
Abstract
Background:
Observational studies suggest an association between thyroid function and risk of dementia, but the causality and direction of these effects are unclear. We aim to test whether genetically predicted variation within the normal range of thyroid function and hypothyroidism is causally associated with the risk of Alzheimer's disease (AD).
Methods:
Mendelian randomization (MR) analyses using genetic instruments are associated with normal range thyrotropin (TSH) and free thyroxine (fT4) levels. Secondary analyses included investigation of the role of hypothyroidism. Bidirectional MR was conducted to address the presence of a potential reverse causal association. Summary statistics were obtained from the ThyroidOmics Consortium involving up to 119,715 individuals and the latest AD genome-wide association study data including up to 71,880 cases.
Results:
MR analyses show an association between increased genetically predicted normal range TSH levels and a decreased risk of AD (p = 0.02). One standard deviation increased normal range TSH levels were associated with a decreased risk of AD in individuals younger than 50 years old (p = 0.04). There was no evidence for a causal association between fT4 (p = 0.54) and AD. We did not identify any effect of the genetically predicted full range TSH levels (p = 0.06) or hypothyroidism (p = 0.23) with AD. Bidirectional MR did not show any effect of genetic predisposition to AD on TSH or fT4 levels.
Conclusions:
This MR study shows that increased levels of genetically predicted TSH within the normal range and in younger individuals are associated with a decreased risk of AD. We observed a marginal association between genetically predicted full range TSH and AD risk. There was no evidence for an effect between genetically predicted fT4 or hypothyroidism on AD. Future studies should clarify the underlying pathophysiological mechanisms.
Introduction
Dementia is an umbrella term comprising several neurodegenerative brain disorders that are characterized by the deterioration of cognitive functions including memory, planning, language, recognizing, and reasoning. Alzheimer's disease (AD), frontotemporal dementia, Lewy body dementia, and vascular dementia are four of the most common dementias (1). AD is the most common form of dementia, which is the fifth leading cause of death. AD can hinder the ability of an individual to perform everyday tasks along with several aspects of daily life. Despite decades of research, only a few causal risk factors have been identified, which are mostly nonmodifiable.
Thyroid hormone is important for brain development. However, also in the mature brain, thyroid hormone plays a key role in neurogenesis, myelinization, and cellular repair (2). Thyroid hormone is furthermore important to maintain essential brain functions including neurotransmission and memory (3). For a long time, epidemiological studies have identified associations between hypo- and hyperthyroidism and dementia risk (4). More recently, not only subclinical thyroid dysfunction, but even variation in thyroid function within the normal range has been associated with the risk of AD.
To examine the relationship between free thyroxine (fT4) and thyrotropin (TSH) with dementia, a meta-analysis was carried out that included a total of 11 studies published between 2003 and 2016: 3 case–control studies and 8 cohort studies. The meta-analysis findings showed that higher levels of fT4 were associated with an increased dementia risk. In line with this, lower TSH levels were associated with an increased dementia risk, which was confined to TSH levels below the normal range, rather than levels within the normal range (4). Conversely, the Rotterdam study (5) found that higher TSH levels are associated with a lower risk of developing dementia, both within the full and normal ranges of thyroid function.
This same study also found that high fT4 is associated with an increased dementia risk. In addition, the Framingham study examined the relationship between thyroid function and AD and found that both high and low TSH levels within the normal range were associated with a more than twofold greater AD risk in women but found no association between TSH and AD in men (6). Another study by van Osch et al. (4) also found that lower TSH levels within the reference range were associated with an increased AD risk; however, in contrast to the Framingham study, these results were independent of sex. Gan et al. report that with older age, the feedback between TSH and fT4 attenuates (7). Thus, decreased TSH is associated with decreased fT4, which is associated with cognitive decline.
Recent literature investigated the role of normal range thyroid function in men and women and the effect on AD (8). As large-scale meta-analyses of genome-wide association studies (GWASs) on thyroid function have significantly increased the number of genetic variants associated with normal-range TSH and fT4 levels, therefore, it is now the optimal moment to perform a well-powered Mendelian randomization (MR) study to evaluate the (causal) associations between thyroid function and AD. In this study, we interrogate the role of thyroid function within the normal range on AD, and we further explore the effect of full range TSH levels on AD. We perform additional analysis focusing on individuals <50 years old and we also explore the effect of hypothyroidism on AD risk.
Materials and Methods
MR is an observational epidemiological method that uses genetic data, normally in the form of single nucleotide polymorphisms, to investigate causal relationships between health outcomes and associated risk factors (9).
One benefit of using MR is its ability to overcome reverse causality and confounding, which is when a factor affects both the health outcome and associated risk factor, potentially leading to biased results (10). Mendel's laws of inheritance state that alleles segregate randomly into gametes; the genetic variants used for MR analysis are assorted during the formation of gametes, therefore, are not confounded by lifestyle choices or environmental factors (10).
Main analyses examined the presence of any causal association between variation in normal range thyroid function evaluated by TSH and fT4 levels and the risk of AD.
Secondary analyses examined whether genetic predisposition to hypothyroidism is causally associated with the risk of developing AD. Sensitivity analyses evaluated the role of thyroid function with estimates derived from GWAS in individuals with TSH within the normal range, aged <50 years old or the full range of TSH. Analyses used summary statistics data.
Genetic variants used as instruments
We used 86 and 29 genetic variants, respectively, that were previously found to be associated at a genome-wide significant level (p < 5 × 10−8) with TSH (11) and fT4 (12). We also evaluated the effect of 93 genetic variants associated with hypothyroidism (13). For TSH we also used estimates from the GWAS meta-analysis in the HUNT study for full range TSH levels, TSH within the normal range, and using data only from individuals <50 years old (11).
Summary statistics and study population
The data sets on thyroid function were derived from the ThyroidOmics Consortium (12) and (11), which carried out the largest meta-analysis on thyroid function. Secondary analyses for TSH were performed using estimates from GWAS data for full range TSH levels (HUNT + MGI + ThyroidOmics meta-analysis), TSH only within the normal range (HUNT study), and TSH levels in individuals younger than 50 years old (HUNT study) (11).
The summary statistics for AD were obtained from the GWAS catalog involving a meta-analysis including 71,880 cases and 383,378 controls (14) (Supplementary Tables S1 and S2). AD GWAS data included 455,258 individuals of European ancestry involving 24,087 clinically diagnosed late-onset AD cases and 47,793 AD-by-proxy phenotype cases. Median age of onset was 74.1 years, 59.1% were females (across cohorts). AD-by-proxy, based on parental diagnoses, showed strong genetic correlation with AD (rg = 0.81). Further details for the AD phenotypes used for the generation of the summary statistics used for our MR analyses are described in Jansen et al. (14).
Two-sample MR
Two-sample MR was performed using the genetic data that were extracted from the GWAS summary statistics. We employed the TwoSampleMR package in R (15). We used the inverse variance weighted (IVW) estimator (random effects), which assumes that there is no pleiotropy and is the most optimal as it maximizes the likelihood function and achieves minimal variance (16). For variants that are not in linkage disequilibrium (LD), the IVW estimate can be obtained from an IVW meta-analysis of the individual variants' ratio estimates (17).
Sensitivity analyses included MR-Egger (18), weighted median (WM) (19), and MR Pleiotropy RESidual Sum and Outlier (MR-PRESSO) (20). The MR-Egger method is a robust statistical technique that allows all the variants to have pleiotropic effect on the condition that these effects are not proportional to the effect that the variant has on the risk factor of interest; this is known as the instrument strength independent of direct effect assumption (18). This approach provides less precise estimates than the IVW and WM methods, thus lowering the power for testing causal hypotheses (9).
However, it still gives consistent causal effect estimates regardless of the possibility that all the genetic variants may be invalid instrumental variables. During this investigation, a pleiotropy test was carried out, to evaluate the Egger intercept. This is an indicator to evaluate directional horizontal pleiotropy (15). The MR-PRESSO approach was also used to evaluate the role of pleiotropy. When testing the causal null hypothesis, biased causal estimates and increased type I error rates are often the outcome of having the presence of pleiotropic variants in the MR study (21).
The first test carried out was the “MR-PRESSO global test” that evaluates the overall horizontal pleiotropy. The test compares the observed distance of the variants to the regression line with the expected distance (20). The second test carried out was the “MR-PRESSO outlier test” that identifies variants that could be leading to horizontal pleiotropy and are subsequently removed. This test used the observed and expected distributions of the tested variant to identify the outlier variants. The third test carried out was the “MR-PRESSO distortion test” that tested for significant differences in the causal estimates pre- and postremoval of the horizontal pleiotropic variants (20).
Bidirectional MR
Bidirectional MR was carried out to examine the potential of a reverse causation (22). This approach investigated whether genetic predisposition to AD could have a causal effect on thyroid function. The MR-PRESSO method was also used to test for horizontal pleiotropy. We performed LD pruning (r 2 = 0.001) for the genome-wide AD associated variants used as instruments (14) (Supplementary Tables S3 and S4).
Results
Normal range TSH and fT4 levels
MR analyses suggest that increased levels of genetically predicted TSH within the normal range are associated with a decreased risk of AD (odds ratio = 0.98 [95% confidence interval 0.97–0.99], p = 0.01, IVW, per 1 standard deviation increase in TSH levels). In the MR PRESSO analysis, the global test returned a significant p-value indicating the presence of overall horizontal pleiotropy. Next, we identified these pleiotropic variants using the outlier test. The MR estimate remained significant (p = 0.008) after removal of these horizontal pleiotropic outliers (Fig. 1).
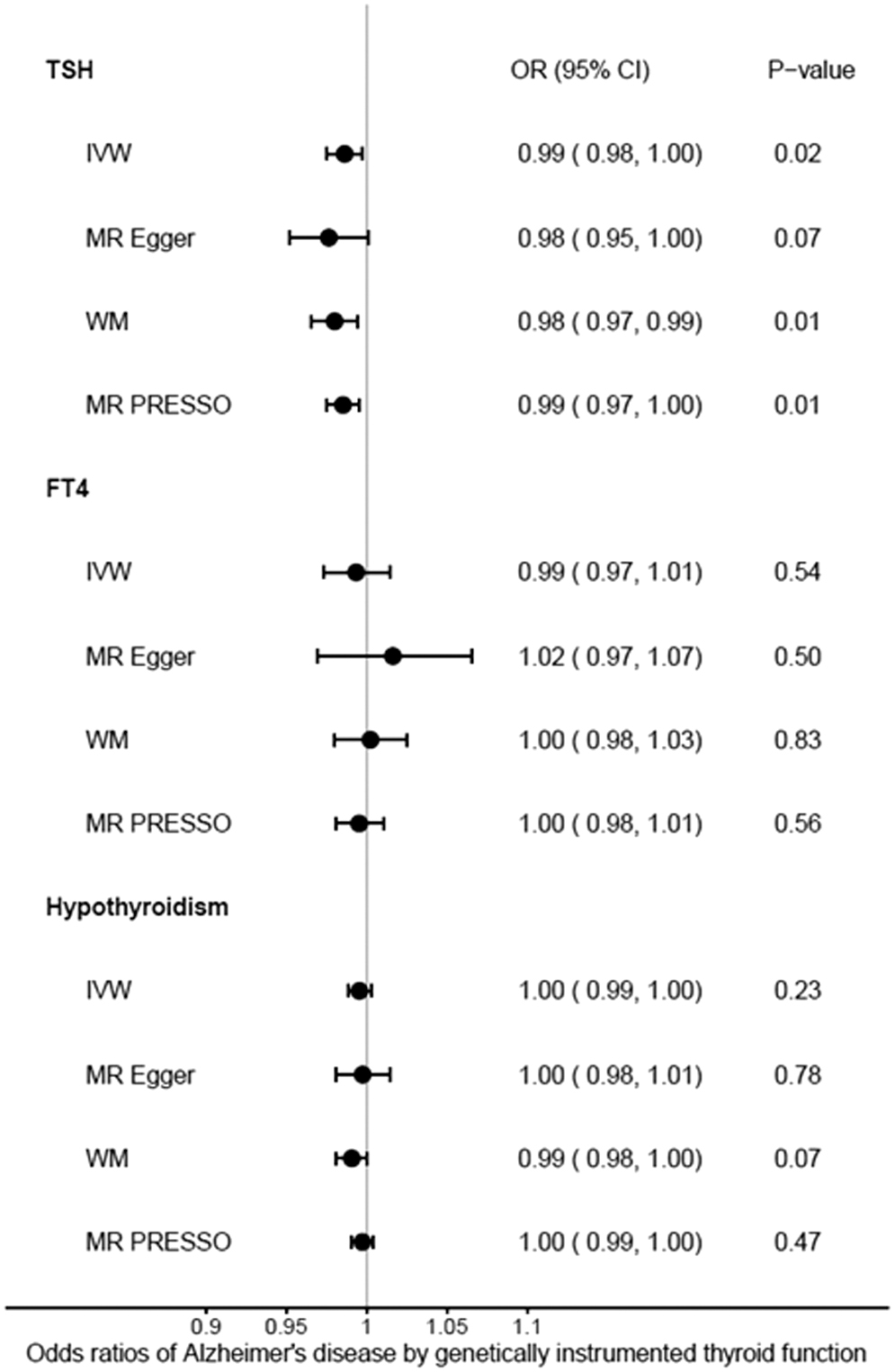
Forest plot: ORs for the effect of genetically determined TSH, fT4, and hypothyroidism on AD risk. ORs refer to 1 SD increase in genetically predicted levels of the exposure. AD, Alzheimer's disease; CI, confidence interval; fT4, free thyroxine; IVW, inverse variance weighted; MR, Mendelian randomization; MR-PRESSO, MR Pleiotropy RESidual Sum and Outlier; OR, odds ratio; SD, standard deviation; TSH, thyrotropin; WM, weighted median.
There was no evidence for causal association between normal range fT4 levels and the risk of developing AD (p = 0.54, MR-PRESSO). The global test returned a significant p-value indicating that overall horizontal pleiotropy was present; the outlier test identified the pleiotropic variants and subsequently removed them. However, after correcting the horizontal pleiotropic outliers, the MR estimate remained null (p = 0.56) (Fig. 1; Supplementary Table S5).
Secondary analyses
Secondary analyses using estimates from GWAS data for full range TSH levels (HUNT + MGI + ThyroidOmics), within the normal range (HUNT study) and TSH levels for individuals younger than 50 years old (HUNT study), revealed nominally significant associations with AD. More specifically, full range TSH: p = 0.06, TSH within normal range: p = 0.04, and participants younger than 50 years old: p = 0.04 (Fig. 2).

Forest plot for the effect of genetically determined TSH on AD risk using summary statistics for full range TSH levels (HUNT + MGI + ThyroidOmics meta-analysis), full range TSH levels (HUNT study), TSH within the normal range in the HUNT study, and TSH levels in individuals younger than 50 years old (HUNT study). HUNT, a longitudinal population health study in Norway; MGI, Michigan Genomics Initiative.
MR-PRESSO global test p-value was significant for all four sets indicating the detection of overall horizontal pleiotropy. However, after the removal of horizontal pleiotropic outliers, the MR estimates remained nonsignificant (Supplementary Tables). There was no evidence for the causal association between hypothyroidism and AD (hypothyroidism: p = 0.99) (Supplementary Tables S6 and S7).
Bidirectional MR analyses
Bidirectional MR analysis was carried out to address a potential reverse causal association and investigate whether AD has a causal effect on TSH levels. Across all MR methods, the results suggest no evidence for causal association between AD and normal range TSH (p = 0.27) of fT4 (p = 0.15) levels. In the MR PRESSO analysis, The global test returned a nonsignificant p-value, suggesting no evidence for horizontal pleiotropy (Supplementary Table S8).
Discussion
This study's main aim was to explore the causal relationships between thyroid function and AD with the use of bidirectional MR techniques. We showed that increased levels of genetically predicted TSH within the normal range were significantly associated with a decreased risk of AD, in agreement with previous evidence (5,7,8). We further explore the effect of full range TSH levels on AD risk by using summary statistics from different data sets, including data from the largest meta-analysis from HUNT+MGI+ThyroidOmics along with analyses only using data from the HUNT study, as a more homogeneous set.
As a more extreme phenotype, we further explored the effect of variation in normal range TSH on AD risk in individuals younger than 50 years old. In addition, we evaluated the role of genetically predicted hypothyroidism on AD risk, as not only variation in normal range TSH, but also hypothyroidism has been associated with AD in epidemiological studies. We refrained from performing MR analyses on hyperthyroidism instruments and AD risk, as the number of consistently associated hyperthyroidism variants is limited.
Both normal range fT4 levels and hypothyroidism had no significant associations with AD. Bidirectional analyses showed no causal effect of genetically predicted AD on TSH or fT4 levels.
The nonthyroidal illness syndrome (NTIS) is characterized by changes in serum thyroid function tests in the absence of thyroid or hypothalamic-pituitary-thyroid axis (HPT) dysfunction. NTIS has not only been observed in critically ill patients, but also in up to one-third of patients suffering from neuropsychiatric diseases. In addition, Tan et al. (6,23) theorized that the link between thyroid function and AD is based on the aggregation of amyloid β peptides that leads to less thyrotropin-releasing hormone (TRH) being secreted by the hypothalamus.
This affects the TRH's role within the pituitary gland, thus decreasing the production of TSH, leading to a decrease of thyroxine levels (23). Our finding that increased thyroid function increases the risk of AD and not vice versa makes these proposed explanations unlikely, and improves our understanding of the associations between thyroid function and AD observed in epidemiological studies.
We identify thyroid function as a novel AD risk factor that can be modified. This is also of interest since there is an ongoing discussion on whether mild (subclinical) variations in thyroid function should be treated or not (24,25). Future studies should determine below what TSH level onward the risk of AD increases in a clinically relevant manner, and whether modifying thyroid function indeed modifies AD risk.
There are several inconsistencies in previous observational studies regarding the relationship between thyroid function and AD. A recent study that looked at the relationship between decreased regional cerebral blood flow (rCBF), associated with AD, and thyroid function found significant correlations between TSH and rCBF (26). However, this result was only seen within patients exhibiting mild cognitive impairment and not in patients with AD.
The Framingham study of 2008 found that both the upper and lower tertiles of TSH in the normal range indicated an increased risk of dementia in women (6), but not in men. Wu et al.'s meta-analysis showed that high fT4 and low TSH outside the normal range were significantly associated with AD (27). These findings partly concur with our findings as low TSH levels within the normal range were found to be a risk factor for AD.
This affects the TRH's role within the pituitary gland, thus decreasing the production of TSH leading to a decrease of thyroxine levels (23). In addition, another meta-analysis study found that higher fT4 and lower TSH were a risk factor in patients developing dementia (27). The theory also implies that AD had a causal relationship on TSH and fT4, rather than the inverse. Our study's bidirectional analysis did not show any significant causal relationship between AD and thyroid function. A potential cause for the differing results when looking at the relationship between AD and thyroid function could be that some studies were cross-sectional looking at the correlations as opposed to the causal relationship.
In addition, these observations are in line with results from previous studies in which various classical thyroid-related endpoints [atrial fibrillation, stroke, cholesterol levels, etc. (28)] were associated with the TSH instruments but not with the fT4 instruments. This strongly suggests that the TSH instruments are associated with thyroid function in a classical sense (i.e., higher TSH levels and lower fT4 levels), whereas the fT4 instruments do not. This is also plausible when taking a closer look at the individual fT4 instruments as these include a heterogeneous group of genes that predominantly have a role in determining peripheral thyroid hormone status (e.g., transporters and deiodinases), instead of a role in the central HPT axis.
This is a well-powered study that could detect even small effects of variation in thyroid function on AD. There are many strengths for using MR as a method to find causal relations and reduce confounding. The summary statistics used were from the largest GWAS published to increase statistical power. Pleiotropy was tested using sensitivity analyses, and possible pleiotropic variants were removed, which did not significantly change the results. The use of MR approaches to investigate nonconfounded causal associations is becoming more prevalent due to the many advantages that the method has over more traditional observational epidemiological studies.
Furthermore, multiple methods of MR were used to reduce biased estimates that helped in finding consistent results. A potential limitation of our study is that we focused our analyses on individuals of European ancestry, suggesting that these results could not be easily transferred to other populations. We also did not perform nonlinear MR to examine potential nonlinear effects. In addition, we potentially did not observe an association between hypothyroidism and AD due to the fact that various autoimmune diseases coincide and have a shared genetic basis, leading to a heterogeneous group of genetic instruments.
Conclusions
We show that increased levels of genetically predicted TSH within the normal range are associated with a decreased risk of AD. These results were concordant for individuals younger than 50 years old. The effect of an increase in the genetically predicted full range TSH was marginally associated with a decrease in AD risk. In contrast, our results do not show any evidence for a causal association between neither fT4 nor hypothyroidism with AD. These results could be clinically relevant, as appropriate management of thyroid function could benefit an individual's risk of developing AD. Our study could encourage further studies involving randomized control trials for thyroid function and AD. Additional studies would be needed to clarify the exact underlying mechanism.
Footnotes
Authors' Contributions
Study conception and design were done by E.M. and P.D. Analyses were carried out by E.M., L.Y., R.O., and A.D.K. Draft of the article was done by E.M., L.Y., and R.O. Supervision of the study was carried out by E.M. and P.D. Interpretation of results, critical editing, and article approval were done by all authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study forms part of the research themes contributing to the translational research portfolios of the Barts Biomedical Research Centre funded by the U.K. National Institute for Health Research (NIHR) (E.M. and P.D.).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8