
Abstract
Background:
In contrast to the thyroid hormones (TH) 3,3′,5-triiodothyronine (T3) and thyroxine (T4), current literature on thyroid hormone metabolite concentrations in the hypothyroid and hyperthyroid states is inconclusive. It is unknown how thyroidectomy affects thyroid hormone metabolite concentrations and if levothyroxine (LT4) replacement therapy after thyroidectomy restores thyroid hormone metabolite concentrations in those without a thyroid gland. The treatment of patients with differentiated thyroid cancer (DTC) covers the euthyroid, hypothyroid, and (subclinical) hyperthyroid states and therefore provides a unique model to answer this. Here, we prospectively studied nine TH and its metabolites (THM) across different thyroid states in a cohort of patients treated for DTC. Also, three potentially important determinants for THM concentrations were studied.
Methods:
We prospectively included patients aged 18 to 80 years who were scheduled for DTC treatment at the Erasmus MC. Peripheral blood samples were obtained before surgery (euthyroid, endogenous TH production), after surgery just before radioactive iodine therapy (hypothyroid), and six months later on LT4 therapy ([subclinically] hyperthyroid, exogenous T4 supplementation). Nine THMs were quantified in serum with an established liquid chromatography/tandem mass spectrometry method. Repeated measurement analysis was used to compare the three different thyroid states with each other for each THM, while linear regression was used to determine the association between THM concentrations and age, sex, and kidney function.
Results:
In total, 77 patients (mean age 49 years; 65% women) were eligible for the study. 3,5-diiodothyronine and 3,3′,5-triiodothyroacetic acids were below the lower limit of detection. Compared with the euthyroid state, all THMs were significantly decreased in the hypothyroid state and significantly increased in the (subclinically) hyperthyroid state, with T3 concentrations remaining within the reference interval. Higher age was associated with higher 3-monoiodothyronine (3-T1) concentrations (p < 0.001). Women had higher L-thyronine concentrations than men (p = 0.003). A better kidney function was associated with lower 3-T1 concentrations (p < 0.001).
Conclusions:
All THMs decrease after a thyroidectomy and increase under thyrotropin (TSH)-suppressive LT4-therapy, suggesting that formation of thyroid hormone metabolites is dependent on peripheral extrathyroidal metabolism of T4. This is also reflected by T3 concentrations that remained within the reference interval in patients receiving TSH-suppressive LT4-therapy as T3 has some thyroidal origin.
Introduction
The thyroid hormones (TH) thyroxine (T4) and 3,3′,5-triiodothyronine (T3) are essential for a proper function of virtually every tissue in the human body. The thyroid gland predominantly secretes the prohormone T4. T4 is metabolized by deiodination into the active metabolite T3. The major biological activity of TH is mediated by binding of T3 to nuclear TH receptors. T4 and T3 can be further metabolized to form other thyroid hormone metabolites (1). Potential roles for thyroid hormone metabolites have been described in processes such as energy metabolism, lipid metabolism, bone remodeling, and cardiac hypertrophy (2 –6).
Hypothyroidism is a very common endocrine disorder that can be treated with levothyroxine (LT4) (7). Despite LT4 treatment, 10–15% of the patients show significant physical and psychological impairment compared with matched controls or the general population (8 –13). Altered thyroid hormone metabolite concentrations could possibly contribute to these residual complaints. Although it has been reported that patients on T4 supplementation generally have lower concentrations of serum T3 than euthyroid controls, it is currently unknown if T4 supplementation can adequately restore concentrations of other thyroid hormone metabolites (14,15).
Current literature on thyroid hormone metabolite concentrations in the euthyroid, hypothyroid, and hyperthyroid states is inconclusive for iodothyronines such as 3-monoiodothyronine (3-T1), 3,5-diiodothyronine (3,5-T2), and 3,3′-diiodothyronine (3,3′-T2), and for iodothyroacetic acids such as 3,3′,5-triiodothyroacetic acid (triac, TA3) and 3,3′,5,5′-tetraiodothyroacetic acid (tetrac, TA4) (Table 1) (16 –35). These inconsistencies between studies are likely due to the fact that most studies have small sample sizes (n < 30), and thyroid hormone metabolites were measured with (radio)immunoassays. Low selectivity is an important limitation of (radio)immunoassays.
Literature on Thyroid Hormone Metabolites in Euthyroid, Hypothyroid, and Hyperthyroid States
Nonsignificant compared with the euthyroid subjects.
3-T1, 3-monoiodothyronine; 3,3′-T2, 3,3′-diiodothyronine; 3,5-T2, 3,5-diiodothyronine; LC-MS/MS, liquid chromatography/tandem mass spectrometry; LLoD, lower limit of detection; TA3, 3,3′,5-triiodothyroacetic acid; TA4, 3,3′,5,5′-tetraiodothyroacetic acid.
Compared with (radio)immunoassays, liquid chromato-graphy-tandem mass spectrometry (LC-MS/MS) methods are more reliable due to increased selectivity as selection is based on chromatographic behavior, mass, and fragmentation pattern. Furthermore, thyroid hormone metabolite concentrations at different thyroid states were not compared within the same subject in these earlier studies. In addition, while age, sex, and kidney function are potentially important determinants for concentrations of TH and its metabolites (THM), only very limited clinical information was reported (32,36 –40). Until now, it therefore remains unclear if all THMs are affected to the same extent in hypothyroid and hyperthyroid states, or if compensatory metabolic mechanisms are in place. In addition, it is unclear if LT4 therapy is able to restore serum concentrations of all these THMs after thyroidectomy.
Historically, patients with differentiated thyroid cancer (DTC) are treated with total thyroidectomy followed by radioactive iodine (RAI) therapy, and subsequently with LT4 in a thyrotropin (TSH)-suppressive dose (41). Patients are usually euthyroid before surgery, hypothyroid after three to four weeks of thyroid hormone withdrawal (THW) just before RAI therapy, and (subclinically) hyperthyroid during TSH-suppressive therapy. These patients therefore provide a unique model to study how thyroidectomy without and later with LT4 replacement therapy affects THM concentrations.
Recently, we developed an LC-MS/MS panel for seven iodothyronines and two iodothyroacetic acids in human serum, and subsequently established reference intervals in healthy adults (38). Here, we use this extensive panel to prospectively analyze how thyroidectomy without and with T4 supplementation affects THM concentrations in patients treated for DTC.
Materials and Methods
Study population
Patients aged 18 to 80 years who were scheduled for a total thyroidectomy for DTC followed by RAI therapy between April 2013 and September 2018 at the Erasmus MC University Medical Center, Rotterdam, The Netherlands, were deemed eligible for this study. All included patients had tumor diameters larger than 1 cm and were treated in line with the current Dutch guidelines with a total thyroidectomy followed by RAI therapy (42). Exclusion criteria were inadequate understanding of the Dutch language, another active malignancy, known thyroid disease, an active inflammatory disease, or using any drugs known to influence TH metabolism.
We recorded demographic, physical, disease, and treatment characteristics. Demographical variables included age at diagnosis and sex. Physical characteristics included height, weight, and BMI. Disease characteristics included disease type and AJCC/TNM stage (8th edition). Data regarding treatment consisted of extent of surgery, RAI therapy dose, and (weight-corrected) LT4 dose. The study was approved by the Institutional Review Board of the Erasmus Medical Center (MEC-2012-561).
Peripheral blood samples were obtained from all participants at three visits, that is, before surgery when patients were euthyroid (visit [V] = 0), just before RAI therapy when patients were hypothyroid due to three to four weeks of THW (V = 1), and six to nine months thereafter when patients were (subclinically) hyperthyroid during TSH-suppressive therapy by LT4 (V = 2) (Fig. 1). DTC patients receiving RAI therapy after recombinant human TSH (rhTSH) stimulation, instead of THW, were included to assess the influence of THW on TH metabolism; these patients treated with rhTSH were (subclinically) hyperthyroid and not hypothyroid at V = 1 (Fig. 1).
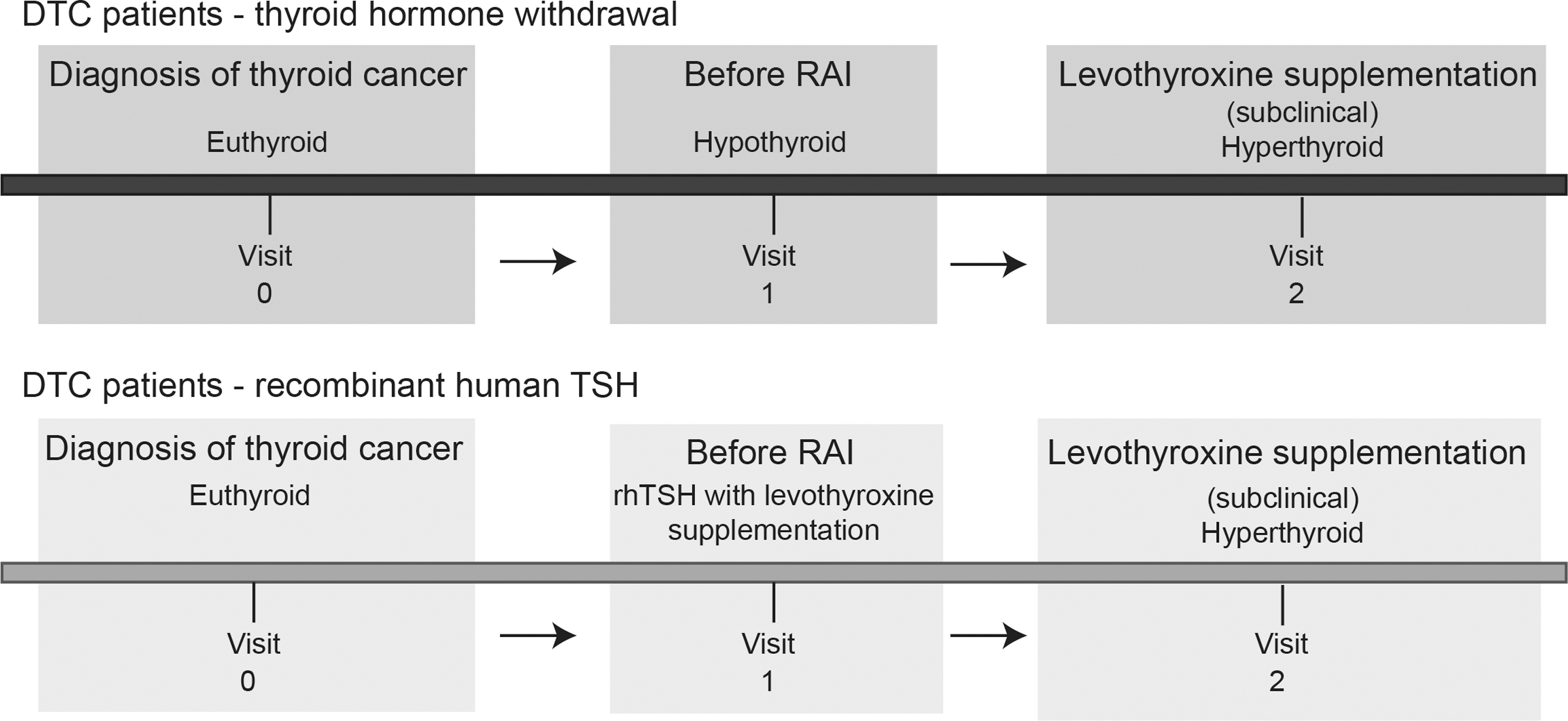
DTC model. DTC, differentiated thyroid cancer, RAI, radioactive iodine; rhTSH, recombinant human TSH; TSH, thyrotropin.
Laboratory measurements
Peripheral blood sample measurements were processed on the same day. We measured TSH and free T4 (fT4) as markers of thyroid function. Serum TSH was measured by a sandwich immunoassay (Immulite 2000 XPi; Siemens, Los Angeles, CA), and serum fT4 was measured by a competitive immunoassay (Vitros ECI Immunodiagnostic System; Ortho-Clinical Diagnostics, Rochester, MI). Of note, the fT4 immunoassay was calibrated to an in-house-established equilibrium dialysis method, and as such, a 23% correction above the manufacturer's instruction was needed. The magnitude of correction was comparable with the correction needed to agree with the reference measurement procedure (43). Creatinine was measured with an enzymatic method in heparin plasma (Cobas 8000 modular analyzer series; Roche, Indianapolis, IN). Kidney function was estimated by calculation of estimated glomerular filtration rate (eGFR) using the CKD-epi equation (44).
We determined nine THMs in serum samples stored at −80°C using our previously published method (38). Briefly, an internal standard and an antioxidant mixture were added to 500 μL of serum. Samples were precipitated with acetonitrile, followed by a solid-phase extraction and evaporation to dryness under a stream of nitrogen at 50°C. After reconstitution, samples were injected onto a UPLC column (Waters Acquity UPLC BEH C18 1.7 μm, 130 Å, 1.0 × 100 mm) separating THMs with a gradient of MilliQ +0.1% formic acid as mobile phase A and acetonitrile +0.1% formic acid as mobile phase B. After liquid chromatography, compounds were detected with targeted mass spectrometry (Sciex QTRAP 6500+). Data were analyzed with analyst 1.7 software and MultiQuant 3.0.3 software packages.
Statistical analysis
For continuous variables, we calculated means and standard deviations, or in case of a non-normal distribution, medians with 25th–75th interquartile ranges. For categorical variables, absolute numbers with percentages were recorded.
To assess differences in THM concentrations across the three different thyroid states, we used repeated measurement analysis to compare the three different thyroid states with each other for each THM; we used marginal models, and the appropriate covariance matrix that best fitted the data was selected to account for the correlation between the repeated measurements of each patient. In these analyses, we adjusted for age and sex. If needed, appropriate (natural) logarithmic transformation of the THM concentrations was applied to obtain normal distributions.
We used linear regression to compare THM concentrations between the THW and rhTSH patients at V = 2 adjusted for age, sex, and weight-corrected LT4 dose. Correlations between the different THMs were assessed at V = 0 using the nonparametric Spearman correlation test as THM concentrations were non-Gaussian distributed. Linear regression was performed (at V = 0) to determine the association between THM concentrations and age, sex, or kidney function; all these analyses were performed unadjusted. To account for multiple testing in the different analyses, we used Bonferroni correction, and therefore, p-values below 0.005 were considered statistically significant.
All analyses were performed using either SPSS Statistics for Windows (version 25.0) or R statistical software, including the “nephro” package to calculate the eGFR with the CKD-Epi equation (version 3.4.1) (45).
Results
Population characteristics
During the inclusion period, 119 patients were eligible for the study, of which 42 patients were not included because they were not willing to participate (n = 7), were missed to be included (n = 11), or did not have a blood sample at each thyroid state (n = 24). The remaining 77 patients were included.
Descriptive characteristics of the participants are shown in Table 2. The mean age of the participants was 49.0 years (range 19 to 80 years), BMI at baseline was 27.1 kg/m2, 65% were women, 88% had papillary thyroid carcinoma, eGFR was 90.8 mL/min/1.73 m2, and 88% received RAI therapy after THW and 12% after rhTSH. Median time between RAI therapy and V = 2 was six months.
Characteristics of the Study Population
Values are means (± standard deviations), medians (25–75 interquartile ranges), or numbers (percentages).
eGFR, estimated glomerular filtration rate; mCi, milliCurie; RAI, radioactive iodine; rhTSH, recombinant human thyrotropin; THW, thyroid hormone withdrawal; TT, total thyroidectomy.
TSH, fT4, and THM
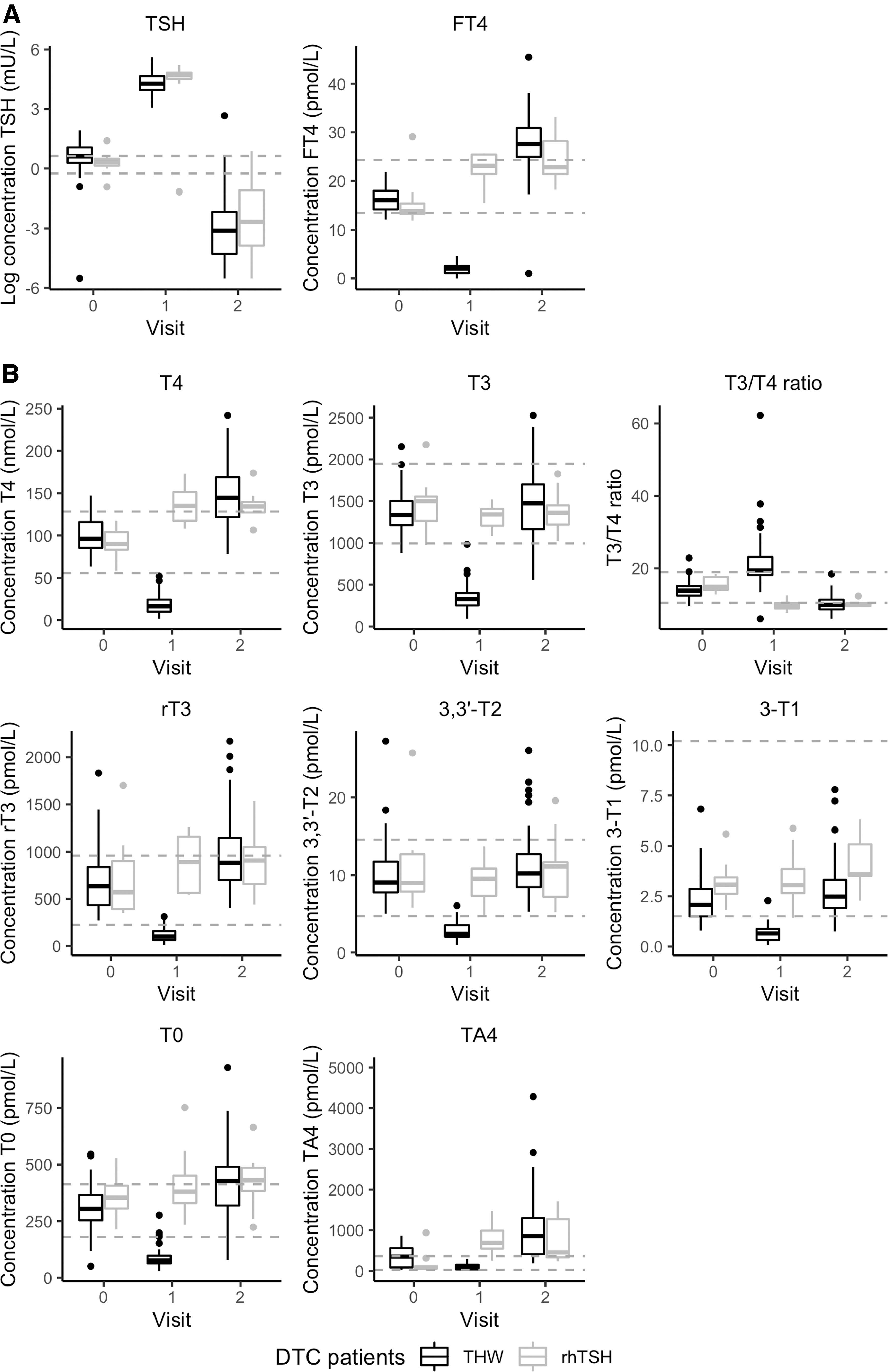
At V = 0, all patients were euthyroid as confirmed by TSH and fT4 concentrations within the reference interval (Fig. 2A). At V = 1, patients undergoing THW were hypothyroid with a median TSH of 71.8 mU/L and a median fT4 of 2 pmol/L (Fig. 2A). At V = 1, patients treated with rhTSH had a median fT4 of 23.1 pmol/L (Fig. 2A). At V = 2, patients who underwent THW and patients treated with rhTSH were both (subclinically) hyperthyroid as confirmed by a median TSH of, respectively, 0.026 and 0.069 mU/L, and a median fT4 of, respectively, 27.6 and 22.8 pmol/L (Fig. 2A).
TSH, fT4 (
The majority of the measurements of 3,5-T2 (>90%) and TA3 (100%) were below the lower limit of detection, and could therefore not be used in further analyses.
In patients undergoing THW, all THMs were significantly decreased after thyroidectomy (hypothyroid state [V = 1] compared with euthyroid state [V = 0]), and all THMs significantly increased after LT4 supplementation (hyperthyroid state [V = 2] compared with the hypothyroid state [V = 1]) (Fig. 2B and Table 3). When comparing the hyperthyroid state with the euthyroid state, all THMs were significantly increased except for T3 (p = 0.138) (Table 3).
Comparison of the Three Different Thyroid States with Each Other and Between Patients Treated with Thyroid Hormone Withdrawal or Recombinant Human Thyrotropin for Each Thyroid Hormone and Thyroid Hormone Metabolite, Thyrotropin, and Free Thyroxine
Values are the differences between both thyroid states expressed in natural log-transformed units.
p-Values (age and sex adjusted) for comparing both thyroid states in THW patients.
Values are the differences between THW and rhTSH expressed in natural log-transformed units.
p-Values (age, sex, and weight-corrected levothyroxine dose adjusted) for comparing rhTSH and TWH patients at V = 2.
p-Values below 0.005 are considered significant.
fT4, free thyroxine; rT3, 3,3′,5′-triiodothyronine; T0, L-thyronine; s.e., standard error; T3, 3,3′,5-triiodothyronine; T4, thyroxine; V, visit.
In patients treated with rhTSH, all THMs remained normal or increased when comparing V = 1 with V = 0 (Fig. 2B). At V = 2, adjusted for age, sex, and weight-corrected LT4 dose, none of the THMs, except for 3-T1 (p = 0.0047), was significantly different between rhTSH patients and THW patients.
Serum levels of T3 and T4 are dependent on deiodinating enzymes (deiodinases), thyroid function, and the binding capacity of binding proteins. Therefore, ratios between these THMs are thought to better reflect peripheral deiodination. Therefore, we calculated the T3/T4 ratios in each thyroid state. In patients undergoing THW, the T3/T4 ratio significantly increased in the hypothyroid state and significantly decreased after TSH-suppressive LT4 therapy compared with the euthyroid state. (Fig. 2B). In patients treated with rhTSH, the T3/T4 ratio was similarly decreased at V = 1 and at V = 2 compared with the euthyroid state (Fig. 2B).
TSH did not correlate with THM and fT4 concentrations in the euthyroid state (Supplementary Table S1). In the euthyroid state, fT4 was positively correlated with all THMs, except for 3-T1 and TA4 (Supplementary Table S1). Every THM was correlated to its precursor except for 3-T1 with 3,3′-T2 and TA4 with T4 (Supplementary Table S1).
Association of THM concentrations with age, sex, and kidney function
At V = 0, higher age was significantly associated with higher 3-T1 concentrations (p < 0.001) and lower T4 concentrations (p = 0.002). Besides, a higher eGFR was significantly associated with lower 3-T1 concentrations (p < 0.001) and higher T4 concentrations (p = 0.003) (Supplementary Fig. S1 and Supplementary Table S2). Of the other THMs, women had significantly higher L-thyronine (T0) concentrations than men (p = 0.003) (Supplementary Fig. S1 and Supplementary Table S2).
Discussion
To our knowledge, this is the first prospective study investigating the course of different THM concentrations and TH metabolism across different thyroid states in the same patient. At the individual level, all THMs decreased after THW and all THMs increased with TSH-suppressive LT4 therapy, with T3 concentrations remaining within the reference interval. All measured THMs, follow the same trend as T4, suggesting that all measured thyroid hormone metabolites are produced by peripheral metabolism of T4 and have no or negligible thyroidal origin. This is also reflected by T3, which has thyroidal origin (∼20%) and remained within the reference interval in the absence of a thyroid gland and treatment with TSH-suppressive LT4 therapy.
In our study, patients treated for DTC by total thyroidectomy followed by RAI therapy are used as a model to study the course of different THM concentrations across different thyroid states. This DTC model is a known concept (40,46 –48) and has several advantages: (i) three thyroid states can be studied in the same patient in a prospective manner, (ii) hypothyroidism without residual TH production by the thyroid gland is ensured by total thyroidectomy without LT4 supplementation, and (iii) in the absence of the thyroid gland (subclinical), hyperthyroidism is caused by exogenous oral LT4 therapy, and therewith all thyroid hormone metabolites are directly or indirectly derived from LT4.
In the hypothyroid state compared with the euthyroid state, all THMs decreased significantly in patients undergoing THW, while the T3/T4 ratio increased. This is in correspondence with most literature on 3-T1, 3,3′-T2, and T3/T4 ratios (16,24 –31,49). The decrease of all THMs after thyroidectomy and the subsequent rise after LT4 therapy in our study emphasize the dependence of the formation of these thyroid hormone metabolites on T4. The increase of the T3/T4 ratio in patients undergoing THW is in line with reports showing that in a hypothyroid state, the body's response is to ensure sufficient T3 concentrations via transporters, deiodinases, and TH receptors (50).
In the hypothyroid state, T3 concentrations remain at ∼400 pmol/L, while these patients do not have a thyroid gland and do not receive exogenous oral LT4 therapy. The T3 concentration in the circulation at this hypothyroid state is most likely explained by T3 production via peripheral metabolism of residual T4 produced before thyroidectomy. However, it might be that a small residual of the thyroid gland, which still produces a small amount of T3, was left after surgery.
In the (subclinically) hyperthyroid state compared with the euthyroid state, all THMs increased and the T3/T4 ratio decreased after TSH-suppressive LT4 therapy in patients who underwent THW and in patients who were treated with rhTSH. Increased 3,3′-T2, T3, T4, and T3/T4 ratios are in correspondence with earlier reports (32,49). This suggests that exogenous LT4 restores thyroid hormone metabolite concentrations via peripheral metabolism in extrathyroidal tissues, as all patients underwent a total thyroidectomy. All thyroid hormone metabolites follow the same trend as T4. T3 concentrations in (subclinically) hyperthyroid thyroidectomized patients on LT4 therapy are similar to euthyroid concentrations.
This is likely explained by the lack of thyroidal T3 production since T3 can be formed via two different routes: (i) T3 production by the thyroid gland (∼20% of serum T3 is derived from thyroidal T3 secretion in the euthyroid state) and (ii) peripheral metabolism of T4 via deiodination. In our study, T3 formation at V = 2 is completely dependent on peripheral metabolism, as patients usually do not have any remaining thyroid tissue after surgery and RAI therapy. Peripheral metabolism likely explains our finding that T3 concentrations were within the reference interval, while fT4 levels were elevated, which is a known phenomenon (14,15).
To our knowledge, this is the first study investigating the correlation of TSH or fT4 with T0, 3-T1, and 3,3′-T2, which was previously impeded by the lack of selective analytical methods to quantify these thyroid hormone metabolites. Unexpectedly, TSH was not correlated with fT4 or any of the other THMs in the euthyroid state. The previously reported log-linear relationship between TSH and fT4 in a large population-based study was weak (51), suggesting that our study might be underpowered to identify such a relationship. The euthyroid state itself is another possible explanation for the absence of the correlation between TSH and fT4 as this relationship is mainly observed in diseased states. The absence of a correlation between TSH and TA4 was in accordance with previous literature in healthy individuals and patients with Graves' disease (35).
Associations between serum creatinine levels and T3 and T4 have been reported in the literature, and also across different thyroid states (36,37,40). The relationship between TH levels and kidney function is well known, but the causality remains a topic of interest in both health and disease states (52). In the euthyroid state, our data are in agreement with these studies for T4, but not for T3. This difference might be ascribed to our smaller sample size, the lower selectivity of (radio)immunoassays, and/or only looking at a single thyroid state instead of comparing different thyroid states. Especially in kidney dysfunction, potential interferences of TH binding proteins such as T4-binding globulin, transthyretin, and albumin become more relevant.
We discovered that women had significantly higher T0 concentrations than men, but we do not have a good explanation for this sex difference. Therefore, further research is needed to understand this result. We were also the first to discover the significant association between age and 3-T1 and T4. Earlier longitudinal studies showed mixed results for fT4 and T3 changes with increasing age (53). Therefore, further studies on this topic are needed. Further research into the relationship between THM and other factors such as body weight, smoking, or quality of life is also of interest.
The current study has some limitations. First, we would have preferred to measure all THMs with the current panel, but unfortunately lower concentrations of 3,5-T2 and TA3 could not be measured, suggesting that our method might not be sensitive enough. The strength of our innovative method is that we measure a panel of thyroid hormones and thyroid hormone metabolites, but this approach also restricts the possibilities for optimizing the sample preparation, and the liquid chromatography and the mass spectrometry settings. Other thyroid hormone metabolites with only a positive charge such as 3-iodothyronamine are also of interest, but the selectivity of our sample preparation for negatively charged ions limits this possibility. Second, our study might be underpowered especially for the group of patients treated with rhTSH. Third, kidney function measurements were unfortunately not available in the hypothyroid and (subclinically) hyperthyroid state impeding further thorough investigations.
Conclusion
All THMs decrease after a thyroidectomy and increase under TSH-suppressive LT4 therapy, indicating that formation of thyroid hormone metabolites is dependent on peripheral extrathyroidal metabolism of T4, with the exception of T3 that has some thyroidal origin. Further research into the relationship between THM and quality of life is needed to assess whether THM concentrations play a role in the persistent complaints in patients with hypothyroidism undergoing LT4 replacement therapy.
Footnotes
Authorship Confirmation Statement
Rutchanna Jongejan, Evert van Velsen, Robin Peeters, and Yolanda de Rijke designed the current study. Rutchanna Jongejan and Evert van Velsen conducted the statistical analyses and wrote the article. All authors reviewed and revised the article to improve its intellectual and technical content.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
We are grateful to Sciex (Framingham) for their contribution to our collaboration in the development of new diagnostic parameters through which we were able to use the QTRAP 6500+ at no cost.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2