
Abstract
Background:
The syndrome of thyrotoxicosis typically relies on radioactive iodine scans for establishing its etiology. Alternatively, the determination of thyrotropin (TSH) receptor antibodies (TRAbs) helps to distinguish Graves' disease (GD) from thyrotoxic thyroiditis. Current assays are impacted by limitations in sensitivity and/or turnaround time. Therefore, we decided to test a new assay for the detection of TSH receptor stimulating antibodies (TSAbs) and compare it with the clinically available assays.
Methods:
We enrolled 110 individuals in 5 cohorts: patients with incident or recurrent GD (cohort 1); patients with thyroiditis, painless or subacute (cohort 2); patients with Graves' orbitopathy/thyroid eye disease (TED) in cohort 3; patients with Hashimoto's thyroiditis (cohort 4), and a control group of normal volunteers (cohort 5). The patients were tested with the two clinically available assays: Roche Elecsys anti-TSHR assay (ROC-TBII) from Roche Diagnostics and Thyretain™ TSI Reporter BioAssay Kit (QUI-TSI) from Quidel. In addition, the samples were tested with the aequorin TSAb assay (OTS-TSI) provided by Otsuka Pharmaceutical Co., Ltd. (Tokyo, Japan). The data were collected in a cross-sectional manner before initiation of therapy.
Results:
We had 36 cases of GD, 17 cases of thyroiditis, 27 cases of TED, 10 cases of Hashimoto's thyroiditis, and 20 normal volunteers. OTS-TSI had 100% sensitivity and specificity in distinguishing GD from thyroiditis, identical with QUI-TSI but superior to ROC-TBII (sensitivity 86% and specificity 94.1%). OTS-TSI had 93% sensitivity and 100% specificity for the diagnosis of TED, compared with normal controls. QUI-TSI and ROC-TBII performed similarly in this analysis, demonstrating 82% sensitivity and 100% specificity. The range of detectable values for OTS-TSI was 20–29,000 mIU/L and the turnaround time was ≤6 hours, without the need for cell culture equipment.
Conclusions:
OTS-TSI performed excellently, though similarly to QUI-TSI, for the differential diagnosis of GD vs. thyroiditis, while being superior in that respect to ROC-TBII. Furthermore, OTS-TSI has superior sensitivity to QUI-TSI and ROC-TBII for TED diagnosis, while retaining high specificity. It has a short turnaround time and avoids the need for cell culture and sterility. Larger studies in U.S. populations are needed for its validation.
Introduction
Thyroid autoimmunity manifesting as Graves' disease (GD) is the most common cause for thyrotoxicosis in patients not treated with thyroid hormone therapy (1). The entities that most likely mimic this form of thyrotoxicosis are represented by thyroiditis, both painless and subacute (2). With an acute onset and without a nodular thyroid on palpation, these cases of inflammatory thyroiditis typically require an iodine scan and uptake for correct diagnosis. However, at times, that is not feasible (e.g., pregnancy, breast feeding, and recent iodine exposure) or is not easily available in some medical facilities.
The measurement of thyrotropin receptor antibodies (TRAbs) can obviate this step (1) and is thus extremely valuable. The TRAb titer can be measured by a competitive-binding assay, known as thyrotropin receptor-binding inhibitory immunoglobulin (TBII), with labeled thyrotropin (TSH) or a monoclonal thyrotropin receptor (TSHR) antibody (3).
TBII, however, cannot discriminate between stimulating, blocking, or neutral antibodies against the TSHR. Conversely, the thyroid-stimulating immunoglobulin (TSI) bioassay can measure the stimulating component of TRAb and is more sensitive for the diagnosis of GD (3,4) and more closely associated with the pathogenesis of autoimmune thyroid disease. However, current TSI bioassays require tissue culture techniques and overnight incubation of the cell lines used in the assay (5) that may lead to day-to-day assay variability. Using a TSI bioassay without tissue culture requirements and with a shorter turnaround time may lead to improvements over the current assays.
Recently, we tested a new aequorin TSH receptor stimulating antibodies (TSAbs) bioassay (developed by Otsuka Pharmaceuticals) with a turnaround time of six hours and that utilizes ready-to-use frozen cells that express full-length human TSHR, cyclic nucleotide-gated calcium channel (CNG), and aequorin (6) (Fig. 1). In this study we aimed to test whether this new assay is able to (i) correctly diagnose GD versus thyroiditis (subacute and painless) and (ii) identify the presence of TSI in patients with Graves' orbitopathy/thyroid eye disease (TED).

Principle of Otsuka TSAb assay (OTS-TSI). Ligation of TSHR by TSI leads to the activation of adenylate cyclase with production of cAMP. Through activation of a Ca2+ channel, cAMP increases intracellular calcium concentration with generation of aequorin luminescence. The luminescence is directly proportional to the titer of TSI antibodies. OTS-TSI, Otsuka TSI; TSAb, TSH receptor stimulating antibodies; TSHR, thyrotropin receptor; TSI, thyroid-stimulating immunoglobulin.
Materials and Methods
Patient cohorts
A total of 110 individuals were included in this study and distributed as follows. Cohort 1 included patients with incident or recurrent GD, all having had the diagnosis confirmed by biochemical thyrotoxicosis combined with high-normal or elevated and diffuse radioactive iodine (RAI) uptake in the thyroid, independent of TRAb values. Cohort 2 included the main diagnostic comparison group—patients with thyroiditis (painless and subacute)—and required a 24 hours 123I thyroid uptake of <3%. We also included patients with Graves' orbitopathy/TED in cohort 3, as follows: one subgroup with active TED (clinical activity score [CAS] ≥3) and thyroid disease, second subgroup with inactive TED (CAS <3) and thyroid disease, and third subgroup with euthyroid TED either active or inactive (patients with clinical features and orbital imaging consistent with TED yet without any history of thyroid abnormalities).
As control groups, patients with Hashimoto's thyroiditis (cohort 4) and a control group of normal volunteers (cohort 5) were included. The latter cohort did not have any biochemical thyroid abnormalities and had a normal thyroid ultrasound. All the inclusion and exclusion criteria for the various cohorts are listed in Supplementary Data S1.
The study was approved by the Mayo Clinic Institutional Review Board and all patients signed informed consent, confirming their agreement to participate in the study. Furthermore, the authors confirm that the study overall and all its research steps meet ethical guidelines and were performed in compliance with the regulatory environment of the United States.
Laboratory assays for thyroid function and autoantibodies
Serum free thyroxine (fT4), total triiodothyronine (TT3), and TSH were measured at Mayo Clinic Laboratories using the Roche Elecsys electrochemiluminescence immunoassays on a Roche Cobas analyzer (Roche Diagnostics, Indianapolis, IN). TSI was measured by QUI-TSI (Quidel, San Diego, CA), a luciferase reporter gene assay. Patient results are compared against a reference control to calculate a TSI index. TSI index values >1.3 are considered positive. QUI-TSI values <1.0 (lowest limit of quantitation [LOQ]) were estimated at 50% of that value (0.5) for calculation purposes.
TRAb was measured by ROC-TBII (Roche Diagnostics), a third-generation competition-based assay standardized against the National Institute for Biological Standards and Control (NIBSC) 1st IS 90/672 Standard (reference range 0–1.75 IU/L). ROC-TBII values <1.0 (LOQ) were estimated at 50% of that value (0.5 IU/L), whereas values >40 IU/L (upper limit of quantitation) were estimated at 150% of that value (60 IU/L) for calculation purposes. The aequorin TSAb assay kit, OTS-TSI, measures the presence of TSH receptor stimulating immunoglobulin and was provided by Otsuka Pharmaceutical Co., Ltd. (Tokyo, Japan).
The TRAb activates the TSHR, increasing intracellular cAMP levels and leading to the direct activation of the CNG. Calcium influx through the CNG leads to emittance of a blue light from the intracellular aequorin (Fig. 1). As this assay utilizes the rapid cell signaling cascade within cells and does not require de novo gene expression and protein synthesis, it can be run in four hours incubation under nonsterile conditions.
The OTS-TSI assay was performed in 25 μL of serum as described previously (6). The samples were analyzed in batches of 37 samples per batch (plate). The total assay time for the result was five to six hours. The assay is standardized against the NIBSC 2nd IS 08/204 Standard. The reference range is ≤35 mIU/L (6,7). OTS-TSI values <20.0 mIU/L (LOQ) were estimated at 50% of that value (10 mIU/L) for calculation purposes. Since OTS-TSI and ROC-TBII assays are standardized against different international standards, the quantitative results from these assays are not directly comparable.
Statistical analysis
Group statistics for the continuous variables is expressed as mean ± standard deviation or median with interquartile range (IQR), depending on the normalcy of distribution. Comparison of individual variables between groups was performed using two sample test or Mann–Whitney U-test as indicated. Nominal variables were summarized as frequencies and percentages and compared by Pearson's chi square test. The sensitivity and specificity were computed at the manufacturer-specified threshold and at additional thresholds over the range of OTS-TSI values.
Receiver operator characteristics (ROC) curve analyses (Analyse-it for Excel) were performed to estimate the optimal threshold for differentiations of GD, TED, and thyroiditis cases. Statistical graphs and plots were prepared with MedCalc Software Ltd version 19.17 (Ostend, Belgium). We used Jonckheere–Terpstra test to evaluate the trend of OTS-TSI values along the TED subgroups. p-Value <0.05 was considered the cutoff for significance.
Results
Populations studied and their characteristics
Altogether we included 110 individuals in this study. They were separated into five cohorts as described in the Materials and Methods section: C1 (thyrotoxicosis secondary to GD) had 36 cases; C2 (thyrotoxicosis secondary to thyroiditis) had 17 cases: 10 with painless thyroiditis and 7 with subacute thyroiditis; C3 (TED) had 27 cases: 15 active and 12 inactive TED cases, including 5 cases (4 with active disease) of euthyroid TED; C4 (Hashimoto's thyroiditis) included 10 cases and C5 (healthy controls) included 20 cases. The age, sex distribution, and thyroid hormone values of the different cohorts included in the study are detailed in Table 1. There were 63 patients with clinical manifestations of autoimmunity toward the TSHR.
Baseline Characteristics of the Overall Study Population
CAS, clinical activity score; GD, Graves' disease; NA, not applicable; SD, standard deviation; TED, thyroid eye disease; TSH, thyrotropin.
Cohort 1 included 34 index cases of GD and 2 cases of recurrent disease, while cohort 2 included only index cases of thyrotoxicosis. All initial study evaluations were performed before patients received any therapy. Cohort 3 included 7 thyrotoxic patients and 5 hypothyroid patients, while the rest (15 patients) were euthyroid (5 euthyroid TED, 2 patients on antithyroid drugs, and 8 patients on levothyroxine—7 postablation for GD and 1 for Hashimoto's thyroiditis with hypothyroidism). Six out of 10 cohort 4 cases were on thyroid hormone therapy at time of evaluation.
Range of assay values
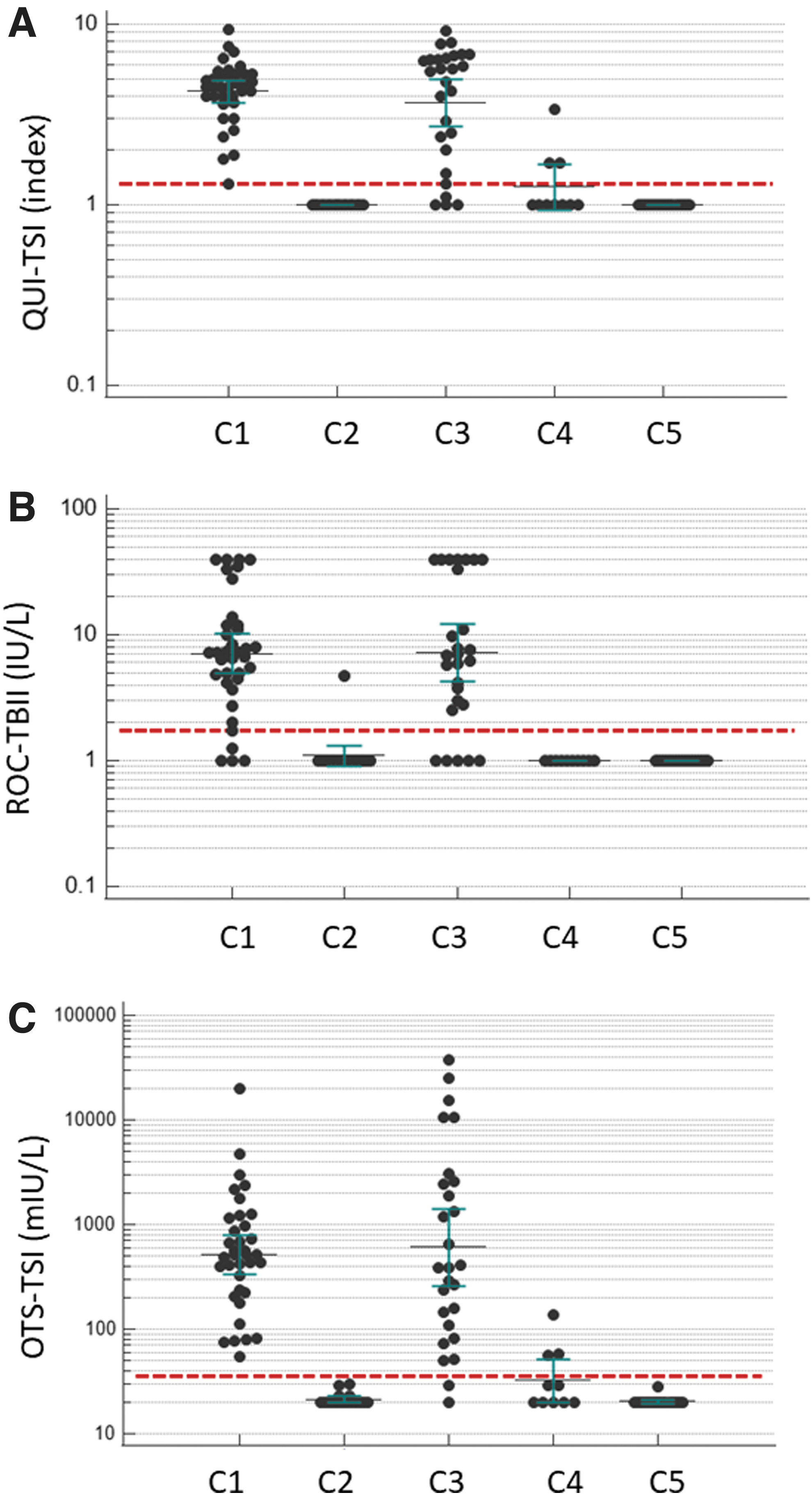
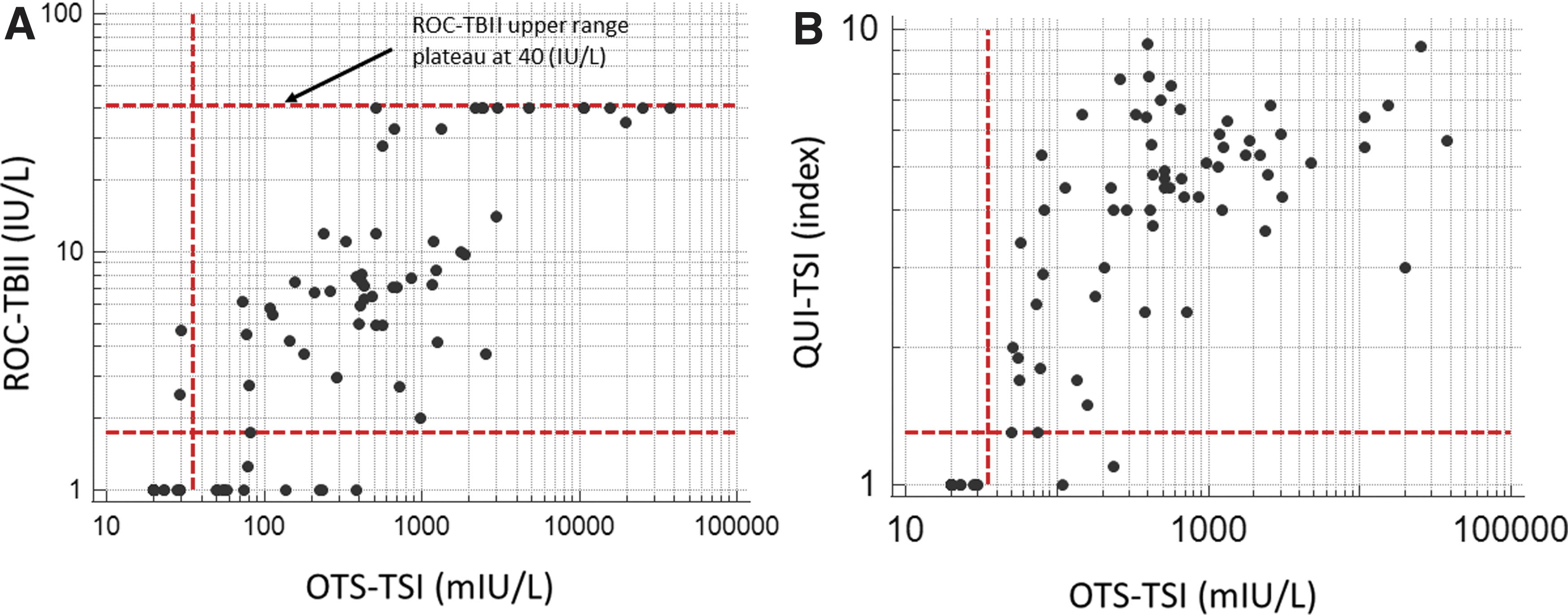
OTS-TSI assay covered a very broad range of values from the lower limit of detection of 20 mIU/L to the upper end of normal values up (35 mIU/L) and then to abnormal values as high at 29,000 mIU/L (Fig. 2A–C). This contrasts with ROC-TBII that plateaus at 40 IU/L and QUI-TSI assay that plateaus at an index of ∼10 (Fig. 3A, B). From a functional perspective, it is interesting that both OTS-TSI and ROC-TBII titers (in GD patients) had a statistically significant linear correlation with TT3 values (r = 0.47 and 0.65, respectively) but only ROC-TBII had such a relationship with fT4 (r = 0.38), while QUI-TSI did not correlate with either TT3 or fT4.
Sensitivity and specificity data
To calculate the sensitivity and the specificity of the assay, we performed three receiver operating curve (ROC) plot analyses. The first ROC analysis found that OTS-TSI had an optimal sensitivity and specificity of 100% for discriminating between cases of GD (cohort 1) from those of thyroiditis (cohort 2). This performance was superior to QUI-TSI in sensitivity (97%) but identical in specificity and it was superior to ROC-TBII in both aspects (sensitivity 86% and specificity 94%) (Table 2).
OTS-TSI Assay Performance and Comparison with Available Clinical Assays
OTS-TSI comparison with QUI-TSI and ROC-TBII for the main clinical assay utilizations, differential diagnosis of GD, and TED.
CI, 95% confidence interval; OTS-TSI, Otsuka TSI; QUI-TSI, Quidel TSI; ROC-TBII, Roche TBII; TBII, thyrotropin receptor-binding inhibitory immunoglobulin; TSI, thyroid-stimulating immunoglobulin.
We then performed the second ROC analysis focusing on the ability of the assays to detect autoimmunity against the TSHR. To this effect, 63 patients with diagnoses indicating such pathophysiology (C1+C3) were compared with the normal controls (C5). OTS-TSI had an ROC area under the curve (AUC) of 0.99, a sensitivity of 97%, and specificity of 100% (Table 2) compared with QUI-TSI having an ROC AUC of 0.98, 91% sensitivity, and 100% specificity. ROC-TBII had the lowest sensitivity at 84% and specificity at 100% for TSHR autoimmunity with an ROC AUC of 0.94 (Table 2).
Subsequently the subset of 27 TED patients was compared with the normal cohort (C5) to understand the utility of the assay in the diagnosis of TED (third ROC analysis). We found that OTS-TSI has 93% sensitivity and 100% specificity, compared with QUI-TSI and ROC-TBII having identical 82% and 100% sensitivity and specificity, respectively (Table 2).
All TED cases with manifest thyroid disease had positive OTS-TSI (thus 100% sensitivity for this subgroup) but the assay was positive in only 60% (3 of 5 cases) of euthyroid TED cases. QUI-TSI was positive in only 2 of the 5 patients (both identified by OTS-TSI), while ROC-TBII was positive in 3 of these 5 cases, 2 overlapping with OTS-TSI. One euthyroid patient had all TRAb assays negative yet clinical inflammatory eye changes (CAS 4) and persistent diplopia with involvement of medial rectus muscles. The work-up was negative for myositis and lymphoma and after two years of monitoring, when inflammatory features resolved, the patient underwent strabismus surgery. Operative findings were consistent with TED.
In contrast, 3 out of 10 (30%) patients with Hashimoto thyroiditis had positive OTS-TSI and QUI-TSI (same patients), yet none of these cases tested positive on ROC-TBII. The actual OTS-TSI titers in these cases were in the low range of the assay, between 56 and 136 mIU/L. Furthermore, in the thyroiditis cohort and the healthy control cohort, no individuals had positive OTS-TSI or QUI-TSI results, while one case of thyroiditis had positive ROC-TBII at 4.7 IU/L.
For optimal sensitivity and specificity, the cutoff limit for a positive OTS-TSI test was selected at >35 mIU/L, in accordance with the published data from Japan (6,7), and with that cutoff value the individual data obtained from the three assays are shown in Figure 2A–C, respectively.
Feasibility of use
Our laboratory experience with the OTS-TSI assay resulted in a turnaround time of six hours from the time the sample was received in the laboratory to the time the result became available. Overall, the turnaround time was <2 hours for ROC-TBII and 2 days for QUI-TSI. From a processing perspective we found the assay to be easily implemented by our technicians after training from the OTS-TSI assay manufacturer.
Discussion
Our study showed that the aequorin TSAb assay (OTS-TSI) has excellent sensitivity and specificity in differentiating the thyrotoxicosis of GD from that of painless and subacute thyroiditis, displaying similar results to QUI-TSI but superior to ROC-TBII. Furthermore, it is superior in sensitivity in detecting stimulating antibodies against the TSHR in TED cases in comparison with both QUI-TSI and ROC-TBII assays, while retaining a high specificity. Historically the second generation TBII assays had a false-positive rate of up to 15% in patients with silent thyroiditis (8), while the third generation TBII assay provided by Roche has a reported sensitivity and specificity of 99% in patients with untreated GD (9). For the GD patients already on antithyroid drugs, the sensitivity declines to 89% while the specificity remains at 99%.
A meta-analysis of studies including untreated hyperthyroid patients identifies the 3rd generations TBII assays having 97% and 99% sensitivity and specificity, respectively (10). Our review (3) of the available data indicates that TSI assays have a range of sensitivity of 80–100% and specificity of 90–100%, depending on the selected cutoff TSI index from 1.3 to 1.8 (11). It is important to consider that in cases of painless thyroiditis when TBII and TSI assays were studied head-to-head, the TSI assay was more reliable having 99% negative rate, compared with 95% for TBII (12).
Our data replicate those findings. Regarding the sensitivity of the OTS-TSI assay in TED patients, we find it to be higher than both comparison assays, while all retain a very high specificity. Given the relatively low sensitivity of all assays in euthyroid TED and the only partial overlap in positivity in these cases, our data indicate potential benefit from obtaining both TSI and TBII testing in these patients. It is likely that in some euthyroid TED cases, like in some GD cases that transitioned to hypothyroidism (12), blocking and neutral antibodies resulting from epitope shifting (13) dominate the pathophysiology and that is why TSI might be negative in these patients.
Current TSI assays express the chimeric human TSHR, which has the amino acids 262 to 335 substituted with 73 amino acids from the rat LH receptor (5), whereas OTS-TSI employs the full-length human TSHR. However, TRAbs are heterogeneous antibodies that have different binding sites on the alpha subunit of the TSHR (14) and presumably some of those antibodies would be unable to bind to the TSHR chimeric section (due to the rat LH receptor segment) of the current TSI assays, affecting their sensitivity. By design, OTS-TSI assay should be able to detect these antibodies, but our small sample size does not allow us to draw a clear conclusion. Further studies will be required to address the antibody binding sites and the molecular mechanisms for the discrepancies of the different assay systems.
Some of the advantages of the OTS-TSI assay compared with current bioassays is the short turnaround time (<6 hours) compared with QUI-TSI (48 hours). In contrast with QUI-TSI, the OTS-TSI assay does not require de novo gene expression and protein synthesis, hence, the need for cell culture and sterile conditions for performing the assay is not necessary. This leads to improved workflow, decreased time and costs in the laboratory. From a practical perspective, it is important to note that TSI assays are not affected by biotin interference, a more common problem these days for some TBII assays due to the large number of over-the-counter high-dose biotin supplements (15).
The standard method of diagnosing the cause of thyrotoxicosis relies on the RAI scan and uptake study. This takes between 6 and 24 hours, requires at least 2 visits to the nuclear medicine department and is few times more expensive than current TRAb assay costs. Furthermore, the use of RAI studies is precluded by the prior use of iodinated contrast material or the use of any iodine-containing medication (e.g., amiodarone). The use of this test is also contraindicated during pregnancy and it must be performed with special precautions during lactation. These scenarios indicate the type of patients where TRAb measurement becomes extremely important for the differential diagnosis of thyrotoxicosis. In addition, the short turnaround time could provide significant benefit for clinicians dealing with severely thyrotoxic patients by allowing for earlier initiation of therapy while likely reducing overall care costs.
The broad range of TSI values displayed by the patients with TSHR autoimmunity could also be an advantage for the OTS-TSI assay. While this wide spectrum of values is not needed for diagnostic utility, they invite speculation on their potential prognostic value regarding the course of TSHR autoimmunity. A larger prospective longitudinal study will be required to understand whether these values can be predictive of the likelihood of GD remission, the risk of TED development, or its course.
We are currently still following the patients in our study and plan to report a medium-term analysis on these items in the future. From that perspective, it is intriguing that in our limited data set, we do note that OTS-TSI values are strongly correlating with baseline TT3 values (though not with fT4) in cohort 1 and that they are highest in the group of patients with active TED and thyroid disease (median 1864 mIU/L, IQR 387–10,727), intermediate in the group of inactive TED with thyroid disease (median 382 mIU/L, IQR 158–2458), and lowest in the group without history of thyroid disease, euthyroid TED (median 51 mIU/L, IQR 29–81, p < 0.001). A larger study might also answer the questions whether different cutoff points might work better in the North American population than the cutoff of 35 mIU/L identified for the Japanese population (see exploratory analysis in Supplementary Data S2).
The values measured with OTS-TSI assay are expressed in mIU/L and reported to a different NIBSC Standard (2nd IS 08/204), which explains some of the differences in values and magnitude in reference to ROC-TBII (expressed in IU/L). Further differences are related to the increase in affinity of OTS-TSI for the stimulating TRAb while ROC-TBII will, by definition, capture blocking and neutral TRAbs that are outside the scope of TSI assays.
With regard to result differences between OTS-TSI and QUI-TSI, it is pertinent that QUI-TSI is a semiquantitative assay and the value is expressed as index %. It will, therefore, have a plateau effect at high value ranges, as noted in Figure 3B. In contrast, OTS-TSI is designed as a quantitative assay and higher values can be obtained with calibration curve after dilution. To allow this, OTS-TSI assay employs aequorin luminescence that delivers high signal-to-noise ratio, thus avoiding the plateau effect.
Limitations
This study represents a small pilot study and its results will need validation in a larger cohort. For example, Roche Elecsys anti-TSHR assay was tested on samples from 436 apparently healthy individuals and 312 patients with thyroid diseases. Furthermore, we did not include patients with toxic multinodular goiter or toxic adenoma given that the physical examination combined with ultrasound use would likely eliminate them from the differential diagnostic of thyrotoxicosis. However, these populations should also be considered in a subsequent validation study along with a much larger cohort of healthy controls.
Conclusions
We described here the clinical performance of the OTS-TSI assay and found it to perform excellent though similar to QUI-TSI for the differential diagnosis of GD versus thyroiditis, while being superior in that regard to the ROC-TBII assay. Furthermore, it has superior sensitivity to QUI-TSI and ROC-TBII in the diagnosis of TED while retaining their high specificity. It has a short turnaround time and avoids the need for cell culture and sterility. Larger studies in U.S. populations will be needed for its validation. At that point, the appealing question whether its wide range of values can have a predictive role in managing GD and TED might also be answered.
Acknowledgments
We acknowledge and thank the Mayo Clinic BioPharma Diagnostics team and Dr. Adrian Vella and his laboratory team for the logistical support they have provided for this project. We also thank Dr. Tao Wang for the methodological insight and the critical review that he provided during the study.
Authors' Contributions
M.N.S. designed the study, acquired the data, interpreted the data, drafted the article, and approved the final version. A.A.-S. and P.T. analyzed and interpreted the data, revised the drafted article, and approved its final version. N.A. designed the study, acquired the data, interpreted the data, revised the drafted article, and approved the final version. V.M. interpreted the data, revised the drafted article, and approved the final version.
Footnotes
Author Disclosure Statement
M.N.S. receives medical consulting fees from Siemens Health care Diagnostics Inc. and Third Rock Ventures and declares no conflict of interest with this study. A.A. and P.T. have no disclosures. V.M. serves on the board of directors for JSS Research Foundation, USA, INC, and declares no conflict of interest with this study. N.A. is employed by Otsuka Pharmaceuticals Co. Ltd.
Funding Information
The study was funded by Otsuka Pharmaceuticals Co. Ltd., through grant OTP001_17 ENDO.
Supplementary Material
Supplementary Data S1
Supplementary Data S2