
Abstract
Background:
The role of minimal extrathyroidal extension (mETE) as a risk factor for persistent papillary thyroid carcinoma (PTC) is still debated. The aims of this study were to assess the clinical impact of mETE as a predictor of worse initial treatment response in PTC patients and to verify the impact of radioiodine therapy after surgery in patients with mETE.
Methods:
We reviewed all records in the Italian Thyroid Cancer Observatory database and selected 2237 consecutive patients with PTC who satisfied the inclusion criteria (PTC with no lymph node metastases and at least 1 year of follow-up). For each case, we considered initial surgery, histological variant of PTC, tumor diameter, recurrence risk class according to the American Thyroid Association (ATA) risk stratification system, use of radioiodine therapy, and initial therapy response, as suggested by ATA guidelines.
Results:
At 1-year follow-up, 1831 patients (81.8%) had an excellent response, 296 (13.2%) had an indeterminate response, 55 (2.5%) had a biochemical incomplete response, and 55 (2.5%) had a structural incomplete response. Statistical analysis suggested that mETE (odds ratio [OR] 1.16, p = 0.65), tumor size >2 cm (OR 1.45, p = 0.34), aggressive PTC histology (OR 0.55, p = 0.15), and age at diagnosis (OR 0.90, p = 0.32) were not significant risk factors for a worse initial therapy response. When evaluating the combination of mETE, tumor size, and aggressive PTC histology, the presence of mETE with a >2 cm tumor was significantly associated with a worse outcome (OR 5.27 [95% confidence interval], p = 0.014). The role of radioiodine ablation in patients with mETE was also evaluated. When considering radioiodine treatment, propensity score-based matching was performed, and no significant differences were found between treated and nontreated patients (p = 0.24).
Conclusions:
This study failed to show the prognostic value of mETE in predicting initial therapy response in a large cohort of PTC patients without lymph node metastases. The study suggests that the combination of tumor diameter and mETE can be used as a reliable prognostic factor for persistence and could be easily applied in clinical practice to manage PTC patients with low-to-intermediate risk of recurrent/persistent disease.
Introduction
Papillary thyroid carcinoma (PTC) is the most frequent subtype of thyroid cancer with a very low disease-specific mortality (1). However, PTC outcome differs according to several factors, including age, tumor size, extrathyroidal extension, and regional or distant metastases (2 –5). While extensive extrathyroidal extension has been associated with higher mortality and recurrence rates (6), the real impact of minimal extrathyroidal extension (mETE) (primary tumor extension to the sternothyroid muscle and/or perithyroidal soft tissue) on clinical outcome is still unclear, particularly in the case of small-sized PTC (7 –13). In the current edition of the American Joint Committee Cancer staging system (14), minor extrathyroidal extension was removed from pathology triiodothyronine (T3) definition and it now does not affect either T category or overall stage.
A recent meta-analysis concluded that mETE may increase the risk of recurrence in patients with differentiated thyroid carcinoma (DTC) (7). However, the absolute risk increase was found to be small. Conversely, mETE was found to have a nonsignificant impact on disease-related mortality and tumor stage (7). Nevertheless, the real impact of this feature as an isolated risk factor for poor outcome is still debated (7,12).
In a recent retrospective study that excluded PTC patients with lymph node metastases from analysis, the rate of patients with poor outcome (structural disease/death/recurrent disease) was significantly higher in patients with mETE compared with patients with intrathyroidal tumor at a median follow-up of 9.1 years (12). However, using chi-squared automatic interaction detection decision tree analysis, mETE was found to be a predictor of poor outcome only in tumors larger than 1.5 cm, while older age was the best prognostic factor for poor prognosis in smaller tumors (≤1.5 cm) with mETE (12).
Currently, only two retrospective studies have investigated the role of mETE in initial treatment response in PTC patients, reporting inconclusive results (15,16). In the presence of mETE, the American Thyroid Association (ATA) guidelines recommend that radioactive iodine (RAI) should be “considered” and “generally favored based on risk of recurrent disease” (17,18). However, there is uncertainty regarding the need for RAI in this subgroup of PTC patients (7). A recent prospective study reported a very low rate of recurrence in patients with mETE and low postoperative thyroglobulin (Tg) levels who were not treated with RAI therapy after surgery (19).
In the light of the scarce available data, we prospectively analyzed more than 2000 cases of PTC managed in 40 diverse health care settings in Italy to assess the role of mETE as a predictor of initial treatment response in PTC tumors. We also evaluated the impact of RAI ablative therapy in patients with mETE using propensity score-based matching to compare the outcome between treated and nontreated patients.
Patients and Methods
The Italian Thyroid Cancer Observatory (ITCO) web-based database was started in 2013 at the Thyroid Cancer Center of Sapienza University of Rome (the network's coordinating center). Since then, the network has expanded to include 49 thyroid cancer centers in the country (20). The database now includes prospectively collected data on more than 9000 patients with histologically confirmed diagnoses of differentiated, medullary, poorly differentiated, and anaplastic thyroid cancer. Cases are included in the database at the time of initial treatment at the reporting ITCO center, or when the patient begins follow-up in the reporting center within 12 months after undergoing initial treatment in a non-ITCO center.
Each record contains information on patient demographics and biometrics, circumstances of the diagnosis, tumor pathology, surgical and RAI treatment, and periodic follow-up examination results. The ITCO provides no guidance or restrictions in terms of patient management since the database is designed to provide a picture of real-world practice. Sensitive patient data are encrypted, and the database is anonymously managed for statistical analysis.
For the purposes of the present study, we reviewed all records present in the ITCO database and selected consecutive cases that satisfied the following criteria: (a) histological diagnosis of PTC and associated variants (with the exclusion of noninvasive follicular thyroid neoplasm with papillary-like nuclear features [NIFTP]); (b) pN0 and pNX PTC tumors; (c) availability of all information on the initial treatment and pathological characteristics of the tumor required for ATA recurrence risk assessment; (d) availability of the results for the 1-year follow-up visit (carried out 6–18 months after initial treatment), including all data needed to classify the estimated treatment response. The occurrence of mETE relied on the pathological report.
Of 7746 case records in the database at data lock (November 2019), 3222 (41.6%) were excluded for failing to meet the inclusion criteria (i.e., tumors diagnosed as medullary thyroid cancer, anaplastic thyroid cancer, NIFTP, tumors with unknown malignant potential, presence of lymph node metastases, or incomplete tumor resection [R2]). A further 2019 cases were excluded since the patient had not yet completed 1-year of follow-up and another 102 cases were excluded because the corresponding treatment center was in the last quartile of center-specific distribution of the number of enrolled patients. Thus, the final cohort consisted of 2237 patients who were followed in ITCO centers (Fig. 1).
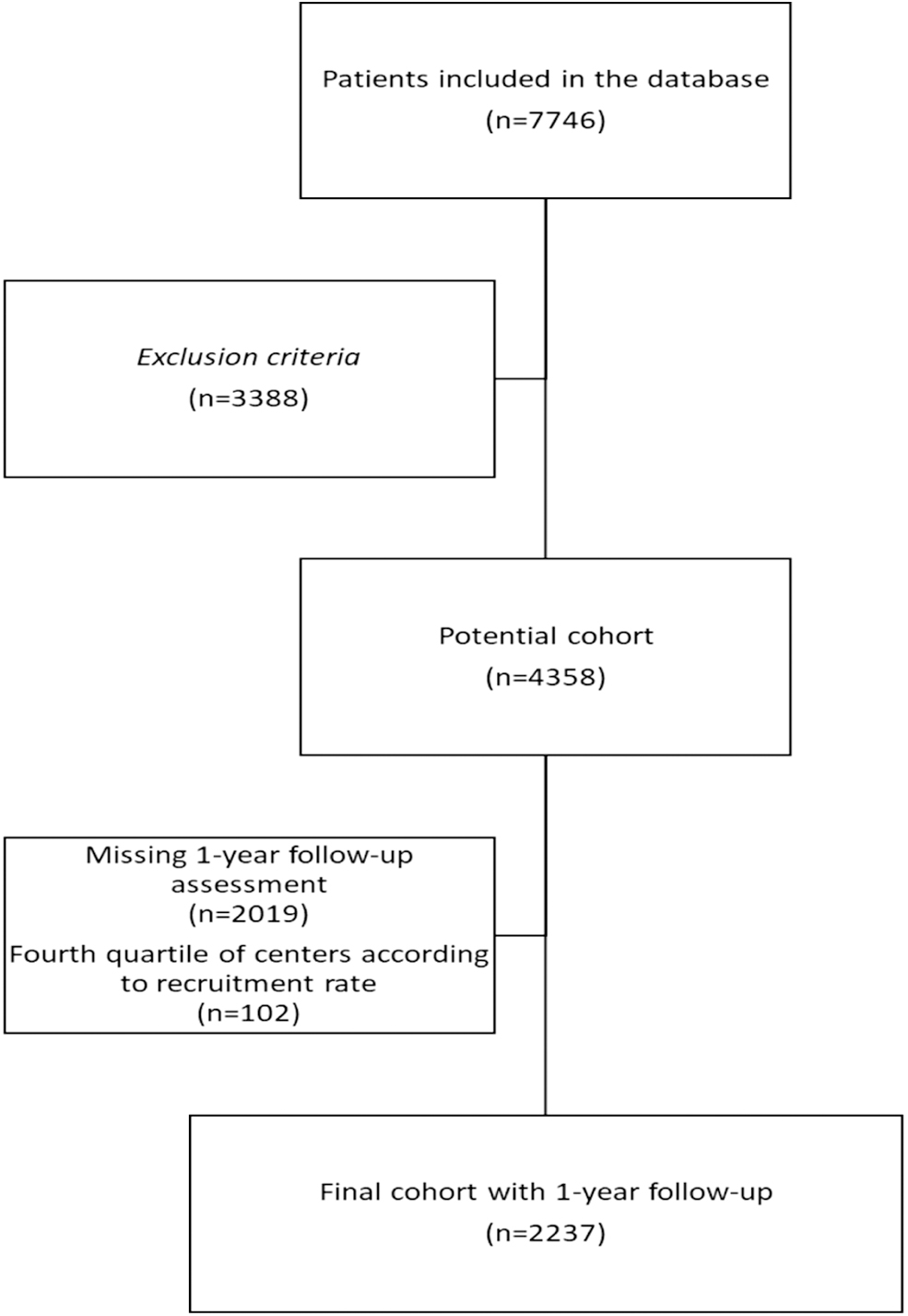
Flowchart of selecting study population.
For each case, we recorded the following information: Initial treatment; Histological variant of PTC; Risk of persistent or recurrent disease; and Response to initial therapy. The procedures followed have been approved by the institutional review committee.
Initial treatment
Treatment of the primary tumor was classified as total thyroidectomy, also including patients who had a completion thyroidectomy following thyroid lobectomy and lobectomy. For all patients who had a total thyroidectomy, we also recorded the use of radioiodine remnant ablation (RRA).
Histological variant of PTC
Tumors diagnosed as tall-cell, columnar-cell, hobnail-cell, solid/trabecular, or diffuse sclerosing PTC variants were classified as tumors with “Aggressive PTC histology.”
Risk of persistent or recurrent disease
The estimated risk level was determined in accordance with the 2009 ATA guidelines (17) and relevant 2015 updates (18). Classification was based on data available immediately after the initial treatment, including results of post-radioiodine treatment whole-body scan, if performed. When treatment consisted of lobectomy followed by completion thyroidectomy, we considered pathological data on tissues collected during both surgical procedures.
Response to initial therapy
Response to initial therapy was evaluated based on data collected during the clinical evaluation carried out at the 1-year follow-up visit. These data included imaging (cervical ultrasound in all patients and RAI scintigraphy in selected individuals) and baseline or stimulated serum Tg as well as anti-Tg antibody levels. Additional imaging studies were performed at the clinicians' discretion. The results were classified as specified in the ATA guidelines (18) for patients who had undergone thyroidectomy followed by RRA, and as advocated by the European Society for Medical Oncology (21) for those whose initial treatment consisted of total thyroidectomy alone or lobectomy (Supplementary Table S1).
Statistical analyses
For exploratory purposes, we summarized the distribution of continuous variables using medians with interquartile ranges (IQR), while nominal variables are described in terms of frequency counts and corresponding percentages. To evaluate significant association in contingency tables, we used either the chi-squared test or a numerical approximation of the Fisher exact test (whenever appropriate, i.e., for 2 × 2 tables). We analyzed treatment response also as a binary variable classified as either an excellent or structural/biochemical incomplete response, and therefore, we did not consider the indeterminate category. To analyze these responses, we used a mixed logit model with a center-specific random intercept. This analysis was performed using the R library lme4 (22). In addition, we decided to analyze potential differences in RAI treatment response.
Since patients undergoing treatment may not be comparable to those not undergoing treatment in terms of risk factors, we defined a propensity score model based on baseline clinicopathologic characteristics and outcomes and adopted propensity score matching to compare treated and nontreated patients. Cases were matched 1:1 between patients treated and not treated with RAI in accordance with age, aggressive histology, mETE, tumor diameter, and center effect on extrathyroidal extension. All statistical analyses were performed using the R statistical software package, MatchIt library (23). A p-value <0.05 was considered statistically significant.
Results
Demographic and clinicopathologic characteristics
As shown in Table 1, the study cohort consisted of 1723 females (77%) and 514 males (23%), with a median age at diagnosis of 51 years (IQR 41–61 years). Total thyroidectomy was performed in 2127 patients (95.1%), while 110 patients (4.9%) underwent near total thyroidectomy lobectomy. Thyroid gland removal was accompanied by simultaneous central neck dissection in 457 patients (20.4%), while lymph node dissection was not performed in the remaining 1780 patients (79.6%). The median tumor size was 10 mm (IQR 6–16 mm). Two hundred fifty patients (11.2%) were diagnosed with histologically aggressive PTC variants, that is, tall-cell, columnar-cell, hobnail-cell, solid/trabecular, and diffuse sclerosing PTC subtypes.
Clinical and Pathological Features of the Study Cohort
AJCC, American Joint Committee Cancer; ATA, American Thyroid Association; IQR, interquartile range; N/A, not applicable; PTC, papillary thyroid cancer.
mETE was documented in 470 patients (21%), while strap muscle invasion was reported in only 20 of them (4.3%). After surgery, 1153 patients (51.5%) received RAI therapy with a median activity of 2590 MBq (IQR 1850–3700 MBq). According to the ATA risk stratification system, 1632 (73%) were classified at a low risk of recurrence and 605 (27%) were classified at an intermediate risk of recurrence.
The effect of clinicopathologic parameters on initial treatment response
At the 1-year follow-up visit, an excellent response was recorded in 1831 patients (81.9%), an indeterminate response was observed in 296 (13.2%), a biochemical incomplete response was reported in 55 (2.5%), and a structural incomplete response was observed in 55 (2.5%). As summarized in Table 2, a similar initial therapy response was observed in patients with and without mETE (p = 0.54).
Treatment Response at 1-Year Evaluation
PTC patients with mETE versus patients without mETE, p = 0.54.
mETE, minimal extrathyroidal extension.
We then analyzed treatment response as a binary variable categorized as either excellent or structural incomplete/biochemical incomplete. The odds ratios (ORs) for incomplete response to the initial treatment were also explored to investigate clinical significance. Multivariate analysis showed that mETE (OR 1.16, p = 0.65), tumor size >2 cm (OR 1.45, p = 0.34), aggressive PTC histology (OR 0.55, p = 0.15), and age at diagnosis (OR 0.90, p = 0.32) were not significant risk factors for a worse initial response to initial therapy in PTC patients (Table 3).
Model for Structural or Biochemical Disease (Versus Excellent Response) at 1-Year Follow-Up as a Function of Clinical and Pathological Features
CI, confidence interval; OR, odds ratio; SE, standard error.
A combination of mETE, tumor size, and aggressive histology was also evaluated. The only interaction term that seemed to be associated with a worse outcome was tumor size (OR 5.27 [95% confidence interval 1.39–19.91], p = 0.014; Table 3). These findings were confirmed when the same analysis was performed after exclusion of patients with aggressive variants of PTC and also when multifocality was included as covariate (data not shown). We estimated joint effect of having mETE and a tumor size >20 mm by considering (summing) the estimated marginal and interaction effects associated with these variables and deriving appropriate standard error for this derived quantity. When considering the standard error and the covariance terms, we obtained an estimate of 1.07 with a standard error estimate of 0.49 (OR 2.90; p = 0.04).
We also included potential differences in mETE and other clinical risk factors between individual reporting centers, which included both academic and nonacademic health care facilities throughout Italy. Center-specific risk factors were included to account for potential biases (such as differences in histological diagnoses, surgical volumes, and tools used) that are difficult to document but can potentially influence treatment response assessment. The mixed-effect model we used took these factors into account by also using a (risk factor-free) center-specific intercept to summarize unobserved center-specific features.
The features of individual recruiting centers did not influence the evaluation of different clinical-pathological features (coefficient −1.60 ± 3.30, p = 0.628 for mETE; −1.10 ± 2.12, p = 0.604 for tumor size; and −0.14 ± 0.20, p = 0.487 for age).
Role of radioiodine ablation in PTC patients with mETE
The role of RAI therapy in the cohort of patients with mETE (n = 470) was also evaluated. In the subgroup of patients treated with surgery plus RAI (n = 370), the 1-year response to therapy was significantly different between the patients who underwent surgery alone compared with those who also received radioiodine therapy (p = 0.005) (Table 4). To verify if this difference was mainly due to the high rate of indeterminate response observed in patients treated with surgery alone, we analyzed treatment response also as a binary variable classified as either an excellent or structural/biochemical incomplete response. Using this approach, the rate of excellent response was 97.5% and 92.8% in patients treated with surgery alone and patients treated with surgery and RAI, respectively, without significant difference between the two groups (p = 0.21).
Treatment Response at 1-Year Evaluation in Patients with Minimal Extrathyroidal Extension According to Initial Treatment (Surgery Alone Versus Surgery Plus Radioiodine Ablation)
To minimize potential selection bias (e.g., due to the inclusion of lower risk patients in the subgroup treated with surgery alone), we performed propensity score matching based on known covariates and risk factors (age, aggressive histology, mETE, tumor diameter, and center effect on extrathyroidal extension). After matching, we did not detect significant differences between PTC patients treated and untreated with RAI (p = 0.28). The rate of excellent response was 97.5% in patients treated with surgery alone and 93.3% in patients treated with surgery followed by RAI therapy (Table 4).
Discussion
Although most PTCs are indolent, a subset behaves aggressively despite the best available treatment. The stratification system based on ATA risk of recurrent disease in DTC (17,18) is widely used to stratify prognosis and guide therapeutic strategies. While definitive recommendations are available for low- and high-risk patients, most of the recommendations reported are not conclusive for intermediate-risk patients, especially regarding chiefly concerning the use of RAI therapy after surgery (18). The 2015 ATA guidelines grouped tumors with mETE in the intermediate risk of recurrence category, citing studies with a 3–9% risk of recurrence, a range that is between low and intermediate risk (18). There is some debate about the appropriateness of classifying PTC patients who only have mETE as intermediate risk, especially if their tumor is small (8,12).
Some studies have suggested that mETE has no impact on disease-free survival (8,12,13), whereas others report a higher risk of persistent/recurrent disease in patients who have PTC with mETE (7,9). The interpretation of studies evaluating mETE is complex due to differences in the definition of mETE and tumor size and the inclusion of patients with and without lymph node metastases (7,24,25). Moreover, in some studies, the degree of extrathyroidal extension was defined on both pathological and intraoperative findings (26,27), while in others, only pathological findings were used (9,10,12,19).
Moreover, it is important to underline that most of the published studies focused on long-term outcomes. Undoubtedly, long-term outcomes remain the most crucial endpoint, but on a day-to-day basis, the initial presentation of patients influences clinical decisions and early therapy response determines the clinical follow-up examination (e.g., dynamic risk stratification according to the latest ATA guidelines).
In light of the limited available findings (15,16) on this subject, we performed a prospective study to assess the impact of mETE on the management and short-term follow-up of PTC patients. We found that the response rate after initial therapy was achieved irrespective of mETE. Nonetheless, when analyzing the combination of different prognostic factors (mETE, tumor diameter, aggressive histology), we found that combining mETE and tumor diameter could more accurately separate patients with persistent disease from those with an excellent initial therapy response. As previously demonstrated (20), the reliability of the model is not affected by the features of the diverse recruiting centers.
A combination of these two pathological factors could represent an effort to modify traditional staging systems and move toward a more personalized system to establish prognosis and treatment.
To date, only two studies have evaluated the impact of mETE on initial therapy response in PTC patients, reaching different conclusions (15,16). Ahmaddy et al. (15) reported identical responder rates in patients with and without mETE (84% in +mETE patients and 84% in −mETE patients, p = 0.988) when 301 PTC patients without lymph node metastases were evaluated. Interestingly, similar results were also observed in the subgroup of patients with lymph node metastases (59% in +mETE patients and 57% in −mETE patients, p = 0.845). Conversely, microscopic positive margins were found to be significantly associated with incomplete initial therapy response in patients with DTC after adjusting for tumor size and cervical lymph node metastases in 101 DTC patients undergoing total thyroidectomy and RAI ablation (16).
mETE is considered a criterion for completion thyroidectomy and RAI ablation therapy, at least in selected cases (18). We also evaluated the role of RAI ablation in PTC patients with mETE. After propensity score-based matching (for tumor size and aggressive histology), we observed a similar rate of excellent treatment response at the first follow-up visit in treated and nontreated PTC patients. Nevertheless, we observed a trend toward significance between the two groups (p = 0.06), probably due to the higher rate of indeterminate responses in PTC patients treated with surgery alone (21% vs. 10%). Indeed, after excluding patients with indeterminate response from the statistical analysis (comparing excellent vs. structural incomplete/biochemical incomplete response), initial therapy response was similar in the two groups (p = 0.28).
Low Tg levels are usually observed in patients treated with total thyroidectomy without RAI therapy or lobectomy (26) and are associated with a very low rate of persistent/recurrent disease (0.6%) in low-to-intermediate-risk DTC patients (28). In the presence of mETE, the ATA guidelines (20) recommend that RAI should be “considered” and “generally favored based on risk of recurrent disease.” Our results suggest that RAI therapy may be avoided in PTC patients with mETE when there are no additional negative prognostic factors.
Outcome studies support our data (7,12,19). In the absence of other adverse features, patients with mETE have a low recurrence risk both in studies where all patients were treated with total thyroidectomy and RAI ablation (3.7% recurrence rate) (7,12) and in studies where patients were treated with either total thyroidectomy or lobectomy at the discretion of the treating physician (3.3% recurrence rate) (7,19).
The present study has some limitations. First, most patients with mETE were treated with RAI therapy because mETE was considered a risk factor at the time of inclusion. Second, primary surgical procedures, initial pathological diagnoses, and follow-up were performed in different hospitals. Although central review of histology slides was not performed, we only included patients with detailed pathology reports that fulfilled the purpose of the study. This is a relevant point since the thyroid gland has an incomplete capsule, so defining mETE may be problematic and requires attention in evaluating the relationship between neoplasm and surrounding muscle and adipose tissues.
Furthermore, this is real-world database study. In this context, missing data can lead to biased estimates of the outcome measures. Finally, we evaluated the predictive value of mETE only in predicting the response to initial therapy. A follow-up study looking at the long-term outcomes of this cohort is ongoing. It will be able to clarify the prognostic role of mETE also in terms of disease-free survival, cause-specific survival, and overall survival.
The strength of our study is the inclusion of a large prospective cohort of PTC patients without lymph node metastases. The inclusion of a more selected group of PTC patients classified as low-to-intermediate risk has allowed us to better assess the prognostic significance of mETE in PTC patients during a short-term follow-up. In addition, the use of propensity score matching has allowed the analysis of a nonrandomized cohort while considering the effect of observed confounders.
In conclusion, the current study fails to show an independent prognostic value for the presence of mETE in predicting initial therapy response in a large cohort of PTC patients without lymph node metastases. However, the combination of tumor diameter >2 cm and mETE appears to be a reliable valid independent prognostic factor for worse outcome. This approach can be easily applied to the clinical practice for the management of PTC patients that are at low-to-intermediate risk of recurrent/persistent disease.
Footnotes
Acknowledgments
We thank all the collaborators of the ITCO Network: Fabio Maino (Department of Medical, Surgical, and Neurological Sciences, University of Siena, Siena, Italy); Marco Biffoni and Laura Giacomelli (Department of Surgical Sciences, Sapienza University of Rome, Rome, Italy); Antonella Carbone (Endocrinology Unit, Tinchi Hospital, Matera, Italy); Simone De Leo and Carla Colombo (Istituto Auxologico Italiano IRCCS, Milan, and University of Milan, Milan, Italy); Michela Marina (Azienda Ospedaliero-Universitaria di Parma, Parma, Italy); Armando Patrizio (Azienda Ospedaliero-Universitaria Pisana, Pisa, Italy); Michela Massa (Department of Clinical Sciences, Fondazione IRCCS Casa Sollievo della Sofferenza, San Giovanni Rotondo, Italy); Maria Grazia Deiana and Federica Presciuttini (Department of Endocrinology and Diabetes, Azienda Ospedaliero-Univeristaria Sant'Andrea, Sapienza University, Rome, Italy); Valentina Verdiani (Endocrinology Unit, Department of Experimental and Clinical Biomedical Sciences “Mario Serio,” University of Florence, Florence, Italy); Maria Grazia Chiofalo, Anna Crocco, and Carmela Casolino (Struttura Complessa Chirurgia Oncologica della Tiroide, Istituto Nazionale Tumori-IRCCS-Fondazione G. Pascale, Naples, Italy).
Authors' Contributions
R.F., G.G., S.F., C.D., and M.G.C. were responsible for study conception and design and carried out clinical data collection and statistical analysis of the results. M.A. and U.F.P. carried out statistical analysis of the results. V.Z., R.G., M.C.Z., I.G., A.P., A.R., S.M., E.P., L.P., M.D., G.C., M.T., B.P., A.A., M.C., L.F., G.S., S.M., R.R., F.M., G.T., A.C., C.S., R.B., A.R., D.T., L.P., and C.P.L. carried out clinical data collection.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by the Sapienza University of Rome Research Grant (RM11916B83A211FC) to C.D.
Supplementary Material
Supplementary Table S1