
Abstract
Background:
The optimal serum thyrotropin (TSH) level for postlobectomy papillary thyroid carcinoma (PTC) patients is unclear. The objective of this study was to examine the association of TSH and recurrence in postlobectomy patients.
Methods:
Patients who underwent lobectomy for PTC in a single tertiary hospital from January 2000 to December 2014 were enrolled. The mean TSH of a patient was calculated based on each serum TSH value during follow-up. The reference range of serum TSH was 0.5–4.0 mU/L. Univariate and multivariable analyses were performed with Cox proportional hazards models. Restricted cubic spline (RCS) functions were used to model relationships between mean TSH and recurrence-free survival (RFS).
Results:
A total of 2297 patients (median age 42 years; 1750 (76.2%) female) were analyzed. Mean TSH below (≤0.5mU/L), in the lower half (0.6–2 mU/L), in the upper half (2.1–4 mU/L), and above (>4 mU/L) the reference range were observed in 668 (29.1%), 1162 (50.6%), 345 (15.0%), and 122 (5.3%) patients, respectively. According to the Cox model and RCS, no association was observed between mean TSH and RFS in the whole cohort, low-risk group and intermediate- to high-risk groups (adjusted p = 0.4737, 0.9314, 0.1859, adjusted p for nonlinear = 0.4589, 0.8622, 0.3010). The only RFS difference observed in the stratified univariate analysis was between patients with mean TSH in the lower half (0.6–2 mU/L, n = 659) and above the reference range (>4 mU/L, n = 68) in the intermediate- to high-risk group (10-year RFS by Kaplan–Meier 84.4% vs. 69.4%, log rank p = 0.011).
Conclusions:
Mean serum TSH levels are not associated with recurrence. A normal TSH reference range is recommended for postlobectomy PTC patients.
Introduction
Thyrotropin (TSH) stimulates the proliferation of normal thyrocytes as well as differentiated thyroid carcinoma (DTC) cells, thereby providing the rationale for TSH suppression therapy for postoperative papillary thyroid carcinoma (PTC) patients. However, the appropriate intensity of TSH suppression therapy remains controversial in recent years (1,2). The 2015 American Thyroid Association (ATA) guidelines suggested a comprehensive consideration of both tumor recurrence and thyroxine suppression risks (3). Although these recommendations are theoretically reasonable, the evidence is still not strong enough, except for high-risk patients, according to the ATA initial risk stratification (4 –6). Moreover, these suggestions are aimed at patients who underwent total thyroidectomy and radioactive iodine ablation, but whether this is applicable in patients who underwent lobectomy is unclear due to the paucity of data.
With an increasingly conservative attitude on the treatment of PTC, indications for lobectomy have expanded (3,7). Although the ATA guidelines recommended an interval that in the mid to lower reference range (0.5–2 mU/L) for low-risk patients who have undergone lobectomy, there is still a continued debate on this point (3). Park et al. revealed that serum TSH ≤1.85 mU/L independently predicted lower early recurrence (within the first 2 years after lobectomy) in patients with low- or intermediate-risk PTC (8). Then the study recommended an optimal TSH range of ≤1.85 mU/L. Park et al. found that there was no significant difference in disease-free survival between postlobectomy PTC patients with different serum TSH levels (9). Owing to the residual thyroid gland, the relation between TSH and tumor recurrence may not be simple or linear, as in patients after total thyroidectomy, and the optimal level of TSH should be considered for postlobectomy patients.
We designed this study to examine the association between the mean TSH level and structural recurrence with a Cox regression model and restricted cubic splines (RCS) and to further examine the recurrence differences between patients with different TSH intervals to determine the optimal TSH level in patients after lobectomy.
Materials and Methods
Patients
Adult patients (18–75 years) who underwent lobectomy for PTC at the National Cancer Center, Cancer Institute and Hospital, Chinese Academy of Medical Sciences between January 2000 and December 2014 were included. Patients with preoperative evidence of distant metastasis, aggressive histological variants, including columnar/tall cells, diffuse sclerosing and insular variants, positive surgical margins or incomplete TSH data during follow-up (< 2 data, < 5 months after surgery or a previous follow-up visit was not recorded) or a follow-up period ≤12 months were excluded. The study was approved by the Ethics Committee of the Cancer Hospital, Chinese Academy of Medical Sciences. Informed consent was obtained at the time of surgery with surgical consent for general use of clinical information for future studies.
Treatment and follow-up
During the study period, lobectomy tended to be performed in patients who had unilateral disease without advanced primary or regional tumors. Prophylactic central node dissection was not routinely performed for cN0 patients, the decision would depend on evaluation on risk factors (large primary size, ETE, multifocality, etc.). The patient demographics and characteristics of the tumors were obtained from the institutional database. Primary tumor size was determined based on pathological reports. The presence of minor extrathyroidal extension and gross extrathyroidal extension were identified on pathological reports and surgical findings, respectively. Hashimoto thyroiditis was determined when the pathological report documented lymphocytic thyroiditis. The patients were staged according to the American Joint Committee on Cancer staging system (8th edition). The initial risk stratification was performed according to the 2015 ATA guidelines.
All patients enrolled were recommended thyroid hormone replacement therapy with
Measurement of serum TSH
Serum TSH concentrations were determined using an automated electrochemiluminescence immunoassay (Cobas e 601; Roche Diagnostics, Mannheim, Germany) with a functional sensitivity of at least 0.01 mU/L and a reference range of 0.5–4.0 mU/L. The mean value of all effective serum TSH throughout the course of follow-up was used to measure the overall TSH level of a patient.
Statistical analysis
All statistical analyses were conducted with the R package, version 3.6.2 (R Foundation for Statistical Computing, Vienna, Austria). Continuous and categorical variables were compared across groups using the t-test and the Pearson χ 2 test, respectively. The association of mean TSH and structural recurrence was assessed using univariate and multivariate Cox regression models with RCS. Optimal numbers of knots were chosen based on the lowest Akaike information criterion, and five knots were placed in the analysis. p for mean TSH and nonlinearity was calculated to evaluate the relation and nonlinear relation between mean TSH and RFS. The RFS differences were also examined using Kaplan–Meier curves and log-rank tests between different mean TSH and recurrence risk subgroups. p < 0.05 was considered statistically significant.
Results
Baseline characteristics of the patients
Between 2000 and 2014, a total of 2297 patients were enrolled based on the inclusion and exclusion criteria (Fig. 1). The median age of the cohort was 42 years (range 18–75 years), and 1750 (76.2%) were female. The mean tumor size in the resected lobe was 1.23 ± 0.98 cm and 59.2% of patients had a tumor less than 1 cm. Central neck dissection and lateral neck dissection were performed in 1629 (70.9%) and 520 (22.6%) patients, respectively. The initial risk stratification indicated that 946 (41.2%), 975 (42.4%), and 376 (16.4%) patients had low-, intermediate-, and high-risk recurrence, respectively (Table 1).
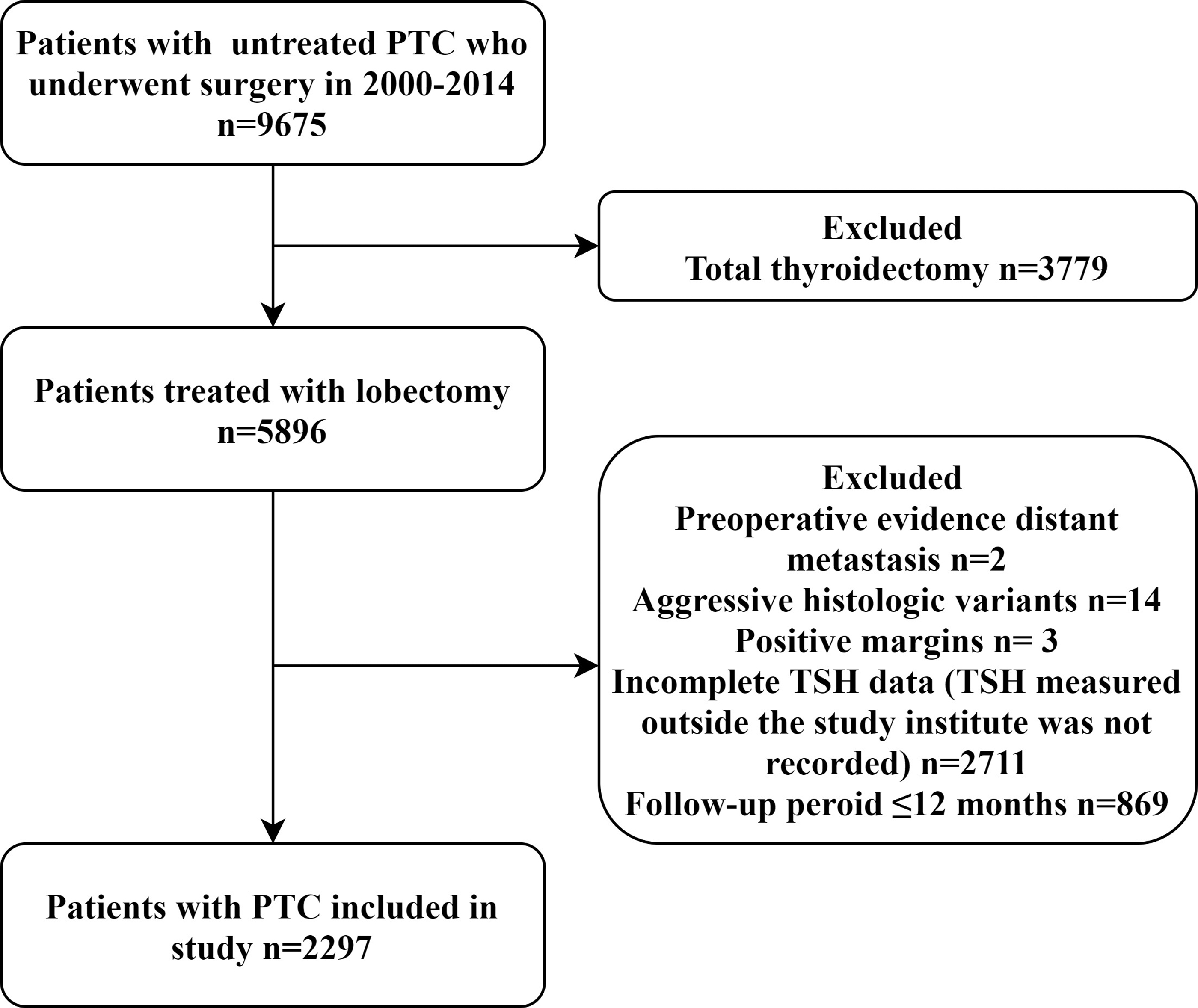
Flow diagram showing the inclusion and exclusion of patients in the study.
Study Cohort Characteristics
ATA, American Thyroid Association.
During a median follow-up of 70 months, 167 (7.3%) structural recurrences were observed, 26 patients died, and 11 of whom died from PTC. Local or regional recurrence accounted for 84.4% (141 patients; 37 local, 66 regional, and 38 both) of recurrences, and distant metastases accounted for 26 recurrences (12 alone and 14 combined with local or regional recurrence). Recurrences in the residual lobe, thyroid bed, central neck, and lateral neck were detected in 71, 6, 60, 90 patients, respectively. The RFS rates at 5 and 10 years were 94.7% and 84.7%, respectively. More than four-fifths of recurrences (81.4%) occurred in intermediate- to high-risk patients.
Serum TSH levels during follow-up
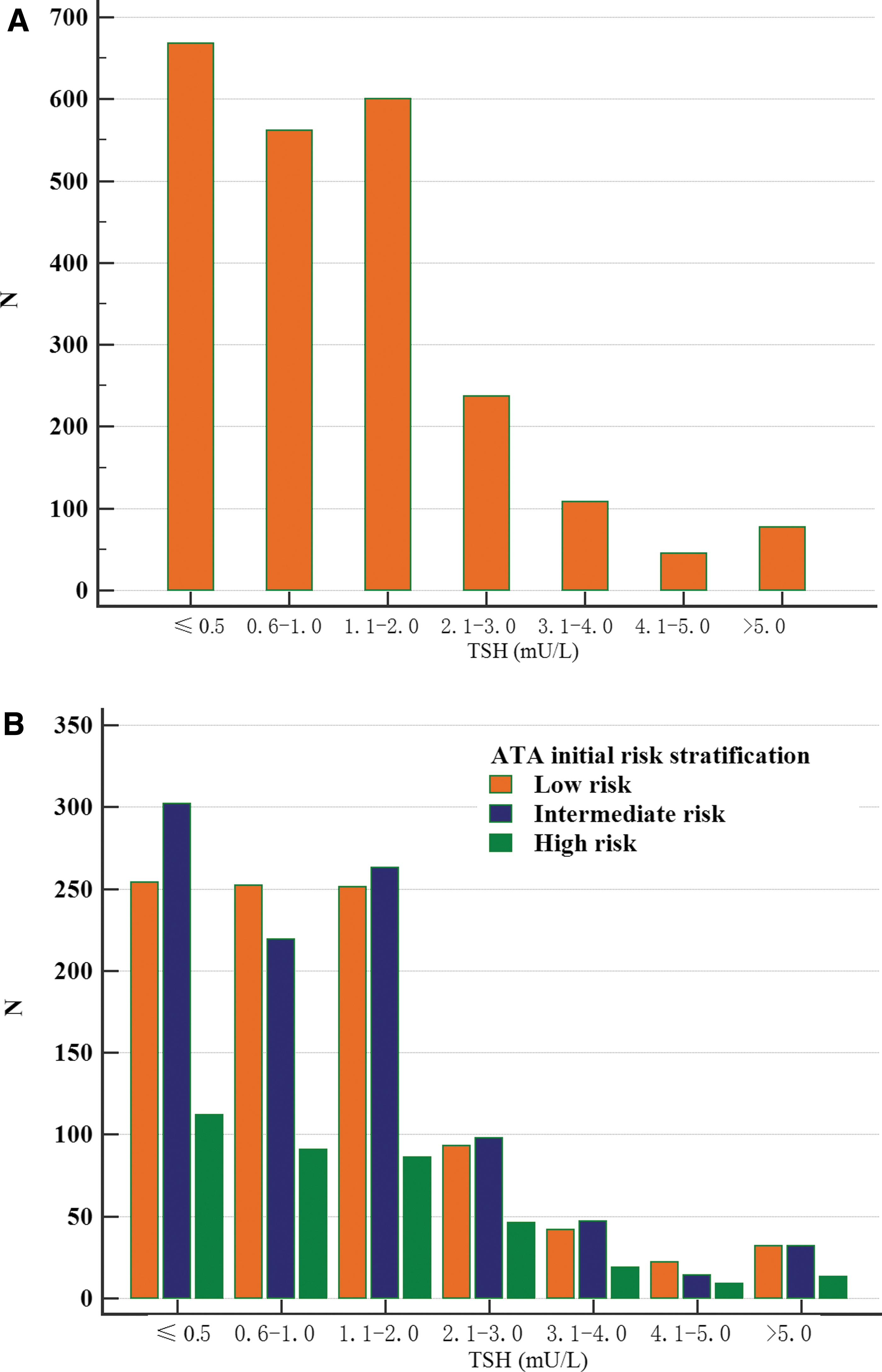
During the study period, the mean TSH of the cohort was 1.456 ± 2.224. Mean TSH below (TSH ≤0.5 mU/L), in the lower half (0.5 mU/L < TSH ≤2 mU/L), in the upper half (2 mU/L < TSH ≤4 mU/L), and above (TSH >4 mU/L) reference ranges were observed in 668 (29.1%), 1162 (50.6%), 345 (15.0%), and 122 (5.3%) patients, respectively (Fig. 2A).
Mean TSH in the overall study cohort (
When considering the ATA initial risk stratification, there was no significant difference in the mean TSH between low-risk patients and indeterminate- to high-risk patients (1.490 mU/L vs. 1.432 mU/L; p = 0.537), and mean TSH ≤2mU/L was observed in 757 (80.0%) low-risk patients, 784 (80.4%) intermediate-risk patients, and 289 (76.9%) high-risk patients (p = 0.327) (Fig. 2B).
Dose–response association between the mean TSH and RFS
In Figure 3, we used RCS to flexible model and visualized the relationship of mean TSH and RFS in low-risk and intermediate- to high-risk groups based on univariate and multivariate Cox proportional models. Five knots were placed for RCS, and unadjusted hazard ratio (HR) was shown in Figure 3A with increasing mean TSH. In Figure 3B, HR was adjusted with primary tumor size, extrathyroidal extension, multifocality, lymph node dissection (no, central or lateral) and N stage. There was no significant overall association between mean TSH and RFS, and no significant nonlinear association was observed in the whole cohort (unadjusted p for mean TSH = 0.1201, p for nonlinear = 0.1763, adjusted p for mean TSH = 0.4737, p for nonlinear = 0.4589). Stratified analysis indicated in patients with low-risk, no significant overall and nonlinear association was observed (unadjusted p for mean TSH = 0.9394, p for nonlinear = 0.8513, adjusted p for mean TSH = 0.9314, p for nonlinear = 0.8622) (Fig. 3C, D), while in patients with intermediate- to high-risk, unadjusted overall association is statistically significant but the significance lost after adjustment (unadjusted p for mean TSH = 0.0384, p for nonlinear = 0.1356, adjusted p for mean TSH = 0.1859, p for nonlinear = 0.3010) (Fig. 3E, F). It was also observed that the dotted line (HR = 1) was always in the confidence interval (blue area), which indicates no significant association between the analyzed variables.

Unadjusted (
Stratified univariate analysis of RFS considering mean TSH and risk stratification
The RFS differences were further examined between patients with different mean TSH in the low-risk and intermediate- to high-risk groups. According to Kaplan–Meier curve and log-rank test, in the low-risk group, patients with mean TSH below, in the lower half, in the upper half and above reference range had similar RFS (10-year RFS 95.1%, 89.4%, 96.1% and 91.2%, respectively, all p > 0.05), and in intermediate- to high-risk group, the 10-year RFS of patients with mean TSH below, in the lower half, in the upper half, and above reference range were 78.5%, 84.4%, 71.6% and 69.4%, respectively, the only RFS difference was observed between patients with mean TSH in the lower half and those above the reference range (84.4% vs. 69.4% p = 0.011) (Table 2).
Ten-Years Recurrence-Free Survival by Kaplan–Meier Curve of Patients with Different Mean Thyrotropin Intervals and Risk Stratifications
Comparisons of RFS between patients with different mean TSH intervals in the same risk stratification group.
RFS, recurrence-free survival; TSH, thyrotropin.
Discussion
It is difficult to comprehensively define the impact of serum TSH levels on PTC prognosis after lobectomy. Although the recurrence risk increasing with elevating TSH is theoretically reasonable, due to the impact of residual thyroid, the relation between TSH and recurrence in postlobectomy patients may be complex. Moreover, most postlobectomy patients analyzed in a previous study had a low risk for recurrence (1.4–4.0%) (9 –11), then a relatively large sample is required to ensure enough statistical power. In this study, we conducted a large cohort with a relatively large number of recurrences, and established a Cox proportional model with RCS and adjustment for multiple recurrence-related variables. These study designs strengthen the findings that postlobectomy serum TSH level may not be significantly related to PTC recurrence.
Another difficulty in clarifying the impact of postlobectomy serum TSH level on tumor recurrence is that TSH may be affected by both
Our findings are consistent with what observed in some previous studies. Lee et al. divided 1528 low-risk DTC patients who underwent lobectomy into four groups (<0.5, 0.5–1.9, 2.0–4.4, and ≥4.5 mU/L) according to the mean and dominant TSH values during the entire follow-up period or five years and observed that neither mean nor dominant TSH values affected RFS (p = 0.15, 0.27) (10). In another retrospective propensity-score matched cohort study including DTC patients (n = 446) who underwent lobectomy with or without TSH suppression therapy, Park et al. found that there was no significant difference in disease-free survival between different serum TSH levels (p = 0.57) (9). A prospective study of 263 PTC patients (65% low risk, 24% intermediate-low risk, and 11% intermediate-high risk) revealed that the rates of structural disease at 1 and 3 years after surgery were similar among different TSH levels measured at 6–18 months (<0.1, 0.1–0.5, 0.5–2, and >2 mU/L) (p = 0.2) (11). In this study, we also compared the patients with different mean TSH levels (below, in the lower half, in the upper half, and above reference range [<0.5, 0.6–2, 2.1–4, and >4 mU/L]) on RFS, and no significant difference was observed in patients below and within the reference range, even in patients belonging the intermediate- to high-risk subgroups. These results also enhance the findings concluded from the RCS curve.
This study has several limitations. First, owing to the retrospective nature of these data, the follow-up period and interval of each TSH measurement of patients enrolled in our study were varied. We excluded patients with less than two recorded data points and selected mean TSH scores to adjust this problem, which can better reflect the dominant TSH and its fluctuation. Second, all patients enrolled in our study were routinely recommended thyroid hormone replacement therapy; however, the dose of
Conclusion
In this study, no association was observed between the mean TSH level and tumor recurrence of postlobectomy PTC patients among the whole interval of TSH, and RFS was similar in patients whose mean TSH was within or below the reference range. A normal reference range is recommended as the optimal level of TSH for these patients.
Footnotes
Authors' Contributions
S.Y.X. participated in the design of the study, data collection, and article writing. Y.H. participated in the design of the study and article writing. H.H. participated in the data collection and helped to draft the article. X.H.Z. participated in the article writing and statistical analysis. J.X.Q. participated in the data collection. X.L.W. and Z.G.X. participated in the design of study and article editing. S.Y.L. participated in the data analysis and interpretation and article review. J.L. participated in the design of the study and helped to revise the article. All authors read and approved the final article.
Statement of Ethics
The study was approved by the Ethics Committee of the Cancer Hospital, Chinese Academy of Medical Sciences.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was funded by the CAMS Innovation Fund for Medical Sciences (CIFMS; Grant No. 2016-I2m-1-002) and Beijing Hope Run Special Fund of Cancer Foundation of China (Grant No. LC2018A26).