
Abstract
Background:
Vitamin A is a factor that suppresses immune responses, including T helper (Th)1 and Th17 responses. However, there has been no report showing the association between vitamin A-related genes (CYP26B1, RARB, and RARG) and the prognosis of autoimmune thyroid disease (AITD). The objective of this study was to clarify the association between vitamin A-related genes and the susceptibility and prognosis of AITD.
Methods:
We genotyped polymorphisms in genes encoding vitamin A-related molecules using the polymerase chain reaction-restriction fragment length polymorphism method. The proportion of T helper cells was analyzed by flow cytometry. Serum interleukin (IL)-17 and interferon (IFN)-γ were examined by enzyme-linked immunosorbent assay.
Results:
CYP26B1 rs3768641 GG genotype and G allele were significantly more frequent in patients with mild Hashimoto's thyroiditis (HT) than in those with severe HT (p = 0.0013 and 0.0024, respectively). The RARB rs1997352 CC genotype was significantly more frequent in HT patients than in controls (p = 0.0207). The proportion of Th17 cells was significantly higher in CYP26B1 rs2241057 TT genotype than C carrier (CC+CT genotypes) (p = 0.0385), in RARB rs1997352 A carrier (AA+AC genotypes) than those with CC genotype (p = 0.0246), and in RARG rs7398676 G carrier (GG+GT genotypes) than in TT genotype (p = 0.0249). In the RARB rs1997352 polymorphism, HT patients with a high concentration of IFN-γ (≥150 ng/mL) were more frequent in the CC genotype than in A carriers (AA+AC genotypes) (p = 0.0226). Serum levels of IL-17 were significantly elevated in subjects with the TT genotype of the CYP26B1 rs2241057 single nucleotide polymorphism (SNP) (p = 0.0026) and in subjects with the GG genotype of the CYP26B1 rs3798641 SNP (p = 0.030). Subjects with a high concentration of IL-17 (≥0.71 pg/mL) were more frequent in RARG 7398676 G carriers (GG+GT genotypes) than in TT genotype (p = 0.0218).
Conclusions:
Polymorphisms in the CYP26B1 gene were related to the proportion of Th17 cells, the level of IL-17 and the severity of HT. Polymorphisms in RAR were related to the proportion of Th17 cells, concentrations of IFN-γ and IL-17, and susceptibility to HT.
Introduction
Autoimmune thyroid diseases (AITDs), such as Graves' disease (GD) and Hashimoto's thyroiditis (HT), are frequent and archetypal organ-specific autoimmune diseases (1,2), and their severity or intractability can vary among patients. GD is the most common cause of hyperthyroidism and is characterized by the presence of anti-thyrotropin receptor antibody (TRAb).
Some GD patients achieve remission through medical treatment, but others do not (3,4). In contrast, HT is the most common cause of hypothyroidism, which is characterized by the presence of anti-thyroglobulin antibody (TgAb) and/or anti-thyroid peroxidase antibody (TPOAb) and by the destruction of thyroid tissue by infiltrated lymphocytes. Some HT patients develop hypothyroidism at a young age, while some remain in a euthyroid state even in old age. Although it is difficult to predict the prognosis of AITD, we have previously reported on several factors associated with the prognosis of AITD (5 –9).
We found that an increase in T helper (Th) 17 cells was associated with the pathogenesis and intractability of GD and that an increase in Th1 cells and the ratio of Th1/Th2 cells were related to the severity of HT (10). Furthermore, polymorphisms in genes coding immunoregulatory factors such as interferon (IFN)-γ, interleukin (IL)-4, and IL-17, and transforming growth factor-β (TGF-β) were also associated with the prognosis of AITD (8,9,11,12). These results indicate that the genetic differences in the balance of Th1/2/17 cell subsets and the production of Th1/Th2/Th17 cytokines are related to AITD (6,10).
Vitamin A is known to suppress immune responses (10,13 –18). Vitamin A taken from meals is metabolized to all trans retinoic acid (ATRA), and ATRA binds to nuclear receptors to suppress the differentiation of Th1 and Th17 cells by regulating transcription (18). This suggests the possibility that the vitamin A metabolism pathway may play a role in susceptibility to AITD.
In addition, CYP26B1 catalyzes the metabolism of ATRA to 4-oxo retinoic acid and affects the concentration of ATRA (19). This suggests, therefore, that CYP26B1 may indirectly affect the differentiation of Th1 and Th17 cells. Interestingly, some single nucleotide polymorphisms (SNPs) in the CYP26B1 gene, which are related to enzyme activity, have been associated with susceptibility to cancer, atherosclerosis, and inflammatory bowel disease (19,20) and with intracellular ATRA concentrations (19). To clarify the genetic associations of CYP26B1 with the pathogenesis of AITD, we focused on two SNPs in the CYP26B1 gene. One is the rs2241057 T/C polymorphism, resulting in Leu (T allele)-to-Ser (C allele) (21), and the C allele of this SNP is associated with a lower concentration of intracellular ATRA (19). In addition, arteriosclerosis patients with the C allele is associated with inflammation (19). In contrast, the T allele is associated with a declining age at the onset of Crohn's disease (20). The second SNP is the rs3768641 G/C polymorphism, which may be involved in enzyme activity, and the C allele of this SNP is related to a high incidence of chronic myelogenous leukemia (22).
Retinoic acid receptor (RAR) is a molecule with three kinds of subunits, α, β, and γ, and is involved in the intracellular effects of vitamin A (23,24). The RARB rs1997352 C allele and RARG rs7398676 G allele have been reported to influence the high production of IFN-γ (23), which was associated with the severity of HT (8).
In this study, we genotyped these four polymorphisms in vitamin A-related genes (CYP26B1, RARB, and RARG) and examined the proportions of Th cell subsets and the levels of IFN-γ and IL-17 in peripheral blood to clarify the association between these genes and the pathogenesis of AITDs.
Materials and Methods
Subjects
We examined each polymorphism in 253 GD patients, 312 HT patients, and 197 healthy volunteers (control subjects) (144 females and 53 males; the age at the sampling were 36.0 ± 14.1 years). All patients with GD had a clinical history of thyrotoxicosis and were positive for TRAb at diagnosis. All patients with HT were positive for anti-thyroid microsomal antibody (McAb) and/or anti-TgAb and showed hypothyroidism or euthyroidism with palpable diffuse goiters. Intractable GD patients and severe HT patients were treated with anti-thyroid drugs and thyroxine, respectively, to normalize thyroid function. Healthy volunteers were negative for thyroid autoantibodies.
Among GD patients, we genotyped 118 patients (96 females and 22 males; the age of onset were 34.0 ± 13.7) who had been treated with methimazole for at least 5 years and were still positive for TRAb (intractable GD), 58 patients (51 females and 7 males; the age of onset were 33.6 ± 14.6 years) who had maintained a euthyroid state and were negative for TRAb for more than 2 years without medication (GD in remission). Among HT patients, we genotyped 117 patients (96 females and 21 males; the age of onset were 38.8 ± 10.5) who developed moderate to severe hypothyroidism before 50 years of age and were treated with thyroxine (severe HT) and 86 untreated euthyroid patients with HT (70 females and 16 males; the age at the sampling were 58.9 ± 12.1) who were more than 50 years of age (mild HT). We could not categorize 77 GD patients into intractable GD or GD in remission groups and could not categorize 109 HT patients into severe HT or mild HT groups at the time of analysis. Genomic DNA was isolated from ethylenediamine tetraacetic acid-treated whole blood cells with a commercially available kit (QIAamp DNA Blood Mini Kit; Qiagen, Tokyo, Japan). Written informed consent was obtained from all patients and controls, and the study protocol was approved by the Ethics Committee of Osaka University (No. 564).
Genotyping of the polymorphisms
We used the restriction fragment length polymorphism (RFLP) method for genotyping all SNPs. Target sequences of each gene were amplified using polymerase chain reaction (PCR), and the PCR product was digested by the addition of restriction enzymes. The sequences of forward and reverse primers, the PCR conditions, and restriction enzymes used for genotyping are summarized in Table 1. DNA fragments were visualized by UV transillumination after electrophoretic separation on an 8% polyacrylamide gel.
Primers, Polymerase Chain Reaction Conditions, and Restriction Enzymes Used in This Study
PCR, polymerase chain reaction.
The proportion of peripheral blood T cells
We compared the proportion of peripheral Th cells with each genotype. The proportions of peripheral blood Th1, Th2, and Th17 cells were examined using flow cytometry. Peripheral blood mononuclear cells (PBMCs) were isolated from heparin-treated peripheral blood. In brief, peripheral blood obtained between 9:00 A.M. and 12:00 noon was isolated by density gradient centrifugation with Lymphoprep (density 1.077; Nycomed Pharma As, Oslo, Norway) at 400g for 30 minutes at room temperature and washed in phosphate-buffered saline (PBS). Separated PBMCs were resuspended at 5 × 105 to 1 × 106/mL in RPMI containing 10% fetal calf serum (FCS). PBMCs were cultured in RPMI containing 10% FCS for 4 hours at 37°C in a humidified atmosphere containing 5% CO2, with 10 mg/mL brefeldin-A (Sigma, St. Louis, MO, USA) plus 25 ng/mL phorbol myristate acetate (Sigma) and 1 μg/mL ionomycin (Sigma). After incubation, the suspended cells were washed twice in cold PBS and resuspended in cold PBS. According to the supplier's protocol, aliquots (100 mL) of PBMCs were incubated with 0.125 μg of Phycoerythrin-Cy5.5 (PE-Cy5.5)-anti-human CD4 antibody (eBioscience, San Diego, CA, USA) for 15 minutes at 4°C. Cells were then fixed with fixation reagent (Fixation Buffer; eBioscience). After incubation for 20 minutes at room temperature in the dark, cells were rinsed twice in 1 mL of appropriate concentration reagent to cross membranes (Permeabilization Buffer; eBioscience). Aliquots (100 mL) of suspended cells in permeabilization buffer were incubated for 20 minutes at room temperature in the dark with 0.125 μg of FITC-anti-human IL-17A antibody, 0.125 μg of PE-anti-human IFN-γ, and 0.05 μg of APC-anti-human IL-4 antibody. After rinsing in 1 mL of permeabilization buffer, PBMCs were resuspended in 500 μL of PBS and analyzed with a FACS-Calibur flow cytometer (Becton Dickinson, San Jose, CA, USA). To distinguish specialized Th (ThSP) cells producing a single cytokine from nonspecialized Th cells producing multiple cytokines, we defined Th1SP, Th2SP, and Th17SP as CD4+IFN-γ+IL-4−IL-17A− cells, CD4+IFN-γ-IL-4+IL-17A− cells, and CD4+IFN-γ−IL-4−IL-17A+ cells, respectively, after gating a lymphocyte area in dot-plot of linear forward light scatter versus linear side-angle light scatter. The Th1SP/Th2SP ratio was calculated as the ratio of the proportion of Th1SP cells in CD4+Th cells to that of Th2SP cells in CD4+Th cells.
Serum concentrations of IFN-γ and IL-17
Serum IFN-γ was measured with enzyme-linked immunosorbent assay (ELISA) kit (TAKARA BIO, INC., Tokyo, Japan), and IL-17 levels were measured with an ELISA Human IL-17 kit (Abcam® PLC). Serum samples were collected from 49 GD, 51 HT, and 22 healthy volunteers. All subjects were euthyroid and had no infectious diseases or history of other autoimmune diseases.
Thyroid function and autoantibodies
The serum concentrations of free T4 (fT4), free T3 (fT3), and thyrotropin (TSH) were measured by electro chemiluminescence immunoassay (ECLIA) (Roche Diagnostics Ltd., Tokyo, Japan). The normal ranges of serum fT4, fT3, and TSH are 0.9–1.7 ng/dL, 2.3–4.3 pg/mL, and 0.5–5.0 μIU/mL, respectively. TgAb and McAb were measured using a particle agglutination kit (Fujirebio, Inc., Tokyo, Japan). A reciprocal titer >1:100 was considered positive. Serum TRAb at onset was measured by the radioreceptor assay using a commercial kit (Cosmic Corporation, Tokyo, Japan). Serum TRAb at sampling was determined by ECLIA (third generation) (Roche Diagnostics Ltd., Tokyo, Japan). The normal value of TRAb was less than 10% in the radioreceptor assay and 2.0 IU/L in ECLIA.
Statistical analysis
We used the chi-square test to evaluate the significance of differences in the frequencies of genotypes and alleles among the groups. Fisher's exact test and Student's t-test were used to evaluate the significance of differences in the Th cell proportion, and serum IFN-γ and IL-17 levels and age of onset, respectively. In addition, the Wilcoxon test and Welch's test were also used to determine serum IFN-γ and IL-17 levels. Data were analyzed with JMP13 software (SAS Institute, Inc., Tokyo, Japan). p-Values of less than 0.05 were considered significant.
Results
Clinical characteristics of the patients genotyped in this study
Among the groups of intractable GD patients, GD patients in remission, severe HT patients, and mild HT patients, there were similar sex distribution, and serum fT4, fT3, and TSH levels were not significantly different. Serum TgAb and TPOAb levels were not significantly different among GD patient groups and among HT patient groups. The goiter sizes (transverse width) were larger in patients with intractable GD (4.8 ± 1.4 cm) than in GD in remission (4.2 ± 0.6 cm; p = 0.0022) and in patients with mild HT (4.5 ± 1.3 cm) than in severe HT (4.1 ± 1.0 cm; p = 0.0471).
CYP26B1 rs3768641 G/C polymorphism
There was no significant difference in the frequencies of genotypes and alleles between AITD patients and normal subjects (Table 2). However, the GG genotype and G allele were significantly more frequent in patients with mild HT than in those with severe HT (p = 0.0013 and 0.0024, respectively) (Table 3).
Genotype and Allele Frequencies of Polymorphisms in Patients with Autoimmune Thyroid Disease and in Control Subjects
Analyzed by chi-square tests, aversus control.
AITD, autoimmune thyroid disease; GD, Graves' disease; HT, Hashimoto's thyroiditis; NS, not significant.
Genotype and Allele Frequencies of Polymorphisms in Patients with Graves' Disease, Hashimoto's Thyroiditis
Analyzed by chi-square tests.
Intractable GD versus GD in remission.
Severe HT versus mild HT.
NS, not significant.
RARB rs1997352 C/A polymorphism
The CC genotype and C allele were significantly more frequent in HT patients than in controls (p = 0.0207 and 0.0133, respectively) (Table 2). However, we found no difference in these frequencies between the patients with intractable GD and those with GD in remission or between patients with severe HT and those with mild HT (Table 3).
CYP26B1 rs2241057 T/C and RARG rs7398676 G/T polymorphisms
There was no significant difference in the frequencies of genotypes and alleles between AITD patients and normal subjects (Table 2). We also found no difference in these frequencies between the patients with intractable GD and those with GD in remission and between patients with severe HT and those with mild HT (Table 3).
Clinical characteristics of the subjects measured for flow cytometry
Serum fT4, fT3, TSH levels, and age were not significantly different between the CYP26B1 rs2241057 C carrier (CC + CT genotype) and the TT genotype subject groups, between the CYP26B1 rs3798641 C carrier (CC + CG genotype) and the GG genotype groups, between the RARB rs1997352 A carrier (AA + AC genotype) and the CC genotype groups, and between the RARG rs7398676 G carrier (GG + GT genotype), and the TT genotype groups.
The proportion of peripheral blood T lymphocyte subsets
The proportion of Th17 cells was significantly higher in individuals with the CYP26B1 rs2241057 TT genotype than in C carriers (CC+CT genotypes) (p = 0.0385) (Fig. 1a). The proportion of Th17 cells was also significantly higher in AITD patients with the RARB rs1997352 A carriers (AA+AC genotypes) than in those with the CC genotype (p = 0.0246) (Fig. 1b). In the case of the RARG rs7398676 polymorphism, the proportion of Th17 cells was significantly higher in G carriers (GG+GT genotypes) than in TT genotype (p = 0.0249) (Fig. 1c).
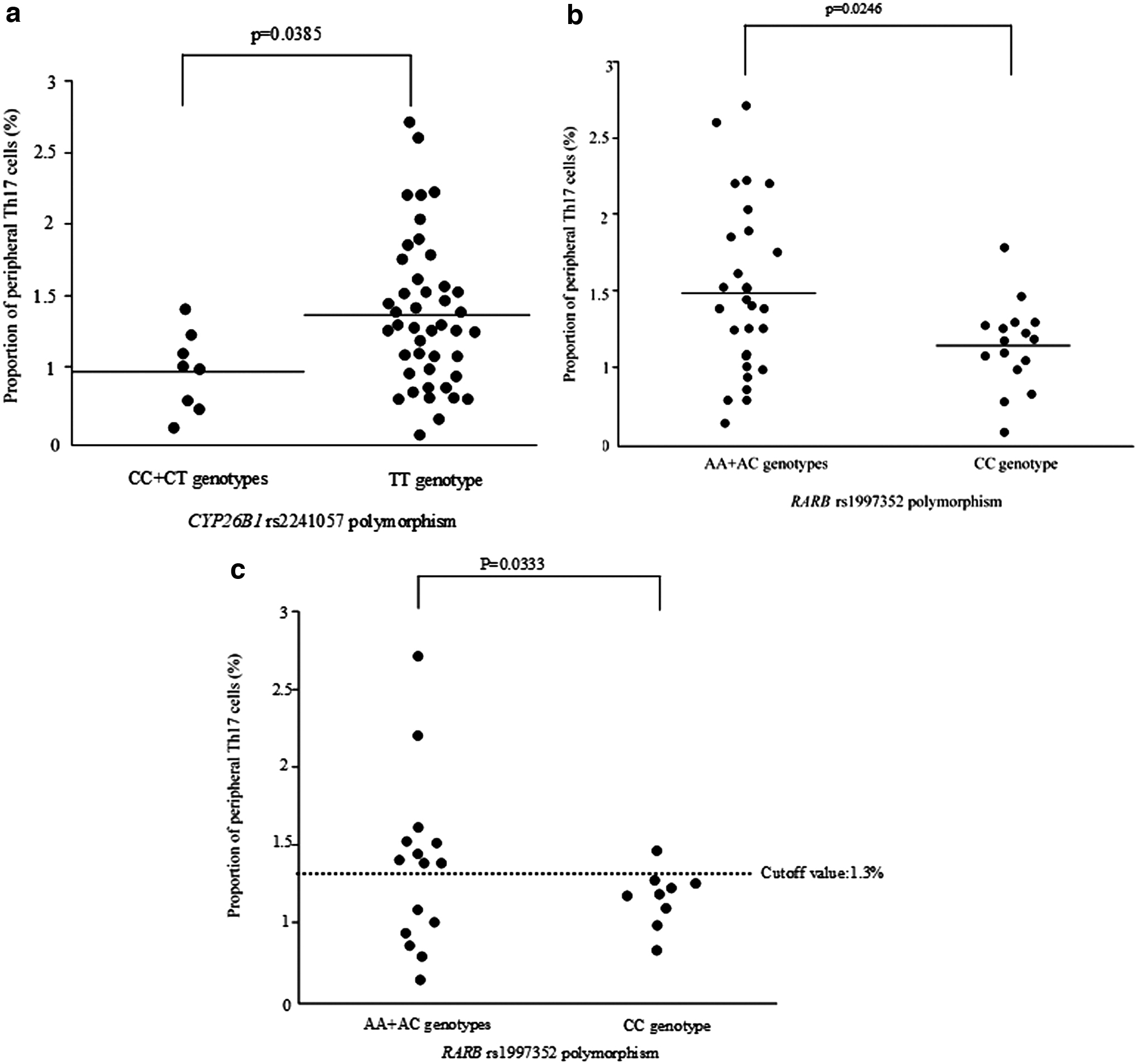
Proportion of Th cell subsets in peripheral blood compared among each genotype of (
The serum IFN-γ and IL-17 levels
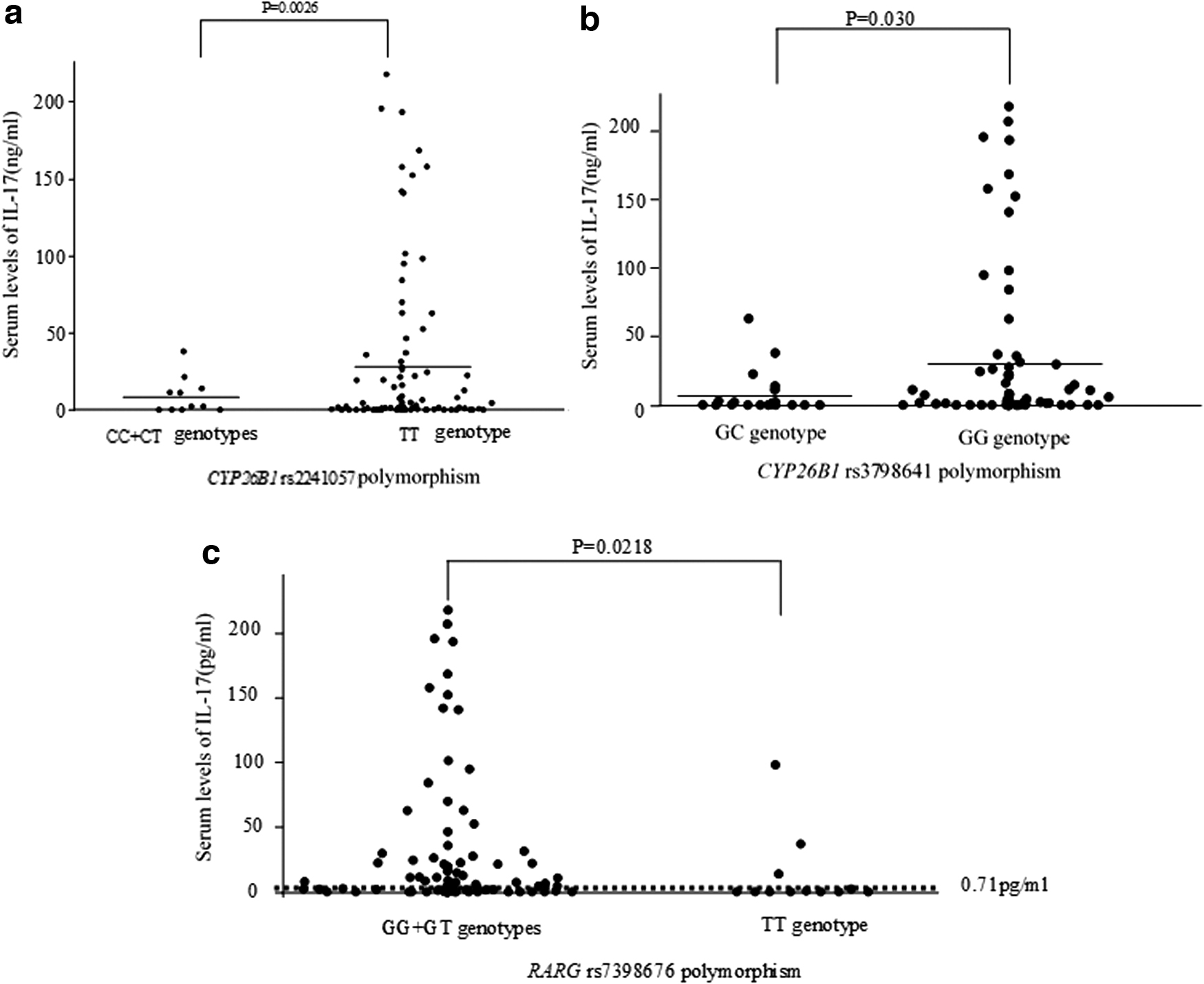
HT patients showing a high level of IFN-γ (≥150 ng/mL) were more frequent in the CC genotype than in A carriers (AA+AC genotypes) of the RARB rs1997352 polymorphism (p = 0.0226) (Fig. 2). Serum levels of IL-17 were significantly higher in subjects with the TT genotype of the CYP26B1 rs2241057 polymorphism (p = 0.0026) (Fig. 3a) and in subjects with the GG genotype of the CYP26B1 rs3798641 polymorphism (p = 0.030) compared with other genotypes in each polymorphism (Fig. 3b). Subjects showing a high proportion of IL-17 (≥0.71 pg/mL) were more frequent in RARG rs7398676 G carriers (GG+GT genotypes) than in TT genotype (p = 0.0218) (Fig. 3c).

Serum IFN-γ level in each genotype of RARB rs1997352 polymorphism in HT patients. Analyzed by Fisher's exact test. HT, Hashimoto's thyroiditis; IFN, interferon.
Peripheral IL-17 level in peripheral blood compared among each genotype of (
Discussion
The results in this study are summarized in Table 4. Specific SNPs in CYP26B1 rs2241057 C were related to decreases in peripheral Th17 cells and serum IL-17 levels (Figs. 1a and 3a). Since this polymorphism is located in the exon and changes the amino acid from Leu (T allele)-to-Ser (C allele) (21), we hypothesized that the structure and function of CYP26B1 can be altered to change the concentration of ATRA. Supporting this, it has been reported that ATRA is rapidly degraded in individuals with the C allele of this polymorphism (19). Although ATRA has been reported to suppress inflammation (13,15,16,19), we found that both the proportion of Th17 cells and the level of IL-17 were decreased in patients who were C carriers (Figs. 1a and 3a). Surprisingly, ATRA induces the generation of Th17 cells in mice by an unclarified mechanism (25 –27). The development of Th17 cells may become weak in individuals with the C allele of this polymorphism.
Summary of the Results in This Study
IFN, interferon; IL, interleukin; NA, no association; Th, T helper.
CYP26B1 rs3768641 C carrier was also related to lower levels of serum IL-17 (Fig. 3B) and was significantly more frequent in patients with severe HT than in those with mild HT (Table 3). We have already found that the severity of HT was related to the increase in Th1 cells and the ratio of Th1/Th2 cells (10). Therefore, we speculate that the levels of ATRA may also be low in individuals with CYP26B1 rs376841 C carriers as in rs2241057 C carriers. However, we could not find any differences in the frequencies of rs2241057 C carriers between severe and mild HT patients. The frequency of the C allele in control subjects was 5.92% for rs2241057 and 11.21% for rs3768641. Therefore, the effect of the rs2241057 polymorphism may be smaller than that of the rs3768641 polymorphism.
In contrast, the RARB rs1997352 CC genotype was significantly more frequent in patients with HT (Table 2). HT patients with a higher level of IFN-γ (≥150 ng/mL) were more frequent in the CC genotype than in A carriers (AA+AC genotypes) of the RARB rs1997352 polymorphism (Fig. 2). This is compatible with a previous report that the C allele of this polymorphism was associated with high IFN-γ production (23). The C allele may be associated with thyroid destruction in HT through an increase in the proportion of Th1 cells and IFN-γ production.
The RARG rs7398676 polymorphism was not related to AITDs in this study (Tables 2 and 3), but the proportion of Th17 cells and the serum concentration of IL-17 were significantly lower in individuals with the TT genotype than in those with the G carrier of this polymorphism (Figs. 1c and 3c). However, there was no difference in the serum IFN-γ levels (data not shown). This may be because the effect of the RARB rs1997352 polymorphism on IFN-γ production was weaker than that of the RARG rs7398676 polymorphism (23).
In conclusion, polymorphisms in the CYP26B1 gene were associated with the proportion of Th17 cells, the level of IL-17, and the severity of HT. Polymorphisms in RAR were associated with the proportion of Th17 cells, IFN-γ and IL-17 levels, and susceptibility to HT.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by JSPS KAKENHI under grant numbers A19H040480 (to M.W.), JP17H04111 (to Y.I.), and JP17K15774 (to N.I.).