
Abstract
Background:
To estimate the incident risk of surgical intervention for nasolacrimal duct obstruction after radioactive iodine (RAI) treatment and elucidate the high-risk group of patients with thyroid cancer (TC).
Methods:
This is a nationwide, population-based cohort study using data from the Korean National Health Claims database. Among the entire South Korean population aged between 20 and 80 years from 2007 to 2019, all patients with TC were included. Among all TC patients, a cohort was established by classifying it into the RAI and non-RAI groups according to whether RAI treatment was performed during the recruitment period. A log-rank analysis was used to evaluate the risk of nasolacrimal duct obstruction surgery in the RAI group compared with that in the non-RAI group. The Cox proportional hazards regression analysis was performed to calculate the adjusted hazard ratio (HR). The analysis was performed stratified by the age group, sex, frequency of RAI treatment, and cumulative dose of 131I.
Results:
Among 55,371 TC patients, who received RAI treatment, 515 (0.93%) underwent nasolacrimal duct obstruction surgeries, and among 56,950 TC patients, who did not receive RAI treatment, 72 (0.13%) underwent the surgeries. The average timing of incident nasolacrimal duct obstruction surgery was 3.8 ± 2.1 years after the first exposure to RAI. The incidence rate of nasolacrimal duct obstruction surgery was 104.04/100,000 person-years in the RAI group. There was a significantly higher risk of nasolacrimal duct obstruction surgery (HR 7.50 [confidence interval, CI: 5.86–9.60], p < 0.001) in the RAI group than in the non-RAI group. The risks significantly increased in the high-dose group (HR 14.15 [CI: 10.88–18.39]) and those younger than 50 years (HR 15.54 [CI: 9.76–24.72]).
Conclusion:
We quantified the risk of RAI-induced nasolacrimal duct obstruction surgery through a long-term follow-up of 9 years, which may contribute to estimating the general health care burden related to RAI treatment for TC patients in a practical setting. Great attention should be paid to its risk in patients younger than 50 years, especially in those treated with high doses.
Introduction
Radioactive iodine (131I, RAI) treatment has been commonly used as an important adjunct to eradicate microscopic cancer cells in the treatment of thyroid cancer (TC) (1). It has been widely applied as a therapeutic option because of its efficacy, tolerability, ease of application, and safety (2,3). The typical adverse effects of RAI treatment are generally well-tolerated.
Ophthalmic problems resulting from RAI treatment, including chronic conjunctivitis, dry eye syndrome, xerophthalmia, and lacrimal and salivary gland dysfunction, are reported to occur in 23% of patients (4 –6). Among these complications, epiphora and nasolacrimal duct obstructions have been noted later and are reported to vary from 2.2% to 18% (7 –11).
As tearing symptoms are not life-threatening and may take insidious onset after exposure to RAI treatment, lacrimal complications have been easily overlooked and potentially underestimated. However, it is important to assess the risk of development of nasolacrimal duct obstruction and provide proper information to patients undergoing RAI treatment because the symptoms mainly affect patients' quality of life and may require surgical intervention. Thus, the rate of occurrence and risk factors for RAI-induced nasolacrimal duct obstruction should be clarified. However, only a few case series have investigated the relationship between RAI treatment and nasolacrimal duct obstruction, and the underlying pathogenesis remains unclear.
Herein, we conducted a population-based cohort study focusing on patients undergoing RAI treatment for TC and surgeries for nasolacrimal duct obstruction based on ophthalmologist-confirmed medical information obtained from the mandatory universal health insurance system database in South Korea. We aimed to determine the incidence rate and quantify the risk of surgeries for nasolacrimal duct obstruction based on the demographic and treatment characteristics of the patients in the RAI group compared with those in the non-RAI group.
Materials and Methods
This nationwide cohort study was approved by the Institutional Review Board of Myongji Hospital, South Korea (IRB No. 2019-10-012), and adhered to the tenets of the Declaration of Helsinki. The requirement for informed consent was waived because of the censored nature of the data.
Data sources
We accessed health claims from 2007 to 2019 recorded via the Health Insurance Review and Assessment (HIRA) service of South Korea. This database has been used widely to identify novel determinants of other diseases, and detailed information about the HIRA database has been provided in previous studies (12,13). HIRA reviews all health claims in South Korea, including those submitted through the Korean National Health Insurance (NHI) scheme, which covers 97% of the South Korean population, and the other available medical assistance programs (the Medical Assistance Program and Medical Care for Patriots and Veterans Affairs Scheme), which cover the remaining 3% of the population. To define the population of South Korea, data from the Population and Housing Census conducted in 2021 (Korean Statistical Information Service; available at:
Participants and sample selection
All patients, who were identified as having TC (registration codes C73 and V193 based on the NHI diagnostic criteria) during the 13-year study period, were enrolled. V codes for carcinoma were obtained based on strict pathologic confirmation after biopsy or surgical removal. All enrollees with these codes were confirmed and registered by the clinicians. For patients with TC included in this study, data on the age, sex, medical visit records, date of diagnosis, and history of comorbidities from the HIRA database were collected.
Analyses
Establishing cohort data
Cohort data to evaluate the risk of nasolacrimal duct obstruction in TC patients who underwent RAI (HD071) were established. To eliminate preexisting nasolacrimal duct obstruction cases from enrollment, we set 2-year washout periods (2007–2008), similar to that in previous studies (12,13). To secure a sufficient period of follow-up, we used a fixed cohort design with an ample sample size, eliminating deviation from a short follow-up. We recruited all incidental TCs during the first 4 years (2009–2012), and they were enrolled in the established cohort.
To evaluate the risk of surgical intervention for nasolacrimal duct obstruction after exposure to RAI, we compared an RAI cohort with a non-RAI cohort. We assembled the RAI/non-RAI cohorts according to the exposure to RAI. We then excluded all patients with conditions that may affect the development of nasolacrimal duct obstruction, history of nasolacrimal duct obstruction (including both diagnosis and related tests), or history of TC or RAI during the washout periods.
Definition and ascertainment of primary outcome
To identify possible episodes of nasolacrimal duct obstruction, all study subjects were linked to outpatient and inpatient records using an encrypted personal identification key. Nasolacrimal duct obstruction was defined in two ways: (1) in patients undergoing surgical intervention comprising silicone tube intubation (S5520), external/endonasal dacryocystorhinostomy (S5525, S5540), conjunctivodacryocystorhinostomy (S5541), or endoscopic laser dacryocystorhinostomy (S5495); or (2) in patients undergoing specific examinations, including probing of the nasolacrimal duct (S5510) or dacryocystography (DCG).
To ensure that confounding conditions that could affect the occurrence of nasolacrimal duct obstruction were not included, all subjects who had any record of an injury of the eye/orbit (S05), connective tissue diseases such as granulomatosis with polyangiitis (GPA; M31), sarcoidosis (D86), or head (S0609), chronic sinusitis (J32), nasal polyp (J33), cancer of the nasal cavity, sinus (C30-31), or nasopharynx (C11-12), lysis of intranasal synechia (O0985), a history of atrophic rhinitis operation (O0980), extirpation of tumors of the nasal/paranasal sinuses (O0961-8), cauterization or nasal packing for epistaxis (O0991-4), removal of nasal cavity foreign body (O0971-2), incision of nasal furuncle (O0973), submucosal resection or septoplasty (O1001-3), or incision of nasal septal hematoma/abscess (O1004), external beam radiation therapy (HD110) were excluded.
Patients newly confirmed to undergo nasolacrimal duct obstruction surgery during the study period were included in the incidence estimates. For those who underwent nasolacrimal duct obstruction surgery, the development interval was defined as the duration between the first index date of RAI and the detection date of the defined nasolacrimal duct obstruction surgery. Among the outcomes, the group that underwent surgery once and the group that underwent two or more surgeries were additionally extracted, and the two groups were used for subanalysis. We censored the follow-up time at the end of this study (December 31, 2019).
All patients were categorized into 12 groups according to 6 age strata and 2 sexes. Among all subjects enrolled in the study group, the risk of nasolacrimal duct obstruction surgery was assessed by possible predictors, including age, sex, and the frequency and cumulative dose of RAI. The frequency of RAI was divided into two groups: one trial and two or more trials. The cumulative dose of RAI was divided into three groups based on the total usage of 131I before the index date of the nasolacrimal duct obstruction: “low” represented a 131I dose ≤30 mCi, “medium” for 30 mCi < 131I dose ≤150 mCi, and “high” for 131I dose >150 mCi. Because a low cumulative dose (≤30 mCi) is commonly used as a test dose to evaluate thyroid cancer and is also used to treat thyroid cancer, we included it in the analysis despite the low exposure.
These covariates were collected based on the diagnostic codes confirmed by physicians in the HIRA system and were used in a Cox proportional hazards analysis of the predictors of nasolacrimal duct obstruction surgery.
Statistics
Data handling and statistical analyses were performed by an independent data analyst (J.-Y.L.) specially trained by the HIRA institute for the HIRA big data (2017). A comparison of continuous variables between the groups was performed using the paired t-test, and a comparison of the proportion of each variable between the groups was analyzed using the chi-square test. The stratified log-rank test was used to compare the incidence rates of nasolacrimal duct obstruction surgery between the two groups. Cox proportional hazards regression was used to compute the adjusted hazard ratios (HRs) for the two groups. A stratified analysis was additionally performed according to sex (male, female) and age group (younger group: <50 years, older group: ≥50 years).
A confidence level of 95% was used for this analysis, and all results are presented as mean ± standard deviation. p-Value <0.05 indicated statistical significance. SAS Enterprise Guide version 6.1 software (SAS, Inc., Cary, NC) was used for all analyses.
Data availability
The raw data used in this study can be extracted by request from any qualified investigator through the national HIRA system.
Results
Demographics
After removing the cases with a history of exclusion conditions during the washout periods, a total of 339,221 subjects were newly diagnosed with TC between January 2007 and December 2019 (Fig. 1). Among those subjects, 19,257 subjects were excluded for history of RAI or nasolacrimal duct obstruction during the washout period, and 319,963 subjects with TC were extracted from the eligible cohort. During the enrollment period (2009–2012), 112,321 subjects comprising 18,860 (16.8%) males and 93,461 (83.2%) females were finally included. A total of 55,371 subjects who underwent RAI treatment were included in the RAI cohort, and 56,950 subjects without RAI treatment were included in the non-RAI cohort. The detailed information is presented in Table 1.

The process of identifying those who underwent radioactive iodine therapy for thyroid cancer treatment in the entire South Korean population.
Demographics of Study Groups According to the Exposure of Radioactive Iodine Therapy in Patients with Thyroid Cancer in an Established Cohort in South Korea
Paired t test.
Chi-square test.
Diagnostic procedures included DCG and probing.
DCG, dacryocystography; NLDO, nasolacrimal duct obstruction; RAI, radioactive iodine therapy; SD, standard deviation.
Risk prediction of surgical intervention for nasolacrimal duct obstruction in the RAI cohort
Incident cases of nasolacrimal duct obstruction surgery were observed in 515 (0.93%) patients in the RAI group and 72 (0.13%) cases in the non-RAI group (Table 2). The mean age for undergoing surgery for nasolacrimal duct obstruction was 48.9 ± 10.9 years in the RAI group and 56.9 ± 9.7 years in the non-RAI group, with a significant difference (p < 0.001). The incidence rate of nasolacrimal duct obstruction surgery was 104.04/100,000 person-years in the RAI group and 14.31/100,000 person-years in the non-RAI group. The total cumulative incidence rate of surgical intervention for nasolacrimal duct obstruction was significantly higher in the RAI group than in the non-RAI group (p < 0.001).
The Effect of Radioactive Iodine Therapy on the Risk of Surgical Intervention for Nasolacrimal Duct Obstruction Based on the Frequency and Cumulative Dose of 13 1I
Adjusted for age and sex.
The cumulative dose was divided into three groups: “low” meant 131I dose ≤30 mCi, “medium” meant 30 < 131I dose ≤150 mCi, and “high” meant 150 mCi < 131I dose.
CI, confidence interval; HR, hazard ratio.
In a multivariate Cox regression analysis, the risk of diagnostic examinations (DCG, probing) and surgery for nasolacrimal duct obstruction among all subjects who underwent RAI treatment was 4.26 times [confidence interval, CI: 3.66–4.95] higher than that of subjects who did not undergo RAI treatment. The risk of surgical intervention for nasolacrimal duct obstruction among all subjects who underwent RAI treatment was 7.50 times [CI: 5.86–9.60] higher than that of subjects who did not undergo RAI treatment. The risk was 7.38 times [CI: 5.74–9.49] higher in those who received RAI treatment once and 7.90 times [CI: 5.92–10.54] higher in those who received multiple RAI treatments.
In the high-dose group (>150 mCi 131I dose), the risk increased 14.15 times ([CI: 10.88–18.39]; all p < 0.001). The mean follow-up period was 8.9 ± 1.1 years. The mean interval between the first exposure of RAI and incident surgical intervention for nasolacrimal duct obstruction was 3.8 ± 2.1 years (range, 0.3–10.4 years).
Risk prediction of surgical intervention for nasolacrimal duct obstruction: stratified by sex and age group
In the male population, the risk of nasolacrimal duct obstruction surgery in the RAI group was 7.26 times [CI: 2.55–20.68] higher than that in the non-RAI group (p < 0.001) (Supplementary Table S1). In the female population, the risk of nasolacrimal duct obstruction surgery in the RAI group was 7.54 times [CI: 5.85–9.72] higher than that in the non-RAI group (p < 0.001). The mean age of development of nasolacrimal duct obstruction was 52.4 ± 14.0 years in the male population, and 49.8 ± 10.9 years in the female population.
In the stratified data divided by the age of 50, the risk of nasolacrimal duct obstruction surgery in the RAI group was 15.54 times [CI: 9.76–24.72] * higher in the younger group, and 4.58 times [CI: 3.40–6.18] higher in the older group (all p < 0.001) (Fig. 2). In the high-dose group of RAI, the risk remarkably increased in the younger group (HR 31.02 [CI: 19.23–50.04]) than in the older group (HR 8.05 [CI: 5.77–11.23]).
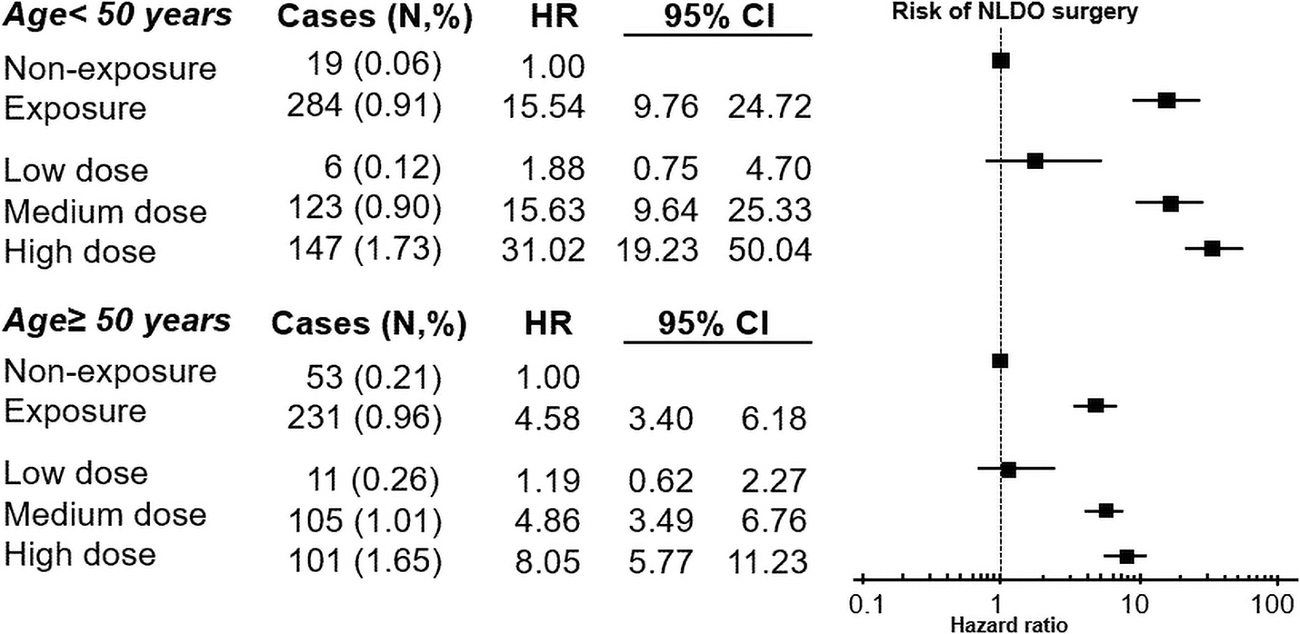
Forest plot presenting a risk prediction of surgical intervention for nasolacrimal duct obstruction according to the two age groups.
Subanalysis for primary outcomes: single surgery versus multiple surgeries
In our subanalysis, statistical comparison was performed between the group that underwent surgery once and the group that underwent two or more surgeries for nasolacrimal duct obstruction (Supplementary Table S2). In the RAI group, 437 (84.8%) patients underwent surgery for nasolacrimal duct obstruction and 78 (15.2%) underwent two or more surgeries for nasolacrimal duct obstruction compared with the non-RAI group (HR 1.29 [CI: 0.66–2.54]; p = 0.456). The frequency of RAI treatment and cumulative dose of 131I did not significantly increase the risk of multiple surgeries for nasolacrimal duct obstruction (p = 0.627 and 0.660, respectively).
Discussion
We found that ∼1% of TC patients, who underwent RAI treatment, were at a risk of undergoing surgeries for nasolacrimal duct obstruction, which was in contrast to 0.13% of the patients, who did not undergo RAI treatment. The risk of nasolacrimal duct obstruction surgery was 31 times higher in the younger age group and up to 8 times higher in the older age group, showing a remarkably high value in the younger age group. In particular, the risk was predicted to be more than 10 times higher in the high cumulative dose group.
RAI treatment can precipitate lacrimal gland dysfunction and increase the risk of nasolacrimal duct obstruction at the same time. Therefore, the incidence of nasolacrimal duct obstruction alone caused by RAI treatment cannot predict the health care burden for TC patients or represent the surgical risk of TC patients with nasolacrimal duct obstruction due to the influence of dry eyes on the surgical decision for nasolacrimal duct obstruction. This study has the strength to show a surgical risk in TC patients with nasolacrimal duct obstruction in a real practice setting.
There were a few previous studies to report this complication of the lacrimal drainage system, and the incidence has differed depending on the study periods or definition of nasolacrimal duct obstruction (Table 3) (7,9 –11,14,15). Kloos et al. presented 10 epiphora patients (3%) out of the total RAI-treated patients, which appeared 6.5 months after the last RAI exposure (16). Other researchers demonstrated 18% of RAI-induced nasolacrimal duct obstruction cases using dacryoscintigraphy regardless of ocular symptoms (15). In a comparative study conducted by da Fonseca et al., there was no significant difference in the frequency of lacrimal drainage system obstruction within a year after the RAI treatment between the study and control groups (17). In their study, a year was used for symptom development duration, which seemed to be too short to elucidate the occurrence of nasolacrimal duct obstruction as sequelae. In our study, using a long-term follow-up of 9 years, the average interval between the first exposure of RAI and surgery for nasolacrimal duct obstruction was 3.8 years. Most of the previous studies were limited to small case series, an unclear definition of nasolacrimal duct obstruction, relatively short follow-up periods, and scarce statistical analysis; therefore, we focused on a clear definition of nasolacrimal duct obstruction using surgical interventions, established a nationwide cohort with long follow-up periods, and statistically predicted a quantified risk of nasolacrimal duct obstruction surgery based on the exposure, frequency, or cumulative dose of RAI.
Literature Review of the Nasolacrimal Duct Obstruction As a Complication After Radioactive Iodine Treatment
Mean cumulative dose of usage of RAI.
Mean interval between the exposure of RAI and lacrimal symptoms or diagnosis.
Mean follow-up periods after the exposure of RAI treatment.
Epiphora.
Conversion of 11.9 GBq to mCi.
Present nasal tissue localization to possibly explain the nasolacrimal duct toxicity.
CT, computed tomography; DCR, dacryocystorhinostomy; Dx, diagnosis (through diagnostic modalities); FDDT, fluorescein dye disappearance test; SPECT, single-photon emission computed tomography; Tx, treatment (through surgical intervention).
Despite the unclear pathophysiology, there are some plausible explanations for the relationship between RAI exposure and lacrimal drainage system obstruction. Base on literature in radiotherapy, † the suggested mechanism is the direct uptake of iodine in the nasolacrimal duct mucosa via the vector of sodium (Na+)/iodide (I) symporter, which is expressed in the stratified columnar epithelial cells of the nasolacrimal duct and lacrimal sac (18,19). Uptake of iodine can induce luminal inflammation of the nasolacrimal duct, leading to eventual fibrosis, which is supported by our findings.
In addition, Ali et al. reported a high nasal localization rate of RAI in patients treated with a high dose (≥150 mCi) using whole-body nuclear scintigraphy and suggested that this finding might be a risk factor for nasolacrimal duct obstruction (14). We observed a possible dose/response relationship between cumulative dose and risk of nasolacrimal duct obstruction surgery. Nasolacrimal duct obstruction was reported to be common in patients with the 131I dose >150 mCi (7,15), whereas few other studies have reported that doses <150 mCi led to lacrimal drainage system obstruction or lacrimal gland dysfunction (20 –22). In the current study, the risk of nasolacrimal duct obstruction surgery drastically increased in cases treated with a cumulative dosage of 30 mCi. Since almost all therapeutic doses of RAI exceed 30 mCi, the risk of nasolacrimal duct obstruction surgery cannot be overlooked even in patients treated with low doses.
Generally, primary acquired nasolacrimal duct obstruction frequently affects older adults and females more than younger adults or males. A previous study reported that age >45 years and female sex are considered to be risk factors for the development of RAI-induced nasolacrimal duct obstruction (7). Unlike these general risk factors, the present study showed a similar high risk of nasolacrimal duct obstruction surgery between sexes, and a much higher risk of nasolacrimal duct obstruction surgery in the RAI group of young age (<50 years). Moreover, the patients with the mean age at which nasolacrimal duct obstruction surgery was performed were ∼2.6 years younger in the RAI group than in the non-RAI group.
Although the incidence rate of RAI-induced nasolacrimal duct obstruction surgery is similar or slightly higher in younger patients than in older patients, the risk would be relatively much higher in younger patients because the incidence of primary acquired nasolacrimal duct obstruction is rare in the general young population. In a few previous studies, Teng et al. reported that in patients with thyroid cancer, the younger age group (20–39 years) had a higher risk of second primary malignancy after RAI therapy (particularly over 150 mCi) (23). In addition, the risk of radiation-induced oral mucositis was reported to be higher in younger patients (24).
Based on the results of previous studies that reported a higher risk of complications in the younger age group, more active inflammatory reactions in the younger age group may have led to more severe obstruction of the nasolacrimal duct in our study. Moreover, it is also postulated that the younger age group may feel more discomfort even with milder symptoms compared with the older age group, leading to a higher frequency of surgery. In turn, based on our findings that males and females had a similar risk of RAI-induced nasolacrimal duct obstruction surgery, the risk should be evaluated carefully in males as in females after RAI treatment, and particular attention should be paid to the development of RAI-induced nasolacrimal duct obstruction in adults younger than 50 years.
This study had several limitations. First, the incidence of nasolacrimal duct obstruction could not be assessed in this study model because only patients who had undergone diagnostic tests or surgical treatments for nasolacrimal duct obstruction were included. Second, we could not determine whether the surgery for nasolacrimal duct obstruction was unilateral or bilateral. When the frequency of the surgery was analyzed, we could not clarify whether the same eye was operated twice or if each eye underwent the surgery subsequently. We assumed that the frequency of surgery itself is meaningful since the repetition of the same type of surgery could have an impact on the health status of the patients.
Third, anthropometric measurements or information on the menopausal status could not be obtained from the HIRA database. Although it was difficult to determine the menopausal status of patients from our study data, it could be controlled by comparing the RAI-treated group with the control group of similar age strata to avoid its influence. At last, although the cumulative dosage and frequency were available, data regarding individual doses and localization of RAI uptake seen on patients' post-therapy scans were not available in our study. Since the therapeutic effect by the degree of RAI uptake can vary depending on whether RAI was administered under a withdrawal or recombinant human thyrotropin (TSH) protocol, the degree of TSH elevation, or the degree of iodine depletion, these factors could potentially be important for inducing nasolacrimal duct obstruction. This needs to be further evaluated in future studies.
However, in Korea, patients are educated to follow a strict low-iodine diet by specially trained dieticians and TSH and urinary iodine concentration levels are measured before administration of RAI, and therefore, most patients are expected to have appropriate TSH levels and iodine depletion state (25). It would also be helpful to correlate or stratify results with the amount and location of RAI uptake seen on patients' post-therapy scans.
The strengths of our study include its large sample size, cohort design, strictly defined RAI treatment, and quantified assessment of surgical risk for nasolacrimal duct obstruction based on detailed information of RAI treatment. In addition, we provided age- and sex-specific risk prediction with novel evidence that can be directly applied in clinical settings.
In conclusion, we demonstrated highly predictive factors and the expected timing of nasolacrimal duct obstruction surgery after exposure to RAI in TC patients. Based on our results, patients younger than 50 years, and those who undergo multiple sessions of RAI or particularly high-dose treatments should be recommended to follow up for the development of nasolacrimal duct obstruction for at least 4 years. From a prevention perspective, early intervention, such as relatively less invasive tests or procedures for tearing symptoms, early use of anti-inflammatory eye drops, and regular ophthalmologic examination, may be helpful to prevent or detect the earliest stage of this complication.
Footnotes
Acknowledgments
Nuclear medicine consultation: Narae Lee, MD, Department of Nuclear Medicine, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Republic of Korea. Internal medicine consultation: Seo Young Sohn, MD, Division of Endocrinology, Department of Medicine Hanyang University College of Medicine, Myongji Hospital, Goyang, Republic of Korea.
Authors' Contributions
J.-Y.L. and K.I.W. designed the study. J.-Y.L. conducted the study, analyzed and interpreted the data, and drafted the article. K.I.W. interpreted the data, revised the article, and approved the final version of the article.
Author Disclosure Statement
All the authors have no conflicting relationship and report no disclosure.
Funding Information
This work was supported by the faculty grant of Myongji Hospital (1902-09-01) and the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT; 2020R1F1A1072264). The sponsor or funding organization had no role in the design or conduct of this research.
Supplementary Material
Supplementary Table S1
Supplementary Table S2