
Abstract
Background:
Follicular thyroid carcinoma (FTC) and Hurthle cell carcinoma (HCC) are rare and aggressive thyroid cancers with limited published data comparing their outcomes or regarding their subtypes. The aim of this study was to describe clinicopathological features and compare clinical outcomes of patients with FTC and HCC based on the 2017 World Health Organization definition and extent of vascular invasion (VI).
Methods:
We retrospectively studied 190 patients with HCC and FTC primarily treated with surgery at Memorial Sloan Kettering Cancer Center between 1986 and 2015. Patients were classified as minimally invasive (MI), encapsulated angioinvasive with focal VI (EA-FVI), encapsulated angioinvasive with extensive VI (EA-EVI), and as widely invasive (WI). To compare clinical outcomes, patients were grouped as follows: group 1 = FTC-MI and FTC EA-FVI, group 2 = FTC EA-EVI and FTC-WI, group 3 = HCC-MI and HCC EA-FVI, group 4 = HCC EA-EVI and HCC-WI. Outcomes of interest were overall survival (OS), disease-specific survival (DSS), recurrence-free survival (RFS), locoregional recurrence-free survival (LRRFS), and distant recurrence-free survival (DRFS). Outcomes were determined using the Kaplan–Meier method and compared with log-rank test.
Results:
Patients with HCC (n = 111) were more likely to be older than 55 years old (59% vs. 27%, p < 0.001) with a tendency to present with more extensive VI (33% vs. 19%, p = 0.07) compared with FTC (n = 79). Comparing groups 1, 2, 3, and 4, group 4 patients were more likely to recur (DFS 98%, 93%, 98% vs. 73%, respectively, p = 0.0069). There was no statistically significant difference in OS, DSS LRRFS, or DRFS. Stratified by extent of VI (no, focal, and extensive VI), patients with extensive VI were more likely to recur (RFS 100%, 95%, 77%, p = 0.0025) and had poorer distant control (DRFS: 100%, 95%, 80%, p = 0.022), compared with patients absent or focal VI.
Conclusions:
Accurate assessment of the extent of VI and tumor phenotype (follicular vs. Hurthle) are essential in identifying patients at higher risk of recurrence.
Introduction
Follicular thyroid carcinoma (FTC) and Hurthle cell carcinoma (HCC) are rare subtypes of well-differentiated thyroid cancer, comprising ∼10% (1) and 5% (2,3) of all well-differentiated thyroid cancers. Since 2017, HCC is classified by the World Health Organization (WHO) as a separate entity, instead of oncocytic variant of FTC (4). This change was largely a result of the recent genomic research demonstrating the differences between HCC and FTC (5 –8). The current classification also categorizes FTC into minimally invasive (MI), encapsulated angioinvasive (EA), and widely invasive (WI). Although this classification is not mentioned in the Hurthle cell chapter of the WHO, most pathologists use these subcategories for HCC as well as FTC.
While there is agreement that MI HCC and FTC are much more indolent tumors compared with their EA and WI counterparts, controversy persists regarding the impact of the extent of angioinvasion. Furthermore, there is still no universal agreement regarding which tumor is more aggressive. Some studies report no difference in outcomes between HCC and FTC (9), while others consider HCC more aggressive (10). There is therefore a need to better understand the prognostic impact of the extent of vascular invasion (VI) and compare the behavior of FTC and HCC.
This study aims to report the clinicopathological characteristics and compare the outcomes of patients with FTC and HCC classified into subtypes and stratified by extent of angioinvasion (4).
Materials and Methods
For this retrospective study, we obtained Institutional Review Board approval and a waiver of informed consent from Memorial Sloan Kettering Cancer Center (MSK). From an institutional database of 6259 patients with well-differentiated thyroid carcinoma primarily treated with surgery at MSK between 1986 and 2015, 190 patients with FTC and HCC were included. Poorly differentiated carcinomas, as defined by presence of tumor necrosis and/or a mitotic count of 1–4 mitosis per 10 high-power fields (corresponding to 2.4 mm2), were not included in this study. Patients with no available slides for review were excluded. Slides were reviewed by head and neck pathologists, blinded to patient outcomes.
Within the study cohort, 114 (61%) tumors were submitted entirely for histologic examination; 45 (24%) had their tumor capsule submitted entirely; whereas the remaining 29 (16%) were representatively sampled with a median of 7 tumor blocks examined histologically per tumor (range: 5–28). Therefore, the thyroid tumors are overall well-sampled at our center. The presence of VI was noted only when such foci were present within or beyond the capsule in accordance with criteria outlined by the current WHO classification (4). In brief, only when the invasive focus protruded into the lumen of the vessel in a polypoid manner covered by endothelial cells, or when it was attached to the vessel wall or associated with thrombus formation was considered true VI. Areas of VI that were closely adjacent to one another were counted as separate foci.
Each tumor was classified into FTC or HCC followed by their subtypes, using a modification of the 2017 WHO classification, stratifying the tumors into four groups (4). In accordance with most pathologists' criteria, a lesion was considered as HCC only when >75% of the tumor was composed of oncocytic cells. If fewer oncocytic cells were present, it was considered as thyroid neoplasm with oncocytic cell features, and was therefore not included in this cohort (4). Patients with encapsulated lesion with capsular invasion only were classified as MI. Patients with encapsulated lesion, regardless of the capsular invasion status, and presence of VI were classified into two groups, according to the number of VI foci identified: EA with focal VI (EA-FVI) if <4 foci; EA with extensive VI (EA-EVI) if 4 or more foci. Finally, patients with partial or absent capsule grossly involving the thyroid and presenting with extensive angioinvasion were classified as WI. Figure 1 illustrates the pathological features that categorize these tumors into their different subtypes.

MI, encapsulated angioinvasive, and WI carcinoma. (
Clinical and pathological characteristics of HCC and FTC as well as those of the subtypes of HCC and of FTC were described. To compare baseline characteristics, we used the chi-square test or Fisher's exact test for categorical variables and Mann–Whitney U-test for continuous variables.
To analyze the clinical outcomes, patients were categorized into four groups: group 1 = FTC-MI and FTC EA-FVI, group 2 = FTC EA-EVI and FTC-WI, group 3 = HCC-MI and HCC EA-FVI, and group 4 = HCC EA-EVI and HCC-WI. Outcomes were determined using the Kaplan–Meier method and compared using the log-rank test. The clinical outcomes of interest were overall survival (OS), disease-specific survival (DSS), recurrence-free survival (RFS), locoregional recurrence-free survival (LRRFS), and distant recurrence-free survival (DRFS). OS was calculated from date of initial surgery until the date of last contact or death. DSS was calculated from surgery date to the date of last follow-up with the institution's disease management team (DMT) or death with disease. For RFS, the follow-up interval was calculated from surgery date to the date of last DMT appointment or first recurrence. Statistical analysis was performed using R (version 3.6.2; R Foundation for Statistical Computing). All tests were two tailed. A value of p < 0.05 was determined to be statistically significant.
Results
Comparison of patient and tumor characteristics of HCC and FTC
Patient characteristics stratified by histology are given in Table 1. There were 111 patients with HCC and 79 patients with FTC. A greater percentage of patients with HCC were older than 55 years of age (59% vs. 27%, p < 0.001) compared with FTC patients. There were no statistically significant differences in sex, stage, median tumor size, tumor size in categories (≤4 cm or >4 cm), extrathyroidal extension (ETE), and VI between the two groups.
Clinical and Tumor Characteristics by Histology
Data are presented as number (percentage) of patients unless otherwise indicated. Percentages have been rounded and may not total to 100.
ETE, extrathyroidal extension; FTC, follicular thyroid carcinoma; HCC, Hurthle cell carcinoma; IQR, interquartile range; pN, pathological nodal; pT, pathological tumor; VI, vascular invasion.
Description of patient and tumor characteristics of HCC and FTC subtypes
Patient and tumor characteristics of HCC and FTC stratified by subtypes are given in Table 2. Of 79 patients with FTC, there were 40 FTC-MI, 38 FTC EA-FVI, and 1 FTC-WI. In FTC groups, the majority of patients were younger than 55 years of age, had T1/T2 tumors with no ETE.
Clinical and Tumor Characteristics by Histological Subtype
Data are presented as number (percentage) of patients unless otherwise indicated. Percentages have been rounded and may not total to 100.
EA, encapsulated angioinvasive; MI, minimally invasive; WI, widely invasive.
Of 111 HCC patients, there were 42 HCC-MI, 61 HCC EA, and 8 HCC-WI. In all groups, most patients were older than 55 years, with no ETE or identified neck metastasis. In the first two groups, most patients were women and had T1/T2 tumors. In the HCC-WI subgroup, the majority of patients had extensive VI (87%).
Our entire cohort had a median follow-up of 82 months (interquartile range [IQR], 35–125) and a median survival of 83 months (IQR, 39–128).
Treatment and outcome of FTC subtypes
Treatment of FTC subtypes is given in Figure 2 and outcome in Table 3. In the FTC MI subgroup (n = 40), 23 patients (57%) were treated by total thyroidectomy with 1 patient (2%) having two-stage total thyroidectomy, meaning a thyroid lobectomy followed by completion thyroidectomy within 1 year of the first surgery. Only 1 patient (2%) required additional neck dissection. Ten patients (25%) received radioactive iodine (RAI). No recurrences were identified in the follow-up period and there were 2 deaths (5%) unrelated to the disease.
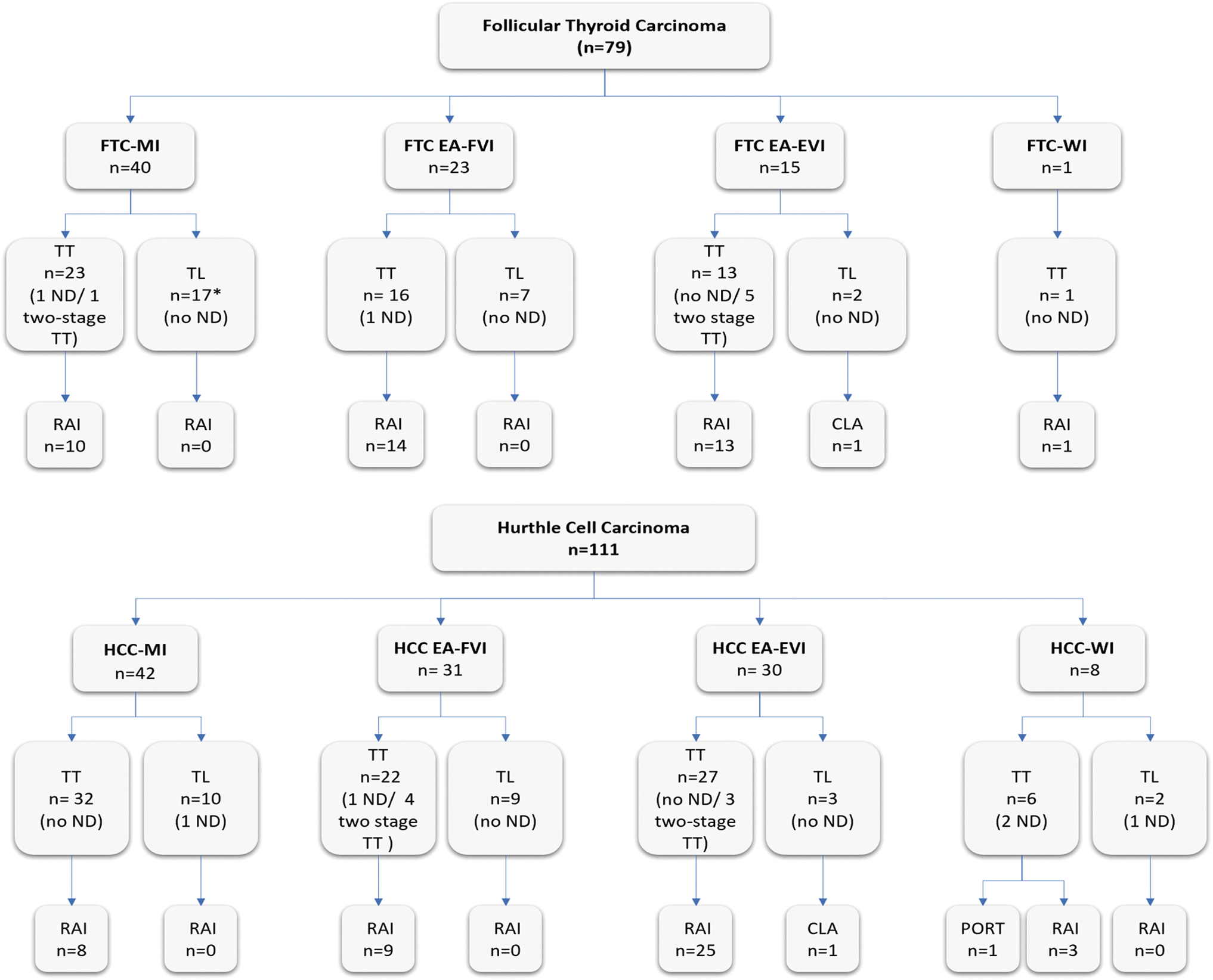
Flow diagrams of the treatment received for follicular cell carcinoma and HCC patients. *Two patients had isthmusectomy. CLA, contralateral lobe ablation; EA-EVI, encapsulated angioinvasive with extensive vascular invasion; EA-FVI, encapsulated angioinvasive with focal vascular invasion; FTC, follicular thyroid carcinoma; ND, neck dissection; PORT, postoperative radiotherapy; RAI, radioactive iodine; TL, thyroid lobectomy; TT, total thyroidectomy.
Outcomes Stratified by Histological Subgroups
EA-EVI, encapsulated angioinvasive with extensive vascular invasion; EA-FVI, encapsulated angioinvasive with focal vascular invasion; M1, distant metastasis.
In the FTC EA-FVI subgroup (n = 23), 16 patients (70%) were treated by total thyroidectomy, 1 (4%) with additional neck dissection, and 14 patients (61%) received RAI. There was 1 distant recurrence (4%) and 1 death unrelated to the disease.
In the FTC EA-EVI subgroup (n = 15), 13 patients (87%) were treated by total thyroidectomy, 5 (33%) by two-stage total thyroidectomy. Thirteen (87%) patients received RAI. No patient had neck dissection. One patient (7%) had distant metastasis at presentation, received a thyroid lobectomy followed by contralateral lobe ablation (CLA) owing to comorbidities and died of the disease. One patient developed distant metastasis during follow-up. There were no deaths unrelated to the disease.
In the FTC-WI subgroup (n = 1), only one patient was treated with total thyroidectomy and RAI. That patient was alive with no evidence of disease at last DMT follow-up.
Treatment and outcome of HCC subtypes
Treatment of HCC subtypes are given in Figure 2 and outcome in Table 3. In the HCC-MI (n = 42) subgroup, 32 patients (76%) were treated with total thyroidectomy. No patient had neck dissection. Eight patients (19%) received RAI. One patient (2%) had distant metastasis at presentation and died of the disease. Nine patients (21%) died of other causes.
In the HCC EA-FVI subgroup (n = 31), 22 patients (71%) were treated with total thyroidectomy and 4 (13%) with two-stage total thyroidectomy. One patient (3%) required additional neck dissection, and 9 patients (29%) received RAI. One patient (3%) had locoregional and distant recurrence and died of the disease. Four patients (13%) died of causes unrelated to the disease.
In the HCC EA-EVI subgroup (n = 30), 27 patients (90%) were treated with total thyroidectomy, 3 (10%) with two-stage total thyroidectomy, and 25 patients (83%) received RAI. One patient was treated with thyroid lobectomy followed by CLA owing to comorbidities and was alive without metastasis at the last assessment. Of the 4 patients (13%) who died of the disease, 2 patients (7%) had distant metastasis at presentation, 1 patient (3%) had a locoregional and distant metastasis, and 1 patient had only distant metastasis. Three other patients (10%) developed recurrences (one locoregional, one regional, and one distant) and were alive at the last assessment. Two patients died of other causes.
In the HCC-WI subgroup (n = 8), 6 patients (75%) were treated with total thyroidectomy, 2 patients (25%) required additional neck dissection. Three patients (37%) received RAI and 1 patient (12%) received postoperative radiotherapy. One patient had distant metastasis at presentation. One patient developed distant metastasis. There were 2 deaths (25%) unrelated to the disease.
Outcomes analysis stratified by group
To perform a statistical analysis, patients were categorized into four groups: group 1 = FTC-MI and FTC EA-FVI, group 2 = FTC EA-EVI and FTC-WI, group 3 = HCC-MI and HCC EA-FVI, group 4 = HCC EA-EVI and HCC-WI.
The median OS time for the entire cohort was 84 months (IQR, 39–128). OS probability at 120 months for groups 1, 2, 3, and 4 were, respectively, 96%, 90%, 87%, and 70%, with p = 0.045 (Fig. 3A). The median DSS time was 64 months (IQR 31–107). DSS probability at 120 months were 100%, 86%, 96%, and 77%, with p = 0.085 (Fig. 3B). The median RFS time was 60 months (IQR, 36–95). RFS probability at 120 months showed a significant difference between groups 1, 2, 3 and 4, with group 4 having the worst RFS (97%, 92%, 98%, and 73%, p = 0.0069) (Fig. 3C). The median DRFS time was 62 months (IQR, 33–103). DRFS probability at 120 months were 98%, 93%, 98%, and 78%, with p = 0.096 (Fig. 3D). The median LRRFS time was 64 months (IQR, 29–104). LRRFS probability at 120 months were 100%, 100%, 98%, and 94%, with p = 0.29.
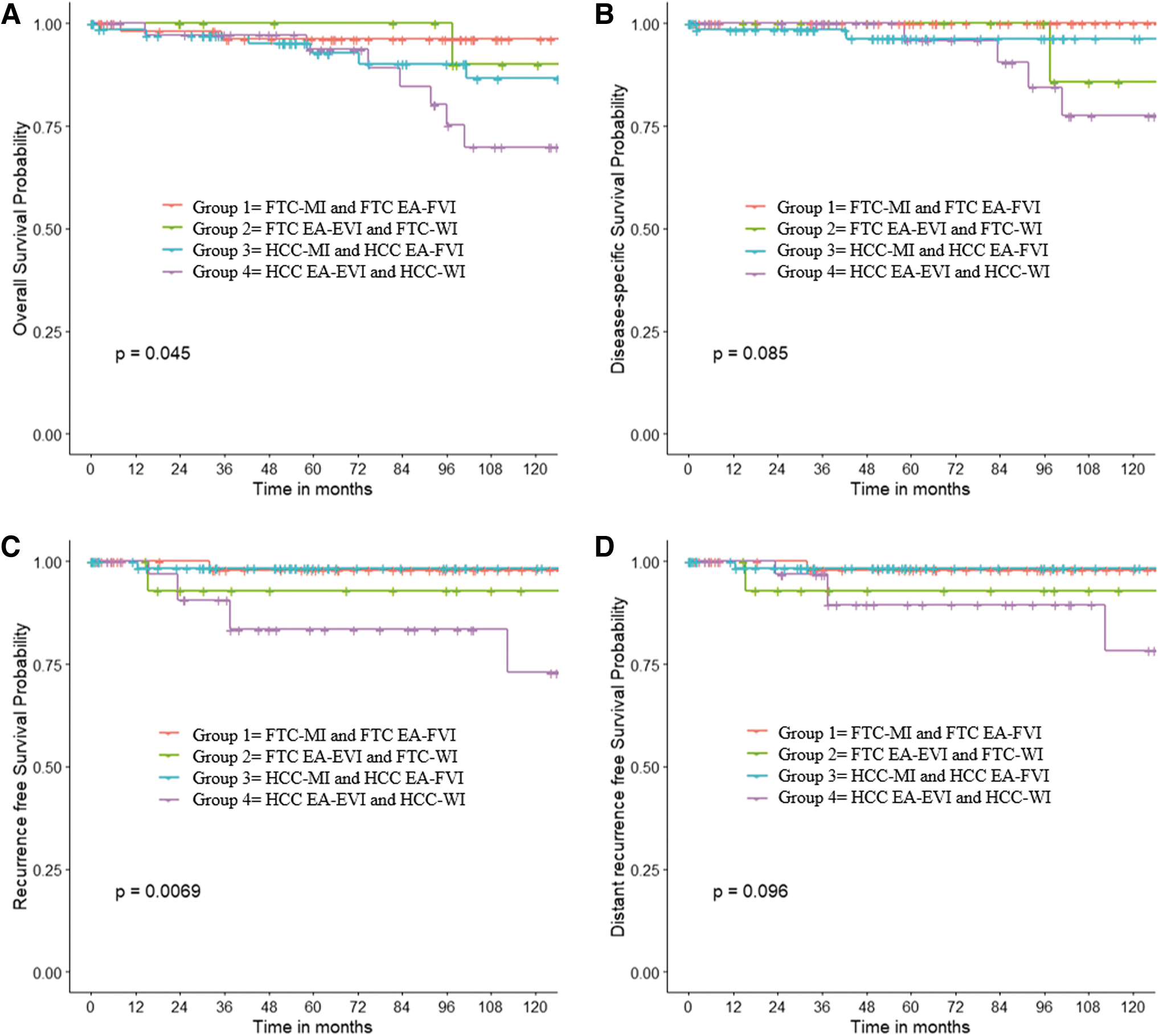
Kaplan–Meier estimates of overall survival (
Outcomes stratified by VI
Outcomes stratified by VI are given in Table 4. Of 84 patients who had no VI reported on the pathological report, 1 patient (1%) had a distant metastasis at presentation and died of the disease. The other 11 patients (13%) died of other causes. Of 106 patients who had any VI, 4 patients (4%) had distant metastasis at presentation. During follow-up, 3 patients (3%) had locoregional recurrences and 7 (7%) had distant recurrences. Six patients (6%) died of the disease and 14 (13%) deaths were unrelated to the disease.
Outcomes Stratified by Vascular Invasion
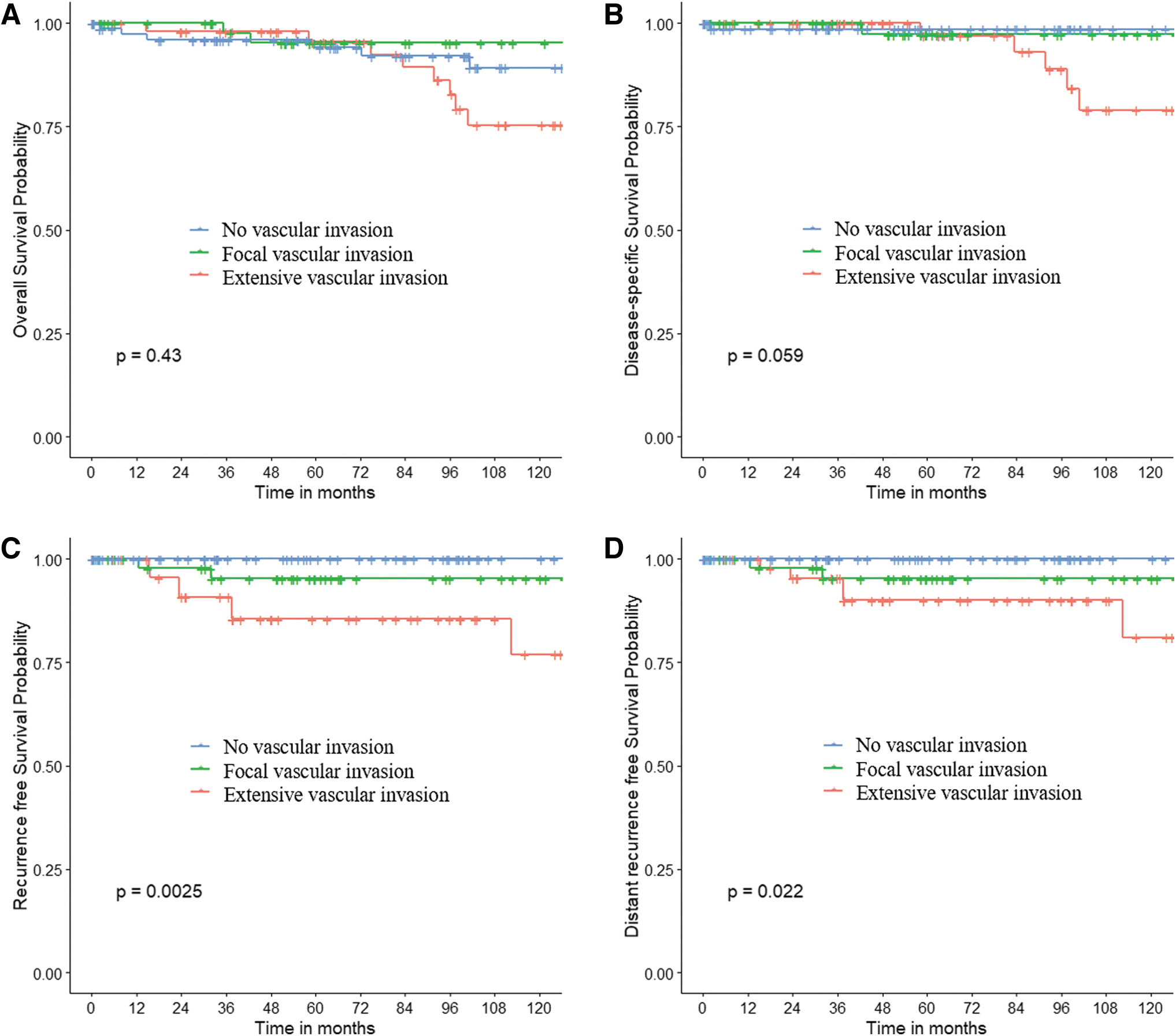
We classified patients into three groups according to the extent of VI: no, focal (<4 foci), and extensive (≥4 foci). Figure 4A–D provides OS, DSS, RFS, and DRFS stratified by extent of VI. Patients with extensive VI had poorer overall RFS (10-year % RFS for no VI, focal VI, and extensive VI: 100%, 95%, and 77%, p = 0.0025) and poorer distant control (10-year % DRFS: 100%, 95%, 81%, p = 0.022). There was a trend to poorer DSS (99%, 97%, 79%, p = 0.059) but this was not statistically significant. There was no significant difference in OS (89%, 95%, and 75%, p = 0.43) and LRRFS (100%, 98%, and 96%, p = 0.29).
Kaplan–Meier estimates of overall survival (
Discussion
The relevance and impact of VI along with phenotype (FTC vs. HCC) on outcome remain unclear. We have carried out a comprehensive analysis of patients with FTC and HCC after a detailed pathological review to identify the fundamental clinical and pathology differences between these two entities and characterize the impact of extent of VI on outcome.
Controversy about VI on outcome
Since VI in thyroid malignancies was first described by Graham in 1924, it has been surrounded by controversies (11). First, there is a lack of consistent and clear criteria to characterize VI. Another area of controversy is whether the presence of VI and the extent of VI has any impact on outcome. There were divergent data concerning the impact of the presence of VI on the biological behavior of tumors (12). Mete and Asa highlighted the presence of VI as a valuable predictor of developing distant metastasis, especially in well-differentiated thyroid cancer (13). In contrast, a study by Sugino et al. showed that VI did not increase the risk for distant metastases (9). It appears these differences are owing to the extent of VI in the tumor, not only the presence of VI. Most studies now emphasize the paramount importance of the extent of VI as a prognostic factor (14 –19). In a cohort of 276 patients with low-grade encapsulated follicular cell-derived thyroid carcinomas, Xu et al. reported that extensive VI (≥4 foci) is an independent prognostic predictor of recurrence (12). Ghossein et al. also demonstrated that ≥4 foci of VI was the most important predictor of recurrence, patients with <4 foci had significant higher RFS compared with ≥4 foci, respectively, 100% versus 20%, p < 0.001 (14). This article reiterates the impact of the extent of VI on the outcomes.
In our cohort, we classified patients as either no VI, focal VI (<4 foci), or extensive VI (≥4 foci). We clearly show that the extent of VI was an important prognostic factor for developing recurrence (mostly distant metastasis). However, most patients even those with extensive VI still do well with a good OS and disease-specific survival.
Controversy on FTC and HCC subtypes
FTC was traditionally classified into MI and WI (20 –22). In 2014, the Armed Forces Institute of Pathology (AFIP) subdivided the MI tumors into three subcategories: tumors with only capsular invasion; tumors with limited VI (<4 foci); and tumors with extensive vascular VI (>4 foci). In 2017, the WHO Classification of Endocrine Tumors (4) classified FTC into three categories: MI (capsular invasion only), EA (presence of angioinvasion, regardless of the number of foci), and WI.
In our study, we used a modification of the WHO classification by stratifying both FTC and HCC tumors into four groups rather than three, because the number of foci of VI seems to impact the clinical outcomes. Our study presents a descriptive comparison of the new subgroups of FTC and HCC, demonstrating differences in the clinical presentation, treatment, pathological findings, and outcomes.
Impact of phenotype (FTC vs. HCC) on outcome
HCC is now recognized as a distinct entity from FTC owing to its peculiar clinical presentation, genomic features, and pathological features (4,5,7,8). A genomic study by Ganly et al. in 2013 reported that HCC was a unique entity with molecular and transcriptomic landscape quite different from FTC (6). More comprehensive genomic studies on HCC were reported by Ganly et al. (7) and Gopal et al. (8) in 2018 using next-generation sequencing and RNASeq; both studies showed that HCC had unique genomic characteristics distinguishable from FTC. Clinically, although there is no consensus across the literature, HCC is usually considered by clinicians to be more aggressive and have a poorer prognosis than FTC (23,24). Our study confirms that HCC has higher recurrence rates than FTC.
Impact of VI and phenotype on treatment
In both FTC and HCC, encapsulated tumors with capsular invasion only are associated with an excellent prognosis. In our cohort, the only patient with absence of VI who died of the disease had distant metastasis at diagnosis. Our group has shown that when distant metastases occur in primary thyroid carcinomas with low-risk histology (such as those with capsular invasion only), they are predominantly found at presentation (25). The other 84 patients with no VI had no recurrences, distant metastases, or deaths related to the disease. The National Comprehensive Cancer Network (NCCN) guidelines, therefore, consider thyroid lobectomy as adequate treatment for these tumors (26).
Tumors with <4 foci of VI are also considered to be less aggressive; thus, the NCCN recommendations are similar to those for tumors with no VI. In our study, the group with no VI had less distant metastasis than the groups with focal or extensive VI. In WI and EA with extensive VI tumors, NCCN guidelines recommend prompt completion thyroidectomy (if the patient had a lobectomy) followed by adjuvant 131I therapy (26). This is also corroborated by our studies, which showed worse RFS in patients with 4 or more foci of VI (12,14). The more aggressive treatment recommendation aligns with the worse prognosis reported in this study.
In our cohort, HCC had higher rates of recurrence. Distant metastases from FTC and HCC are associated with tumors with extensive VI and appear to be more frequent in the HCC phenotype. Surgery, external beam radiation, RAI therapy, and systemic therapies can be used to treat distant metastases from both FTC and HCC (27 –30). In FTC, some lung and bone metastases remain iodine avid and therefore 131I therapy can also be useful. In contrast, this is rarely the case with distant metastases in HCC. Other treatment modalities might be required for patients with distant metastasis. With the identification of the mTOR pathway playing an important role in HCC pathogenesis (31), a randomized phase II trial by the Alliance for Clinical Trials in Oncology is currently underway to compare the progression-free survival in patients with HCC that is RAI refractory in two groups, one treated with sorafenib alone and the other combining sorafenib and everolimus (NCT02143726).
One of the limitations of our study is the small sample size, because these are rare types of thyroid cancers. The rare events of interest such as death or recurrence also have implications for the study power. However, our series is one of the largest studied in the literature. It also has the intrinsic limitation of a retrospective design. There are also the limitations created by selection bias on treatment. Although we have decades of experience in the management of thyroid cancer and a comprehensive DMT with a uniform philosophy of treatment, one can never completely account for the fact there is no randomization of treatments or standardization of interventions between the groups. There is a possible referral bias because all patients were treated in a tertiary cancer care center.
The strengths of our study include the detailed pathological review of cases by expert head and neck pathologists categorizing patients into groups considering the extent of VI. This study highlights that both the extent of VI and the histological phenotype (follicular vs. Hurthle cell) are of great importance when predicting clinical outcomes. They can help stratify patients for therapy, especially regarding 131I therapy and completion of thyroidectomy as well as type of systemic therapy for patients with distant metastases.
In conclusion, compared with other subtypes of HCC and FTC, patients with HCC EA-EVI and HCC-WI are more likely to recur and have poorer distant control. Accurate pathological assessment of VI and pathological subtype are essential to identify patients at higher risk of recurrence and death.
Footnotes
Authors' Contributions
A.Y. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: I.G., L.W., R.R., and D.M. Acquisition, analysis, or interpretation of data: V.H., L.W., R.R., D.M., A.Y., S.P., and I.G. Drafting the article: D.M. and I.G. Critical revision of the article for important intellectual content: D.M., B.X., R.G., M.T., S.P., and I.G. Statistical analysis: A.Y., D.A., and I.G. Administrative, technical, or material support: A.Y. and S.P. Study supervision: S.P., R.G., and I.G.
Author Disclosure Statement
The authors have no financial or personal relationships that could potentially influence this work.
Funding Information
The preparation of this article was funded in part by the NIH/NCI Cancer Center Support Grant No. P30 CA008748 to M.S.K.