
Abstract
Background:
This exploratory study was meant to assess clinical and safety data with a novel fibroblast activation protein inhibitor-based targeted theranostics as a salvage treatment option in radioiodine-refractory differentiated thyroid cancer (RR-DTC) patients who had progressed on tyrosine kinase inhibitors.
Methods:
Patients with metastatic RR-DTC who progressed on sorafenib/lenvatinib were prospectively recruited. If [68Ga]Ga-DOTA.SA.FAPi positron emission tomography/computed tomography scan demonstrated moderate-to-excellent uptake in metastases, and patients had given informed consent, they received intravenous [177Lu]Lu-DOTAGA.(SA.FAPi)2 as therapy at eight-weekly intervals. The primary endpoints were thyroglobulin (Tg) response and functional imaging response. The secondary endpoints were visual analog score (VAS) and Eastern Cooperative Oncology Group (ECOG) performance status. The grading of toxicities was performed by using Common Terminology Criteria for Adverse Events (CTCAEV5.0). The sequential images were acquired by a dual-headed gamma camera, and dosimetric calculations were performed by using OLINDA/EXM V2.1.
Results:
Fifteen patients were recruited [age: 55 ± 9 years (range: 39–67)]. [177Lu]Lu-DOTAGA.(SA.FAPi)2 had median whole-body Teff of 88.06 hours (interquartile range [IQR]: 86.6–99). The colon was identified as a critical organ. The whole-body effective dose was 1.62E-01 ± 1.53E-02 mSv/MBq. A total of 45 cycles were administered, and the median cumulative administered activity was 8.2 ± 2.7 GBq (range 5.5–14 GBq). The median absorbed doses to the tumor lesions were 1.08E+01 (IQR: 4.16E+00 to 8.97E+01) mSv/MBq per cycle. The Serum Tg level significantly decreased after treatment [(median Tg: baseline–10,549 ng/mL (IQR: 3066.5–39,450) versus at the time of assessment: 5649 ng/mL (IQR: 939.5–17,099), p = 0.0005)]. Molecular response assessment revealed no complete response; however, partial response was documented in four, and stable disease in three patients. The VASmax scores [pre-therapy: 9 (IQR: 8–10) versus follow-up: 6 (3–6) (p-0.0001)], and ECOG [3, (IQR: 2–3 vs. 2, (IQR: 2–3) (p-0.0078)] performance scores significantly improved after treatment. None of the patients experienced grade III/IV hematological, renal, or hepatotoxicity.
Conclusion:
These preliminary data suggest that the novel molecule [177Lu]Lu-DOTAGA.(SA.FAPi)2 is safe, seems effective, and, most importantly, opens up a new avenue for the treatment of aggressive RR-DTC patients who have exhausted all standard line of treatments.
Introduction
Radioiodine (RAI) treatment is the mainstay adjuvant treatment option in the management of intermediate and high-risk differentiated thyroid cancer (DTC). However, ∼5% to 15% of locoregional DTC and 40–50% of metastatic DTCs are refractory to RAI treatment (1 –3). It is a well-known fact that RAI refractoriness is associated with poor outcome, leading to cancer-specific mortality of 60% to 70% at 5 years (4). Moreover, patients with RAI refractory metastatic DTC are associated with the worst outcome with a 10-year survival probability of 10% (5).
In recent years, a better understanding of molecular pathways involved in the tumorigenesis, the dysfunction of the Na+/I− symporter system, and abnormal tyrosine kinase pathways have led to the development of multikinase inhibitors (MKIs). Among the various MKIs, sorafenib based on DECISION trial (6) and lenvatinib based on SELECT trial (7) have been Food and Drug Administration (FDA) approved for the use in radioiodine-refractory differentiated thyroid cancer (RR-DTC) patients. Lenvatinib significantly prolonged progression-free survival as compared with the placebo group (18.3 months in Lenvatinib group vs. 3.6 months in the placebo group). However, 23.9% of patients with skeletal metastases progressed on lenvatinib; overall, 75.9% had treatment-related adverse events (AEs) that were grade III or higher. In either of the scenarios, patients cannot further continue MKI treatment and have depleted all lines of treatment.
Apart from the genetic alterations that contribute to the management of aggressiveness of DTC, recent investigations have uncovered the contributions of tumor microenvironment (TME) in the growth and progression of the disease (8). Cancer-associated fibroblasts (CAFs) are the key component of TME, and play a key role in the progression of varieties of human cancers, including abnormally high fibroblast activating proteins (FAPs) expression in thyroid cancer (9 –11). The FAP inhibitors (FAPIs), recently developed as small-molecule radioligands, both for positron emission tomographic (PET) imaging and as radioligand therapy options, are being explored in many cancers. The literature is sparse regarding the use of FAPI radioligand therapies in RR-DTC. A couple of publications in a small number of patients have shown that the presence of CAFs in papillary thyroid cancer (PTC) patients was associated with an increased frequency of lymph nodal metastases (12). Sun et al. (13) have reported a strong relationship between the prevalence of BRAFV600E mutation and the high expression of FAP in human PTCs. The authors also revealed that high stromal reactivity was associated with a shorter overall survival. Targeting CAF to treat thyroid cancer with an aim to arrest or interfere the activation of CAFs and thereby inhibit CAF functions is a new strategy in precision oncology.
Recently, several FAPI molecules such as [68Ga]Ga-labeled FAPI-02 (14), -04 (14), -46 (15), and
Encouraged by the promising dosimetry results and the need for safe and effective treatment stratigies in RR-DTC, this pilot study was undertaken to share the clinical experience with [177Lu]Lu-DOTAGA.(SA.FAPi)2 therapy as a salvage treatment option in advanced-stage RR-DTC patients.
Methods
This prospective study for the treatment of RR-DTC patients with [177Lu]Lu-DOTAGA.(SA.FAPi)2 treatment was approved by the ethics committee of the All India Institute of Medical Sciences, New Delhi on compassionate grounds in patients who have failed standard treatment options (Ref. No: IEC/1054/5/2020).
Eligibility criteria
Eligibility criteria for [177Lu]Lu-DOTAGA.(SA.FAPi)2 treatment included: >18 years of age, histologically (histopathological examination) confirmed DTC, documented radiological/molecular or biochemical disease progression on previous lines of treatment, documented as RR-DTC, Eastern Cooperative Oncology Group (ECOG) status up to 4, cancers that demonstrated high FAPi expression on [68Ga]Ga-DOTA.SA.FAPi PET/computed tomography (CT) scan, patients with greater or equal number of lesions that were positive on [68Ga]Ga-DOTA.SA.FAPi PET/CT scan compared with the corresponding [18F]F-FDG PET/CT scan, and patients who signed the informed consent form.
Patients who received prior anti-cancer therapy in <4 weeks' time, pregnant or lactating women, patients with Hb <9 g/dL, leukocyte counts <4.0 × 109/L, platelet counts <75,000 per mL, inadequate liver function parameters, and serum creatinine >1.2 mg/dL at the baseline were excluded from the study.
Initially, among 19 patients who underwent [68Ga]Ga-DOTA.SA.FAPi and [18F]F-FDG PET/CT scans, 4 were excluded, among whom 2 demonstrated lesser number of lesions on [68Ga]Ga-DOTA.SA.FAPi and the remaining 2 showed mild FAPi expression contrary to the avid uptake on flurodeoxyglucose (FDG) (Fig. 1).
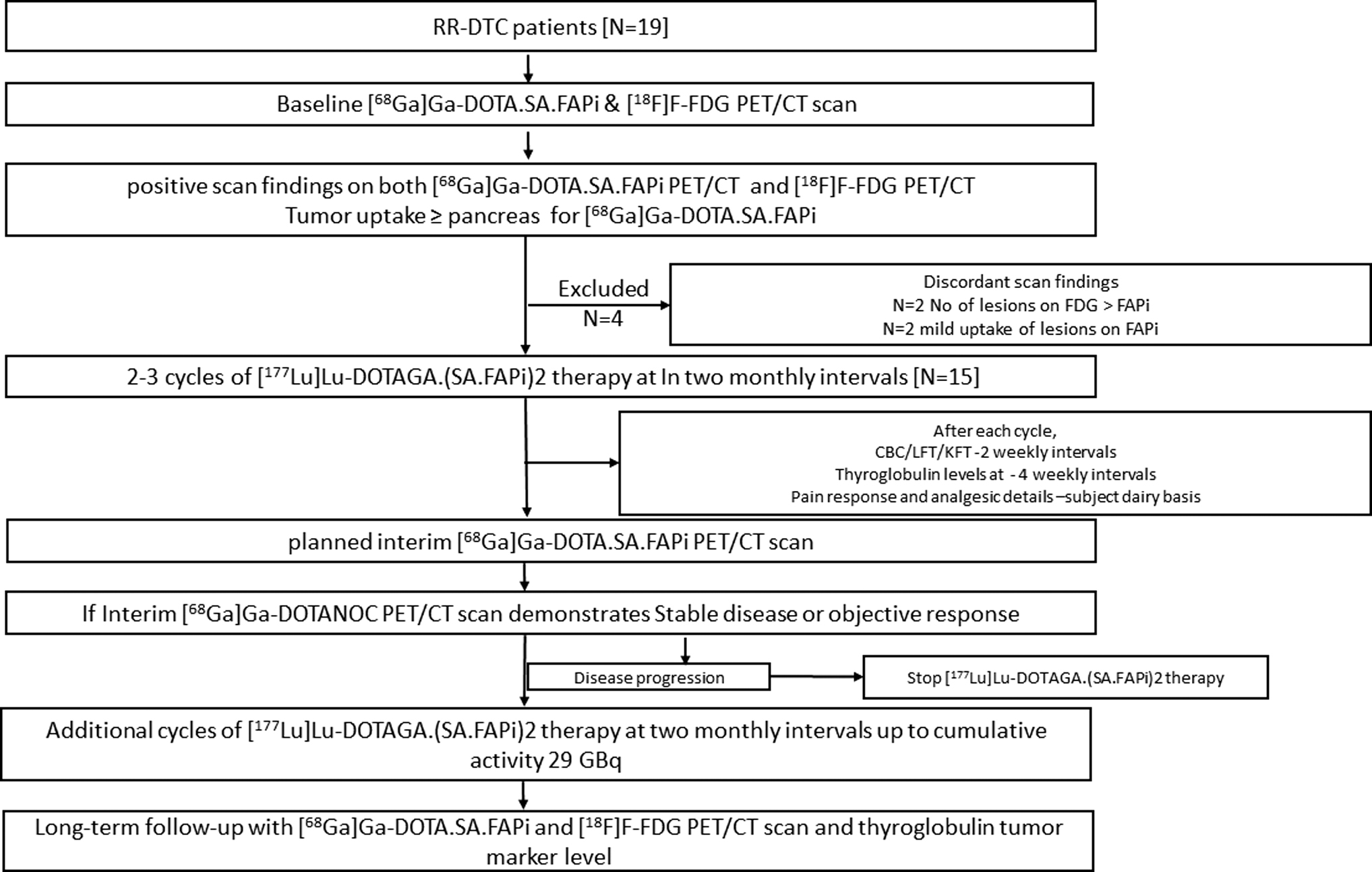
Flow chart depicting the [177Lu]Lu-DOTAGA.(SA.FAPi)2 treatment planning and follow-up protocol.
Finally, our analysis included 15 eligible patients with advanced RR-DTC who progressed from MKIs, and these were treated with [177Lu]Lu-DOTAGA.(SA.FAPi)2. Patients were followed up between October 2020 and September 4, 2021 with a median follow-up duration of 7.2 (interquartile range [IQR]: 6.3–8.1) months. Among them, three patients participated in the dosimetry study (no. 1, 4, and 7) at their first cycle of [177Lu]Lu-DOTAGA.(SA.FAPi)2 treatment.
Definition of RR-DTC
The definition of RR-DTC was adopted as per The American Thyroid Association (ATA) 2015 Guidelines, namely structural progressive disease according to RECIST1.1 (20), with no further indication for RAI treatment, because of a partial or complete lack of RAI uptake, or evidence of progression despite RAI avidity at the time of treatment or after receiving cumulative RAI activity ≥22.2 GBq (600 mCi) (21).
Image acquisition, analysis for [18F]F-FDG and [68Ga]Ga-DOTA.SA.FAPi PET/CT
In all patients, baseline [18F]F-FDG and [68Ga]Ga-DOTA.SA.FAPi PET/CT scans were acquired before the initiation of treatment to compare the sites of lesion uptake between both the radiotracers. During follow-up, as solely patients with FAPi findings (number of lesions)≥FDG at the baseline were treated, only [68Ga]Ga-DOTA.SA.FAPi PET/CT scan was performed to minimize frequent unwanted radiation exposure.
Acquisition protocol
Scans were obtained on a dedicated GE Discovery 710* 128 Slice PET/CT Scanner, with a 40-mm detector at a rotation speed of 0.35 seconds. Although for [18F]F-FDG PET/CT, patients were advised to fast for at least four to six hours before injection, no such preparation was required for a [68Ga]Ga-DOTA.SA.FAPi scan. The mean injected activities were 251.6 ± 61.42 (range: 118.4–333) MBq and 200 ± 74 (range: 111–285) MBq, for [18F]F-FDG, and [68Ga]Ga-DOTA.SA.FAPi radiotracers, respectively. The time interval between [68Ga]Ga-DOTA.SA.FAPi and [18F]F-FDG PET/CT scans was no more than 10 days. For the acquisition, an initial scout image followed by CT, and PET scans were acquired at two minutes per bed. The diagnostic CT parameters involved 300–350 mAs, 120 kVp, slice thickness of 5 mm, and a pitch of 1.
Image analysis
For the head–head comparison, both [18F]F-FDG and [68Ga]Ga-DOTA.SA.FAPi PET/CT scans were loaded simultaneously and co-registered by using carina as an anatomical landmark registration technique. Scan interpretations was conducted by two experienced Nuclear Medicine physicians. Any disagreement in the reports was reviewed by a third observer.
Qualitative analysis
For qualitative interpretations, the visual interpretation method was adopted to compare the concordance or discordance in the uptake between the tracers and compared with the morphological findings on CT. Any disagreement in the findings was reconfirmed either by histopathological correlation or by other imaging modalities. For the ease of analysis, the lesions were interpreted according to four anatomical sites: local disease (primary/residual tumor), nodal metastases, distant metastases (pulmonary, skeletal, liver, brain, etc.), and other metastatic sites.
Quantitative analysis
Quantitative analysis and comparison were conducted according to the region of interest (ROI) methods prescribed by PERCIST 1 criteria (22). In brief, both PET/CT scans were linked followed by placing ROIs on normal organs and lesions on [18F]F-FDG PET/CT scan, which was cloned on the [68Ga]Ga-DOTA.SA.FAPi PET/CT scan. The values in the respective ROIs were presented as standardized uptake value corrected for lean body mass, SULpeak, and SULavg. To compare the uptake in the lesions, a three-dimensional auto contour ROI at a 40% threshold of SULpeak was carefully drawn around the site of [18F]F-FDG/[68Ga]Ga-DOTA.SA.FAPi expressing lesions.
[177Lu]Lu-DOTAGA.(SA.FAPi)2 synthesis
DOTAGA.(SA.FAPi)2 was provided by our collaborators from the University of Mainz, Germany. FAPi dimer of 30 μg was radiolabeled [177Lu]LuCl3, which was obtained from BRIT, India, in sodium acetate buffer, pH 4, in 0.01 M supra pure HCl. The radiolabeled solution was heated at 95°C for 30 minutes. The radiolabeled product of >90% purity was administered to the patients.
Treatment protocol
The detailed patient recruitment and therapy protocol in the form of a flow chart is depicted in Figure 1. [177Lu]Lu-DOTAGA.(SA.FAPi)2 infusion involved a dilution in 30 mL normal saline (0.9%), which was administered intravenously over 10 minutes, with subsequent flushing of 10 mL normal saline. The entire process was performed on an inpatient basis, and patients were discharged in a few hours of observation if they did not show any adverse reaction. In the later phases of the study after understanding the biodistribution and pharmacokinetics of the [177Lu]Lu-DOTAGA.(SA.FAPi)2 radiotracer, patients were instructed to have high fatty food diet and prescribed laxative syrup for the first 72 hours post-treatment to increase the liver–gallbladder excretion and bowel transit of the radiotracer.
Post-therapy [177Lu]Lu-DOTAGA.(SA.FAPi)2 whole-body scintigraphy
The whole body and organ dosimetry were performed as per the methodology detailed in the Supplementary Data. In brief, the planar acquisition of post-therapy whole-body scans (PTx-WBS) was performed by using a dual-headed gamma camera (Discovery NM/CT 670; GE). The camera was equipped with a high-energy general-purpose parallel-hole collimator, and the energy peak was cantered at 113 and 208 keV with a 10% window width. Serial anterior and posterior PTx-WBS emission scans were performed at 1 (pre-void), 4–6, 24, 48, 96, and 144–168 hours post-injection (p.i.), in 3 patients and in the remaining scans were conducted at 24–48 hours p.i.
Similarly, SPECT/CT scans of the abdomen and the lesions were acquired. The SPECT/CT acquisition parameters included a total angular range of 360°, an angle view of 6°, acquired at 25 seconds per view, and a matrix size of 512 × 512.
Tumor dosimetry
For the tumor dosimetry, a sphere model implemented within OLINDA/EXM v2.1 was used. For each considered lesion, the volume was evaluated on pre-therapy [68Ga]Ga-DOTA.SA.FAPi PET/CT and PTx SPECT-CT of the area of interest using the commercially available workstation (GE Xeleris).
For the estimation of tumor absorbed dose, the dose equation based on the medical internal radiation dose formalism (23, 24) is expressed next.

Here, τ is the residence time,
Finally, the residence times of source organs and tumors were entered in the adult female or male The International Commission on Radiological Protection (ICRP) 89 model for normal organs and the sphere model, respectively, that derived the organ absorbed doses, effective dose for each organ as per the ICRP 103 model, and whole-body effective dose, in terms of mSv/MBq. The time-activity graphs and effective half-lives (T e) of various organs and tumors were generated by using GraphPad Prism software (v9.1).
Blood dosimetry
Blood dosimetry was feasible only in three patients. One milliliter of venous blood sample was taken at 0.5 (prevoid), 3.5, 24, 48, 72, 96, 120, 144, and 168 hours after injection from each patient. The marrow dose was derived by using the method of Sgouros (25).
Follow-up
Safety evaluation, based on physical examination and laboratory testing including complete blood counts, kidney function tests, liver function tests, serum thyrotropin, thyroxine, and thyroglobulin (Tg) were determined every month. Patients were suggested to maintain a subject dairy to document the pain score and information on AE experienced and were reviewed on weekly basis. Interim [68Ga]Ga-DOTA.SA.FAPi PET/CT scans were performed six to eight weeks after the two to three cycles of [177Lu]Lu-DOTAGA.(SA.FAPi)2 therapy and evaluated by a single Nuclear Medicine physician.
Treatment response assessment
The study aimed at evaluating the preliminary efficacy and safety of [177Lu]Lu-DOTAGA.(SA.FAPi)2 therapy.
Primary outcome endpoint
The primary outcome endpoint was biochemical and functional imaging response assessment by serum Tg assay and [68Ga]Ga-DOTA.SA.FAPi PET/CT scans.
At the end of analysis on September 4, 2021, we classified the response of patient based on our clinic set criteria into complete response (CR), partial response (PR), persistent disease, and disease progression.
CR was defined as negative imaging, and either nsTg <0.1 or sTg <1 ng/mL with negative structural and functional imaging findings. PR was defined as continuous decreasing levels of nsTg or sTg with or concurrent decrease in the uptake values on PET/CT or structural imaging. An increase in the structural size or appearance of new lesions with a rising trend in the nsTg or sTg values was classified as disease progression.
Secondary outcome endpoints
Other clinical response assessment parameters involved visual analog score (26), analgesic score, global pain assessment (GPA) (27), ECOG performance status, and AE profile. Detailed definitions are mentioned in the Supplementary Data.
Safety assessment
Safety was assessed by dosimetry and AEs graded according to the National Cancer Institute's Common Terminology Criteria for Adverse Event (NCI-CTCAE) version 5.0. (28).
Statistical analysis
The data were examined for normality by using the D'Agostino–Pearson test. Paired sample t-test (parametric test) or Wilcoxon signed-rank test (nonparametric test) was executed to compare parameters at pre- and post-treatment time points. MedCalc statistical software version 12 was used for statistical analyses. p-Values ≤0.05 were considered significant.
Results
Fifteen RR-DTC patients (4 males and 11 females) with a mean age of 55 ± 9 years (range: 39–67) were recruited after demonstrating moderate to high uptake in [68Ga]Ga-DOTA.SA.FAPi PET/CT imaging, and all lesions were in consonance and exhibited comparable uptake with [18F]F-FDG PET/CT scans (Table 1). Subsequently, patients were administered [177Lu]Lu-DOTAGA.(SA.FAPi)2 therapy and PTx-WBS also revealed equivalent visual uptake in all the lesions corresponding to the [68Ga]Ga-DOTA.SA.FAPi and [18F]F-FDG PET/CT scans.
Comparison of Uptake Values Between Baseline [68Ga]Ga-DOTA.SA.FAPi and [18F]F-FDG Positron Emission Tomography/ Computed Tomography Scans
Table 2 summarizes the baseline demographic profile of the patients. All the patients had undergone a minimum of two lines of prior treatments. Out of 10 patients who underwent lenvatinib treatment, 8 demonstrated disease progression, and 2 patients discontinued lenvatinib due to treatment-related AEs. Although 3 (20%) patients were on morphine medications at the baseline, 66.6% (10/15) were on either atypical opioids, non-morphine opioids, or other non-steroidal anti-inflammatory drugs, and the remaining 2 patients did not encounter constant pain, and hence, were analgesic naive.
Demographic and Clinical Details of Patients
13-CRA, 13-cis-retenoic acid; CND, central neck dissection; CT, computed tomography; EBRT, external beam radiotherapy; FCT, follicular carcinoma of thyroid; FVPCT, Follicular variant papillary carcinoma of thyroid; MRND, modified radical neck dissection; PCT, papillary carcinoma thyroid; PD, progressive disease; PET, positron emission tomography; RAI, radioiodine; RR-DTC, radioiodine refractory differentiated thyroid cancer; Tg, thyroglobulin; TKI, tyrosine kinase inhibitor; TT, total thyroidectomy; Tx, therapy.
Before the initiation of [177Lu]Lu-DOTAGA.(SA.FAPi)2 treatment, all patients presented with distant metastases with skeletal metastases detected in 86.6% (13/15), lung nodules in 60% (9/15), and liver metastases in 26.6% (4/15).
Before treatment, nsTg levels were elevated along with abnormal [18F]-FDG and [68Ga]Ga-DOTA.SA.FAPi PET/CT scan findings in 12 patients. Interestingly, three patients had negligible Tg values (probably Tg “nonsecretor”), but on the contrary, demonstrated extensive disease on the PET/CT scans.
[177Lu]Lu-DOTAGA.(SA.FAPi)2 treatment cycles
A total of 45 cycles were administered in 15 patients, among whom 9 received 3 cycles each, 3 were treated with 4 cycles, and the remaining 3 received 2 cycles each. The mean cumulative activity administered was 8.2 ± 2.7 GBq (range 5.5–14 GBq) (221.6 ± 75 mCi; range 150–378 mCi) (Table 3).
[177Lu]Lu-DOTAGA.(SA.FAPi)2 Treatment Details and Outcomes
AS, analgesic score; NA, not assessed; PR, partial response; SD, stable disease; VAS, visual analog score.
Organ and tumor dosimetry
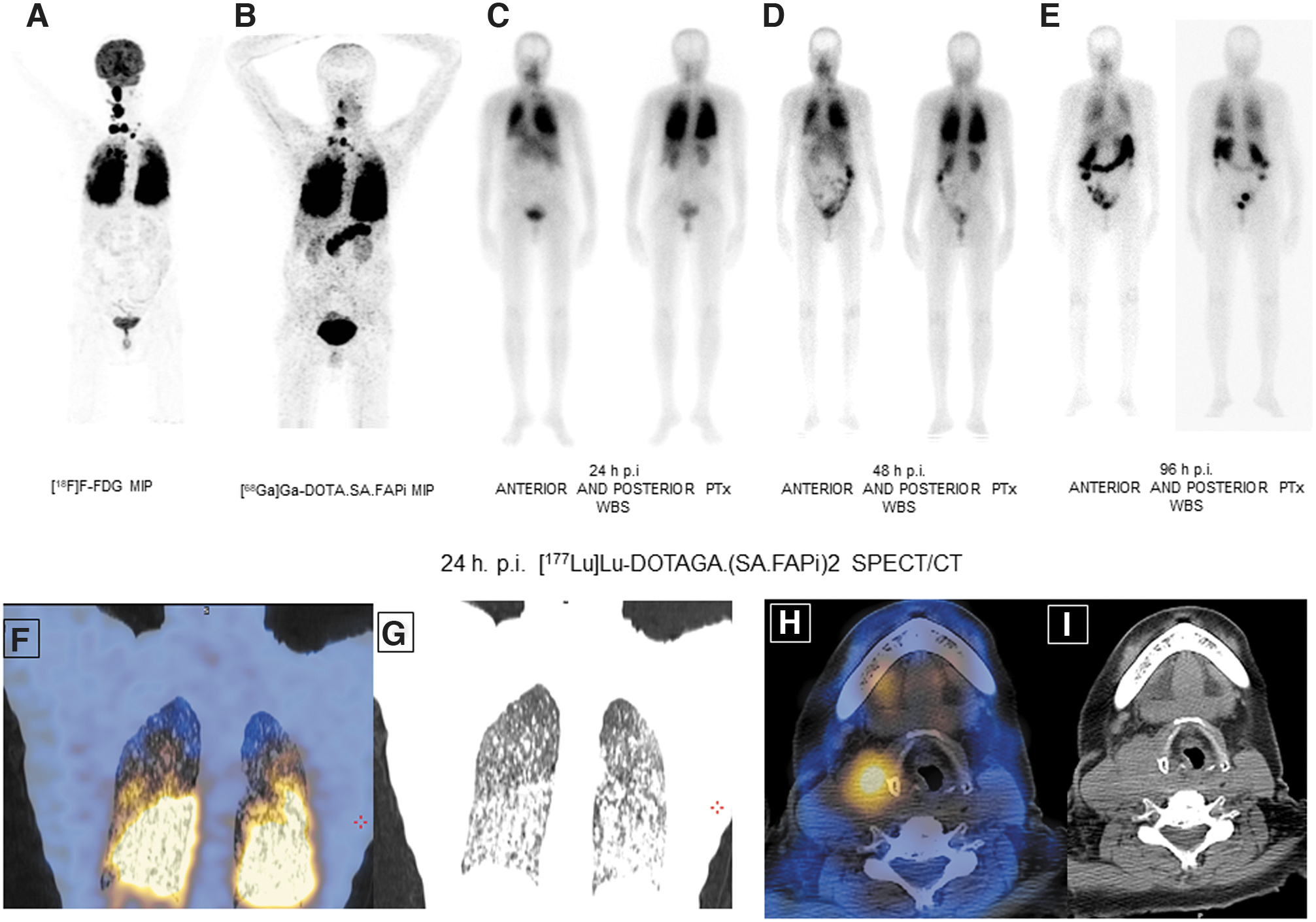
The mean organ and the tumor absorbed doses are enumerated in Tables 4 and 5. Physiological biodistribution of [177Lu]Lu-DOTAGA.(SA.FAPi)2 involved liver, gall bladder, colon, pancreas, kidneys, and urinary bladder contents, lacrimal glands, oral mucosa, and salivary glands (Figs. 2 and 3). The whole-body effective dose for [177Lu]Lu-DOTAGA.(SA.FAPi)2 was 1.62E-01 ± 1.53E-02. The highest organ radiation dose was observed for the colon (left colon: 1.97E+00 ± 1.68E-01 mSv/MBq, and right colon: 7.56E-01 ± 1.15E-01 mSv/MBq). Pancreas, gall bladder, kidneys, liver, and salivary glands received 7.20E-01 ± 6.41E-02, 7.09E-01 ± 1.12E-01, 3.02E-01 ± 2.86E-01, 2.11E-01 ± 3.24E-02, and 1.11E-01 ± 2.52E-03 mSv/MBq, respectively. [177Lu]Lu-DOTAGA.(SA.FAPi)2 had remarkably long/adequate median whole-body Te 88.06 hours (IQR: 86.6–99). The median absorbed doses to the tumor lesions were 1.08E+01 (IQR: 4.16E+00 to 8.97E+01) mSv/MBq per cycle.

A 50-year-old woman with a follicular variant of papillary carcinoma failed RAI therapy, Soranib and Lenvatinib. The patient had clinically progressive disease with Tg >3,00,000 ng/mL. Baseline [68Ga]Ga-
A 62-year-old female was diagnosed with papillary carcinoma of the thyroid in 2018, and she received >22.2 GBq of RAI treatment followed by sorafenib treatment. The patient had multiple neck lymph nodes and extensive lung metastases, which demonstrated intense FDG uptake (
Absorbed Dose and Effective Dose Estimate of [177Lu]Lu-DOTAGA.(SA.FAPi)2
All values are mentioned as mean ± standard deviation.
ICRP, The International Commission on Radiological Protection.
Effective Half-Life (T e) and Dosimetry Estimate of Tumor Lesions with [177Lu]Lu-DOTAGA.(SA.FAPi)2
Response assessment
Biochemical and functional imaging response
At the time of assessment (September 4, 2021), Tg levels had decreased in all patients with a significant decrease in the Tg levels before treatment (median Tg: baseline-10,549 ng/mL (IQR: 3066.5 to 39,450) versus at the time of assessment: 5649 ng/mL (IQR: 939.5–17,099), p = 0.0005).
No patients in the series demonstrated CR. A continuous decrease in the Tg levels indicating biochemical response was observed in all patients. Among the seven patients who underwent an interim [68Ga]Ga-DOTA.SA.FAPi PET/CT scan, two patients (no. 5 and 11) belonged to the non-secretory group and the scan findings were suggestive of PR and stable disease (SD), respectively. In the remaining five patients, three achieved both biochemical and molecular response (Table 3 and Fig. 2 and Supplementary Fig. S1), and two others observed a remarkable decrease in Tg levels but SD on molecular imaging assessment (Tables 3 and 6). One patient no. 3 with non-secreting Tg denied treatment after receiving two cycles, but on follow-up presented with clinical appearance of a new neck node, which was stony-hard on palpation with no symptoms of fever and was hence classified as clinically progressive disease. Patient 2 and 3 are alive, but they discontinued further treatment (Table 3).
Efficacy Assessment
Seven patients underwent an interim [68Ga]Ga-DOTA.SA.FAPi PET/CT scan.
Among them, 5 (a) belonged to the Tg secretor group and 2 (b) were from the Tg Non-secretor group.
Clinical disease progression.
SUV, standardized uptake value.
Clinical response assessment
The results of both VASmax and GPA response criteria were in complete concordance with CR in 23% (3/13), PR in 38.4% (5/13), minimal response in 30.7% (4/13), and no response in 1 patient (patient 2) with an overall response rate of 92% (Table 7).
Comparison of Visual Analog Score and Global Pain Assessment Response Criteria with Analgesic Scores
In two patients, pain score criteria were not assessed as they did not take any pain medications.
CR, complete response; GPA, global pain assessment criteria; MR, minimal response; NR, no response.
At a median follow-up of 7.2 months, there was a significant improvement in the VASmax scores [pre-therapy: 9 (IQR: 8–10) vs. follow-up: 6 (3 –6) (p-0.0001)], and ECOG performance status [3, (IQR: 2–3 vs. 2, (IQR: 2–3) (p-0.0078)]. In concordance with the VASmax and GPA scores, there was a decrease in the intake of analgesics in the respective response groups (Table 7).
Interestingly, the median time for the initiation of pain relief was 6 days (IQR: 6–10 days). Patient 1 initially experienced complete pain relief after the first cycle, but showed recurrence in pain after four weeks of the second cycle, and hence, analgesics were resumed. Among the 13 patients on analgesics (Table 3), all patients except 3 experienced pain relief after the first cycle of treatment, and the remaining three patients experienced relief after the second cycle. Only 1 patient (patient no. 2) experienced <20% decrease in the pain score from the baseline. Two patients, no. 12 and 15, experienced an initial flare in the pain after the first cycle, but both found relief after their second treatment cycle.
Safety and tolerability
None of the patients experienced grade III/IV hematological, renal, or hepatotoxicity from [177Lu]Lu-DOTAGA.(SA.FAPi)2 therapy (Table 8). No other treatment-related toxicities were observed. Grade 1 diarrhea occurred in 1 patient after each cycle of her treatment, which lasted up to 24 hours and was replenished by oral hydration solution. In three patients with Gr-I fatigue at the baseline a further increase in fatigue was observed, which lasted for up to three days post-treatment.
Laboratory Parameters at Baseline and Post-Treatment
ALP, alkaline phosphatase; CI, 95% confidence interval.
No patient in the series experienced any episodes of vomiting, nausea, or fluctuations in the vital parameters during and after [177Lu]Lu-DOTAGA.(SA.FAPi)2 therapy. In two skeletal metastases patients who reported a flare in the pain after treatment, the symptoms subsided approximately after one week of treatment cycle.
At the time of recruitment, six patients presented with G1 anemia, three patients presented with G2 anemia, and one patient had G1 thrombocytopenia that did not deteriorate with treatment. Interestingly, in 1 patient with pre-existing renal insufficiency, kidney function normalized after 6 weeks of first treatment where the creatinine values decreased gradually from 1.2 to 0.5 mg/dL. No grade hepatotoxicity was observed.
Discussion
The pivotal role of RAI for the management of distant metastases from DTC in the past eight decades, since its introduction in the early 1940s by Seidlin et al. (29), is unparallel in clinical oncology. The routine measurement of Tg and anti-Tg as tumor biomarkers, and generous use of ultrasonography, contrast enhanced CT/magnetic resonance imaging, and [18F]F-FDG PET/CT imaging in the surveillance of DTC patients have resulted in diagnosing a higher percentage of RR-DTCs than in the earlier times. However, the definition of RR-DTC is itself controversial. The ATA 2015 Guidelines have for the first time tried to define RR-DTC, but controversies in literature demand for further refinement of the definition of RR-DTC (30). However, three facts are non-controversial: (a) de novo absence of RAI uptake in metastatic sites, (b) loss of the ability by the metastatic deposits over time for taking up RAI, or (c) moderate to high uptake of RAI in metastases but demonstrable progressive disease on conventional/functional imaging.
It was initially difficult to manage these so-called RR-DTC patients without safe and effective systemic therapy options. In the past decade, two important drugs got FDA approvals following the multicentric phase-III randomized trials, namely DECISION trial (6) for sorafenib and SELECT trial (7) for lenvatinib.
The object response rate for sorafenib is about 12%, and for lenvatinib, it is significantly better, which is about 65% but is accompanied with a higher grade III/IV AEs. Moreover, in a certain cohort of patients, ∼25% even fail to respond to sorafenib/lenvatinib. The high percentage drug-related toxicities interfere with the course of treatment and lead to the early discontinuation of the drug (34/207; 16.4%) in patients on sorafenib and ∼37 out of 261 (14%) with lenvatinib. In the current study, although 7 out of 15 (46.6%) patients exhausted both sorafenib and lenvatinib, the remaining patients were treated with tyrosine kinase inhibitors (TKIs) at least once in their treatment tenure. Recently, a pivotal phase III COSMIC-311 trial (31) on cabozantinib in RR-DTC also revealed a promising progression-free survival that was not attained at the time of assessment, but at the same time significantly high grade III/IV toxicities in 57% patients and serious AEs in 16 patients were observed.
This large percentage of early dropout from the treatment regimen strongly supports the unmet need of additional highly targeted salvage treatment options in this subset of aggressive thyroid cancers. Currently, there are sparse options available for them to manage, and thus, there is an ongoing search for suitable, safe, and effective therapeutic options for these heavily pretreated RR-DTC patients who have progressed on TKIs. Research has also been ongoing and has proved 13-cis-retinoic acids (32) to be beneficial in the re-differentiation of RR-DTC, but further large-scale research is needed in each sub-category of RR-DTC patients as defined by ATA.
Recently, targeting FAP with various small-molecule FAPIs has gained momentum and extensive clinical research on its role in cancer therapeutics is ongoing. FAPI agents ([68Ga]Ga-DOTA-FAPI-02 and FAPI-04) for imaging are well established for a wide spectrum of cancers. However, a major challenge has remained on the therapeutic front pertaining to the early tumor washout and short tumor retention time, thereby delivering negligible tumor absorbed dose and, thus, limiting the therapeutic efficacy. For an effective radioligand therapy, it is critical that the biological half-life of pharmacophore must match the physical half-life of radionuclide to give best effective tumor half-life. Lutetium-177 is nick-named as “metallic iodine” with a physical half-life of 6.71 days and beta energy similar to 131I.
Our department in collaboration with the Department of Chemistry at Mainz, Germany also observed the same pattern of untimely tracer washout with one of the initially synthesized squaric acid linker-based molecules,
The favorable dosimetry data encouraged us to use [177Lu]Lu-DOTAGA.(SA.FAPi)2 for therapeutic use, and in an interest to know whether the findings hold true from the therapeutic clinical aspect, we therefore studied the efficacy and safety of [177Lu]Lu-DOTAGA.(SA.FAPi)2 in RR-DTC patients. From our findings in this study, the first-in-human application confirmed [177Lu]Lu-DOTAGA.(SA.FAPi)2 therapy safe for the treatment of heavily pretreated advanced stage RR-DTC patients.
In our study, all patients demonstrated a positive uptake on the [68Ga]Ga-DOTA.SA.FAPi PET/CT scan and [18F]F-FDG PET/CT scans. Similarly, the post-treatment serial biodistribution scan findings also corroborated with the PET/CT scan findings and additionally showed promising tumor retention even up to six days after treatment. Unlike our findings, initial results on [177Lu]Lu-FAPI-labeled compounds observed a rapid tumor washout and, hence, suggested the use of shorter half-life radionuclides such as Yttrium-90 with the FAPi molecule (33). However, Yttrium-90, attributing to its longer-range beta emission, might increase the risk of hematological toxicity. It is important to note that the present argument is based on only the physical characteristics of the radionuclide and this assumption can only be validated with longer follow-up high-evidence-based prospective studies.
Our study recognized a variation in the administration of treatment doses across the patients, which is apparently prevalent when investigating new radiopharmaceuticals where the biodistribution, pharmacokinetics, and dosimetry data are unknown. Although majority of the patients were administered with an average of 2 GBq per treatment cycle, in the later phases of recruitment, after we noted the treatment was safe from the clinical and dosimetry point of view, we escalated the dose to ∼4 GBq. Consistent with the dosimetry findings, the rate of hematologic AEs was minimal, transient and more importantly did not differ even in patients treated with higher doses.
Most remarkably, 1 patient (no. 7) with multiple extensive skeletal metastasis refractory to RAI, external beam radiotherapy, and lenvatinib demonstrated biochemical, molecular, and remarkable clinical responses after 2 cycles of [177Lu]Lu-DOTAGA.(SA.FAPi)2 therapy (median activity 50 mCi/cycle) (Fig. 2). In this patient, the dose has been further escalated to 4 GBq/cycle in the third and fourth cycle of treatment. The adequate effective-tumor half-life in this patient ranging between 48.6 and 89.5 hours reflects the promising response to treatment (Table 5, patient 7).
Our dose estimates suggest a mean 1.36 mSv/MBq to the colon, which is the critical organ. Hence, according to the maximum safe limit of radiation dose to the colon, which is 38 Gy as reported with external beam radiotherapy, a maximum tolerable cumulative dose of 29 GBq (780 mCi) can be administered safely.
The dose fractionation protocols and treatment intervals are yet to be studied based on the tumor burden, physiological radiotracer biodistribution, and transit aspects in the gut, which widely varies from patient to patient. Despite the fact that there is no evidence regarding the use of intervention, such as a high fatty food diet, and laxatives, to accelerate the excretion from liver–gall bladder and the administration of laxatives to hasten the intestinal motility, we incorporated a high fatty food diet and laxatives in patients for the first three days after the treatment. However, the effect of accelerating agents is not yet quantified and calls for a head-to-head dosimetry comparison between the intervention naïve and intervention groups. If the positive impact of intervention holds true, it can aid in lowering radiation dose to the liver and gut, provide a scope for administering larger cumulative doses of the radiotracer, and thereby achieve a better therapeutic effectiveness.
[177Lu]Lu-DOTAGA.(SA.FAPi)2 treatment induced clinical response, as indicated by a significant reduction in the pain scores and the intake of analgesics with a similar trend of biochemical response to treatment was observed.
To the best of our knowledge, this study is the first comprehensive investigation to evaluate preliminary therapeutic efficacy and safety of [177Lu]Lu-DOTAGA.(SA.FAPi)2 therapy in RR-DTC patients after exhaustion of all standard line treatment options, including sorafenib/lenvatinib. This pilot study has opened up a new avenue to be explored in the management of RR-DTC patients who have reached an end-of-the-road situation.
The major limitation of this study is the small patient number and the short follow-up duration. This was not a systematic dose-escalation study, and heterogenous activities were administered due to the unavailability of previous reports on the dosimetry of this radiotracer. However, the insights gained from this study may be of assistance to execute large-scale, prospective clinical trials in RR-DTC patients particularly, who have progressed on TKIs.
The initial results of [177Lu]Lu-DOTAGA.(SA.FAPi)2 therapy are encouraging, with significant biochemical and molecular responses. This pilot study demonstrated promising results of FAPI-based targeted therapy in the aggressive cohort of thyroid cancer patients.
Footnotes
Authors' Contributions
S.B. and M.P.Y.: conception, design, obtained ethical approval, acquisition, data collection, analysis interpretation, and article drafting and refinement. E.S.M., F.R.: molecule development, testing its in vitro pharmacokinetics, and standardization of radiolabeling. S.K.: dosimetry and PET/CT scan acquisition. S.A.: pathology review of the patients, article refinement. M.T., B.S.M., and A.T.: clinical data management, reviewing the PET/CT scans, and recruitment of patients. R.K.S.: referring patients to Nuclear Medicine, conception, and design. C.B.: design, conception, recruitment, clinical follow-up, follow-up with adverse events, analysis, article drafting, and final approval.
Employment
No recent (within the past five years), current, or anticipated employment by an organization that may gain or lose financially from publication of the article.
Ethical Statement
Ref. no. IECPG-22/2020 for the clinical use of [68Ga]Ga-DOTA.SA.FAPi, and Ref. no. IEC/1054/5/2020 for the clinical use of [177Lu]Lu-labeled FAPi radiotracers in various cancers.
Informed Consent
Written informed consent was obtained from all patients to participate in the study.
Disclaimer
The current work has not been submitted for review or is not under acceptance for publication in any journal.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
Supplementary Figure S1