
Abstract
Background:
While the popularity of lobectomy for differentiated thyroid cancer (DTC) has increased since the 2015 ATA (American Thyroid Association) guidelines, recent studies reported that adverse histological features (minimal extrathyroidal extension [mETE], multifocality, vascular invasion, and lymph node [LN] metastases) may be found in 30–60% of lobectomy specimens, questioning the validity of this approach.
Aim:
To assess the prevalence adverse histological features in occult DTC detected in autopsy studies.
Methods:
Meta-analysis of autopsy studies of the thyroid in subjects without known history of thyroid cancer.
Results:
Twenty-nine studies including 8750 subjects fulfilled the inclusion criteria, with incidentally discovered DTC in 740 autopsies (8.5%). Age was reported in 17 studies, with a median age of 61 years (range 41–68 years). Multifocality was reported in 27 studies with a calculated event rate of 28.2% ([CI 23.1–33.8], I 2 = 46.3%), with bilateral involvement in 18% [CI 12.6–25.1]. mETE was reported in 5 studies, with an event rate of 24.5% ([CI 9.3–50.7], I 2 = 88.5%), and the presence of LN metastases were reported in 13 studies with an event rate of 11% ([CI 6.1–19.1], I 2 = 69.5%). Vascular invasion was reported in seven studies with an event rate of 16% ([CI 4–47], I 2 = 86.8%). Of 25 studies with whole body autopsies (722 subjects), 3 cases of distant metastases were reported, of which 2 had fatal metastatic disease (where thyroid origin was not diagnosed before death), and 1 had occult disease.
Conclusions:
Adverse histological features including mETE, LN metastases, multifocality, and vascular invasion are common in occult DTC. When minimal in size, these adverse histological features do not seem to be markers of aggressive disease and may not be an indication for completion thyroidectomy or radioiodine therapy.
Introduction
The extent of surgery for differentiated thyroid cancer (DTC) is determined by the risk of disease recurrence and by whether radioiodine therapy is required after surgery. While in the past total thyroidectomy was recommended for all papillary thyroid cancer (PTC) >1 cm (1), the 2015 American Thyroid Association (ATA) guidelines have greatly expanded the option for thyroid lobectomy for patients with low risk disease up to 4 cm (2). This was based on multiple studies showing similar survival rates between lobectomy and total thyroidectomy (3 –8), together with locoregional recurrence rates of <5% and completion thyroidectomy rates of <10% in properly selected patients (8 –11).
A major disadvantage of lobectomy as an initial surgical strategy is the need for completion thyroidectomy in some patients, based on adverse histological characteristics reported on final pathology, which are considered risk factors for recurrence (that were unknown before surgery). These may include minimal extrathyroidal extension (mETE), lymph nodes (LNs) metastases, multifocality, vascular invasion, or high-risk histological variants. While the prevalence of these features was considered low in seemingly low-risk PTC patients undergoing lobectomy, several recent studies reported these features in up to 30–60% of patients who are candidates for lobectomy according to the 2015 ATA guidelines (12 –15).
Importantly, the designation of some of these histological features as risk factors for recurrence (sometimes called “high risk” features) has been questioned in recent years. For example, in an article from 2012 the ATA surgical affairs taskforce stratified LN metastases according to their size, number, as well as presence of extranodal extension, leading the 2015 ATA guidelines to include five or less LN metastases <2 mm in the low risk of recurrence category. Similarly, the risk associated with mETE or multifocality was recently shown to be lower than previously thought (9,16). Owing to the conflicting data regarding these histological characteristics, some authors recommend completion thyroidectomy for patients with these features (12 –15), while others would not recommend additional therapy if these features are minimal in size and spread (9,16,17).
The high prevalence of adverse histological features in lobectomy specimens may be counterintuitive, as most of these tumors are small in size and many are incidentally found. Data from recent years demonstrate that occult PTC is common in the general population, with a reported prevalence up to 11.2% in a recent meta-analysis (18). Most people with small undiagnosed thyroid cancers will live their lives without knowledge of the disease, and without any health implications. If adverse histological features are associated with disease growth and spread, we would expect them to be uncommon in occult disease. Conversely, if these features are found to be common in occult disease, it would suggest a low aggressive potential. We, therefore, evaluate the presence of adverse histological features in people with occult PTC in a meta-analysis of autopsy studies of subjects without known history of thyroid cancer.
Methods
Data sources
We searched PubMed (January 1966 to December 2020), CENTRAL (The Cochrane library, up to December 2020), and conference proceedings in endocrinology, oncology, and thyroid surgery. The terms “thyroid cancer” and similar and “autopsy” and similar were crossed. We scanned references of all included trials and reviews identified for additional studies.
Study selection and data extraction
Inclusion was restricted to autopsy studies of the thyroid gland in subjects without history of thyroid cancer. Studies with DTC lesions and details on at least one high-risk histological feature were included. No language or date restrictions were used.
Data extraction and quality assessment
Two reviewers (B.N. and L.R.) independently extracted data from the included trials. In the case of any disagreement between the two reviewers, a third reviewer (A.R.) extracted the data. Two independent reviewers assessed the trials for methodological quality.
Definition of outcomes
The primary outcome was the rate of “high risk” features in incidentally discovered DTC. These included (i) mETE, (ii) LN metastases, (iii) high-risk histology defined according to the 2015 ATA guidelines, (iv) multifocality, and (v) vascular invasion. The prevalence of occult thyroid cancer in each autopsy study included was a secondary outcome. Subgroup analysis was performed for year of publication, radiation exposure, and number of subjects with occult DTC included in each study.
Data synthesis and analysis
We analyzed data by calculating the event rate, with uncertainty expressed using confidence intervals [CI] (Comprehensive Meta-Analysis (CMA) v3, Biostat, NJ). We utilized a random-effect model for pooling trial results throughout the review, reflecting the heterogeneity of the populations in the included trials. Risk of bias was assessed using the COSMOS-E guidance on conducting systematic reviews and meta-analyses of observational studies of etiology (19). We assessed the heterogeneity of trial results by calculating a chi-square test of heterogeneity and I 2 measure of inconsistency.
Results
Description of the studies
Twenty-nine studies of thyroid autopsies, including 8750 subjects fulfilled the inclusion criteria, with incidentally discovered DTC in 740 autopsies (prevalence of 8.5%) (20 –48). Twenty-seven studies were identified by literature search, and two studies that were not indexed in PubMed were detected by reference screening. Reasons for exclusion are detailed in Figure 1. Included studies were published between 1966 and 2011, with most studies published before 1990 (17 of 29) (Table 1). Fourteen studies were from Europe, five from South America, three from the USA, three from Japan, two from the Middle East, and one from Singapore.
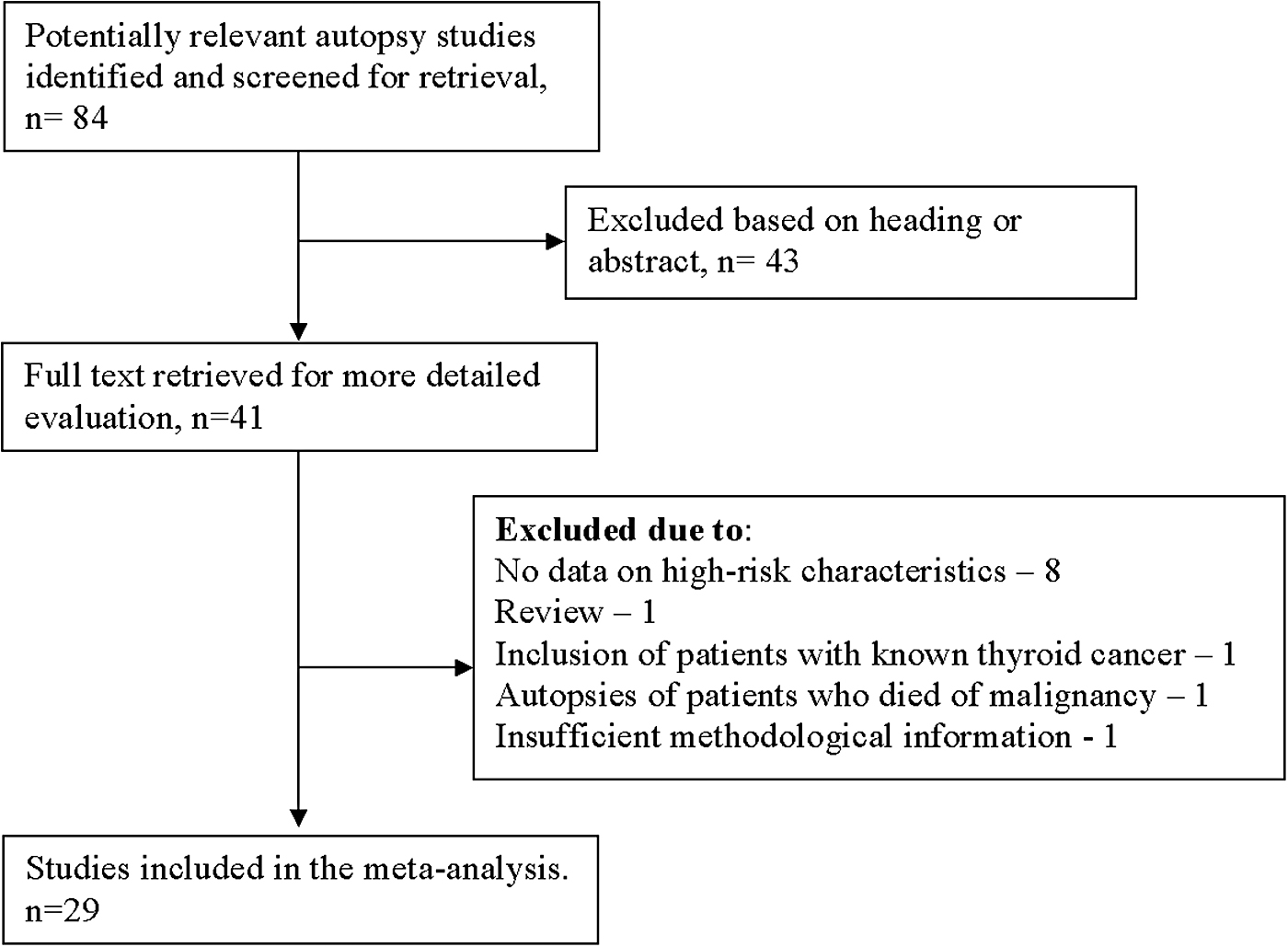
Selection process of included studies.
Included Studies
Data from the entire autopsy cohort.
Rates with partial analysis of the thyroid specimen.
DTC, differentiated thyroid cancer; F, female.
In all studies except for one, adverse histological features were secondary endpoints as part of a general description of occult DTC. Only Sampson et al. defined a high-risk feature as the primary endpoint, evaluating rates of LN metastases from occult DTC (22). Risk of bias was defined as high in all included studies due to bias in selection of participants (selection bias), bias in measurement of outcomes (information bias), and bias due to missing data (selection bias). The risk of bias is of under-reporting of histological features that were not intentionally searched for.
Rates of occult DTC
Rates of occult DTC ranged between 1% and 35.6% with a median of 7%, depending on the population evaluated and methodology of gland examination (Table 1). In studies comparing partial examination with whole thyroid examination, the rates of occult DTC ranged from 1.9% with examination of only a single block of tissue compared with 26.5% with whole examination (24), and 5.3% in sections from only grossly visible lesions compared with 22% with whole examination (39). Geographically, studies with the highest rates of occult DTC were from Japan (11.3–26.5%, with some included subjects exposed to radiation), and the lowest rates were from the USA (2.7–4%).
Other causes of heterogeneity include age, specimen processing (slices thickness), and single center versus multicenter studies (Table 1). Mean ages of the entire autopsy cohorts were reported in 17 studies, with a median reported ages of 61 years (range of means 41–68 years). Specimen processing included slices ranging from 1 to 4–5 mm. Nineteen studies were performed in a single medical center, and 10 were multicenter studies.
Adverse histological characteristics
Multifocality
Presence of more than 1 focus of PTC was reported in 27 studies (Fig. 2), with multifocality rates ranging from 9.5% to 43% of included autopsies. Using a random effect model (assuming multifocality rates are different in different populations), the calculated event rate of multifocality was 28.2% ([CI 23.1–33.8], I 2 = 46.3%). Presence of bilateral multifocality was reported in 10 studies, with bilateral event rate of 18% [CI 12.6–25.1]. Subgroup analysis for patients without radiation exposure (all studies but one) resulted in multifocality event rate of 27.1% [CI 22.2–32.7]. Analysis according to cohort size (≥30 subjects vs. <30 subjects with occult DTC) and year of publication year (≥1990 vs. earlier studies) resulted in similar event rates of multifocality (30.4% vs. 25.6%, NS; 29.2% vs. 28.3%, NS).
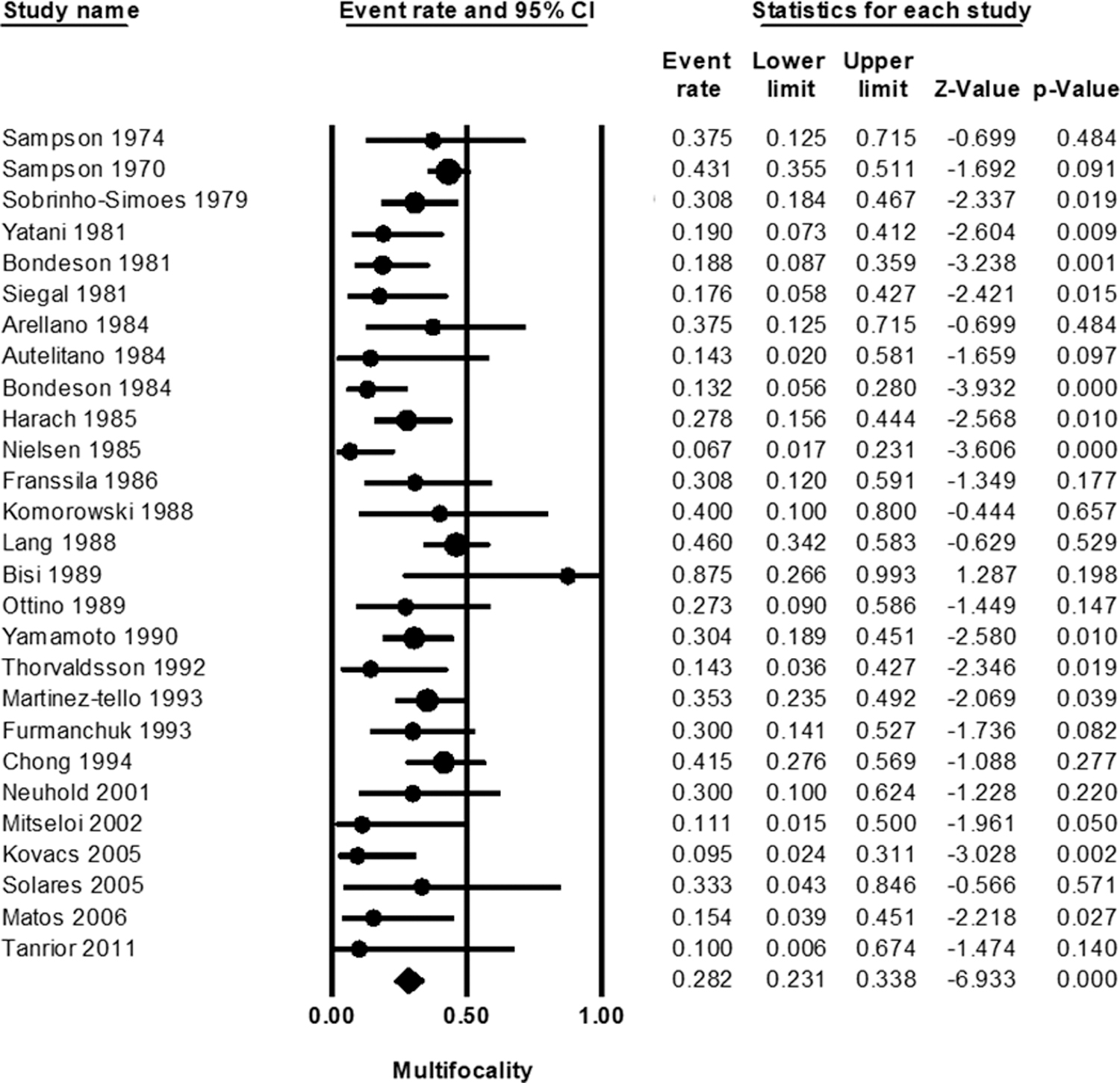
Forest plot of multifocality event rates.
Minimal extrathyroidal extension
mETE was reported in five studies, with calculated event rate of 24.5% ([CI 9.3–50.7], I 2 = 88.5%) (22,23,30,33,39). Rates in individual studies ranged widely between 7.7% and 57.5%, with a median rate of 20% (Fig. 3). The highest rates were reported by Sampson et al. (22), which included only cases where LN were available for examination, and with history of radiation exposure. Subgroup analysis excluding this study (due to risk of bias) resulted in calculated event rate of 18% [CI 10.5–29.3]. Studies with larger cohorts (3 studies with ≥30 subjects with occult DTC) resulted in higher rates of mETE compared with smaller cohorts (34.2% vs. 9.6%, p = 0.05). None of the studies defined the histological criteria for mETE, and there were no data regarding anterior versus posterior invasion.

Forest plot of minimal extrathyroidal extension event rates.
LN metastases
Thirteen studies reported the presence of LN metastases in occult PTC, with a calculated event rate of 11% ([CI 6.1–19.1], I 2 = 69.5%) (Fig. 4) (21 –23,25,26,28,31,34,36,37,39,41,42). In a study from Japan (including patients with history of radiation exposure), Sampson et al. (22) specifically evaluated 153 specimens with cervical LN available for analysis, of which 45 (29.4%) were positive for LN metastases. Most of the metastases were occult, not recognized on macroscopic examination, and LNs were minimally if at all enlarged. This study is, however, unique as it is the only one to include patients with radiation exposure, and the only one to evaluate LN metastases as the primary endpoint. When excluded, the calculated event rate of LN metastases was 9.7% [CI 5.7–16.1]. A higher rate of LN metastases was reported in small studies (6 studies with <30 occult DTC) (15% vs. 8.5%, p < 0.05), but the year of publication had no effect. None of the studies reported the size of involved LNs or LN ratio between metastatic and normal LNs.
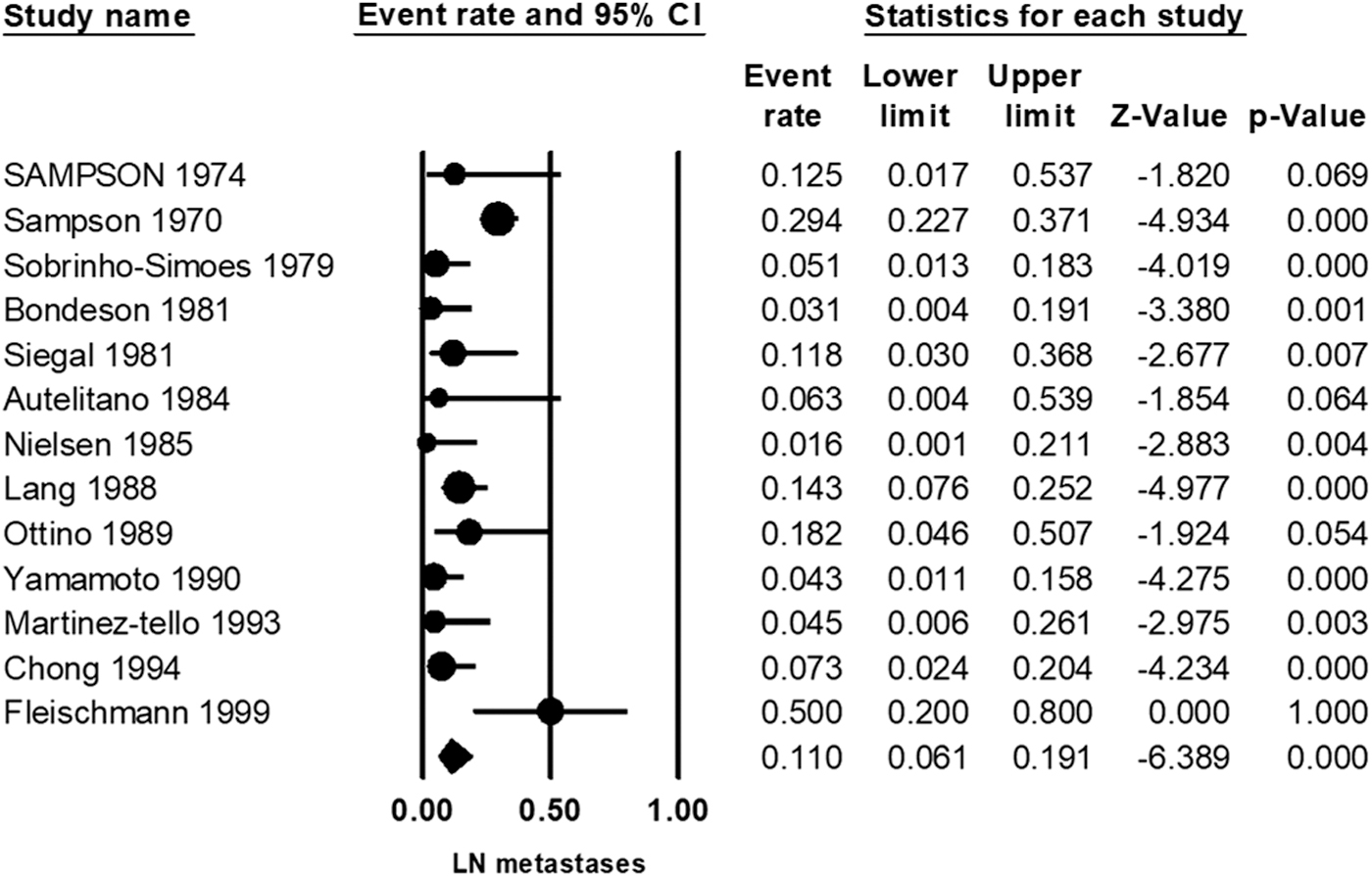
Forest plot of lymph node metastases event rates.
Lymphovascular invasion
Eight studies reported the presence of lymphovascular invasion (LVI), with a calculated event rate of 16% ([CI 4–47], I 2 = 86.8%) (Fig. 5) (22,26,27,31,35,39 –41). Subgroup analysis excluding patients with radiation exposure resulted in calculated event rate of 11.7% [CI 5.9–21.9]. Subgroup analysis for cohort size resulted in significantly higher rates of LVI in larger studies (26.1% vs. 9.6%, p = 0.012).
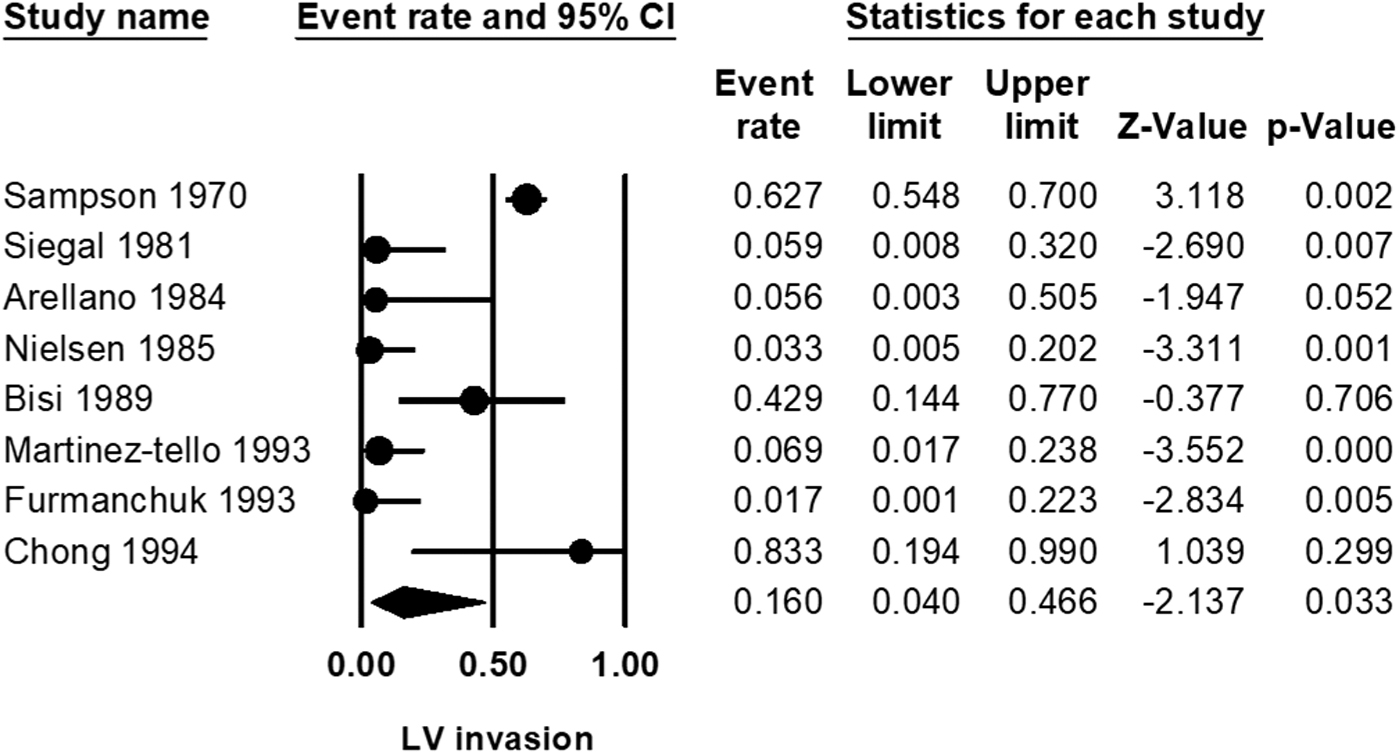
Forest plot of lymphovascular invasion event rates.
PTC variants
Variants of PTC were described in 10 studies, of which 7 reported only of classic and follicular variants (28,30,32,40,45,46,48). Three studies described cases with PTC variants associated with higher risk of recurrence (39,41,43). Martinez-Tello et al. described in 1993 a series of 29 occult PTC cases, including 9 patients with trabecular variant, 11 with sclerosing variant, and 1 with solid variant. Chong reported in 1994 of 2 diffuse sclerosing variants out of 41 occult PTC cases, and Neuhold et al. reported in 2001 of 2 tall cell variants out of 14 occult PTC cases.
Distant metastases
Thyroid examination was part of a full body autopsy in 25 of the 29 included studies (20 –30,32 –34,36 –39,41 –45,47). Data on distant metastases were described in 4 studies (including 223 subjects), and in 21 studies (including 499 subjects) there was no mention of distant metastases from thyroid cancer. Sampson et al. reported of 1 case from Nagasaki, Japan (exposed to radiation) with fatal metastatic disease out of 153 subjects with occult disease (22). The thyroid origin of his cancer was not diagnosed before his death and, therefore, was included in our analysis. Siegal and Modan reported in 1981 of 2 patients out of 17 who were diagnosed with distant metastases (26). Metastatic disease was the cause of death in one case (in whom the thyroid origin was unknown before death) and in one case the metastatic disease was an incidental finding. There were no data regarding the extent of neck disease in these cases. Two studies reported that no distant metastases were detected out of 7 and 46 cases of occult DTC (28,37).
Discussion
With the increased popularity of thyroid lobectomies for low-risk thyroid cancers based on the 2015 ATA guidelines, significant controversy has emerged regarding the impact of clinically unrecognized adverse histological features found in pathology reports after surgery. Specifically, several recent studies reported of these features in up to 30–60% of patients who were candidates for lobectomy, and would need completion thyroidectomy according to current guidelines (12 –15). This is in contrast to multiple previously published studies and meta-analyses demonstrating that thyroid lobectomy is an effective and safe surgery for low-risk DTC (49 –54).
To better understand the prevalence and significance of these histological features, we performed a meta-analysis of autopsy studies evaluating occult DTC as a model for clinically insignificant or “subclinical” thyroid cancers. Surprisingly, our results demonstrate that these “adverse” histological features are relatively common in occult DTC, with event rates of 28.2% for multifocality, 24.5% for mETE, 11% for LN metastases, and 16% for LVI.
The epidemiology of thyroid cancer, as demonstrated both by autopsy studies and by population-based studies, is characterized by a large reservoir of undiagnosed low-risk disease, and incidence that is closely related to the increased use of neck imaging (18,55,56). Specifically, in 2016, Furuya-Kanamori et al. published a meta-analysis of 35 autopsy studies, demonstrating thyroid cancer prevalence of 11.2% in people who have died of other causes. This is in comparison with only 0.3% of the U.S. population diagnosed thyroid cancer in 2018 according to the Surveillance, Epidemiology, and End Results (SEER) program (893,094 people out of 327 million) (57), so for each patient diagnosed with thyroid cancer there are ∼37 people with occult disease.
According to these numbers, it is reasonable to assume that the vast majority of subjects included in the current meta-analysis represent true occult or “subclinical” disease, with a minority of cases that might have progressed given time. These numbers may also explain the experience from South Korea with thyroid-cancer screening, showing a 15-fold increase in thyroid cancer incidence between 1993 and 2011 after the initiation of a national screening program (55). While the goal of this screening program was to detect early-stage disease to prevent progression to advanced disease, in practice, there was virtually no change in mortality rates.
In contrast to these data from large-scale studies, when lobectomy specimens from apparently low-risk patients (based on preoperative ultrasound) undergo histological evaluation, many of them are found to harbor features that are traditionally considered to increase risk of recurrence (sometimes even termed “high-risk” features), such as LN metastases or mETE. Kluijfhout et al. evaluated 1000 consecutive patients operated for DTC, of which 287 would have been eligible for lobectomy according to the 2015 ATA guidelines.
Upon review of the specimens, 122/287 (43%) patients were found to have adverse histological features that would require completion thyroidectomy (12). Similar results were reported in three other studies (13,14,34). This discrepancy may be better understood after several publications that re-evaluated the risk imposed by these histological features. In 2012, Randolph et al. published a study by the ATA surgical affairs committee, demonstrating that the prognostic significance of LN metastases can be stratified based on size, number, and extranodal extensions (17).
Small-volume microscopic N1 disease, which is sometimes found in lobectomy specimens, has little effect (if any) on the risk of recurrence. Similarly, other publications showed that mETE (defined as extension that is not seen on ultrasound or by the surgeon) has little impact on the risk of recurrence, and several studies showing little risk of recurrence associated with microscopic multifocality (9,16,58,59). This explains the current ATA risk stratification, which does not include multifocality as a risk factor, includes small central neck LN in the low-risk group, and defines mETE as low–intermediate risk.
Our study goes one step further, to evaluate these histological features in occult thyroid cancer, which are found in autopsy studies of subjects without history of thyroid cancer. We hypothesized that these features would be common in occult thyroid cancers, similar to rates the reported in low-risk disease referred for lobectomy. In the present meta-analysis, occult DTC was detected in 740 out of 8750 subjects (prevalence of 8.5%). In patients without history of radiation exposure, the most common histological feature was multifocality (27.1%), followed by mETE (18%), LVI (11.7%), and LN metastases (9.7%). Since each feature was reported separately, we could not assess the overall number of subjects with ≥1 high risk feature, but can estimate it to be more than a third of subjects.
Moreover, in 28 of the 29 included studies, high-risk histological features were secondary outcomes and, therefore, we estimate that these features were under-reported and would have been more prevalent upon in-depth inspection. Overall, the presence of these features in such a large proportion of subjects with occult disease strongly suggests a spectrum of risks, from mETE or minimal LN involvement, which seem to carry very low risk of adverse outcomes, to more significant spread that has been associated with adverse outcome in previous studies. We, therefore, suggest that early stages of these histological features should be considered as ATA low risk or low–intermediate risk, and should not be considered an automatic indication for completion thyroidectomy.
Our study has several limitations. First, most included studies (17 of 29) were published before 1990. Although the description of several histological features such as LN metastases and multifocality remained the same since that time, pathological variants of PTC have changed, and other features including vascular invasion and mETE remain controversial until this day (9,60,61). Vascular invasion has different definitions in several major guidelines (International Collaboration on Cancer Reporting data sets, World Health Organization classification, and College of American Pathologists checklist) (62) and the diagnosis of mETE has poor agreement among expert pathologists as a result of both variation in individual pathologists' interpretations and disagreement on the histological criteria for mETE (63).
These controversies emphasize the need for standardization of histopathological criteria for vascular invasion and mETE. Multifocality was assessed in most included studies, but none performed molecular analysis to determine whether these were distinct clonal primary lesions or intrathyroidal spread of a single primary lesion. Moreover, since the definition of DTC variants has changes significantly along the years, it could not be assessed in this study (64). Second, included studies employed various autopsy techniques, from studies evaluating the whole thyroid gland using 1–2 mm slices, to studies using 4–5 mm slices (Table 1). This, together with description of histological features as secondary outcomes (in all studies but one), could have led to under-reporting of some histological features.
Third, there were little data regarding distant metastases detected in autopsy. Of 25 studies with whole body autopsies (722 subjects), 3 cases of distant metastases were reported, of which 2 had fatal metastatic disease (although not considered occult disease, were included as thyroid origin was not known before death). Of note, none of the studies described the methodology of pathological examination outside the thyroid. These data are in accordance with a recent study from Memorial Sloan Kettering Cancer Center, showing that distant metastases in an apparently low-risk DTC is a rare occurrence, and is almost always found at disease presentation (65). Finally, autopsy studies may not be representative of low-risk patients who are referred for lobectomy. Indeed, the size of occult DTC in this study was mostly <1 cm (Table 1). In terms of age, the median reported ages in the included studies was 61 years (range 41–68 years), which is slightly older than age at diagnosis in current clinical practice (66).
In conclusion, histological features that are generally considered high risk for recurrence are common in occult DTC found in autopsy studies, and when minimal in size, do not seem to be markers of aggressive disease. While few of the included cases might have progressed to over time, most cases represent occult disease that would not have affected the patients' overall health or lifespan. These results may support a less aggressive therapeutic approach in patients with microscopic adverse histological features that were not detected on preoperative ultrasound.
Footnotes
Authors' Contributions
Conception of the study, data analysis and interpretation, and drafting the article by E.R.
Data collection and critical revision of the article by B.N., L.R., and A.R.
Data analysis and interpretation, and critical revision of the article by G.B., K.K., and I.S.
Conception of the study, data analysis and interpretation, drafting the article, and critical revision of the article by A.M. All authors gave final approval of the version to be published.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.