
Abstract
Background:
Image-guided radiofrequency ablation (RFA) for benign nonfunctional thyroid nodules in adults has been shown to be effective and safe, but few trials address the use of RFA in children. Therefore, this study was designed to assess the efficacy and safety of RFA application to benign nonfunctional thyroid nodules in children.
Methods:
A retrospective study of RFA for 70 benign nonfunctional thyroid nodules in 62 children with four-year follow-up was conducted. Volume reduction ratio (VRR), technique efficacy, regrowth rate, symptom score, and cosmetic score were calculated to evaluate the efficacy. Complications and side effects were recorded. Logistic regression analysis was performed to identify risk factors, and subgroup analyses were performed.
Results:
Patients were followed up for at least four years (59.1 ± 10.5 months, range 48–85 months). After RFA treatment, the VRR and technique efficacy rates were highest at the first year * (77.5% and 91.4%, respectively) but decreased by four years (55.1% and 81.4%, respectively). The symptom score decreased from 4.0 ± 2.1 * to 0.8 ± 1.6 (Z = −6.82, p < 0.001), and the cosmetic score decreased from 3.3 ± 0.7 to 1.3 ± 0.9 (Z = −7.0, p < 0.001). * The nodule regrowth rate was 22.9%, of which 56.3% of cases represented loss of efficacy. In the cases of loss of efficacy, 66.7% had greater volume than their initial presentation. Patients who received a second RFA treatment due to loss of efficacy lost efficacy again. Bilateral nodules, low vascularity, and low cystic components were independent risk factors correlating with technique efficacy. Bilateral nodules correlated with low VRR, low efficacy rate, and high regrowth rate. Nodules with a higher proportion of cystic components had higher VRR. The overall complication rate was 4.8%.
Conclusions:
RFA was effective in reducing the volume of benign nonfunctional thyroid nodules in children, providing significant symptomatic relief with a good safety profile during short- and long-term follow-up. RFA is a good minimally invasive treatment modality for selected pediatric patients, and it may not be appropriate for the treatment of bilateral thyroid nodules in children.
Introduction
The incidence of thyroid nodules in children is 0.2% to 5% and is lower than in adult patients (1). Most pediatric patients with thyroid nodules are asymptomatic, and ∼80% are benign (2). However, some benign thyroid nodules grow in size, causing patients compression symptoms or cosmetic concerns. The guideline for the treatment of pediatric thyroid nodules, which was developed by the American Thyroid Association in 2015 and endorsed by the American Academy of Pediatrics in 2018, recommends that surgery may be considered for nodules in this condition (3,4). However, surgery, especially in pediatric patients (5), may lead to some permanent complications, such as hypoparathyroidism and vocal cord paralysis, and even uncomplicated thyroid surgery can significantly affect quality of life (6). There have also been attempts to treat thyroid nodules with levothyroxine, but its efficacy and safety is not entirely certain (7,8). Therefore, for pediatric patients, this treatment modality is not yet recommended (3). Based on these facts, research on new treatment modalities for benign thyroid nodules in children is still necessary.
Thermal ablation techniques, including radiofrequency ablation (RFA), laser ablation (LA), high-intensity focused ultrasound (HIFU), and microwave ablation, are increasingly being used to treat symptomatic benign thyroid nodules as access to this technology increases. Of these, RFA and LA have been the most intensively studied. Recent studies have shown that nodules treated with RFA have higher volume reduction compared with LA and microwave ablation (9 –12). HIFU is more likely to be applied to smaller nodules (13,14). Therefore, for benign thyroid nodules that require treatment, RFA may have a broader application (15).
RFA uses an electrode needle to generate an alternating electric field with a frequency of 200 to 1200 kHz, thereby generating a local heat source of 50°C to 105°C in the tissue and causing local tissue necrosis (16 –18). The first application of RFA for the treatment of benign thyroid nodules was in 2003 (19). Since that time, a large number of clinical trials have been conducted and have confirmed the safety and efficacy of RFA in the treatment of benign thyroid nodules (16,20,21). To date, six medical societies, in a variety of countries, have issued guidelines, consensus statements, or recommendations for the treatment of benign thyroid nodules with RFA (22 –27). Unfortunately, most studies mainly focus on adult patients; although some clinical studies may include pediatric patients, they have not specifically studied the pediatric population. Only one small study (12 patients) has focused on evaluating the safety and efficacy of RFA for benign thyroid nodules in children (28).
The safety and efficacy of RFA for children with benign thyroid nodules in the short and long terms have not been fully investigated. Considering that the clinical features of thyroid nodules in children are different from those in adults (29), as well as considering differences in children's general physiological characteristics, the effect of RFA for thyroid nodules in children still needs to be fully evaluated. In this study, we retrospectively analyzed 70 thyroid nodules in 62 children treated with RFA, with at least four years of follow-up, to evaluate efficacy and safety of RFA treatment and risk factors for regrowth and efficacy.
Materials and Methods
Patients
The study protocol was approved by the hospital Ethics Committee and written consent was obtained from patients' parents. Pediatric patients with benign thyroid nodules treated with RFA in the Department of Thyroid Surgery at our hospital between July 2014 and August 2017 were included in the study. The inclusion criteria were: age ≤18 years; benign nodules confirmed by two separate fine-needle aspiration cytology biopsies or one core needle biopsy; ultrasonography results showing no suspicious malignant features; existence of compressive symptoms, cosmetic problems, or other concerns of caregivers; refusal of surgery; normal thyroid function; availability of information from at least four years of follow-up; and consent to participate. The exclusion criteria were: having received other thyroid treatments within one year before RFA treatment; lack of postoperative follow-up information; or refusal of patients or their caregivers to participate in this study. Ultimately, 62 pediatric patients were included in this cohort.
Assessment before ablation
Ultrasonography was utilized to evaluate the thyroid nodules. The nodule volume was calculated according to the following formula: V = 3.14 × length × width × depth ÷ 6. The nodule composition was recorded. The vascularity of the nodules was quantified using a four-point grading scale from 0 to 3. A nodule was considered grade 0 when no vascularity signal was detected. A nodule was considered grade I when signal was detected in <25% of the nodule. A nodule was considered grade II when signal was detected in 25 to 50% of the nodule. A nodule was considered grade III when signal was detected in more than 50% of the nodule.
Subjective symptoms were assessed by the patient or caregivers and were scored on a scale from 0 to 10 using a visual analog scale. Objective symptoms were assessed by physicians and rated on a cosmetic score of 1 to 4. The detailed score standard used in this study are as described previously (11).
Procedure
All patients were hospitalized. Local anesthesia with 2% lidocaine was used in most patients, and general anesthesia was used in two younger children. Experienced ultrasonographers and thyroid surgeons performed the operation together. A radiofrequency (RF) generator from STARmed (Goyang, South Korea) was used. The 18-gauge electrode needle had a 5 mm tip and was operated under ultrasound (APLI0500; Toshiba, Tokyo, Japan) guidance using trans-isthmic and moving-shot technique with 20 to 40 W of power. When treating nodules with a cystic component, aspiration was performed to remove the fluid. Intraprocedural and postprocedural complications were evaluated based on clinical signs and symptoms. The classification criteria of complications referred to the reporting standards of the Society of Interventional Radiology (30).
Follow-up
The first follow-up was performed at 3 months after treatment, the second at 6 months, and the third at 12 months. Thereafter, follow-up was performed at one-year intervals. Ultrasonography and laboratory tests were required at each follow-up visit. The volume reduction ratio (VRR), which was applied to assess the extent of nodule volume reduction, was determined using the formula: VRR(%) = (initial volume − final volume) ÷ initial volume × 100. To evaluate the effect of single-session RFA treatment, the VRR of secondary treatment (including RF treatment and surgery) was not calculated.
Technique efficacy was defined as a VRR ≥50%. Regrowth was defined as a measured volume that was at least 150% of the minimum volume measured during the follow-up period.
Statistical analyses
All statistical analyses were conducted with SPSS 22 software (IBM, New York). Quantitative variables are displayed as mean ± standard deviation. Categorical variables are displayed as percentages. The nodule volumes represented repeated measurement data, which were compared using the Friedman test. Univariate logistic regression was used to identify the risk factors for regrowth and technique efficacy. Since we only counted the VRR of nodules treated with initial RFA, we chose the second-year technique efficacy rate, which had the largest amount of data, as the criterion for determining the technique efficacy logistic regression-dependent variable. Variables were entered into multivariate logistic regression when their p-values were <0.15. Other comparisons between two groups were made using the chi-square test, Mann–Whitney test or Wilcoxon test, depending on the type of data and distribution characteristics. A p-value <0.05 was considered to represent a statistically significant difference.
Results
Baseline characteristics
The patient selection process is as shown in the flow chart (Fig. 1). The study cohort included 62 patients with a total of 70 thyroid nodules (Table 1). The mean age of the patients was 14.4 ± 3.1 years (range 5–18 years). Of the study cohort, 75.8% (47 cases) were female and 24.2% (15 cases) were male. The mean follow-up time was 59.1 ± 10.5 months (range 48–85 months). Fifty-four patients had one thyroid nodule requiring treatment, and eight children had two thyroid nodules requiring treatment. In this latter group, the two nodules were located in each thyroid lobe. The numbers of small (volume ≤10,000 mm3), medium (10,000 < volume ≤20,000 mm3), and large nodules (volume >20,000 mm3) were 52, 15, and 3, respectively. The number of thyroid nodules with a cystic component ≥50% was 37, and the number of nodules with a cystic component <50% was 33. The mean vascularity score of the nodules was 1.5 ± 1.0. The mean symptom score for children was 4.0 ± 2.1 † , and the mean cosmetic score was 3.3 ± 0.7 † .

Flow chart for selection of study cohort. FTC, follicular thyroid carcinoma; MTC, medullary thyroid carcinoma; PDTC, poorly differentiated thyroid carcinoma; PTC, papillary thyroid carcinoma; RFA, radiofrequency ablation.
Baseline Clinical Characteristics
Evaluation of the effectiveness of RFA
After RFA treatment, the mean of the volumes of the nodules was significantly reduced (Table 2). During follow-ups from three months to four years, the mean VRR was 65.1% (three months), 74.7% (six months), 77.5% (one year), 60.3% (two years), 68.5% (three years), and 55.1% (four years) (Table 2). RFA treatment efficacy rates at each time point were 82.9%, 90.0%, 91.4%, 84.3%, 82.9%, and 81.4%, respectively.
Changes in Thyroid Nodule Volume and Volume Reduction Ratio After Radiofrequency Ablation
RFA, radiofrequency ablation; VRR, volume reduction ratio.
In addition, ultrasonographic examination revealed that 36 nodules (51.4%) had strong echogenicity or hyperechogenicity at three months, and 6 of these still had this phenomenon at six months. At the one-year time point, only one nodule still had this phenomenon and it disappeared in the second year. A representative image is shown in Figure 2.
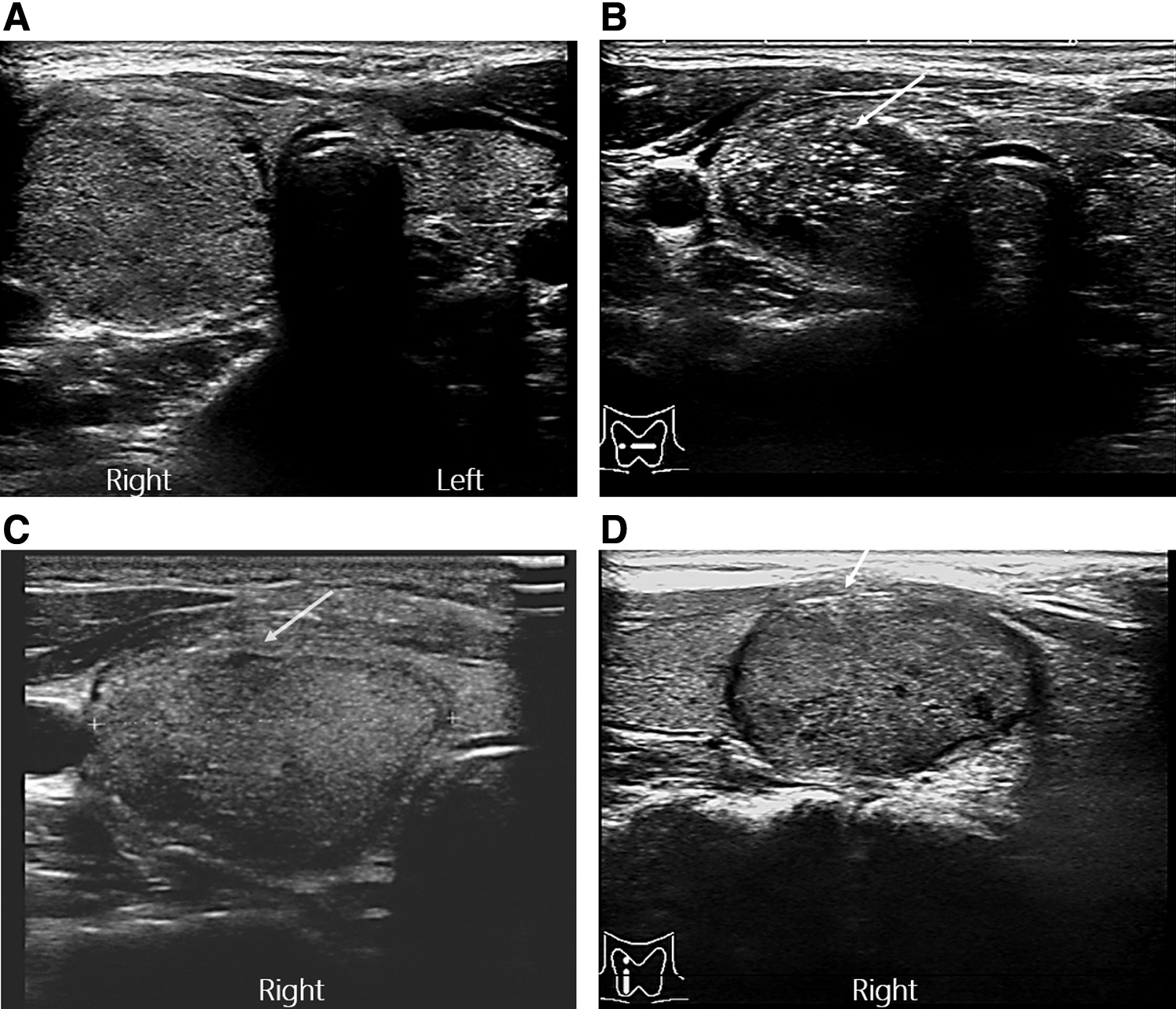
Ultrasonography changes of thyroid nodules before and after RFA treatment and during the follow-up period. (
From laboratory tests, only one patient had a transient thyrotropin (TSH) elevation (TSH:6.8 μIU/mL, FT3 5.47 pmol/L, FT4 11.41 pmol/L) in the second year after RFA, which was not treated with medication and later returned to normal.
RFA treatment was also effective in improving subjective and objective symptoms in children. The symptom score decreased from 4.0 ± 2.1 to 0.8 ± 1.6 (Z = −6.82, p < 0.001) and the cosmetic score decreased from 3.3 ± 0.7 to 1.3 ± 0.9 (Z = −7.0, p < 0.001). §
Of the 70 examined nodules, 16 (22.9%) began to regrow following initial treatment (Fig. 3), but all fine-needle aspiration biopsy results indicated that these growing nodules were benign. Of the regrowing nodules, 56.3% (9/16) had VRR <50%, and 43.8% (7/16) had VRR ≥50% (Fig. 4). When the VRR was <50%, it was defined as loss in treatment efficacy. Furthermore, 66.7% (6/9) of the nodules with VRR <50% became larger than before treatment. Of the nodules with VRR <50%, three nodules had a second RFA treatment, and two nodules had surgery. Nodules that had a second RFA treatment still responded poorly, and both second RFA treatments eventually lost their effectiveness. Nodules that underwent surgical treatment were shown to be benign on pathology.
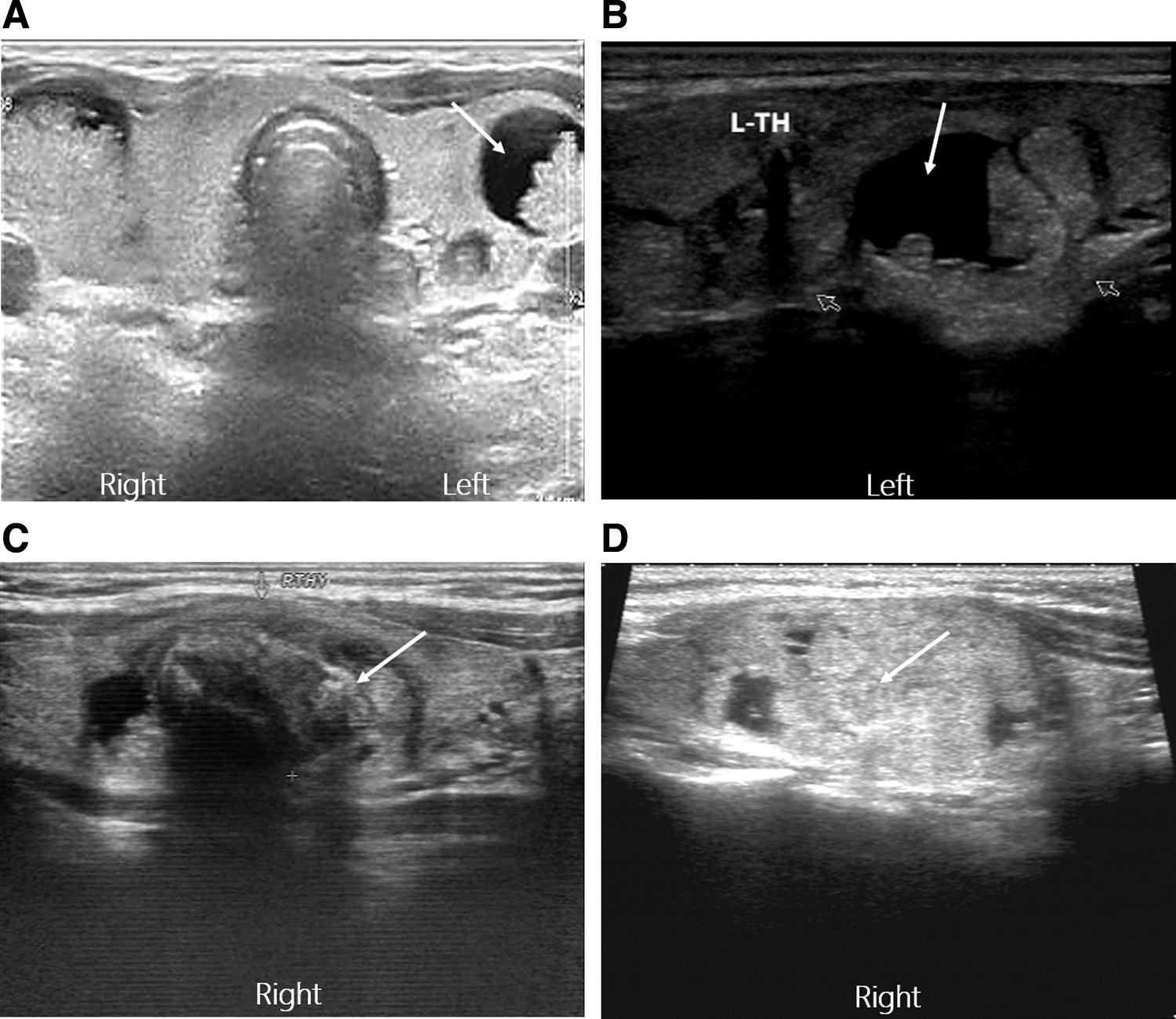
Ultrasonography of thyroid nodules with regrowth. (

Outcome of thyroid nodules with regrowth. FNAB, fine-needle aspiration biopsy; VRR, volume reduction ratio.
Identification of risk factors for technique efficacy and nodule regrowth and performance of subgroup analyses
By logistic regression analysis (Table 3), higher cystic components and higher vascular scores were found to be independent positive factors for technical efficacy, and the existence of bilateral nodules was an independent negative risk factor for technical efficacy. For thyroid nodule regrowth, bilateral nodules and nodules with lower vascular scores were more likely to regrow.
Logistic Regression Analysis for Technique Efficacy and Regrowth
CI, 95% confidence interval; OR, odds ratio.
On subgroup analyses (Table 4), treatment of nodules located in both lobes of the thyroid was found to correlate with VRR, technique efficacy and regrowth rate. Specifically, for bilateral nodules, there was a lower VRR (13.6% vs. 74.1%, p < 0.001), lower technical efficacy (56.3% vs. 90.7%, p = 0.001), and higher regrowth rate (68.8% vs. 9.3%, p < 0.001) compared with unilateral nodules.
Comparison of Volume Reduction Ratio, Technique Efficacy, and Regrowth Between Subgroups
Regarding nodal composition, nodules with a higher cystic component (≥50%) had a higher VRR (72.4% vs. 46.7%, p = 0.001) than nodules with a lower cystic component (<50%), but there were no statistical differences in technical efficacy (86.5% vs. 78.8%, p = 0.394) or regrowth rates (27.0% vs. 18.2%, p = 0.379).
For thyroid nodule vascularity, high vascular score was associated with a lower regrowth rate compared with the low vascular score group (12.1% vs. 32.4%, p = 0.043), but there were no differences in technical efficacy (87.9% vs. 78.4%, p = 0.462) or VRR (73.9% vs. 48.1%, p = 0.261).
Complications of RFA
The total complication rate was 4.8%. A major complication, that was, voice change, occurred in one patient, while minor complications, skin burn and hematoma, occurred in one case each, respectively. In addition, three patients complained of local pain after RFA treatment. All patients recovered well with no sequelae. No other complications or side effects were found during or after the procedure.
Discussion
To our knowledge, this is the first study of a large study cohort (70 nodules in 62 children) and long-term follow-up (≥4 years) on the use of RFA to treat benign nonfunctional thyroid nodules in children. There has been only one previous study of RFA for thyroid nodules in children; this study followed 12 patients for an average of three years (28).
In the treatment of benign thyroid nodules, the main purpose is the elimination of compressive symptoms and cosmetic concerns rather than the complete elimination of nodules. A VRR of at least 50% is generally considered to indicate successful treatment. In our study, the mean VRR values from all follow-up periods, from three months to four years, were >50%, and the technical efficiency rates were >80%. In addition, in these pediatric patients, since most of the nodules were not large and the symptom scores were not particularly high, improving cosmetic symptoms should be more important, especially in adolescent patients. In an adult study, RFA-treated patients were more satisfied with the improvement in cosmetic symptoms compared with surgical patients (31). In this study, RFA also significantly improved cosmetic symptoms. This suggests that the short- and long-term effects of RFA treatment are acceptable in most children. In the previous study of 12 children, the data also showed that RFA was effective. It should be noted that the data from the previous study are not directly comparable with ours (28), because VRR was not calculated in that study, and data were not collected at specific time intervals.
Although the majority of pediatric patients in our study had acceptable efficacy rates, the results did not appear to be as good as those for adults. The VRR and efficacy rate in this study reached a maximum at one year (77.5% and 91.4%) and decreased to 55.1% and 81.4%, respectively, at the four-year follow-up. In comparison, a multicenter Italian study of RFA for adult patients, which included a large sample size (n = 216) and a long follow-up period (≥5 years), the VRR values at follow-up, from years 1 through 5, were 72%, 75%, 76%, 76%, and 77%, respectively (10). Thus, the overall trend of VRR continued to rise steadily for adult patients. Similarly, in a meta-analysis (32), which included 12 studies of RFA treatment of thyroid nodules, the VRRs at follow-up were 68%, 75%, and 87%, respectively, showing an increasing trend in VRR with time. According to these results, the effect of RFA on adults seems to be better than that for children we found in the current study.
The main reason for this difference may be the regrowth of nodules in some pediatric patients over time, but the number of RFA sessions may also be considered as a reason: in the present study, VRRs were determined after the initial treatment, while in some other studies, the VRRs were determined after single or multiple RFA treatments (32). However, notably, in the Italian study (10), VRR data were collected after a single-session treatment, and the VRR at year-4 was better than in the present study (76% vs. 55.1%).
The majority of thyroid nodules (51.4%) had hyperechoic or strong echogenicity, and this disappeared within two years. It is worth noting that such echogenicity, although requiring long-term follow-up, does not indicate malignant transformation. Often, the strong echogenic foci that appear in the immediate postprocedural period are the result of gas produced during RFA treatment. Postprocedural ultrasound of necrotic tissue shows hyperechoic or strong echogenicity. This disappears when the necrotic tissue is absorbed.
Regrowth is an unsolved clinical problem in the treatment of thyroid nodules with RFA (33). In the current study, regrowth was defined as a volume >50% larger than the minimum volume after RFA. We found the overall regrowth rate was 22.9% in our study cohort, of which 56.3% of regrowth events represented loss of efficacy. In studies of RFA treatment of thyroid nodules in adult patients, regrowth rates ranged from 0% to 34% (21), and treated nodules were generally no larger than before ablation. However, in the present study, 66.7% of the nodules with VRR <50% became larger than before treatment. This may be the reason why the VRR at year-4 was worse than that in adults. Possible reasons for the observation of larger nodule volumes than before RFA treatment are as follows: first, the nodule growth rate was not in a stable state; second, RFA may stimulate the growth of the nodule; third, RF therapy is a technique and experience-dependent treatment, and the effect of treatment varies by provider; fourth, the late follow-up interval may be too long; and fifth, although the regrowth of nodules were benign on reassessment by fine-needle aspiration biopsy they may have been malignant (i.e., false-negative result).
In addition, it is worth noting that all nodules treated with a second RFA due to a loss of efficacy will eventually be expected to lose responsiveness, so the second RFA treatment for thyroid nodule regrowth in children may not be suitable. Of course, the sample size testing retreatment with RFA in this study was very small, so more prospective studies are needed to determine efficacy. In this study, most of the regrowth occurred in the third year, and in an adult study this also became more pronounced in the third year of follow-up (34). Therefore, we believe that active follow-up is necessary, at least three years for some patients, to detect any regrowth of nodules in a timely manner.
In this study, we found that bilateral nodules requiring treatment had lower VRRs, lower therapeutic efficacy and higher rates of regrowth, and the presence of bilateral nodules was an independent factor related to efficacy and regrowth. The specific reason for these associations is unclear. In addition, such results have not been reported in adult studies. Thus, RFA may not be appropriate for the treatment of bilateral thyroid nodules in children. In addition, we also found that the presence of more cystic nodules correlated with higher VRR, which was similar to findings from multiple adult studies (35 –39). In these studies, and in our study, nodules with a cystic component were aspirated to remove fluid before RFA. The volume of the nodules was not recalculated after aspiration.
This may account for the better efficacy. In addition, for cystic and predominantly cystic nodules, ethanol ablation remains the preferred treatment modality given its lower cost and high efficacy (25,40,41). We found that thyroid nodule vascularity was positively associated with efficacy. However, in the subgroup analysis, there were no differences in VRR and efficacy by thyroid nodule vascularity score. Commonly, increased vascularity leads to increased heat loss and decreased efficacy (42). The relationship between vascularity and efficacy needs to be further investigated.
Regarding safety, the use of RFA for adult nodules has proven to be safe. A meta-analysis, including 2786 nodules treated with RFA, showed that the overall complication rate of RFA for thyroid nodules (both benign and malignant) was 2.38% and the rate of major complications was 1.35% (43). The complication rate of our study was 4.8%, and none was permanent. Similar results were reported for the small pediatric study of Min Ji Hong (28). Thus, the short- and long-term safety profile of RFA in children appears to be satisfactory.
Overall, RFA has some advantages over surgical treatment. As a minimally invasive treatment, RFA produces less neck scarring. Patients are more satisfied with the improvement in cosmetic symptoms and have a better quality of life (44). RFA also has less impact on thyroid function, fewer major complications, and no life-threatening complications (45,46). RFA is mostly performed in outpatient settings, saving time and posing less risk of anesthesia, and in some countries, the cost may be lower (46). However, there are some non-negligible disadvantages of RFA compared with surgery. The most important is the regrowth of nodules (47). RFA treatment requires careful selection of nodules, for example, in this study, bilateral nodules with poor outcome may not be suitable for RFA treatment. In addition, RFA-treated patients require long-term follow-up (33,47).
In addition, the lack of pathological examination leads to the possibility that malignancy cannot be excluded. Equally important, this treatment requires specialized treatment centers, specialized equipment, and highly skilled and experienced physicians, so access to RFA may also be a barrier to its use (48). Therefore, we believe that RFA is more likely to be a complementary treatment modality to surgical treatment rather than an alternative in children with thyroid nodules.
There are some limitations of our study. For example, we did not use validated tools to assess endpoint events regarding quality of life, such as compressive symptoms and cosmetic issues. The current studies we compared our findings to are mostly from Asian studies of RFA treatment and not all were prospective studies (11,36,38,49). It will be important to use validated tools, such as the ThyPRO, to assess treatment effects (50 –52). The current study was retrospective and nonrandomized, and the findings will need to be confirmed by prospective studies. For instance, the recording of complications and side effects may be subject to a selection bias and their incidence may be underestimated. In addition, the study did not compare RFA results to those of traditional surgery or other thermal ablation treatments. Finally, some of the cases in the study were diagnosed only by fine-needle aspiration biopsy, and diagnoses in these cases were not confirmed by histopathological evaluation.
In conclusion, RFA was effective in reducing the volume of benign nonfunctional thyroid nodules in children, providing significant symptomatic relief with a good safety profile during short- and long-term follow-up. RFA should be considered as a beneficial, minimally invasive treatment modality for selected pediatric patients, but RFA may not be appropriate for the treatment of bilateral thyroid nodules in children.
Authors' Contributions
L.L.W. and Q.X.G. codesigned this experiment and participated in data collection and processing, article writing, and revision.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.