
Abstract
Background:
The incidence of thyroid disease is generally increasing, and it is subject to major geographic variability, between and within countries. Moreover, the incidence rates and the proportion of overdiagnosis for thyroid cancer in Italy are among the highest worldwide. This study aimed to estimate population-based frequency and trends of thyroidectomies in Italy by type of surgical procedure (total/partial), indication (tumors/other conditions), sex, age, and geographical region.
Materials and Methods:
Age-standardized rates (ASRs) of thyroidectomies were estimated from 2001 to 2018 using the national hospital discharges database.
Results:
In Italy, ASRs of thyroidectomies were nearly 100 per 100,000 women in 2002–2004 and decreased to 71 per 100,000 women in 2018. No corresponding variation was shown in men (ASR 27 per 100,000 men) in the overall period. A more than twofold difference between Italian regions emerged in both sexes. The proportion of total thyroidectomies (on the sum of total and partial thyroidectomies) in the examined period increased from 78% to 86% in women and from 72% to 81% in men. Thyroidectomies for goiter and nonmalignant conditions decreased consistently throughout the period (from 81 per 100,000 women in 2002 to 49 in 2018 and from 22 to 16 per 100,000 men), while thyroidectomies for tumors increased until 2013–2014 up to 24 per 100,000 women (9 per 100,000 men) and remained essentially stable thereafter.
Conclusions:
The decrease in thyroidectomies for nonmalignant diseases since early 2000s in Italy may derive from the decrease of goiter prevalence, possibly as a consequence of the reduction of iodine deficiency and the adoption of conservative treatments. In a context of overdiagnosis of thyroid cancer, recent trends have suggested a decline in the diagnostic pressure with a decrease in geographic difference. Our results showed the need and also the possibility to implement more conservative surgical approaches to thyroid diseases, as recommended by international guidelines.
Introduction
Thyroid diseases are increasingly being diagnosed across the world over the past three decades (1 –4). National and international clinical practice guideline recommendations directing the management of thyroid diseases are also rapidly changing (5 –7), with recent efforts aimed to reduce overuse of diagnostic procedures that may lead to resource waste (8,9), overdiagnosis (10,11), and overtreatment (12). Moreover, thyroid diagnostic tests are increasingly being used in many regions of the world (13,14), including some Italian areas (15). The increase in thyroid diagnostic testing has occurred in parallel with a large, although heterogeneous, rise in thyroid cancer incidence over the past three decades (11,16 –18).
Several authors have reported a large variability in the frequency and type of thyroid surgeries performed across regions and over time. In particular, variations of surgery rates across French regions have been observed (17), as well as across hospital referral areas in the United States, suggesting widely divergent beliefs and practice patterns for the management of thyroid nodules and cancer (19). Studies carried out in the first decade of the 2000s showed an increasing share of total thyroidectomies (TT) versus partial thyroidectomies (PT) both in the United States (20) and in Europe (21,22). However, population-based research on the frequency of thyroidectomies and type of surgical approach adopted is lacking in Italy. The Italian National Hospital Discharges database presents a unique opportunity to investigate thyroid surgical treatment, from 2001 to 2018, at national level.
The aim of this study was to estimate the geographical patterns and time trends of thyroidectomies in Italy across two decades, by type of procedure (PT or TT), discharge diagnosis (i.e., thyroid cancer and other thyroid diseases), sex, and age groups, thus adding real-world (i.e., population-based) information on the surgical management of thyroid diseases and adherence to guidelines in the last 20 years.
Materials and Methods
In Italy, a public welfare system guarantees universal health care. The National Health Service (NHS) is centrally organized under the Ministry of Health, and it is administered on regional basis. Hospitals (public and private ones) submit their health claims to the regional health authority for reimbursement. These claims are collected in a unique national database containing information at individual level (Hospital Discharges-HD database). Each record refers to a single hospital episode and includes demographic information (date of birth, sex, place of birth, place of residence), clinical information (main discharge diagnosis and up to five secondary discharge diagnoses, main intervention/procedure and up to five secondary interventions/procedures coded according to International Classification of Diseases, 9th Revision, Clinical Modification—ICD-9-CM), and administrative information (coded according to the Diagnosis Related Groups—DRG coding system and dates of admission and discharge). Since 1999 the Ministry of Health has applied data quality control procedures and annually publishes reports on completeness; all variables are mandatory.
In Italy, regional and national health authorities are legislated as collectors of personal data for surveillance purposes without explicit individual consent. Research ethics committee approval for research involving this database is not required for a descriptive analysis of anonymous aggregate data without any direct or indirect intervention on patients (Decreto del Presidente del Consiglio dei Ministri, March 3, 2017, Identificazione dei sistemi di sorveglianza e dei registri di mortalità, di tumori e di altre patologie, 17A03142, GU Serie Generale n.109 del 12-05-2017,
The HD database used for this analysis included all hospitalizations occurred in Italy from January 1, 2001 to December 31, 2018. We included in the analysis all hospitalizations owing to thyroid surgical interventions identified according to the following ICD-9-CM codes (23,24) in each procedure/intervention: 06.4, 06.50, 06.52 associated to TT; 06.2, 06.3x, 06.51 associated to PT (lobectomy and other procedures). Hospitalizations owing to thyroidectomy were then classified according to discharge diagnosis in three major groups: malignant thyroid cancers (ICD-9-CM: 193); thyroid neoplasms of uncertain behavior and thyroid adenomas (ICD-9-CM: 226, 237.4, 239.7); and goiter and other diagnoses (ICD-9-CM: 240–246). If a patient had more than one hospitalization owing to surgical procedure, all the hospitalizations were included in the analysis.
The following indicators were calculated: - Age-specific and age-standardized rates (ASRs per 100,000) of thyroidectomy (TT and PT combined); - Ratio between TT and PT (TT/PT ratio).
The European Standard Population was used for ASRs. Thyroidectomy rates and TT/PT ratio were stratified by sex and area of residence. Stratification by area was conducted by administrative regions or autonomous provinces and aggregated by four macro-areas: North-West (Liguria, Lombardia, Piemonte, Valle d'Aosta), North-East (Emilia-Romagna, Friuli Venezia Giulia, Trentino, Alto Adige, Veneto), Center (Toscana, Umbria, Marche, Lazio), and South and Islands (Abruzzo, Molise, Campania, Puglia, Basilicata, Calabria, Sicilia, Sardegna).
Time trends of ASR in 2001–2018, expressed as annual percentage change (APC) with 95% confidence intervals, were investigated by log-linear models; possible significant changes were assessed by the permutation test using the JoinPoint Regression Program (25).
Results
Between 2001 and 2018, a total of 542,143 and 162,380 thyroidectomies were reported in Italy for women and men, respectively, equally distributed in the three 6-year time periods: 2001–2006, 2007–2012, and 2013–2018 (Table 1). The mean age at surgical intervention was 52 years in women and 54 years in men, with a slight increase over the study period. In women, the percentage of TT among all thyroidectomies were higher for Center (88%) and South and Islands (88%) than for northern Italy (77%) and increased until 2012 (from 78% to 87% and from 72% to 83% in women and men, respectively) to stabilize thereafter. There was an increasing trend in the proportion of thyroidectomies due to malignant cancer for both sexes and in all areas of residence; it varied from ∼18% and 20% for women and men, respectively, in the period 2001–2006, to ∼28% and 31% for women and men, respectively, in the last period 2013–2018. The trend was similar in all areas even if lower proportions of thyroidectomies for tumors emerged in South and Islands in women and men.
Distribution of Total and Partial Thyroidectomies by Sex, Period, and Area of Residence—Italy, 2001–2018
Bold represents the overall period.
PT, partial thyroidectomy; TT, total thyroidectomy.
The age-standardized thyroidectomy rates by region in 2001–2018 are given in Figure 1. Overall rates of thyroidectomies were 87.7 per 100,000 women and 27.0 per 100,000 men. A wide (i.e., greater than twofold) heterogeneity in rates of thyroidectomies was observed across Italian regions, with the highest rates observed in southern regions and Lazio (central Italy), in both sexes, and lowest in all northern regions (except in Emilia-Romagna region).
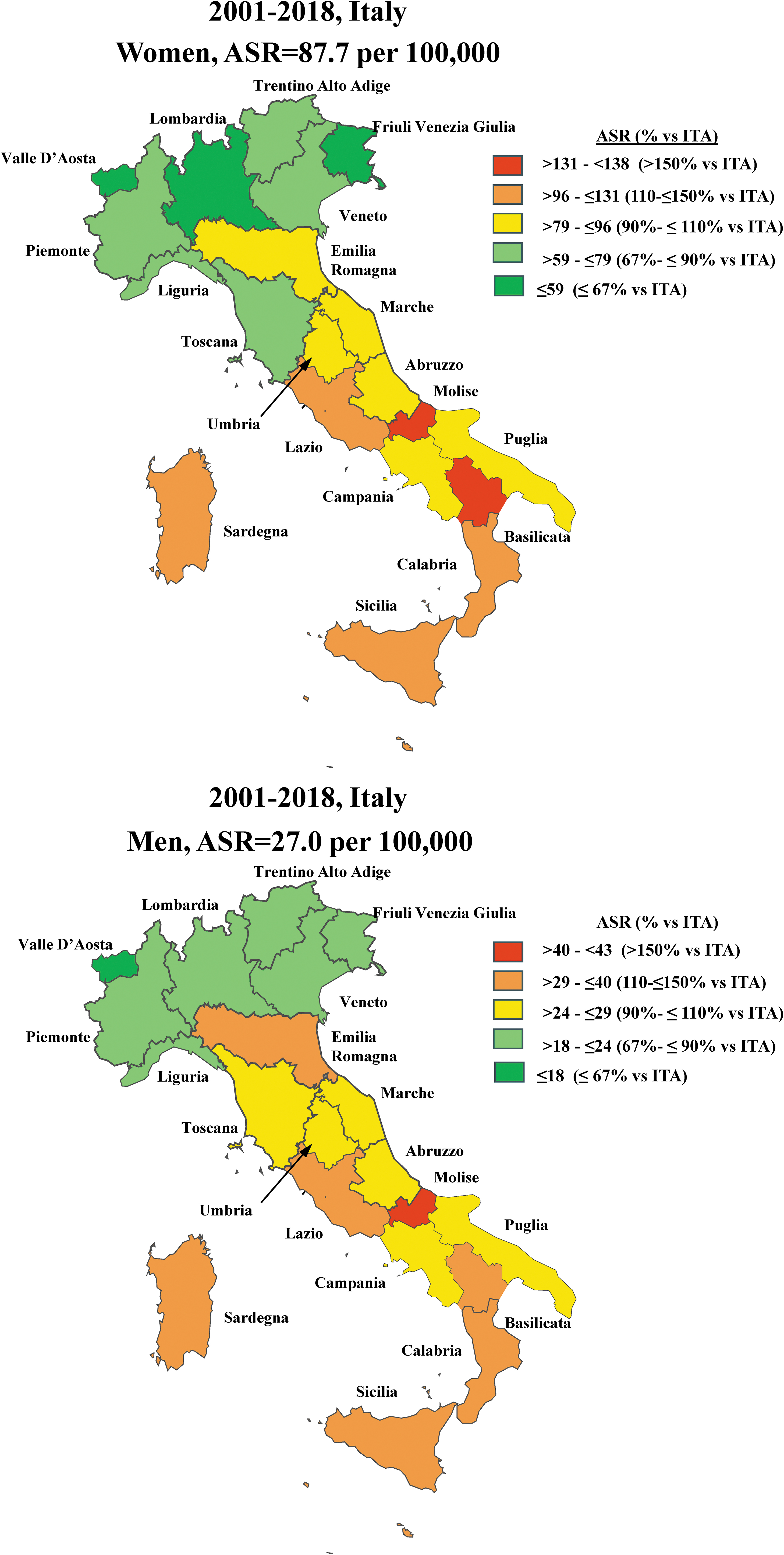
Age-standardized thyroidectomies (ASR) rates by sex and region of residence. Italy, 2001–2018.
The overall thyroidectomy rates by 5-year age classes and sex are given in Figure 2. Among women, the rate of thyroidectomies increased with age up to a level of ≥200 per 100,000 in the age class 45–64 years in the first period 2001–2006 and decreased in the subsequent periods. The highest rates of 192 and 155 per 100,000 in 2007–2012 and 2013–2018, respectively, were observed between 50 and 64 years of age. Among men, in the three periods examined, the rate of thyroidectomies increased with age up to a peak of between 70 and 74 per 100,000 men in the age class 55–64 years and decreased thereafter; curves of subsequent calendar periods overlapped.
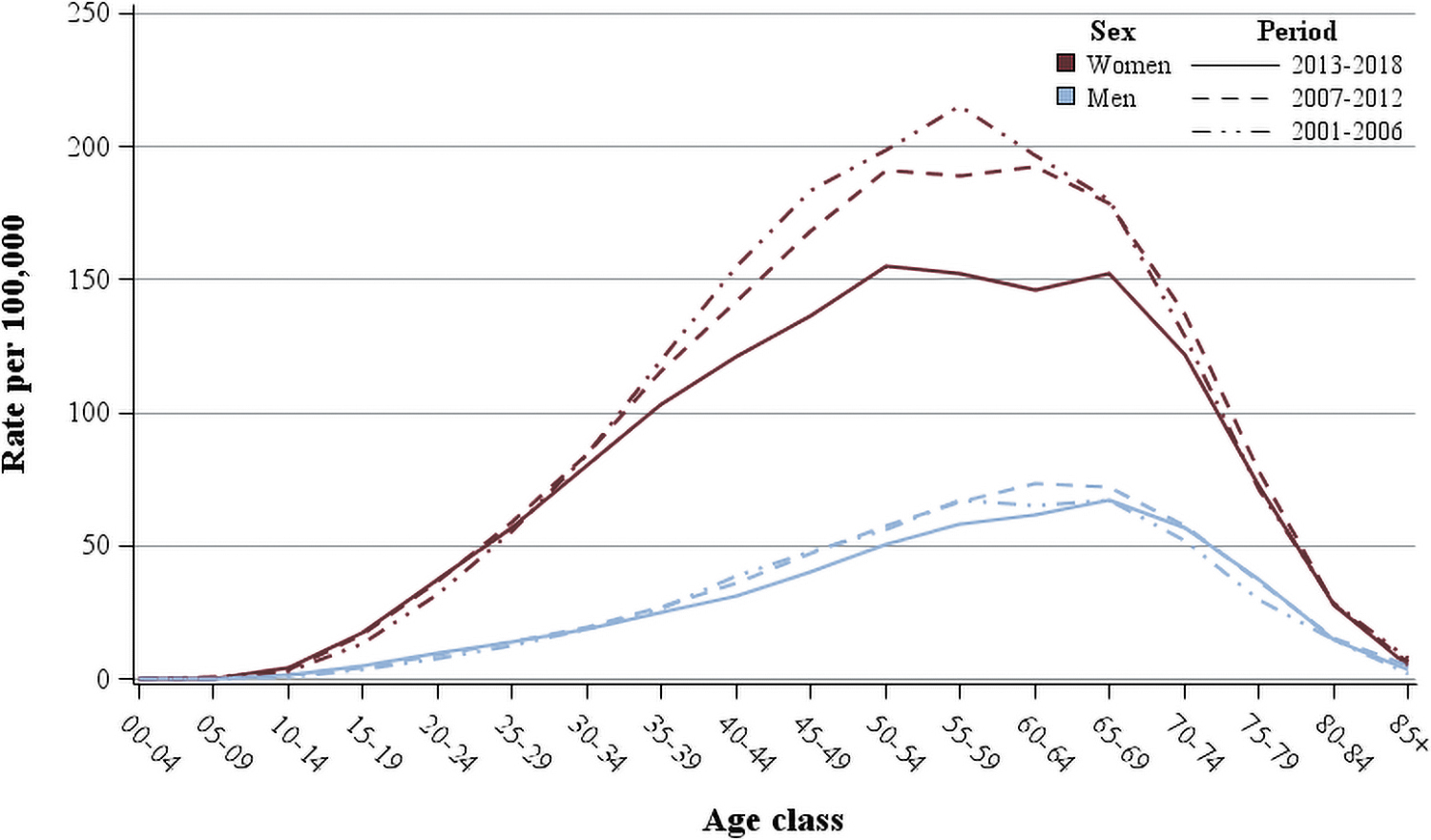
Age trends of thyroidectomies rates by period and sex. Italy, 2001–2018.
The time trends of ASR for thyroidectomy rates by sex and macro-area are given in Figure 3. ASRs were 95–98 per 100,000 women between 2002 and 2008, and gradually decreased to 71 per 100,000 women in 2018 (i.e., a decrease of ∼1 per 100,000 per year) (Fig. 3). In men, the ASRs were less than one-third those in women, that is, 27–29 per 100,000 men until 2013 and decreased to 24 per 100,000 men at the end of the study period. These trends were confirmed by the JoinPoint regression. For women the APC was +1.05 up to 2007 and −2.75 thereafter; for men the APC was +2.12 up to 2006, −0.33 up to 2013, and −3.55 thereafter.
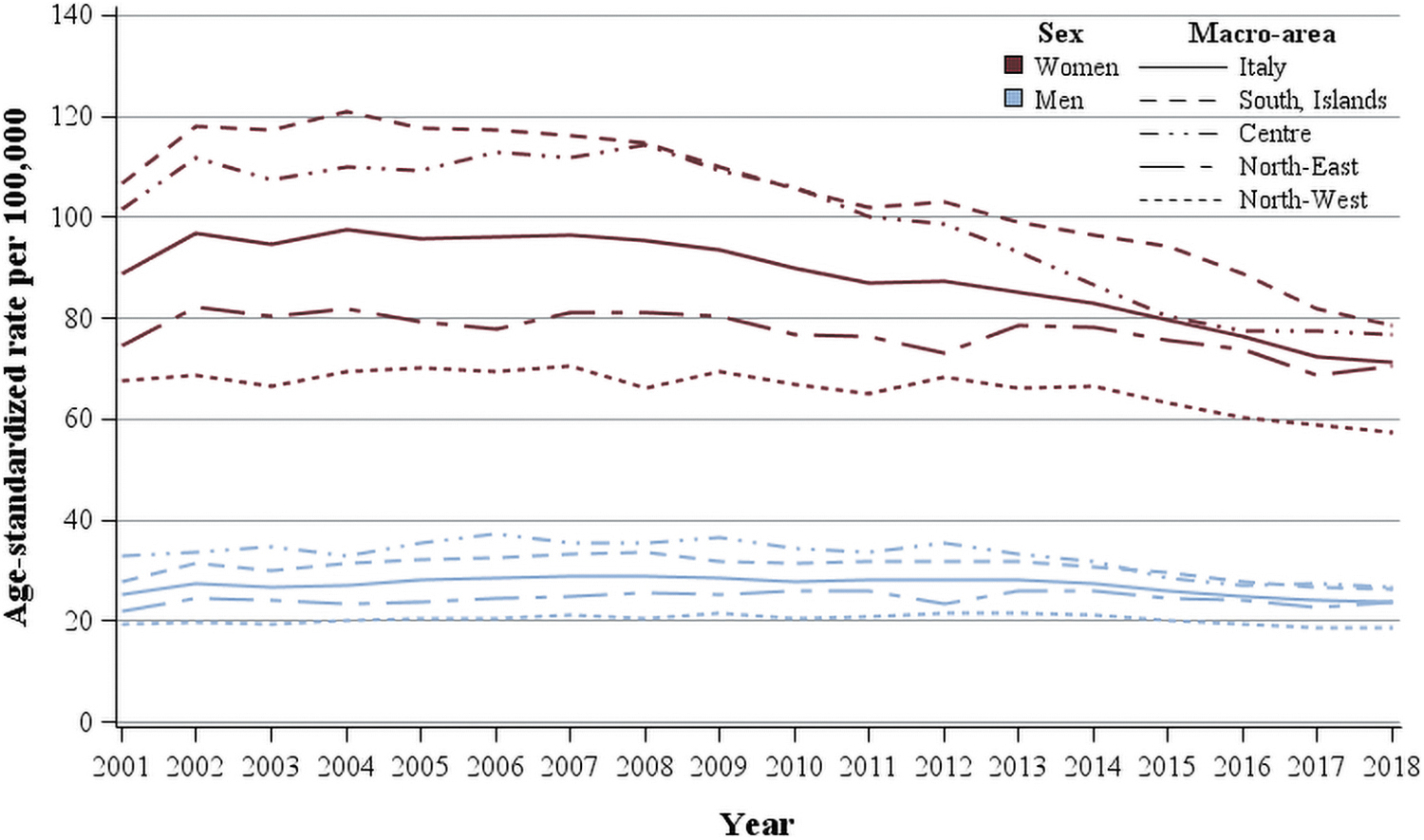
Time trends of ASR for thyroidectomies by sex and macro-area of residence. Italy, 2001–2018.
The frequency and type of thyroidectomy varied by macro-areas, north-western regions having the lowest levels of thyroidectomies (66 per 100,000 women and 20 per 100,000 men), followed by north-eastern regions (77 per 100,000 women and 25 per 100,000 men), central, and southern regions/islands (>100 per 100,000 women until 2011 and >30 per 100,000 men until 2014). The differences between macro-areas diminished during the study period as the decrease in thyroidectomies was most marked in central and southern Italy from 2010 onward.
Overall in Italy, TT/PT ratio steeply increased from 2001 (2.2 in women and 1.7 in men) to 2012 (7.8 and 5.4, in women and men, respectively) and decreased thereafter to 4.5 and 3.3 in women and men, respectively, in 2018 (Fig. 4). There was a marked geographical variation across regions with south and islands showing the highest TT/PT ratio (14.1 in women and 9.3 in men in 2012, that were reduced to 7.1 in women and 5.5 in men in 2018), followed by center (10.8 in women and 8.1 in men in 2012, decreasing to 5.4 in women and 4.2 in men in 2018) and northern regions, showing the same declining trend, but with TT/PT ratios <5 in women and <3 in men over the whole study period.
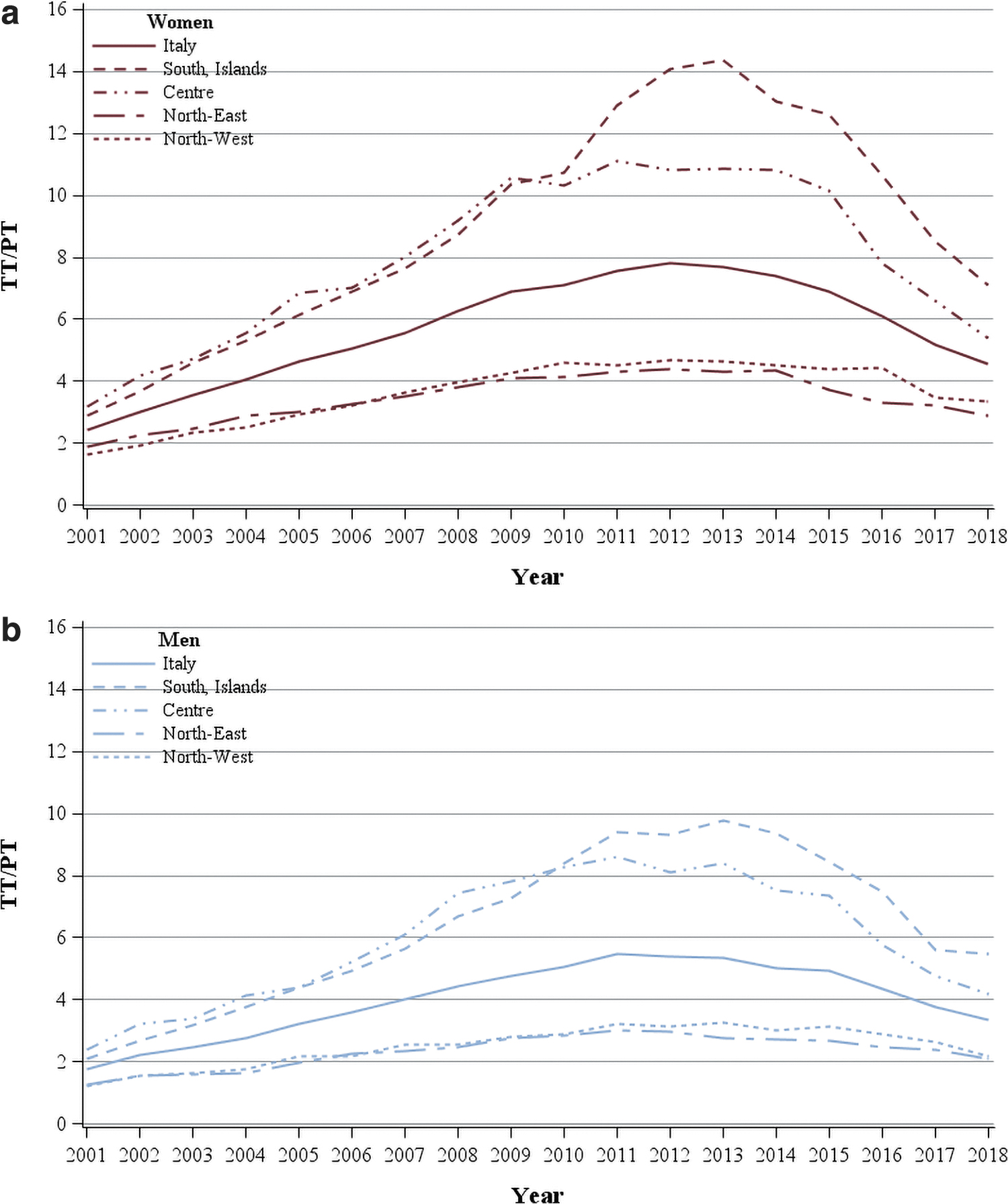
Time trends of TT/PT ratio by sex and area of residence: women (
The time trends of ASR of PT and TT by sex and discharge diagnosis in Italy are given in Figure 5. The thyroidectomy rates for malignant cancer increased until 2013–2014 up to 24.3 per 100,000 women (8.6 per 100,000 men) and remained essentially stable thereafter for men and women. Annual rates of thyroidectomies for benign or uncertain neoplasms slightly decreased in women (>7.5 per 100.000 women until 2007 and <7 after 2015), and they were lower and less variable during the all study period in men (i.e., between 2.1 and 2.6 per 100,000 men). Rates of thyroidectomy for goiter and other thyroid diagnoses decreased for both genders but a downward trend was particularly evident in women with rates >70 per 100,000 until 2004 and <50 after 2015. Meanwhile, TT/PT ratio increased from 2001 to 2012 in women and men for all discharge diagnoses and decreased thereafter (data not shown).

Time trends of ASR of thyroidectomies by sex and discharge diagnosis. Italy, 2001–2018.
Discussion
During the 2001–2018 period a total number of 704,523 thyroidectomies were performed in Italy, corresponding to ∼40,000 per year. Thyroidectomy rates decreased over time, especially among women where they were ∼3 times more frequent than among men (the women-to-men ratio slightly decreased from 3.6 in 2001–2006 to 3.1 in 2013–2018), with a peak of 1.5–2 surgeries per 1000 women at age 55–59 years.
The frequency of thyroidectomies varied also by geographical areas and in terms of surgical approach, with southern and central regions having had 50% more surgeries and a three times higher TT/PT ratio than northern regions. The TT/PT ratio increased from 2001 to 2012 and decreased thereafter. At the same time, the distribution of surgeries by discharge diagnosis changed; thyroidectomy rate related to malignant cancer increased, whereas rate related to goiter and other diseases decreased.
To date, population-based studies on thyroidectomies were mainly limited to the United States, where, from 2006 to 2011, surgeries for thyroid nodules (benign and malignant) increased from 99,600 to 130,200; the number of TT showed a 12% yearly increase, whereas the number of PT did not change significantly (16). This shift toward TT was observed for benign thyroid diseases in 1993–2007 (26) as well as for thyroid cancer in 1978–2004 (27). An overall increase in the number of thyroid surgeries with a shift toward TT was shown also in Illinois, United States, in the period 1999–2009 (20). More recently, a hospital-based study showed an opposite trend with an increase of PT related to malignant cancer diagnosis after the release of the 2015 American Thyroid Association (ATA) guidelines on management of differentiated thyroid cancer and thyroid nodules in adults (28). A similar pattern of PT related to benign and malignant thyroid diseases was also observed in a study based on medical claims (29).
Rates of thyroidectomies in this study (i.e., 87.7 per 100,000 women and 27.0 per 100,000 men, including all ages) were comparable with those presented in the United States among US Medicare beneficiaries (19) aged 65 years or older (i.e., 60 per 100,000, men and women combined) and in France (∼50 per 100,000, all ages, men and women combined) (17).
Only sparse data are available outside the United States. In England, hospitalizations owing to thyroid surgery increased from 7,726 in 1997–1998 to 12,019 in 2011–2012, especially those related to cancer diagnosis (30). In Wales, in the period 1999–2010, the overall thyroidectomy rates declined, whereas thyroidectomies performed for cancer and TT for benign thyroid diseases increased (21). In Denmark, thyroidectomies for benign thyroid diseases slightly declined in 1990–2007, with a growing percentage of TT (31). In Taiwan, in the period 1996–2010, <20% of thyroidectomies were TT, the other being lobectomies and other partial procedures (32).
Overall, findings from this study confirmed other European studies showing an increased number of thyroidectomies because of cancer and an increasing resort to TT at least over the first decade of 2000. In Italy, however PT relatively increased a few years before the publication of ATA guidelines (5), probably because more conservative guidelines and recommendations were anticipated by caveats from authoritative meetings and publications (15).
The disposition toward TT versus PT can be explained by both the evolution of guidelines suggesting a less aggressive approach (5,33 –36) and the observation that, although recurrence may occur in nearly a quarter of patients with benign thyroid nodules or microcarcinomas treated with PT (37), PT in selected well-differentiated thyroid carcinomas does not impair survival and diminish surgical and medical complications that can affect patients' lifelong quality of life (38).
Data available on the changing prevalence of benign thyroid diseases in Italy are limited and mainly based on repeated surveys carried out in small areas. The spread of iodized salt consumption in Italy after 2005 has probably contributed to the decrease of iodine deficiency (39) and the prevalence of goiter and non-autoimmune hyperthyroidism observed in the last two decades (40). Since the reduction in iodine deficiency involved the whole national territory (39), it is unlikely that iodine deficiency played a major role in the observed geographical variation in thyroidectomies in Italy and the variations in thyroid cancer incidence (10,41) and mortality (42). The observed reduction in thyroidectomy rates, particularly among women aged 30–69 years, may therefore be the consequence of both the reduction in goiter prevalence and changes in treatment of benign thyroid diseases, such as nonfunctioning thyroid nodules and toxic goiters, which during the recent years were less commonly referred to surgery. In particular the development of new therapeutic strategies, such as thermal ablation and laser treatment, and the publication of clinical guidelines suggesting the use of the above-mentioned procedures, as well as of medical treatment and/or radioiodine for toxic goiters can have played an important role (43 –46).
In the more recent study period, the upward trend in thyroidectomies for cancer leveled off in Italy. Declines in diagnostic pressure, particularly the use of fine-needle aspiration biopsies of thyroid nodules, was already observed in some Italian areas after 2014 (15) and so was active surveillance and minimally invasive treatments of thyroid microcarcinoma (47,48). These favorable trends might lead to further reductions of unnecessary thyroidectomies (49) and repeated surveillance of the phenomenon is warranted (50).
The main strength of the study is that the national HD database collects data from all Italian public and affiliated private facilities, including day hospitals, and thyroidectomy is not administered in outpatient settings in Italy. Therefore, the availability of almost two decades of hospitalization data at the national level provided a unique opportunity to study changes in frequency of thyroidectomies in Italy by type of intervention and discharge diagnosis.
We acknowledge several important limitations. First, the HD database included administrative data that are susceptible to coding errors. In Italy, the diagnoses are coded on hospital record using the information available at patient discharge, at this time histology might have not been assessed. Therefore, there could be a proportion of thyroid cancers that are incidentally discovered during surgery for goiter and classified as benign thyroid disease. This might have affected trends of surgeries by indication; however, such impact was probably negligible in the study period. This problem has been already acknowledged in previous European analyses of thyroid surgeries from discharge records (22,51). Population-based figures on incidentally discovered thyroid cancers are rarely reported in the international literature (e.g., ∼14% in Queensland, Australia in 2013–2016) (52), and not reported in the Italian literature. Nonetheless, studies from Italian tertiary care institutions demonstrated a high prevalence of incidental papillary microcarcinoma already in the mid-2000s (53).
Furthermore, hospital records do not include information about the reasons for choosing the surgical approach: TT versus PT, that is, if the decision is exclusively based on the patient's clinical conditions or if it derives from the consultation between clinician and patient. As future development, the HD database could be also used to investigate thyroid surgical complications and postsurgical radioactive use.
In Italy, the ATA clinical practice guidelines on thyroid care are generally followed. Recently, a consensus of six Italian scientific societies provided recommendations on management of differentiated thyroid cancer (7). Yet, a recent study (50) evaluated the impact on clinical practice of ATA guidelines, showing that Italian practices were characterized by a limited use of thyroid lobectomy. The dissemination and implementation of guideline recommendations (7), and change in practice patterns, require some time.
In conclusion, the substantial variations in the frequency of surgical procedures for thyroid diseases have been present in the last two decades across otherwise similar Italian areas. These findings demonstrate the need for a reappraisal of thyroidectomy practice (in particular TT) in the direction of a full implementation of less aggressive approaches consistent with recent national and international guidelines and recommendations (5,7,43).
Data Availability
Dataset supporting our findings is available, upon reasonable request, by the corresponding authors.
Ethics Approval and Consent to Participate
The Italian legislation identifies regional and national health authorities as collectors of personal data for surveillance purposes without explicit individual consent. The approval of a research ethic committee is not required, because this study is a descriptive analysis of anonymous aggregate data without any direct or indirect intervention on patients (Decreto del Presidente del Consiglio dei Ministri, 3/3/2017, Identificazione dei sistemi di sorveglianza e dei registri di mortalità, di tumori e di altre patologie, 17A03142, GU Serie Generale n.109 del 12-05-2017). Available at:
Footnotes
Acknowledgments
The authors thank Mrs. Luigina Mei for editorial assistance. Members of the Diagnostic Examinations and Pathway of THyroid diseases (DEPTH) Working Group: Francesco Avossa (Epidemiological Department, Azienda Zero, Padua, Italy); Rossana De Palma (Emilia Romagna Region); Rosa Vattiato (Romagna Cancer Registry); Andrea Polverino (Trento Province); Fabio Vittadello (South Tyrol Cancer Registry); Giuseppe Fanetti (CRO, Aviano, Italy).
Authors' Contributions
D.P., U.F., and L.D.M. drafted the study protocol and designed the study with the support of S. Francisci and S. Franceschi. A.D.P., D.S., E.D.F., F.F., S.Fe., P.G.R., G.M., S.P., F.T., M.V., and M.Z. revised the study protocol. D.P. and S. Francisci collected data for the study database and did the statistical analyses with the support of U.F., A.D.P., V.M., and L.D.M. D.P., U.F., S. Francisci, A.D.P, and L.D.M. drafted the article. R.E., C.G., E.B., G.Z., and S.V., specifically discussed clinical implications of study results. All authors contributed to the interpretation of study results, reviewed, and approved the final version.
Author Disclosure Statement
The authors have declared no competing interests.
Funding Information
This work was supported by the Italian Association for Cancer Research (AIRC; Grant No. 21879) and by the Italian Ministry of Health (Ricerca Corrente, RCR-2020-23670066, Alliance Against Cancer: Overdiagnosis, overtreatment, and outcome in cancer patients, WP 7). The funding sources had no involvement in the study design, in the collection, analysis, and interpretation of data, in the writing of the report, and in the decision to submit the article for publication.