
Abstract
Background:
Iron deficiency affects thyroid hormone synthesis by impairing the activity of the heme-dependent thyroid peroxidase. The prevalence of iron deficiency is elevated particularly in pregnant women. This study aimed to investigate the effects of iron status on thyroid function in a nationally representative sample of mildly iodine-deficient pregnant women.
Methods:
The study population comprised a sample of pregnant women in Belgium during the first and third trimesters of pregnancy (n = 1241). Women were selected according to a multistage proportional-to-size stratified and clustered sampling design. Urine and blood samples were collected, and a questionnaire was completed face to face with the study nurse. Concentrations of free thyroxine (fT4), total thyroxine (T4), free triiodothyronine, thyrotropin (TSH), thyroglobulin (Tg), thyroid peroxidase antibodies, Tg antibodies, hemoglobin, serum ferritin (SF), soluble transferrin receptor, urinary iodine concentrations (UICs) were measured and body iron stores (BIS) were calculated.
Results:
Median UICs were 117 and 132 μg/L in the first and third trimesters of pregnancy, respectively (p < 0.05). The frequency of SF <15 μg/L was 6.2% in the first trimester and 39.6% in the third trimester of pregnancy (p < 0.05). UIC was a significant predictor of serum Tg concentrations (p < 0.01) but not of thyroid hormone or TSH concentrations. The frequency of fT4<percentile 10th in the third trimester of pregnancy was 24% and 14% in pregnant women with negative BIS and positive BIS, respectively (p < 0.05). SF and BIS were significant predictors of fT4 and T4 in the first trimester of pregnancy (p < 0.05). Hemoglobin was a significant predictor of fT4 in both trimesters (p < 0.01) and for T4 in the third trimester (p = 0.015).
Conclusion:
Iron deficiency, but not mild iodine deficiency, is a determinant of serum fT4 and T4 in pregnant women. Correcting iron deficiency may help to maintain optimal thyroid function, in addition to preventing anemia during pregnancy.
Introduction
Hypothyroxinemia during pregnancy has been associated with impaired cognitive function in offspring (1,2). Severe iodine deficiency is one of the main nutritional determinants of hypothyroxinemia in pregnant women. Mild iodine deficiency occurs frequently in many countries including industrialized nations (3). During pregnancy, mild iodine deficiency induces a homeostatic response to compensate for low iodine intake. However, apart from an increase in maternal and neonatal thyroid volume associated with higher thyroglobulin (Tg) concentrations, thyroid hormone and thyrotropin (TSH) concentrations are generally not affected in pregnant women and newborns (4).
Recently iron deficiency has also been identified as a determinant of thyroid function (5,6). Iron status directly affects thyroid hormone synthesis by impairing the activity of the heme-dependent thyroid peroxidase (7). Iron deficiency decreases, and iron supplements increase the efficacy of iodine supplements in iodine-deficient children (8,9). Iron deficiency is extremely frequent particularly among pregnant women, peaking at 28% and 44% in industrialized countries and developing countries, respectively (10). The public health implications arising from the effect of iron deficiency on the thyroid could be even more relevant than mild iodine deficiency considering the very high prevalence of iron deficiency in both women of childbearing age and pregnant women. During pregnancy, the requirement of both iodine and iron increases, exposing pregnant women to a higher risk of combined deficiency. Daily iron requirements are estimated at 4 and 6 mg during the second and third trimesters of pregnancy, respectively (11,12).
This study hypothesized that iron status is a nutritional determinant of thyroid function in pregnant women. Therefore we aim to investigate the effects of iron status on thyroid function in the first and third trimesters of pregnancy among a nationally representative sample of mildly iodine-deficient pregnant women in Belgium.
Subjects and Methods
Sampling
The target population comprised all pregnant women in Belgium in the first and third trimesters of pregnancy. Women were selected according to a multistage proportional-to-size stratified and clustered sampling design, with the antenatal clinic as unit of cluster. Because mild iodine deficiency is considered likely to affect thyroid function during pregnancy and because previous population-based data suggested that the prevalence of iodine deficiency is higher in the south, compared with the north of the country, the clinics were stratified by region (13). A 30-cluster survey was performed in both the north and the south of Belgium with a total of at least 20 women per individual cluster.
In each region, all antenatal clinics were ranked by province and size based on the number of deliveries over the past year. Sixty clusters of four clinics were selected using systematic sampling (although accounting for the number of past deliveries) to have sufficient replacement clinics available in case some refused to participate. Of these 60 clusters, 30 clusters were randomly selected and within each cluster the first clinic was invited to participate. In each clinic, all gynecologists were invited to participate to level out a possible gynecologist-related effect.
A questionnaire about sociodemographic and socioeconomic characteristics, smoking and alcohol consumption, thyroid diseases, and use of iodine-containing supplements was completed face to face with the study nurse. All women under current treatment with thyroid hormones or antithyroid drugs were excluded.
Body mass index (BMI) was recorded by the gynecologist during the first consultation for both first- and third-trimester pregnant women.
The study was approved by the Medical Ethics Committee of the Erasme Hospital in Brussels, and informed written consent was obtained from the pregnant women.
Assays
Maternal serum free thyroxine (fT4), free triiodothyronine (fT3), TSH, Tg, thyroid peroxidase antibodies (TPO-Ab), and thyroglobulin antibodies (Tg-Ab) were measured using a third-generation chemiluminescence immunoassay (Roche). Total thyroxine (T4) was measured by radioimmunoassay (Cisbio). Serum Tg assay was standardized against Certified Reference Material for human Tg (CRM-457). Reference values were 10.3–21.9 pmol/L for fT4, 2.8–7.1 pmol/L for fT3, 58–142 nmol/L for T4, and 0.1–4.0 mU/L for TSH as recommended (14). The reference range was 0–115 U/mL for TPO-Ab. TPO-Ab titers >34 U/mL and Tg-Ab titers >115 U/mL were considered positive.
Hypothyroxinemia and hypotriiodothyroninemia were defined as fT4 and fT3 concentrations below the 10th percentile.
Urinary iodine concentrations (UICs) were measured in duplicate by a modification of the Sandell–Kolthoff reaction using spectrophotometric detection (15). The sensitivity of the assay was 12 μg/L. The Erasme laboratory participated successfully in the Program to Ensure the Quality of Urinary Iodine Procedures, as defined by the U.S. Centers for Disease Control and Prevention (16). Urinary creatinine concentrations were determined by a colorimetric method based on the Jaffe reaction (17).
Hemoglobin and mean cell volume were measured using a Beckman Coulter ACT8 Hematology Analyzer (Beckman Coulter, Inc.). Serum ferritin (SF) and soluble transferrin receptor (sTfR) concentrations were measured by immunoassay (RAMCO).
Anemia was defined as Hb <110 g/L in the first and third trimesters (18). Severe anemia during pregnancy was defined as Hb <70 g/L. SF concentration <15 μg/L indicates iron depletion in all stages of pregnancy, and levels of <12 μg/L are associated with total depletion of iron stores (19,20). In this study, iron-deficiency anemia was defined as Hb <110 g/L and SF <15 μg/L. SF concentrations were not corrected for inflammation and, in particular, for C-reactive protein concentrations. Iron deficiency was further investigated through use of more sensitive indicators, specifically sTfR concentrations and body iron stores (BIS). Pregnant women with sTfR values more than 8.5 mg/L are said to suffer from iron deficiency (21), although there are little data on the use of sTfR values in pregnancy. BIS (mg/kg), and positive or negative values were calculated as [log(sTfR/SF) 2.8229]/0.1207 (22).
Statistical analyses
Statistical analyses were carried out using SPSS for Windows, version 26.0. (SPSS, Inc.). Normally distributed data were expressed as the mean (SD); non-normally distributed data (UIC, TSH, and Tg) were expressed as the median (25–75 percentile) and were log-transformed for further analysis. For continuous variables, differences between trimesters were tested using the Mann–Whitney test or a t-independent test. A multiple linear regression analysis was carried out with thyroid hormones, log serum TSH, and log serum Tg as dependent variables. Independent variables known or likely to be determinants of the dependent variables, gestational age, age, race/ethnicity, seasons, and log UIC/Cr, were used to build the model using the Enter method. Markers of iron status were then included separately in the model. Multiple logistic regression analysis was used to analyze the risk of hypothyroxinemia, hypotriiodothyroninemia, low T4, high TSH, and high Tg controlling for age, gestational age, and BMI.
All women undergoing treatment with thyroid hormones or antithyroid drugs, as identified from the questionnaire, were excluded from the study analysis.
A sample size calculation based on an estimated 70% prevalence of iodine deficiency (23), a 95% confidence interval, a desired precision of 5%, and a design effect of two resulted in a required sample size of 645 women in each region.
Results
Characteristics of the pregnant women
The characteristics of the 1241 pregnant women are shown in Table 1. Most pregnant women took multivitamin supplements during pregnancy. This number was even significantly higher among third-trimester pregnant women (p < 0.001). All the multivitamins prescribed for pregnant women in Belgium contained both iodine (150 μg) and iron (10 mg). In the first trimester of pregnancy, 20% of women smoked or consumed alcohol. In the third trimester, the frequency of pregnant women smoking was significantly lower (p < 0.001), but alcohol consumption was the same compared with the first trimester of pregnancy.
Characteristics of Pregnant Women by Trimester
p < 0.001.
BMI, body mass index.
Iodine and iron status
The median UIC indicates that pregnant women were at risk of mild iodine deficiency particularly during the first trimester (Table 2). By contrast, iron deficiency was significantly more frequent during the third trimester of pregnancy (p < 0.001). The prevalence of iron deficiency varies considerably according to the biomarker use to assess iron deficiency. Based on SF concentrations below 15 μg/L and negative BIS, iron deficiency prevalence was more than 6- and 10-fold higher in the third-trimester compared with first-trimester pregnant women. The significantly higher frequency of iron deficiency in third-trimester pregnant women was associated with a significant decrease of mean Hb (p < 0.001).
Thyroid Function, Iodine and Iron Status of Pregnant Women by Trimester
p < 0.001.
p < 0.05.
BIS, body iron stores; fT3, free triiodothyronine; fT4, free thyroxine; ID, iron deficiency; MCV, mean corpuscular volume; SF, serum ferritin; sTfR, soluble transferrin receptor; T4, thyroxine; Tg, thyroglobulin; Tg-Ab, thyroglobulin antibodies; TPO-Ab, thyroid peroxidase antibodies; TSH, thyrotropin; UIC, urinary iodine concentration.
Thyroid function in first- and third-trimester pregnant women
In third-trimester pregnant women, mean serum fT4 and fT3 concentrations were significantly lower and T4 higher (p < 0.001) compared with first-trimester pregnant women (Table 2). Mean serum TSH and Tg concentrations were significantly higher (p < 0.05), and hypothyroxinemia and hypotriiodothyroninemia were about 16-fold higher in the third trimester compared with the first trimester. The overall prevalence of thyroid autoimmunity was about 5% in the first trimester and lower in the third trimester, but the difference was significant only for Tg-Ab (p < 0.05).
Thyroid function and iodine status
UIC was not a predictor of serum fT4, T4, fT3, or TSH concentrations in first- and third-trimester pregnant women (Table 3). Maternal age and vitamin supplements were predictors of TSH in the first and third trimesters of pregnancy. In contrast to thyroid function, UIC was a strong predictor of serum Tg concentrations both during the first and third trimesters of pregnancy. Smoking and alcohol consumption were negatively associated with Tg concentrations, but for alcohol the association was significant only in the first trimester of pregnancy (p = 0.026).
Predictors of Serum Free Thyroxine, Thyroxine, Free Triiodothyronine, Thyrotropin, and Thyroglobulin in Pregnant Women in a Multiple Linear Regression Model by Trimester Including Separately the Indicators of Iron Status
Caucasian, Asian, African, North African, and Hispanic.
Thyroid function and iron status
The frequency of low fT4 (Fig. 1A), but not low T4 (data not shown), was significantly greater in pregnant women with negative BIS (p = 0.035) or Hb <110 g/L (p = 0.012) during the third trimester of pregnancy (the data for the first trimester are not shown because the number of negative BIS or Hb <110 g/L was small). Mean fT4 was also significantly lower in third-trimester pregnant women with negative BIS (p = 0.033) or Hb <110 g/L (p = 0.001). The frequency of low fT3 (Fig. 1B) was significantly greater (p = 0.040), and mean fT3 lower (p = 0.041) in pregnant women with Hb <110 g/L but not in pregnant women with negative BIS. Serum fT4, fT3, or T4 was not significantly different in pregnant women with SF <15 μg/L compared with pregnant women with SF ≥15 μg/L.
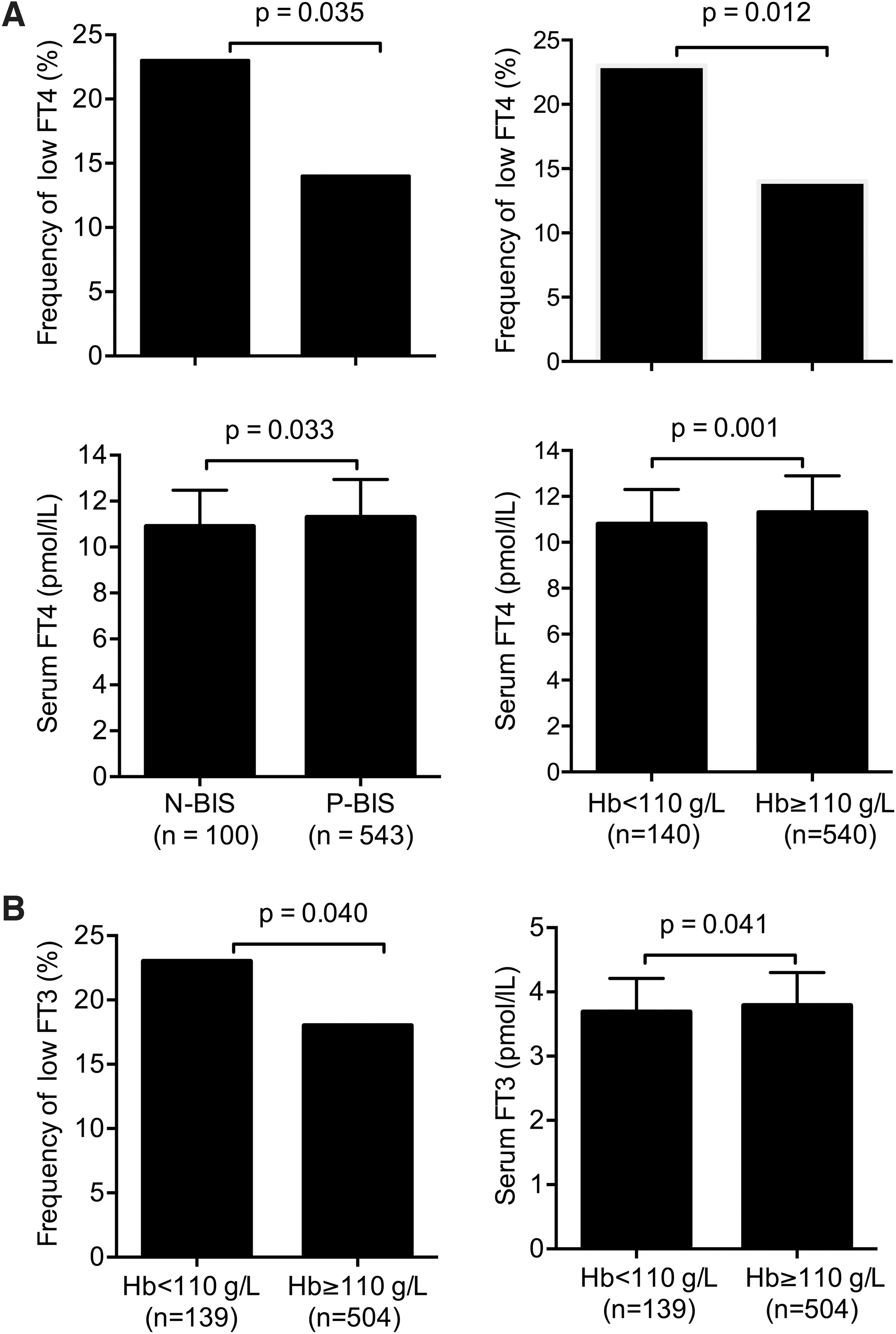
Frequency of low fT4 and mean serum fT4 in pregnant women with N-BIS, P-BIS, and with Hb <110* and Hb ≥110 g/L at the third trimester of pregnancy (
Figure 2 shows the relationship between serum fT4 and Hb in first- and third-trimester pregnant women. Serum fT4 was significantly and positively associated with Hb both in the first (p < 0.01) and third trimesters (p < 0.001). The same relationship was found for fT3 and Hb (data not shown).

The relationship between serum fT4 and Hb in first-trimester (
Table 3 shows the results of the multiple regression with fT4, fT3, T4, TSH, and Tg as the dependent variables and including separately the indicators of iron status after controlling for age, gestational age, BMI, UIC, vitamins, smoking, alcohol, and ethnicity.
BIS, SF, and Hb were significant predictors of serum fT4 concentrations in first-trimester pregnant women (p < 0.05), but only Hb was a predictor of fT4 in the third trimester of pregnancy (p < 0.0001). BIS (p = 0.020) and SF (p = 0.002) were predictors of serum T4 concentrations in the first trimester, and Hb was a predictor of T4 in the third trimester of pregnancy (p = 0.015).
For serum fT3 concentrations, sTfR was a predictor in the first trimester (p = 0.010) and Hb in both trimesters (p < 0.01). Finally, none of the iron status biomarkers was associated with TSH or Tg concentrations.
Table 4 shows the results of the multiple logistic regression, including hypothyroxinemia, hypotriiodothyroninemia, low T4, high TSH, and high Tg as dependent variables after including separately the indicators of iron status after controlling for age, gestational age, and BMI. In the logistic regression with Tg as a dependent variable, we include in the model UIC as well (the data for the first trimester are not shown because the number of negative BIS, Hb <110 g/L, or SF <15 μg/L was small).
Predictors of Hypothyroxinemia, Hypotriiodothyroninemia, Low Thyroxine, High Thyrotropin, and High Thyroglobulin in Pregnant Women in a Multiple Logistic Regression by Trimester
Low T4, T4 below the percentile 10. High TSH, TSH above the percentile 10. High Tg, Tg above the percentile 50. The data for the first trimester are not shown because the number of negative BIS or Hb <110 g/L was small.
[CI], 95% confidence interval.
The risk hypothyroxinemia was significantly lower in pregnant women with positive BIS than in pregnant women with negative BIS (p = 0.019). Pregnant women with Hb >110 g/L had also a lower risk of hypothyroxinemia than women with Hb <110 g/L (p = 0.005). The risk of hypotriiodothyroninemia was also lower in pregnant women with positive BIS, Hb >110 g/L, and also for pregnant women with SF >15 μg/L. The risk of low T4, high TSH, and high Tg was not significantly modified by iron status.
Discussion
In this population-based study, we demonstrate that iron deficiency, but not mild iodine deficiency, is a significant determinant of fT4 and T4 in pregnant women. These findings have important implications since iron deficiency is extremely frequent and because hypothyroxinemia during pregnancy can adversely affect the neurodevelopment of offspring (1,2). Our results are in line with previous studies reporting a higher risk of hypothyroxinemia, not just in iron-deficient pregnant women but also in the general population (6,24 –26). To our knowledge, this is the first population-based study showing such an association in pregnant women in a mildly iodine-deficient country. In a previous study carried out in Switzerland among second- and third-trimester pregnant women, iron status was found to be a determinant of serum T4 and TSH (6). In our population, fT4 and T4 were associated with BIS and SF in first-trimester pregnant women unlike serum TSH. These differences may be explained by a higher prevalence of iron deficiency in pregnant women from Switzerland than in Belgium. The frequency of negative BIS was 9% and 28%, respectively, in Belgium and Switzerland.
There are few other regional or hospital-based studies on iron status and thyroid function in pregnancy. Studies from two iodine-sufficient regions in China reported a significant association between iron status and fT4, but not with TSH in first-trimester pregnant women and in women of childbearing age (24,25). The prevalence of iron deficiency (ID) in China was low, only 3% of pregnant women were iron deficient. Our findings not only corroborate the results from China but also suggest that iron deficiency is a determinant of total T4 in the first trimester of pregnancy. In our study, Hb was associated with fT4 and fT3 during both the first and third trimesters. Our results indicate that anemia or iron deficiency is associated with hypothyroxinemia. In fact, during pregnancy, iron deficiency is the main nutritional determinant of Hb. Therefore, anemia can be considered in pregnant women a surrogate of severe iron deficiency. The effect of anemia on fT4 is thus secondary to the decreased heme-dependent thyroid peroxidase activity by the insufficient iron dietary supply and not due to a direct effect of low Hb on fT4.
In Belgium, a hospital-based study showed a small but significant negative correlation of SF with TSH and a positive correlation with fT4 during early pregnancy (27). The median SF in these pregnant women was 10 μg/L much lower than in our population-based study. Taken together, these data suggest that iron deficiency may affect both serum fT4 and also T4 concentrations in pregnant women.
The effect of iron status on thyroid function is not just limited to pregnant women but also affects the general population, including women of childbearing age (25). In a recent national survey of adults in a Spanish population, a significant association was found between ID and hypothyroxinemia and hypotriiodothyroninemia, but not with serum TSH (26).
In Belgium, pregnant women, particularly during the first trimester of pregnancy, are at risk of mild iodine deficiency. During the third trimester, iodine status improves because most pregnant women start taking iodine-containing multivitamins (150 μg iodine) when pregnancy is confirmed (3,28). Unlike mild iodine deficiency, the frequency of iron deficiency is relatively low in first-trimester pregnant women but increases significantly with gestational age, despite iron supplementation (14–28 mg). Two-thirds of pregnant women in Belgium take iodine-iron-containing multivitamins by the end of pregnancy although in contrast to iodine status, iron status was worse in the third-trimester compared with first-trimester pregnant women.
Interestingly, despite the fact that iron deficiency was more frequent in the third trimester of pregnancy, iron deficiency was not a determinant of fT4 concentrations in third-trimester pregnant women. This finding may be explained by the presence of other determinants of fT4 during the third trimester, which exert greater effect on fT4 concentrations than ID. Among those, there is the well-known decrease of fT4 concentrations in the third trimester, even in healthy pregnant women, attributed to poor analytic performances of fT4 immunoassays (29). In addition, physiologic hemodilution during the third trimester may also override the effect of iron deficiency on fT4 (29).
The effect of iron deficiency on fT4 and T4 in first-trimester pregnant women is of concern, given the critical role of thyroid hormones in the neurodevelopment of the fetus during the first trimester of pregnancy. At a population level, the lowering effect of iron deficiency on fT4 and T4 may affect an important number of pregnant women. In our population, 6% of first-trimester pregnant women had an SF <15 μg/L indicating iron deficiency, and 25% had an SF <30 μg/L, the cutoff for iron deficiency in the general population indicating suboptimal iron stores. At a European level, the prevalence of women of childbearing age with suboptimal BIS (SF <30 μg/L) affects 40–55% of women, while the prevalence of iron deficiency is estimated at 24–85% (30). Consequently, the prevalence of women with prepregnancy inadequate BIS is extremely high even in industrialized countries exposing pregnant women to a higher risk of thyroid dysfunction.
In addition to iron deficiency, iodine deficiency, if severe enough, also increases the risk of hypothyroxinemia during pregnancy (31,32). The potentially adverse consequences of combined iron and iodine deficiency on fetal neurodevelopment must be considered, given the high frequency of both micronutrient deficiencies worldwide. In our population of pregnant women, iodine status was a determinant of Tg concentrations, but not of thyroid hormone or TSH concentrations. This situation is frequently observed in mildly iodine-deficient regions such as in Belgium. Iodine supplements taken during pregnancy by mildly iodine-deficient pregnant women significantly decreased Tg concentrations in mothers and in newborns, but did not modify thyroid hormone concentrations (4). Consequently, it is unlikely that mild iodine deficiency will increase the risk of hypothyroxinemia in our population of iron-deficient pregnant women. However, we have considered this eventuality (data not shown). We found that the frequency of hypothyroxinemia was no different in pregnant women with combined iodine and iron deficiency (grouped in quartiles according to UIC and SF) when compared with women with iron deficiency alone. The situation can be different in countries where iron and iodine deficiencies are more severe. The combined effect of both deficiencies could increase the risk of severe hypothyroxinemia during pregnancy and thus has an adverse effect on the development of fetus.
Iron deficiency during perinatal and early life may impair the optimal neurodevelopment of children (33,34). In addition, experimental rodent models of iron deficiency have shown that maternal hypothyroxinemia decreases neonatal triiodothyronine (T3) concentrations in the brain (35). The lowering of neonatal brain T3 concentrations was associated with a reduction of thyroid-responsive genes in the neonatal cerebral cortex and hippocampus (36). In addition, iron-deficient pups showed retarded sensorimotor skills. Interestingly, the occurrence of hypothyroxinemia precedes brain iron depletion, suggesting that brain and Hb synthesis is protected to some extent from iron deficiency at the expense of iron-containing enzymes such as TPO.
One strength of the present study is that it is a population-based study. In addition, and unlike previous studies, we also measured total T4 and fT3. The study design and the finding that iron deficiency was a determinant of fT4 and also of T4 reinforce the potential effects that iron status has on thyroid function.
The main limitation of the study is that pregnant women taking iodine–iron supplements were not excluded. The frequency of pregnant women taking supplements was high in the first trimester and even higher in the third trimester. The inclusion of pregnant women taking iron supplements may have underestimated the effect of iron deficiency on thyroid hormone concentrations. However, the fact that iron deficiency increases significantly in the third trimester of pregnancy suggests that the effect of iron supplementation has little impact on pregnant women's iron status and is unlikely to affect thyroid function.
In conclusion, this is the first population-based study suggesting that iron deficiency, unlike mild iodine deficiency, is a determinant of fT4 and T4 in pregnant women. Our results support the correction of iron deficiency before pregnancy or during early gestation, not just to avoid anemia but also to maintain optimal thyroid function and normal fetal development. Given the high prevalence of pregnant women and women of childbearing age with iron deficiency, our findings require urgent further investigation. The public health implications of iron deficiency on thyroid function may be even more relevant for pregnant women living in regions where the risk of severe iron and iodine deficiency is greater than in industrialized countries.
Footnotes
Acknowledgments
We thank the hospitals and gynecologists who agreed to participate and all the participating pregnant women.
Authors' Contributions
R.M.-R. and S.V. designed and coordinated the research. R.M.-R., B.C., and S.V. wrote the article. C.D., F.W., and C.F.P. contributed to data interpretation of the results and critically revised the draft versions of the article.
Disclaimer
The article has been submitted solely to this journal and is not published, in press, or submitted elsewhere.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by funding from the Belgian Federal Public Service of Health, Food Chain Safety and Environment.