrence of a potential second hit that could trigger mechanisms leading to hypercholanemia. We have previously shown that overt hyperthyroidism in early pregnancy only persisted into late pregnancy in 8.4% of cases (30), limiting our statistical power to study the effects of prolonged overt hyperthyroidism. Prolonged hyperthyroidism is more likely to be caused by underlying TSH receptor antibodies or autonomous thyroid nodules than transient hyperthyroidism confined only to early pregnancy, but it is unlikely that these underlying causes would increase the risk of hypercholanemia in itself. These data, together with our recent findings that persistent hyperthyroidism was associated with a lower birth weight (31), agreed with the current recommendations for follow-up women with hyperthyroid function in early pregnancy until signs of normalization.
We were able to study the association of thyroid function with hypercholanemia using a large prospective hospital-based cohort with detailed data and repeated thyroid function measurements. Furthermore, this study is limited by its hospital-based design, as after screening TBA concentrations in early pregnancy, some women were followed up and treated based on the insights of the physicians and/or obstetricians. Because of this, more severe cases of gestational hypercholanemia may have been excluded from analyses, which may have reduced the effect estimates reported in this study. Finally, it is important to note that the observational design of this study limits any statements on causality of the presented associations.
In conclusion, this study shows that higher fT4 is associated with a higher TBA and a higher risk of hypercholanemia particularly when this persists from early to late pregnancy. These data support the recommendations for biochemical follow-up of women with hyperthyroidism in early pregnancy.
Footnotes
Acknowledgments
We thank the pregnant women who participated in this study. We also thank the doctors and nurses who assisted in recruiting patients for this study.
Authors' Contributions
Study conception, design, and data analysis by X.Y. and C.Z. Drafting the original version of article by X.Y. Interpretation of results and critical editing by C.W., Y.L., Y.Z., C.L., L.C., Y.Z., T.K., W.W., and J.F. Article approval by all authors. T.K., W.W., and J.F. are the guarantors for this study and accept full responsibility for the conduct of the study, had access to the data, and controlled the decision to publish.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Key Research and Development Program of China (2018YFC1004602), National Natural Science Foundation of China (81971392), and the Shanghai Municipal Committee of Science and Technology (19ZR1462200).
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3