
Abstract
Background:
Despite the implementation of the universal salt iodization (USI) program for correction of iodine deficiency in China for ∼20 years, the actual iodine nutrition status of Chinese residents and the prevalence of iodine deficiency and iodine excess are issues that need to be addressed. This nationally representative cross-sectional study was conducted across all 31 provinces of mainland China to gather extensive data on iodine nutrition status and the influential factors.
Methods:
This study included 78,470 participants, aged 18 years or older, who were interviewed and asked to answer a questionnaire. Urine iodine concentration (UIC) was measured by the inductively coupled plasma mass spectrometry method, and goiter was examined by thyroid ultrasonography. In addition, sixty 9–11 years old school children in each province were randomly selected to evaluate the UIC and thyroid ultrasonography. The iodine nutrition status was determined according to the World Health Organization guidelines.
Results:
The iodized salt coverage was 95.37%. The median urine iodine (MUI) was 177.89 μg/L (interquartile range [IQR], 117.89–263.90 μg/L) and goiter prevalence was 1.17% (confidence interval [95% CI 0.95–1.43]) in the adult population. The MUI was 199.75 μg/L (IQR, 128.41–303.37 μg/L) in school-age children, and goiter prevalence was 3.50% [95% CI, 2.93–4.13]. The percentage of individuals with UIC <50 μg/L was 3.43%, <20%. Analysis indicated that sex, age, geographic factors, body mass index, and smoking habits influence the iodine nutrition level.
Conclusion:
The mandatory USI program has successfully eliminated iodine deficiency disorders, and the findings indicate that the iodine nutrition level in the general population is within the safe range.
Introduction
Iodine is a necessary element for thyroid hormone synthesis. Iodine deficiency can cause iodine deficiency disorders such as cretinism and goiter. According to data published by the World Health Organization (WHO) in 1993, one-third of the world's population was at risk of iodine deficiency. For the same year, the estimated goiter prevalence worldwide was 12% (1), and it was 20.4% in China (2). Thereafter, the WHO called for universal salt iodization (USI) programs around the world, and China implemented the USI program in 1996.
After this, the iodized salt coverage has been >90%, and the median urinary iodine (MUI) of children aged 8–10 years in China increased from 164.8 μg/L in 1995 to 330.2 μg/L in 1997. Furthermore, the prevalence of palpable goiter in China declined dramatically from 10.9% in 1997 to 5.0% in 2004, and it continued to decrease to 2.4% in 2011, based on the findings of ultrasonography examinations. The iodized salt coverage, goiter prevalence, and MUI data from iodine deficiency disorder surveillance by the Chinese Disease Control Center are given in Supplementary Table S1.
In the 5 years after implementation of the USI program in China, the MUI values continued to be >300 μg/L (normal range = 100–200 μg/L). The epidemiological investigation has shown that excessive iodine levels increase the risk of certain thyroid diseases (3). There have also been concerns about excessive iodine intake caused by salt iodization. When the USI policy was first implemented in China, the standard levels set for iodized salt were “not less than 40 mg/kg at the factory level, and not less than 20 mg/kg at the household level.” Later, in 2002, the Chinese government changed the salt iodination policy to lower the daily salt iodine intake concentration to 35 ± 15 mg/kg.
In 2011, this concentration was decreased further to 20–30 mg/kg, and provincial authorities were allowed to set the salt iodine concentration according to local conditions. The noniodized salt is available for customers in China. In recent years, people have also been choosing noniodized salt due to concerns about excess iodine intake and its adverse effects. The iodized salt coverage was reported to decrease to 88% previously in some regions in China (4,5). As a result of these changing trends, the current dilemma is how iodine excess can be avoided while simultaneously preventing the re-emergence of iodine deficiency (6).
To solve this dilemma, more epidemiological data are required to determine whether adjustment of intake concentrations at the national level and individual choice can lead to optimal iodine nutrition levels in the population and prevent diseases caused by iodine excess or deficiency. Therefore, this large-scale cross-sectional study tried to contribute to the available knowledge on this topic by evaluating the actual iodine nutrition status of Chinese residents and the associated factors. The study is part of the thyroid, iodine nutrition, and diabetes epidemiology (TIDE) investigation (5), and the study population includes Chinese residents from 31 provinces.
Materials and Methods
Study population
The research protocols were approved by the medical ethics committee of China Medical University (serial number: IRB[2008]115). The estimated sample size was 2651 in each province. All subjects provided their written informed consent after the research procedures were explained to them in detail. The staging and sampling strategy were the same as previously reported (7). The adult respondents included were 18 years or older, and had been living in the selected community for at least 5 years. The exclusion criteria were intake of iodine-containing drugs in the past 3 months, use of iodine-containing contrast agents for imaging in the past 3 months, and pregnancy.
Every participant was asked to fill in a questionnaire regarding lifestyle factors, including demographic characteristics, smoking habits, salt consumption, family income, and education level. There were two questions used for the assessment of salt consumption: (a) What is the type of your household salt? (i) iodized salt and (ii) noniodized salt. (b) Please estimate your daily amount of salt consumption. (i) >10 g/day, (ii) 5–10 g/day, and (iii) <5 g/day. Bodyweight and height were measured with the participants barefoot and wearing normal indoor clothes. All subjects were asked to provide a urine sample when they visited the center.
All participants underwent thyroid ultrasonography by qualified observers, who had trained and passed the examination in the project center, using a portable instrument (LOGIQ 100 PRO, GE, Milwaukee, WI, the United States with 7.5 MHz linear transducers). We conducted unified training for sonographers before the survey, and sonographers with kappa value >0.8 and agreement rate >90% could pass the test. Furthermore, after the survey, we randomly selected 100 respondents for consistency analysis, with kappa value of 0.8186 and agreement rate of 95%.
In addition, sixty 9–11 years old school children were sampled from each province for ultrasonography examination of the thyroid gland and fasting urine collection. Five milliliters of urine was transported using the cold chain system to the central laboratory in Shenyang, China, and stored at −20°C until analysis. Ten randomly selected participants in each province were asked to provide a sample of their household salt. The salt samples were transported to the central laboratory in Shenyang, China.
Laboratory tests
Urine iodine concentration (UIC) and salt iodine concentration were determined using inductively coupled plasma mass spectrometry (Agilent 7700x; Agilent Technologies). The measurement quality was controlled using certified reference material (GBW09108, GBW9109, and GBW9110) from the Center for Disease Control in China. The target values of the standards GBW09108, GBW9109, and GBW9110 were 70.8 ± 9.0, 143 ± 10, and 224 ± 14 μg/L, respectively; the interassay coefficients of variability (CV) values were 2.3%, 2.5%, and 2.4%, respectively; and the intra-assay CV values were 2.7%, 1.4%, and 2.3%, respectively.
Definitions
The MUI was used for the evaluation of iodine nutrition status. The cutoff points of MUI used for classifying iodine nutrition into different degrees referenced to the guidance of WHO, UNICEF, and ICCIDD (8): excessive iodine intake ≥300 μg/L, more than adequate intake 200–299 μg/L, adequate iodine intake 100–199 μg/L, mild iodine deficiency 50–99 μg/L, moderate iodine deficiency 20–49 μg/L, and severe iodine deficiency <20 μg/L.
The adequate iodine intake and more than adequate iodine intake categories have been combined under “sufficient iodine intake” by WHO. According to the recent guidance of UNICEF, the population UIC <100 μg/L should not be used to describe the prevalence of iodine deficiency because UIC varied highly from day to day. The goiter was defined as the thyroid volume >22.5 mL for women and >25.4 mL for men. The thyroid volume was calculated by the equation recommended by WHO: V = V left lobe (0.479 × length × width × thickness) + V right lobe (0.479 × length × width × thickness).
The cutoff value was established by our previous survey (9). It corresponded to the mean (+2 SD) in 478 healthy male subjects and 596 female subjects living in iodine sufficient areas without known thyroid disease, without a family history of thyroid disease, without antithyroid antibodies, without goiter, nodules, or an abnormal echo pattern on B-mode ultrasonography. The cutoff value for evaluating goiter in school-age children was >5.0 mL for 9 years, >6.0 mL for 10 years, and >7.0 mL for 11 years. The cutoff value for evaluating goiter in school-age children was recommended by the Diagnostic Criteria for Endemic Goiter of China (WS 276–2007).
Statistical analysis
The calculations of MUI and percentages of different iodine nutrition levels were adjusted to represent the Chinese adult population based on the weighted coefficients derived from the 2010 national census data of China and the sampling strategy of the current survey. The UIC was described by the median and interquartile range (IQR). The significance of differences between MUI values was assessed using nonparametric analysis. Categorical data presented as counts and percentages were analyzed with the chi-square test and Fisher's exact test, as appropriate.
Adjusted odds ratios (ORs) with confidence intervals (95% CIs) were calculated by multivariable logistic regression to examine the association of demographic factors, body mass index (BMI), smoking habits, and education and income levels with UIC categories and goiter prevalence. p < 0.05 was considered to indicate statistical significance. All statistical analyses were conducted using the SUDAAN software, version 10.0 (Research Triangle Institute), SPSS v.21 software, and Statistical Analysis System (SAS) version 9.3 (SAS Institute, Inc.).
Results
UIC and prevalence of iodine deficiency
Of the 78,470 respondents, 77,933 completed urinary iodine tests and met the quality control standards. The results showed that the MUI was 177.89 μg/L (IQR 117.89–263.90 μg/L) in the general population and 199.75 μg/L (IQR 128.41–303.37 μg/L) in school-age children. The data presented the iodine status was sufficient in China. The proportion of the iodine status categories in different sex and age groups is given in Table 1.
The Median Urine Iodine with Interquartile Range, Percentage of Different Iodine Category, Goiter Prevalence, and Iodized Salt Coverage of Chinese Population in Different Sex and Age Groups
Data are expressed as median (interquartile range) or percent. [95% CI]. p Values for comparison between participants and nonparticipants. Categorical data presented as counts and percentages were analyzed with the chi-square test and Fisher's exact test, as appropriate. Adjusted p < 0.05 was considered to indicate statistical significance.
CI, confidence interval; MUI, median urine iodine; UIC, urine iodine concentration.
Based on the MUI of school-age children in the 31 provinces surveyed for iodine nutrition, there were no iodine-deficient provinces: iodine intake was sufficient in 30 provinces, and iodine excess was observed in 1 province. Based on the MUI of adults, iodine intake was sufficient in 27 provinces and iodine excess was noted in 4 provinces. The proportion of UIC <50 μg/L was 3.43% in the whole population. In all the regions, the proportion of UIC <50 μg/L was <20%. The iodine nutritional levels of the provinces are given in Supplementary Table S2.
Effectiveness of USI
According to our survey, the iodized salt coverage was 95.37%, varying from 64.24% (Zhejiang province) to 99.96% (Jiangxi province) in different provinces. The iodized salt coverage and salt iodine concentration data are given in Supplementary Table S2. Among the 31 provinces surveyed, except for Shanghai, Tianjin, and Zhejiang, the rate of usage of iodized salt was >90%. The MUI of individuals who consume iodized salt was 179.99 μg/L (IQR 120.00–267.00 μg/L), and this was significantly higher than the MUI of 136.92 μg/L (IQR 87.60–204.93 μg/L) in individuals who consumed noniodized salt. The proportion of UIC <50 μg/L was 7.69% in noniodized salt users.
Prevalence of goiter
The overall goiter prevalence was 1.17% [95% CI 0.95–1.43] in adults and 3.50% [95% CI 2.93–4.13] in school-age children. The prevalence of goiter was not significantly different between users of iodized salt and users of noniodized salt. However, the people with UIC <100 μg/L had a higher prevalence of goiter (1.68%, [95% CI 1.35–2.1]) than the adequate iodine group (1.13%, [95% CI 0.87–1.46]). The goiter prevalence was also higher in females, elderly individuals (given in Table 1), individuals with a BMI of >24 kg/m2, those with a lower education level, and those with a lower income level (shown in Table 2). The multivariable regression results indicated the risk of goiter was higher in residents living in southern China (OR 1.54, [95% CI 1.06–2.24]) and nonsmokers (OR 1.46, [95% CI 1.16–1.82]).
The Median Urine Iodine with Interquartile Range, Percentage of Different Iodine Category, Goiter Prevalence, and Iodized Salt Coverage of Chinese Population Grouping by Potential Influential Factors
Data are expressed as median (interquartile range) or percent (95% CI). p Values for comparison between participants and nonparticipants. Categorical data presented as counts and percentages were analyzed with the chi-square test and Fisher's exact test, as appropriate. Adjusted p < 0.05 was considered to indicate statistical significance.
BMI, body mass index.
Other factors that influence iodine nutrition
The MUI level, iodine intake level, goiter prevalence, and iodized salt coverage of the subjects according to different influential factors are given in Tables 1 and 2, and the multivariable logistic regression analysis results are given in Table 3. The results indicated that iodized salt is the most critical factor affecting the MUI level.
Factors Influencing Iodine Levels and Goiter
Adjusted odds ratios with 95% CI were calculated by multivariable logistic regression, p < 0.05 was considered statistically significant. Three models with progressively increased adjustment of risk factors were applied. Model 1 was calculated by adjusting age and sex. Model 2 was calculated by adjusting age, sex, and whether to use iodized salt. Model 3 was calculated by adjusting all other potential risk factors including age, sex, ethnic, geographic factors, BMI, whether used iodized salt, smoking habit, education level, and family income level.
Sex and age had a consistent impact on iodine nutrition levels. As shown in Figure 1, MUI decreased with age in the overall study population, and the MUI level in men was slightly higher than that in women.
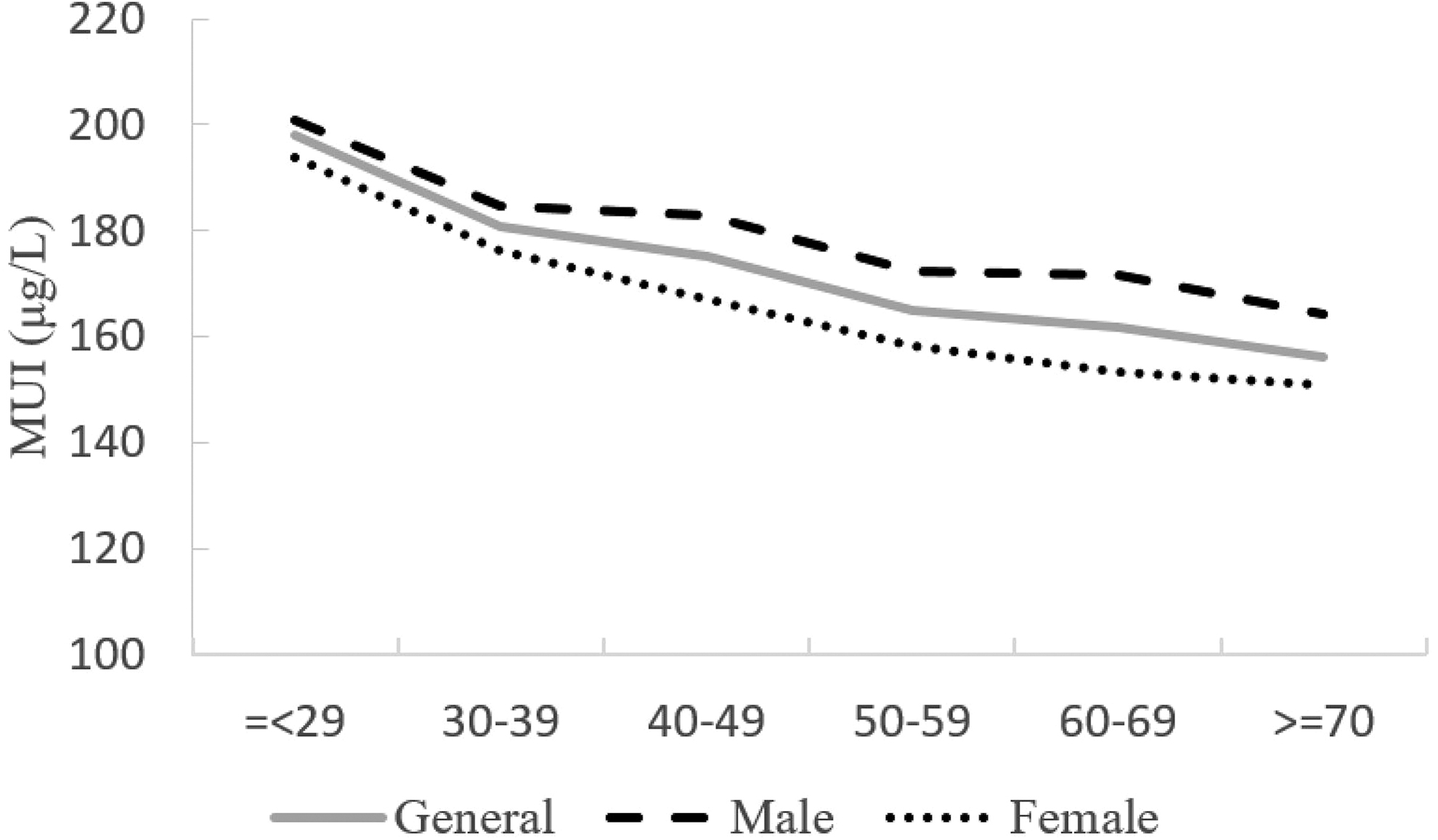
MUI by age in the general population. MUI, median urine iodine.
Inhabitants of coastal areas had a significantly lower MUI than those inhabiting inland areas (163.3 μg/L, IQR 105.97–248.29 μg/L vs. 189.00 μg/L, IQR 128.10–275.80 μg/L). After adjustment for other influential factors such as the use of iodized salt, multivariable logistic regression analysis still indicated that living in coastal areas increases the risk of iodine deficiency. We also compared the MUI level of people who consume noniodized salt in coastal areas and inland areas, and the results showed that people in coastal areas still have a lower MUI. This difference was also observed in iodized salt users (Supplementary Table S3).
Inhabitants of south areas had a slightly lower MUI (174.29 μg/L, IQR 116.09–255.89 μg/L) than those inhabiting north areas (179.70 μg/L, IQR 119.00–268.19 μg/L, p = 0.015). The inhabitants of areas with an altitude lower than 500 m had lower MUI (173.29 μg/L, IQR 114.37–259.06 μg/L) than those living in altitude 500–1500 m (191.48 μg/L, IQR 129.29–280.02 μg/L) and in altitude higher than 1500 m (195.93 μg/L, IQR 133.64–278.19 μg/L), p = 0.02. People living in urban and rural areas had similar MUI. However, the multivariable regression did not find these factors to affect the iodine nutrition levels.
BMI was found to be a two-way influential factor. As the BMI increased, the proportion of UIC <100 μg/L and UIC >300 μg/L decreased. Multivariable logistic regression analysis results adjusted for influential factors showed that lower BMI was a risk factor for both iodine deficiency and more than adequate iodine intake.
The data also demonstrated that the MUI level was lower in individuals who never smoked than in smokers after adjustment for sex and other influential factors. Comparison of groups based on education level and family income showed that the MUI was not significantly different in individuals with different education or income level.
Discussion
Our large-scale cross-sectional data on iodine nutrition status obtained from 31 provinces showed that the MUI of the general Chinese population was 177.89 μg/L, and the proportion of UIC <50 μg/L was 3.43% in the whole population. This meets the WHO criteria for elimination of iodine deficiency, that is, MUI >100 μg/L and urine iodine levels of <50 μg/L in <20% of the population. Our study did not include pregnant women. However, according to a recent study (10), the MUI of pregnant women across China was 146 μg/L, which was close to the cutoff value of 150 μg/L. Based on this evidence, we can conclude that the iodine nutrition status of Chinese people is generally within the safe range.
The high effectiveness of salt iodination and the surveillance system has made China one of the most successful countries in eliminating iodine deficiency. The USI program has been implemented since 1996, and the iodized salt coverage has been maintained at >90% since 1999. In this survey, the iodized salt coverage calculated based on self-reported data was 95.37% in the general population. The relatively high iodized salt coverage is the result of the Chinese government's efforts over the past two decades to ensure that the USI policy is implemented.
Remarkable progress toward eliminating iodine deficiency disorders has been made worldwide over the past two decades. According to the data reported by the iodine global network, the countries classified with iodine deficiency have decreased from 113 in 1990 to 21 in 2018 (11). Eighty-eight percent of households worldwide were consuming iodized salt. The iodized salt coverage was lowest, but still 76% in west and central Africa despite food shortage. And the coverage reached 92% in east Asia and the Pacific (12).
The iodine nutrition level had been excessive in China for several years. Iodine excess is a universal problem in the process of iodine fortification (13,14). In the 1970s, there were concerns about the safety of salt iodization in the United States, when the MUI was 320 ± 6 μg/L, as reported by NHANES I. Therefore, the use of iodine was reduced as a dough conditioner for bread and supplement in the dairy industry; this was followed by a decline in the MUI level to 145 ± 3 μg/L in 1988–1994 (NHANES III) (15). An increase in hypothyroidism incidence, serum thyrotropin, thyroid autoantibody, and goiter was observed after the excessive iodine fortification worldwide (16,17). Close population monitoring and adjustment of salt iodine concentration are necessary for the prevention of iodine excess.
Insufficient iodine fortification or low coverage of iodized salt is also one of the main concerns of countries that use iodized salt for iodine fortification (18,19). For example, the re-emergence of iodine deficiency has been documented in Britain and Australia (20 –23). Furthermore, although iodized salt was used in >80% of the households in Switzerland, reproductive-age women still had borderline iodine deficiency due to the low coverage of iodized salt in the processed food industry (18).
To shed light on the issue of ensuring optimal iodine levels, in this study, we analyzed the risk factors for iodine deficiency and iodine excess in the observed population. The results indicate that besides iodized salt, age and sex were the main influential factors for iodine status. In agreement with our findings, other studies have also demonstrated that women have lower urine iodine levels and are more vulnerable to iodine deficiency (24,25). However, the findings related to the relationship between age and iodine are not consistent.
In the NHANES survey of 2005–2006 and 2007–2008 (25), the distribution of MUI concentration according to age showed a U-shaped pattern. In our survey, UIC tended to decline as age increased. Our study included the largest population for urine iodine evaluation, as compared with other reported individual studies about iodine nutrition. Therefore, the steady relationship between age and iodine nutrition could be attributable to the large sample size.
In coastal areas of China, mild iodine deficiency appeared to re-emerge partially because of the tendency to use noniodized salt (26,27). In this study, too, we found that noniodized salt users in the coastal areas had lower MUI than inland noniodized salt users, and iodized salt users in coastal areas had lower MUI than inland iodized salt users. The same phenomenon has been reported by other researchers too (4).
The difference in the urine iodine level between coastal and inland subjects may be partially attributable to the tendency to use iodized salt. This is because coastal residents, who are believed to be iodine sufficient, tend to use noniodized salt and have a higher incidence of iodine deficiency. These results indicate that it is necessary to continue to implement the salt iodization policy to avoid iodine deficiency disorders in both coastal and inland areas.
Iodine deficiency remains a major threat to health, particularly in pregnant women. Furthermore, even in areas where the MUI was optimal in general, iodine deficiency was still a threat in a part of the population, especially vulnerable subjects such as pregnant or lactating women (28 –30). Thus, balancing the iodine requirements of pregnant or lactating women and school-aged children or other adults is an unsolved problem worldwide (31). Unfortunately, addressing the iodine nutrition requirements of specific population groups was beyond the scope of this study. This is an important topic that needs to be covered by future research though.
Our data also showed lower BMI was a risk factor for both iodine deficiency and more than adequate iodine intake, and the MUI level was lower in individuals who never smoked than in smokers. But iodine nutrition status was influenced by geographical, environmental, and other factors, the cross-sectional data cannot demonstrate whether the association is statistically false positive. Smoking was associated with higher thiocyanate intake, but the interaction between smoking and iodine nutrition was rarely reported. Cho et al. (32) and Bivolarska et al. (33) found a slight negative association between smoke and iodine intake. Further pieces of evidence are needed to verify the results and unveil the mechanisms involved in the observed phenomena. The conclusion should be drawn with caution.
There are several limitations to this article. First, the study is a cross-sectional investigation, so the data did not have enough power to demonstrate the causal relationship between the risk factors and iodine deficiency. Second, we excluded pregnant or lactating women in this study, but their iodine status needs special attention and has not been addressed. Last, as true for most research on this topic, iodine status, as an indicator, can only reflect the iodine status of the general population but not individuals. For example, the MUI of school-age children, which has been used for iodine nutrition classification for years, cannot represent the iodine status of the general population or other groups such as pregnant or lactating women. Therefore, an indicator of individual iodine status needs to be developed in the future.
In summary, the present findings indicate that the iodine nutrition status is satisfactory in the general population of China. The prevalence of goiter is maintained at a low level. Iodine deficiency still slightly increased the risk for goiter. Increased age, living in coastal areas, lower BMI, and nonsmoking were associated with iodine deficiency according to our data. Iodine supplementation and continuous iodine nutrition status monitoring are necessary.
Footnotes
Acknowledgments
We are grateful to all the participants who took part in this study. For continuous support, assistance, and cooperation, we thank Wei Gong, Chenling Fan, Hong Wang, Hongmei Zhang, Shuangning Ding, and Xiaochen Xie (The First Hospital of China Medical University); Caiping Li and Jian Huangfu (The Affiliated Hospital of Inner Mongolia University); Nan Jin (Chinese PLA General Hospital); Wuquan Deng and Fang Deng (Third Military Medical University); Haicheng Zhou (The First Affiliated Hospital of Dalian Medical University); Qingling Lu (Cardiovascular and Cerebrovascular Disease Hospital of Ningxia Medical University); Yunfeng Shen (The Second Affiliated Hospital of Nanchang University); Guodong Liu (The First Affiliated Hospital of Harbin Medical University); Junxiu Hou and Zhiqiang Zhang (The Affiliated Hospital of Inner Mongolia Medical University); Hong Zhang (The Second Xiangya Hospital); Xiaodong Mao, Qifeng Wang, and Kun Wang (Nanjing University of Chinese Medicine); Yanping Wang (Fujian Medical University Union Hospital); Xiaojun Ma (The First Affiliated Hospital of Zhengzhou University); Liheng Meng (First Affiliated Hospital of Guangxi Medical University); Weihua Linle and Tuanyu Fang (Hainan General Hospital); Xingjun Liu and Yanru Zhao (The First Affiliated Hospital of Xi'an Jiaotong University); Lulu Chen, Jiaoyue Zhang, and Hanyu Wang (Huazhong University of Science and Technology); Jingfang Liu and Songbo Fu (The First Hospital of Lanzhou University); Qingguo Lv (West China Hospital); Chenglin Sun (The First Hospital of Jilin University); Qiuming Yao and Ronghua Song (Shanghai University of Medicine & Health Science Affiliated Zhoupu Hosipital); Tingting Chen (The First Hospital of An Hui Medical University); Ben Niu (The First People's Hospital of Yunnan Province); Mingtong Xu and Feng Li (Sun Yat-sen Memorial Hospital); Lizhen Lan (The First Hospital of Shanxi Medical University); Jun Yue and Jia Song (People's Hospital of Tibet Autonomous Region); Yanan Li and Wei Luo (Qinghai Provincial People's Hospital); Xiaoming Lou and Zhe Mo (Zhejiang Provincial Center for Disease Control and Prevention); Nianchun Peng and Lixin Shi (Affiliated Hospital of Guiyang Medical University); Mian Wang, Qiuxiao Zhu, and Lingling Yuan (Second Hospital of Hebei Medical University); Haiqing Zhang (Shandong Provincial Hospital affiliated with Shandong University); Yong Fan (The First Affiliated Hospital of Xinjiang Medical University); and Hongyan Wei (Tianjin Medical University General Hospital).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Research Fund for Public Welfare from the National Health and Family Planning Commission of China (Grant No. 201402005).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3