
Abstract
Background:
The characteristics of pediatric differentiated thyroid cancer (DTC) are substantially different from those of adult DTC. This study investigated whether the cutoff age of 18 years, as recommended by the American Thyroid Association (ATA) management guidelines for pediatric DTC, is appropriate based on clinical characteristics and outcomes.
Methods:
The medical records of 288 patients aged <21 years with DTC, who underwent initial surgery between 1979 and 2014, were retrospectively reviewed. Disease-free survival (DFS) rates and distant metastasis-free survival (DMFS) rates were calculated using the Kaplan–Meier method. As per the International Incidence of Childhood Cancer Report and the ATA management guidelines, cutoff ages of 14 and 18 years were analyzed in this study.
Results:
The age distributions of the subjects were as follows: 53 patients were aged <15 years (18.4%), 118 patients were aged 15–18 years (41%), and 117 patients were aged 19–20 years (40.6%). The DMFS rates were significantly different between the two cutoff ages. The DMFS was also significantly different between patients aged >15 years and patients aged 15–18 years; however, no significant difference was observed between patients aged 15–18 and 19–20 years. Multivariate analyses showed that clinically apparent lymph node metastasis (cN1) and gross extrathyroidal extension were significant factors related to DFS and DMFS. Although age as a continuous variant was not a significant factor related to either DFS or DMFS, when the cutoff age was set as 14 years rather than 18 years, differences in patient characteristics related to DMFS and DFS stood out.
Conclusions:
This study found that age was not significantly related to clinical outcome. However, in the younger patient group, more patients had factors that related to DFS and DMFS. Due to the indolent biological behavior of DTC, age at presentation or thyroidectomy does not always represent the age at occurrence, but patients aged <15 years had distinct clinical manifestations. Age <15 years rather than <19 years may therefore be a more suitable cutoff age in pediatric DTC.
Introduction
In differentiated thyroid cancer (DTC), age is considered an important factor related to survival and/or recurrence (1,2). Young DTC patients are reported to have an excellent prognosis, and even patients with distant metastases (DM) have been categorized into stage II in the TNM staging classification of DTC. In the recent eighth TNM staging of DTC (3), the cutoff age was changed from 45 to 55 years based on the results obtained from previous studies. However, a definitive reason as to why 45 years was determined to be the cutoff age in the former seventh TNM staging is unclear. It is speculated (4) that 45 years of age was the median age in many previous studies. However, the cutoff age in the American Thyroid Association (ATA) guidelines for pediatric DTC (5) is defined by the physiological changes of growth or by the cutoff age adopted in the majority of the previous studies. In pediatric DTC, advanced stage at presentation, frequent recurrences, and a spectrum of genetic mutations are characterized compared with adult DTC, and therefore, different treatment strategies should be considered. However, the relationship between a patient's age and the biological behavior of DTC is not clearly defined. Many previous studies of pediatric DTC included individuals up to 21 years of age. The cutoff age in these studies is, however, arbitrary. A uniform cutoff age would allow for a more accurate comparison of results and increase consistency of results within this field.
The setting of a cutoff age is important for clinical practice; however, it can occasionally cause some confusion. Specifically, the guidelines for pediatric DTC recommend a total thyroidectomy as standard surgical treatment for patients who are at any risk, whereas the ATA guidelines for adult DTC (6) allow a lobectomy for low-risk DTC patients. Therefore, for example, according to these guidelines, the treatment recommendation for an 18-year-old patient with T1N0M0 DTC will be a total thyroidectomy, whereas a 19-year-old patient with same stage DTC would be treated with a lobectomy or even active surveillance according to the adult guidelines. To the best of our knowledge, there are no studies that investigate the appropriate cutoff age between adults and children with DTC based on their clinical features or outcomes.
In this study, we attempted to investigate whether the cutoff age of 18 years in the ATA management guidelines for pediatric DTC is appropriate with regard to both clinical characteristics and outcomes.
Patients and Methods
This study included 288 patients aged <21 years with DTC who underwent initial surgery in our hospital between 1979 and 2014. All information used in this study, including patient demographics, operative findings, postoperative treatment, and follow-up, was collected from the patients' medical records. Fourteen patients were referred to other hospitals, and the remaining patients were followed up in the outpatient department of our hospital. Follow-up information for patients who were referred to the other hospitals was obtained through correspondence with the other hospitals. The median follow-up period was 15.6 years (range, 18–460 months). At the initial visit, their disease was evaluated by several modalities, including palpation, chest radiograph (CXR), neck ultrasonography (US), computed tomography (CT), and fine-needle aspiration biopsy cytology (FNABC). DM was mainly diagnosed by CT, CXR, and/or postoperative radioactive iodine (RAI) scintigraphy. Synchronous metastases were defined as DM confirmed before initial surgery or within six months of initial surgery. Metachronous metastases were defined as DM detected more than six months after initial surgery. Clinically apparent nodal disease was evaluated by palpation, US, FNABC, and intraoperative inspection and was defined as clinical N1 (cN1), whereas no clinically apparent nodal disease was defined as clinical N0 (cN0). Microscopic metastatic lymph nodes diagnosed by histology alone were defined as pathological N1 (pN1). In our hospital, treatment strategies are adapted according to the risk factors related to recurrence or survival, that is, cN1, gross extrathyroidal extension (ETE), or DM, but not according to the patient's age. As for the extent of the thyroidectomy, a rather conservative approach, as in adult patients, was adopted (7,8). Ipsilateral lobectomy was standard procedure except for patients with synchronous DM, bilateral disease detected by US, concomitant benign thyroid disease, and patients with cN1 or ETE. RAI therapy was recommended after total thyroidectomy for patients with synchronous DM. Postoperative follow-up examinations were usually performed at 1, 3, 6, and 12 months, and every 6 months thereafter. The serum thyroglobulin (Tg) level was routinely measured at every hospital visit. CT scans were performed whenever a gradual increase in postoperative Tg level was observed in patients who had not undergone total thyroidectomy. However, the presence of thyroglobulin antibody (TgAb) interferes with the Tg immunometric assay and makes the Tg levels unreliable. Patients with positive TgAb were followed by CT and US. If these examinations resulted in detection of metastases, completion thyroidectomy was performed followed by RAI scintigraphy. Postoperative thyrotropin (TSH) suppression therapy was performed selectively in patients with DM, ETE, and cN1, but these patients' TSH levels were not analyzed in this study.
The cutoff ages used in this study were 18 years as recommended in the ATA guidelines for pediatric DTC management (5) and 14 years as used in the pediatric data set in the International Incidence of Childhood Cancer (IICC) (9).
The data were analyzed using the statistical software program (JMP 12.0; SAS Institute, Inc., Cary, NC). Disease-free survival (DFS) rates and distant metastasis-free survival (DMFS) rates were calculated using the Kaplan–Meier method. The DFS was evaluated only in patients who underwent initial curative surgery. Multivariate analyses related to DFS and DMFS were conducted using Cox's proportional hazard model. A chi-squared or Fisher's exact test was performed for categorical variables. All p-values were two-sided, and a p-value <0.05 was considered significant.
The protocol for this study was reviewed and approved by the institutional review board, and the study was performed in accordance with the Declaration of Helsinki.
Results
The patient characteristics are shown in Table 1. None had a history of radiation exposure. There were 251 female and 37 male patients, with a median age of 18 years (range 7–20 years). The age distribution of the subjects is shown in Figure 1. Seven patients (2.4%) were aged <10 years, 46 patients (16%) were aged 10–14 years, 118 patients (41%) were aged 15–18 years, and 117 patients (40.6%) were aged 19–20 years. More than 80% of the subjects were aged ≥15 years. The histological diagnosis after thyroidectomy was papillary thyroid cancer (PTC) in 250 patients and follicular thyroid cancer (FTC) in the remaining 38 patients. The median primary tumor size was 26 mm (range 1–100 mm). Clinically apparent metastatic lymph nodes at presentation (cN1) were observed in 65 patients, and 21 patients were diagnosed as having synchronous DM (M1). Gross ETE was observed in 20 patients. The sites of extension were as follows: the recurrent laryngeal nerve in 15, the trachea in 12, and the esophagus in 5, including overlapping cases. Total thyroidectomy was performed in 84 patients, and 204 patients underwent less than total thyroidectomy. Neck dissection was performed in 241 patients (83%). Sixty-three patients underwent therapeutic modified radical neck dissection, and 176 patients underwent prophylactic neck dissection (prophylactic central node dissection for 59 patients and prophylactic modified neck dissection for 117 patients). Complete neck dissection could not be performed in two cN1 patients due to widely invasive metastatic lymph nodes. Of the 176 cN0 patients who underwent prophylactic neck dissection, metastatic lymph nodes in the dissected area were diagnosed histologically in 154 patients (87.5%).
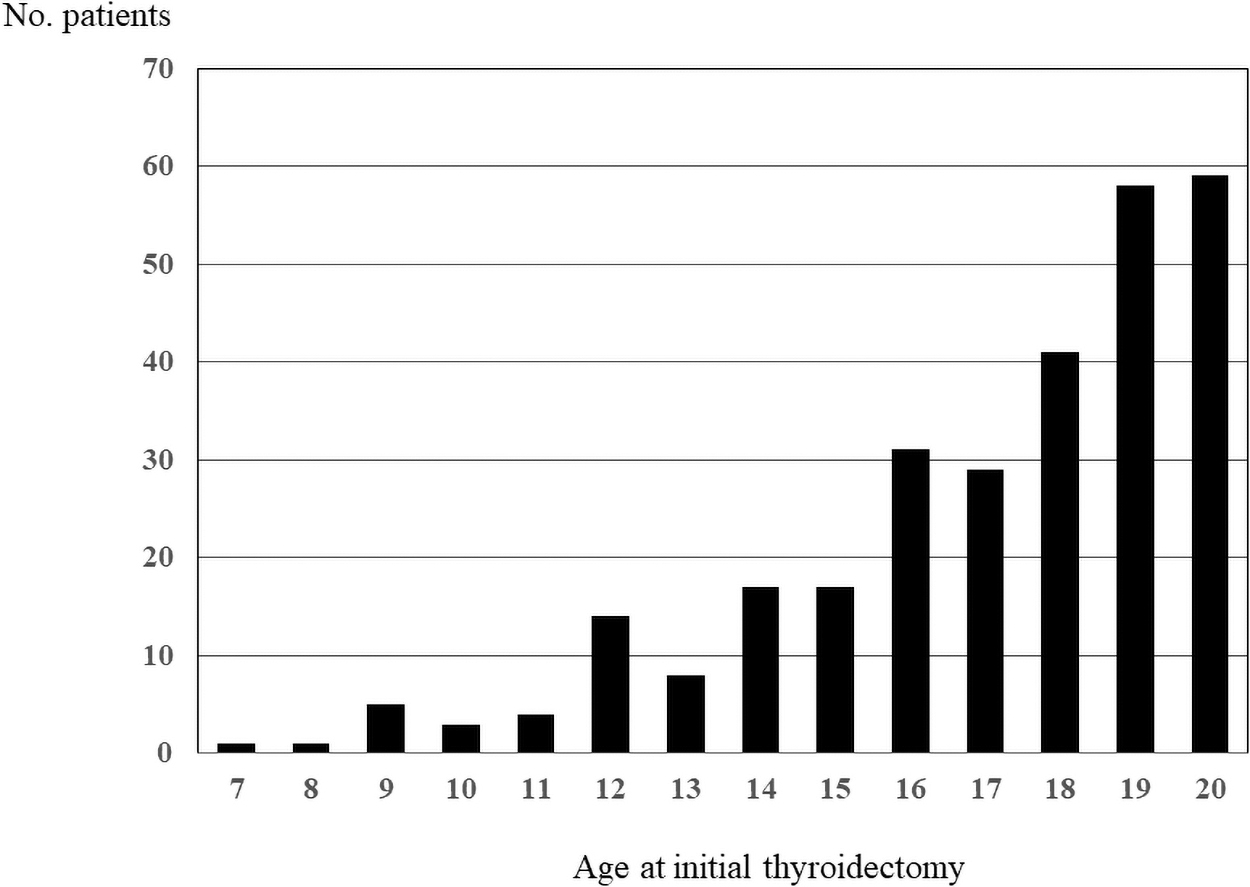
Age distribution of the subjects.
Patient Characteristics
Number in parentheses represents percentage.
cN1, clinically apparent lymph node metastasis at presentation; ETE, extrathyroidal extension; DM, distant metastasis; Neck dissection, therapeutic dissection and prophylactic dissection; RAI, radioactive iodine.
Clinical outcomes and factors related to clinical outcomes
During the follow-up period, disease-specific deaths occurred in 3 patients aged 9, 12, and 17 years at the time of diagnosis, and aged 31, 48, and 23 years at the time of death, respectively. All patients had DM at initial surgery (synchronous DM) and died of respiratory failure. Their lung disease was RAI-avid, and they underwent RAI therapy several times. Although disease-specific death was rare, all patients in whom this occurred were aged ≤19 years at the time of presentation. Fifty-two patients (18.1%) developed disease recurrence during the follow-up period. Recurrences were observed in regional lymph nodes in 37, in distant organs (lung) in 14, and in remnant thyroid in 9, including overlapping cases. The 54 patients with recurrences consisted of 53 PTC patients and 1 FTC patient. Recurrence was observed in the remnant thyroid in one FTC patient. Although one FTC patient had synchronous DM, none of the other FTC patients developed DM.
Excluding 21 patients who did not undergo initial curative surgery, the 10-, 20-, and 30-year DFS rates (Fig. 2A) were 85.3%, 76.4%, and 68.0%, respectively. The 10-, 20-, and 30-year DMFS rates (Fig. 2B) were 89.3%, 87.9%, and 85.8%, respectively. The DFS rates were compared between the two cutoff age groups (Fig. 3A, B), and no significant difference was found. However, comparison of the DMFS rates revealed significant differences (p < 0.01) between the two cutoff ages (Fig. 4A, B). Patients aged <15 years had significantly lower DMFS rates than patients aged 15–18 years (p < 0.01) and patients aged 19–20 years (p < 0.01); however, no significant difference was found between patients aged 15–18 years and patients aged 19–20 years (Fig. 4C). In univariate and multivariate analysis, the clinical factors related to DFS and DMFS are shown in Table 2. Multivariate analyses showed cN1, ETE, and numbers of metastatic lymph node as significant factors related to DFS (Table 2A). Significant factors related to DMFS were sex, cN1, ETE, and total thyroidectomy by multivariate analyses (Table 2B). Age as a continuous variable was not a significant factor in either DFS or DMFS. Total thyroidectomy was a negative predictor for DMFS as more patients with advanced disease underwent total thyroidectomy.

DFS rates and DMFS rates. (
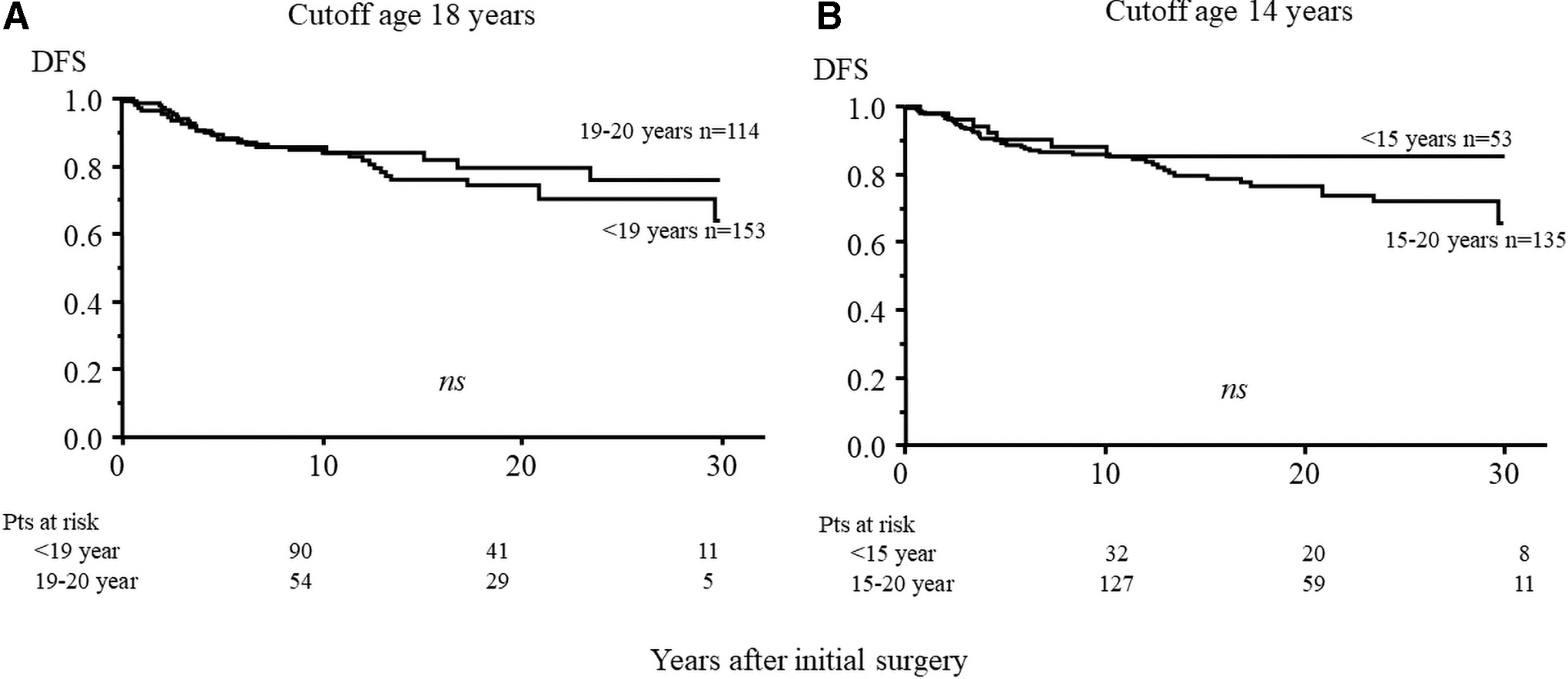
Comparison of DFS rates between the two cutoff age groups. (
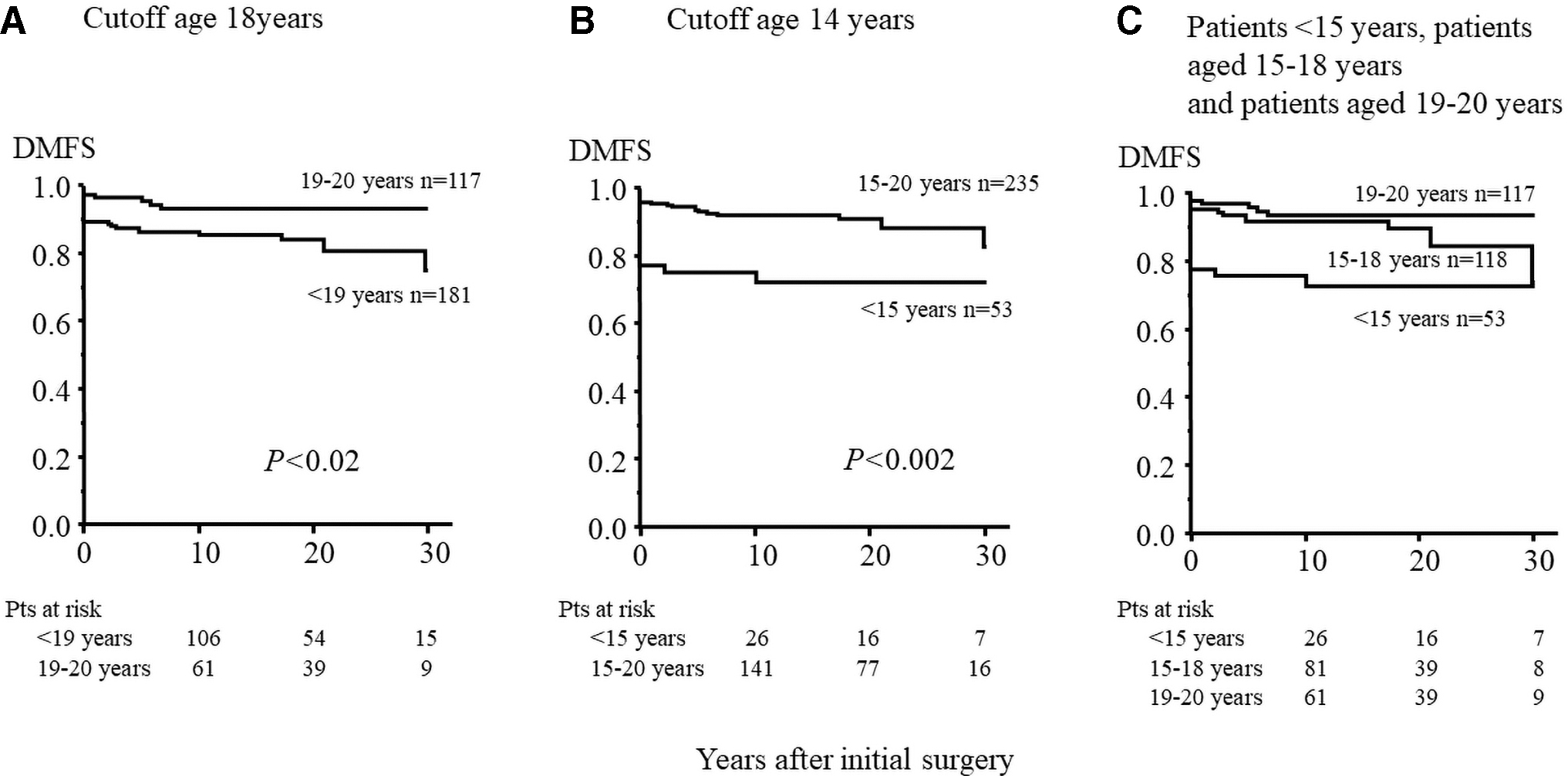
Comparison of DMFS rates. (
Clinical Factors Related to Disease-Free Survival and Distant Metastasis-Free Survival
CI, 95% confidence interval; DFS, disease-free survival; DMFS, distant metastasis-free survival; HR, hazard ratio; PTC, papillary thyroid cancer; TT, total thyroidectomy; LND, modified radical neck dissection; NMLNs, numbers of metastatic lymph node; ns, not significant.
Comparison of clinical features according to age group
The clinical characteristics among the different age groups are shown in Table 3. Although the number of patients aged <15 years is small, more patients with cN1, ETE, large primary tumor size, and synchronous DM were observed in this younger age group. These characteristics decreased with advancing age.
Patient Characteristics by Age Group
Number in parentheses represents percentage.
As described in the Patients and Methods section, the cutoff ages in this study were defined as 14 and 18 years and the subjects were divided into groups according to this. There were 53 patients aged <15 years, 118 patients aged 15–18 years, and 117 patients aged 19–20 years. A comparison of the patient characteristics between the two cutoff ages is shown in Table 4A and B. Both cN1 and ETE were more frequently observed in the younger group of patients. However, statistical significance was only observed when the cutoff age was set at 15 years. Significantly high numbers of patients with synchronous DM were observed in the younger patients in both cutoff ages. The extent of initial treatment including thyroidectomy, neck dissection, and ablation was similar in both groups.
Comparison of the Clinical Characteristics and Outcomes According to the Age Groups
Number in parentheses represents percentage.
Discussion
Several differences in both the clinical and genetic manifestations of pediatric and adult DTC patients have been reported. Although advanced local disease, as well as distant disease, is often observed in both the pediatric and adolescent population at presentation, patients generally respond well to surgery and radioiodine therapy, and the cumulative survival rate in the young age group is excellent (10,11). The ATA guidelines for pediatric DTC (5) state that “Studies of pediatric DTC have variously included individuals extending up to 21 years of age. With uncommon exception, the majority of pediatric patients have completed growth and development by ≤18 years of age. To more accurately define the impact of the physiologic changes of growth and development on tumor behavior, the upper limit for pediatrics should be defined as patients ≤18 years of age.” This cutoff age was therefore not based on clinical features or outcome and has not been verified as appropriate. There have been many studies on pediatric and adolescent DTC (10 –15), but the age range in the subjects varies from study to study. As in the TNM classification for thyroid cancer, the cutoff age should be set based on clinical features and outcome (3,4). In previous studies (16 –19), the age at presentation of childhood DTC with lymph node metastasis or synchronous DM was younger than that of children without metastases at presentation, despite similar tumor size, and, similarly, children who developed metastases during follow-up were younger than those who did not. This has, however, not been confirmed by other studies, and a sufficient number of patients, especially patients aged <10 years, were not included (18,19).
The cutoff age that separates children from adults is not universally defined. The American Academy of Pediatrics has previously published a statement defining the upper age limit of pediatrics as 21 years (20). Reports from the IICC and Cancer Incidence and Survival among Children and Adolescents: United States SEER Program (21) use 14 years as one of the cutoff ages. In the most recent epidemiological studies of pediatric thyroid cancer based on the cancer registration system, the incidence of pediatric DTC patients was reported to be increasing, especially in older pediatric patients (22 –24). These studies included patients >18 years, and the majority of the patients were >14 years (>70%) (22,24). In this study, patients aged >14 years accounted for more than 80% of the subjects and patients aged ≥15 years showed a sharp increase. The clinical study of pediatric or adolescent DTC including older patients would therefore reflect the strong impact of older patients' characteristics and outcomes and lead to biased results. The cutoff of age between pediatric and adult DTC is a very important issue, necessary to better identify the clinical manifestations and therefore appropriate treatment strategy for each patient. To the best of our knowledge, studies assessing the appropriate cutoff age in these populations have not been carried out. Our study, one of largest cohorts of pediatric thyroid cancer with relatively long follow-up, found that significant factors related to DFS and DMFS were cN1 and ETE, and that more patients in the younger population were observed as having these risk factors. This indicates that younger patients would have poor DFS and DMFS. One of the clinical characteristics in pediatric DTC is frequent occurrence of DM. We found age to be a significant factor related to DMFS, although only by univariate analysis. Age as a continuous variable was not a significant factor related to DFS and DMFS, and we could not show an appropriate cutoff age in this population from a perspective of therapeutic outcomes. Due to the infrequent occurrence of DTC in the pediatric population especially in the prepubertal population, sufficient numbers of patients would be necessary to better determine the appropriate cutoff age for pediatric DTC patients. Further studies using a sufficient number of young DTC patients will be necessary to identify the cutoff age.
Several differences in the genetic aspects of DTC between adult and pediatric patients have, however, been reported (25 –29). For example, BRAF mutations are reported as the most common abnormality in adult PTC (30) but are infrequent in pediatric PTC and virtually absent from the youngest patients (27). Fusion genes are more frequently observed in childhood DTC than in adult DTC (28,29). This may be important because point mutations in BRAF lead to genomic instability and dedifferentiation manifested by decreased expression of the sodium–iodide symporter (31). Rearranged during transfection PTC rearrangements are more common in PTC in children and do not lead to genomic instability. These molecular differences might be one of the reasons for a better response to RAI therapy in children with PTC and could partially explain their low mortality rate and rare progression to less-differentiated tumors. However, there are still controversies concerning genetic variation in pediatric DTC. In a recent study by some Japanese colleagues (32), a BRAF point mutation was the main genetic alteration found in young PTC patients diagnosed by ultrasound screening in the Fukushima prefecture after the Fukushima Daiichi nuclear power plant accident. A BRAF mutation was detected in 40% of patients aged ≤14 years and in 75% of patients aged 15–19 years and was correlated with age at surgery. Although controversies still exist, the cutoff age between pediatric and adult DTC might be set in accordance with these aspects of genetic alteration.
In conclusion, we found that the cutoff age could not be clearly defined by clinical outcomes alone. However, in the younger patient group, significantly more patients had risk factors related to DFS and DMFS. Although the indolent biological behavior of DTC means that the age at presentation or at thyroidectomy does not always represent the age at occurrence, patients aged <15 years had distinct clinical manifestations. We therefore suggest that an age cutoff of <15 years rather than <19 years may be more suitable in pediatric DTC.
Footnotes
Authors' Contributions
K.S. wrote the article. All authors reviewed the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.