
Abstract
Background:
With the emergence of mutation-based systemic therapies for patients with advanced thyroid cancer, molecular profiling has become an important component of care. Although next-generation sequencing (NGS) gene panels are accessible to clinicians, there is no consensus on the optimal approach to testing. This study investigates the clinical application of NGS results in the management of advanced thyroid cancer.
Methods:
Patients with advanced thyroid cancer with NGS completed as part of the Integrated Molecular Profiling in Advanced Cancers Trial (IMPACT; NCT01505400) or Ontario-wide Cancer TArgeted Nucleic Acid Evaluation (OCTANE; NCT02906943) clinical trials at the Princess Margaret Cancer Centre were included. Electronic medical records were reviewed to collect clinicopathologic and treatment data. The OncoKB framework was used to categorize molecular alterations based on levels of actionability. Patients with an actionable alteration by OncoKB framework who had treatment with a drug targeting the alteration were categorized as receiving “matched” therapy. Time-to-event data were analyzed using the Kaplan–Meier method. This study was approved by the University Health Network Research Ethics Board (ID# 19-5888).
Results:
NGS was performed on 118 patients with advanced thyroid cancer between 2013 and 2020. The most common molecular alterations included BRAF V600E (62%) and NRAS (15%) mutations in papillary thyroid cancer, RET alterations (78%) in medullary thyroid cancer, and BRAF V600E (38%) and TP53 (62%) mutations in anaplastic thyroid cancer. Actionable alterations were found in 87% of patients, and 57% of patients had at least one Level 1 or 2 alteration for which Food and Drug Administration (FDA)-approved drug is available. BRAF and RET alterations made up 86% of Level 1 and 2 alterations. A matched therapeutic approach was undertaken in 13% of patients.
Conclusion:
This study uses a structured framework to analyze the actionability and clinical use of NGS results in advanced thyroid cancer. Most patients had at least one potentially actionable mutation and 57% of patients had at least one Level 1 or 2 alteration, predominantly driven by BRAF V600E and RET alterations. This study rationalizes the need for routine multigene NGS testing or reflex BRAF and RET testing in the management of patients with advanced thyroid cancer.
Introduction
The global incidence of thyroid cancer has increased in the past 30 years, with an estimated 586,000 new cases diagnosed in 2020 (1,2). Although most thyroid cancers are curable with surgery, with or without adjuvant therapy, a subset of patients will develop distant metastatic disease requiring systemic treatment.
Currently, systemic therapies for advanced thyroid cancers mostly consist of multitargeted tyrosine kinase inhibitors such as lenvatinib or sorafenib for differentiated follicular cell-derived carcinomas, and vandetanib or cabozantinib for medullary thyroid cancer (MTC) (3 –6). In recent years, there has been an increased emphasis on personalized or “precision medicine” treatment approaches in oncology, aiming to identify an oncogenic driver specific to an individual's cancer and use a genotype-matched therapy. Examples of targeted treatment in advanced thyroid cancer include BRAF inhibitors in patients with a BRAF V600E mutation, and RET inhibitors for RET-altered cancers (7 –10). Hence, molecular characterization has become a crucial part of care, with direct implications on treatment decisions.
Next-generation sequencing (NGS) is an attractive method of molecular testing, allowing for rapid parallel sequencing of multiple genes while minimizing the amount of tissue required. NGS panels are becoming increasingly accessible to clinicians, with commercially available assays. Despite the ability to do this testing, NGS is not yet standard of care for all cancer patients in Canada or many other jurisdictions. Recent European Society of Medical Oncology (ESMO) guidelines for NGS in metastatic cancers do not provide a definitive recommendation for multigene panel testing, stating that this “could be ordered, considering the benefit for the patient and the cost for the public health care system,” leaving the final decision to the physician and patient (11).
It is difficult to quantify the likelihood that NGS will change a patient's treatment plan, and the direct implications of NGS findings on treatment and outcomes remain undefined. There is no consensus on the optimal testing approach in advanced thyroid cancer, and different society guidelines have differing recommendations (11 –16). Studies are needed to inform the optimal use of this technology in the routine care of patients with thyroid cancer. In this study, we aim to (a) characterize the frequency and nature of molecular alterations in advanced thyroid cancer and (b) investigate the actionability and clinical application of NGS findings in the current treatment landscape to guide recommendations for testing approaches.
Methods
Patient cohort
This study was approved by the University Health Network (UHN) Research Ethics Board (ID# 19-5888). All patients with advanced (defined as unresectable locally advanced or distant metastatic disease) thyroid cancer referred to medical oncology for systemic therapy who had NGS performed at the Princess Margaret Cancer Centre as part of the Integrated Molecular Profiling in Advanced Cancers Trial (IMPACT; NCT01505400) or Ontario-wide Cancer TArgeted Nucleic Acid Evaluation (OCTANE; NCT02906943) clinical trials between 2013 and 2020 were included. The protocols for IMPACT and OCTANE have previously been described (17,18).
In brief, these trials enrolled patients with advanced incurable solid tumor cancers receiving palliative treatment and performed targeted panel sequencing on archival tumor samples (previously collected biopsy or surgical specimens). Electronic medical records were reviewed to collect data, including baseline patient demographics, clinicopathologic characteristics, treatment and follow-up information. For differentiated thyroid cancer (DTC) patients, radioactive iodine (RAI) refractoriness was defined as meeting at least one of the following: (a) structural disease without uptake on 131I scan; (b) structural tumor progression within 12 months of 131I therapy; or (c) cumulative dose of 131I > 600 mCi (19). Structural disease progression was defined according to the response evaluation criteria in solid tumors (RECIST) version 1.1 criteria (20).
Next-generation sequencing
IMPACT used extracted tumor deoxyribonucleic acid (DNA) on the TruSeq Amplicon Cancer Panel (TSACP; Illumina) on the MiSeq sequencer (Illumina, San Diego, CA, USA). The TSACP was targeted to hotspot regions in the 48 genes, and would not detect large deletions or insertions (> 25 bp), gene amplifications or loss, or fusions. Two panels were used for OCTANE: the UHN Hi5 Panel, which examined tumor DNA for 555 genes using SureSelect Target Enrichment hybrid capture (Agilent, Santa Clara, CA, USA) with paired-end sequencing on the Illumina platform (NextSeq550, San Diego, CA, USA), and Oncomine Comprehensive Assay v3, which is a 161-gene panel (Thermo Fisher Scientific, Waltham, MA, USA) examining DNA and ribonucleic acid (RNA) sequenced on the Ion S5 XL platform (Thermo Fisher Scientific).
The Hi5 Panel analyzed exonic coding regions and 5 bp of intron flanking exons for targeted genes, with detection of single nucleotide substitutions and small insertion/deletion variants (<25 bp) to a lower limit of variant allele fraction of 5%, using a custom bioinformatics script with alignment to genome build GRCh37/hg19. Large deletions or insertions (>25 bp), gene amplifications or losses, and fusions were not detectable by the Hi5 Panel. The Oncomine Comprehensive Assay v3 analyzed regions of 161 genes, with coverage of hotspot regions in oncogenes, full gene analysis in tumor suppressor genes, fusion analysis for common fusion partners, and copy number variants in genes with reported copy gains or losses.
Sequence variants (single nucleotide substitutions, small insertions and deletions <25 bp) were detectable to a lower limit of variant allele fraction of 5%. Copy number variants were detectable if below the lower threshold of 0.5 copies, or above upper threshold of 4 copies. Gene fusions were reported if the established acceptable read count threshold of >50 read counts with the specific fusion was met. Analysis used the Oncomine Variant Annotator to annotate variants in Ion Reporter 5.6 (Thermo Fisher Scientific).
Actionability and genotype-matched therapy
The OncoKB Therapeutic Levels of Evidence V2 framework was used to classify alterations by actionability (21). Level 1 represents an “FDA-approved biomarker predictive of response to an FDA-approved drug for the indication,” Level 2 is a “standard care biomarker predictive of response to an FDA-approved drug,” Level 3 is “compelling clinical evidence supporting the biomarker as being predictive of response to a drug,” and Level 4 is “compelling biological evidence supporting the biomarker as being predictive of response to a drug.” In our study, patients with an alteration classified as actionable by the OncoKB framework who had treatment with a drug targeting the actionable alteration were categorized as receiving “matched” therapy.
Statistical analysis
Time-to-event data were analyzed using the Kaplan–Meier method. Overall survival (OS) was defined as the time from first consultation with a medical oncologist to the time of death or last follow-up. Differences in OS across tumor histology groups were assessed using the log-rank test.
Results
Patient characteristics
In total, 131 consecutive patients with advanced thyroid cancer were consented for IMPACT or OCTANE at the Princess Margaret Cancer Centre from 2013 to 2020. Of these, 13 patients were excluded for screen failure mostly due to insufficient or inadequate tissue, leaving 118 who underwent NGS (Fig. 1). Baseline clinicopathologic characteristics at the time of first medical oncology consultation are shown in Table 1. The median age at initial diagnosis was 53 years, and 59% were male. Tumor histology was papillary thyroid carcinoma (PTC) in 52% (N = 61), follicular thyroid carcinoma 3% (N = 3), oncocytic (Hürthle cell) thyroid carcinoma 1% (N = 1), poorly differentiated thyroid carcinoma (PDTC) 14% (N = 17), anaplastic thyroid carcinoma (ATC) 11% (N = 13), and MTC 19% (N = 23).
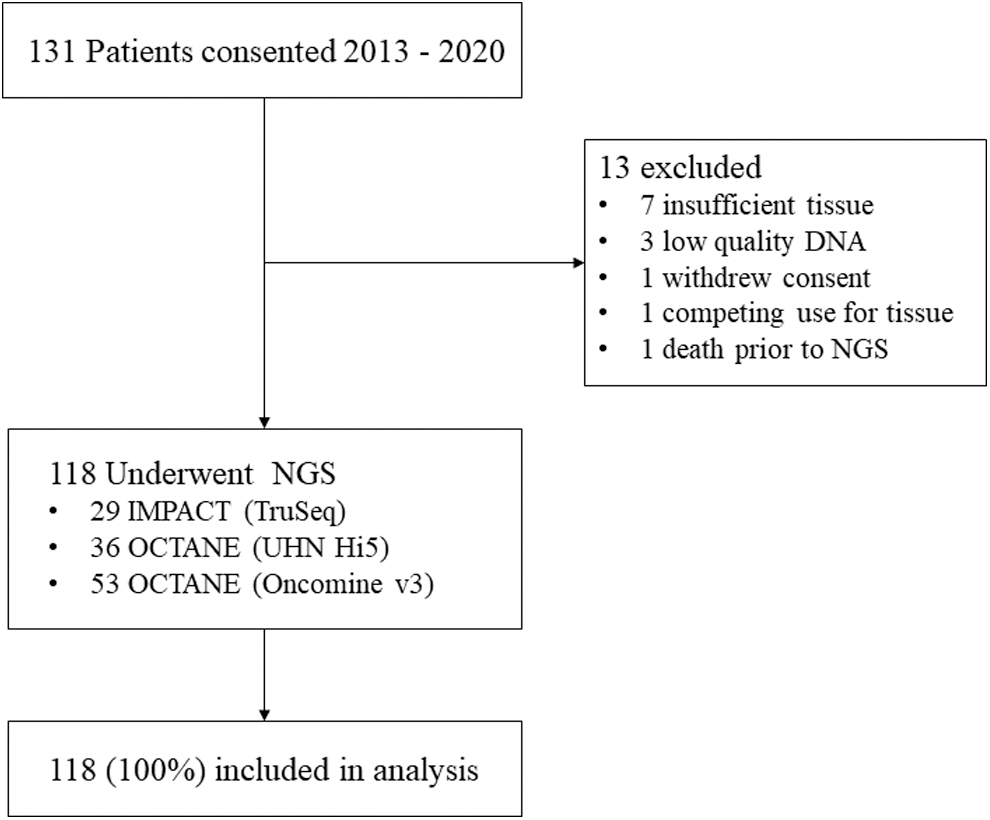
Enrollment, NGS molecular profiling, and analysis. NGS, next-generation sequencing.
Clinicopathologic Characteristics of Advanced Thyroid Cancer Patients
ECOG Performance status.
RAI; differentiated thyroid cancer patients only.
RAIR, as defined as meeting at least one of the following criteria: (a) disease without uptake on 131I scan, (b) progression within 12 months of 131I therapy, or (c) cumulative dose of 131I > 600 mCi.
ECOG, Eastern Cooperative Oncology Group; RAI, radioactive iodine; RAIR, radioactive iodine refractory.
Within the poorly differentiated and anaplastic carcinomas, a well-differentiated thyroid carcinoma (WDTC) was present in 43%. Distant metastases were present in 96% of patients at enrollment. Sites of disease at initial medical oncology consultation were lung (76%), locoregional (52%), lymph node (32%), and bone (19%). At the time of last follow-up, 89 patients (75%) had been treated with systemic therapy (Table 2). Of DTC patients, 88% were RAI refractory at enrollment. The most commonly used first-line therapy in DTC was lenvatinib (66% of patients who received treatment), while vandetanib was the most common first-line treatment in MTC (87% of patients who received treatment). The median follow-up time for all patients was 3 years [confidence interval; CI 0–14.4]. The median OS for WDTCs was 6.5 years [CI 5.7–10.2], MTC 10.6 years [CI 4.4–14.4], PDTC 4.3 years [CI 3.1–4.3], and ATC 0.9 years [CI 0.5–1.5] (Fig. 2).
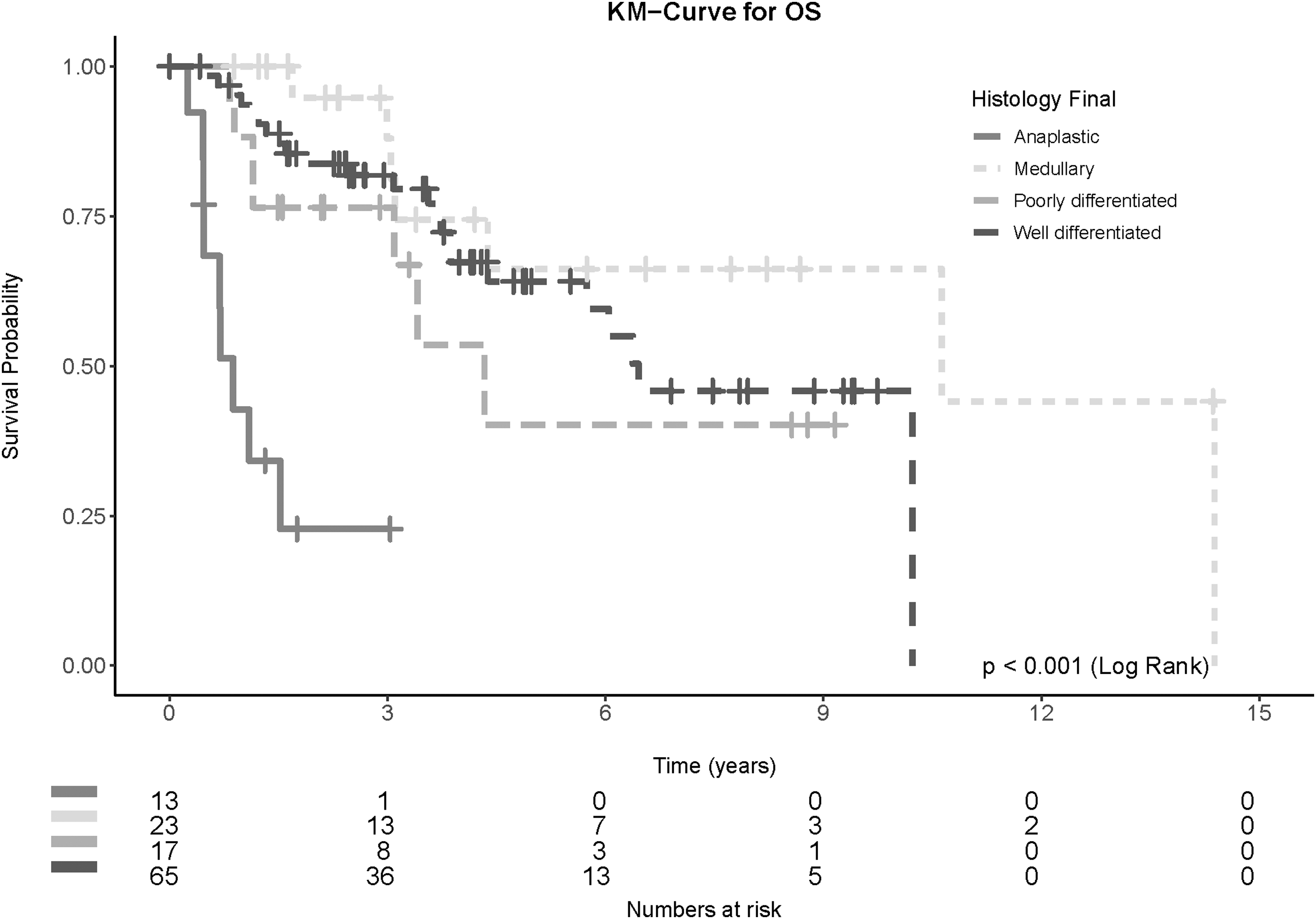
OS of advanced thyroid cancer patients by histological type. OS, overall survival.
Treatment Characteristics of Advanced Thyroid Cancer Patients Receiving Systemic Therapy
NGS findings
Patients underwent NGS as part of the IMPACT (N = 29) or OCTANE (N = 89) clinical trials (Table 3). Samples used for NGS were the primary tumor in 58% (N = 68) and metastasis in 42% (N = 49). The common pathogenic alterations are displayed in Table 4. A complete list of pathogenic alterations is found in Supplementary Table S1.
Next-Generation Sequencing Usage Characteristics in Advanced Thyroid Cancer
NGS, next-generation sequencing; UHN, University Health Network.
Common Pathogenic Genomic Alterations According to Tumor Type
Some tumors had multiple alterations in tumor suppressor genes, thus numbers do not add up to 100%.
ATC, anaplastic thyroid carcinoma; DNA, deoxyribonucleic acid; MTC, medullary thyroid cancer; PDTC, poorly differentiated thyroid carcinoma; WDTC, well-differentiated thyroid carcinoma.
The most common pathogenic alterations in WDTC (N = 65) included BRAF V600E (62%; N = 40), and NRAS mutations (15%; N = 9 NRAS Q61R and N = 1 NRAS G13R), which were mutually exclusive. TERT promoter mutations occurred in 14% of patients (N = 9), of whom 7 had a co-occurring BRAF V600E mutation. One patient without BRAF or RAS mutation was found to have an ETV6::NTRK3 fusion.
The predominant molecular alterations in PDTC (N = 17) included mutations in RAS (53%; N = 8 NRAS and N = 1 HRAS) and TP53 (N = 4; 24%). Two patients had rare non-V600E BRAF mutations (BRAF K601E and BRAF G469A).
In patients with ATC (N = 13), the frequency of BRAF V600E mutations was 38% (N = 5), RAS 23% (N = 2 HRAS, N = 1 NRAS), TP53 62% (N = 8), and TERT promoter 8% (N = 1). The patient with the TERT promoter mutation also had synchronous BRAF V600E and TP53 mutations. Other common alterations included mutations in the PI3K/PTEN/AKT/mTOR signaling pathway (N = 5; 38%) and NF1/2 mutations (N = 5; 38%).
In MTC, RET mutations were present in 78% (N = 18) of patients. RAS mutations were found in four of the five MTC patients who were RET wild type (N = 3 HRAS Q61R, N = 1 KRAS Q61R).
Clinical actionability and matched targeted therapies
In total, 87% of patients (N = 103) had at least one potentially actionable alteration. Using the OncoKB Therapeutic Levels of Evidence V2 framework, 20% of patients (N = 24) had a Level 1 alteration, 36% (N = 43) Level 2, 23% (N = 27) Level 3, and 7% (N = 8) Level 4 as their highest level of actionability. Multiple potentially actionable alterations were found in 15% of patients (N = 18). Level 1 alterations included RET-altered MTC (N = 18), BRAF V600E-mutated ATC (N = 5), and ETV6::NTRK3 fusion-driven WDTC (N = 1). Level 2 alterations included BRAF V600E mutations (N = 40), PIK3CA mutations (N = 5), BRCA1/2 mutations (N = 2), and TSC2 mutations (N = 2). Level 3 alterations involved NRAS (N = 20), HRAS (N = 9), AKT1 (N = 2), and BRAF K601E (N = 1). Level 4 alterations included mutations in PTEN (N = 7), CDKN2A (N = 3), NF1 (N = 3), ATM (N = 2), CDK12 (N = 1), BRAF G649A (N = 1), and an FGFR1 fusion (N = 1).
Based on NGS results, a matched targeted therapeutic approach was undertaken in 13% (N = 15) of patients (Table 3). Patients receiving matched therapy had PTC (N = 6), ATC (N = 6), or MTC (N = 3). Genomic alterations targeted included BRAF V600E mutations (N = 10), RET mutations (N = 3), NF1 mutation (N = 1), and MSH6 deletion (N = 1). BRAF therapy was given in the first-line in seven patients, second-line in two patients, and third-line in one patient. Treatment duration on matched therapy is displayed in Figure 3. Of patients with a Level 1 or 2 alteration who did not receive matched therapy (N = 52), 13% (7/52) died before a targeted drug was available, 35% (18/52) remain on active surveillance and have not yet started systemic therapy, and 25% (13/52) are still receiving first-line lenvatinib or vandetanib.
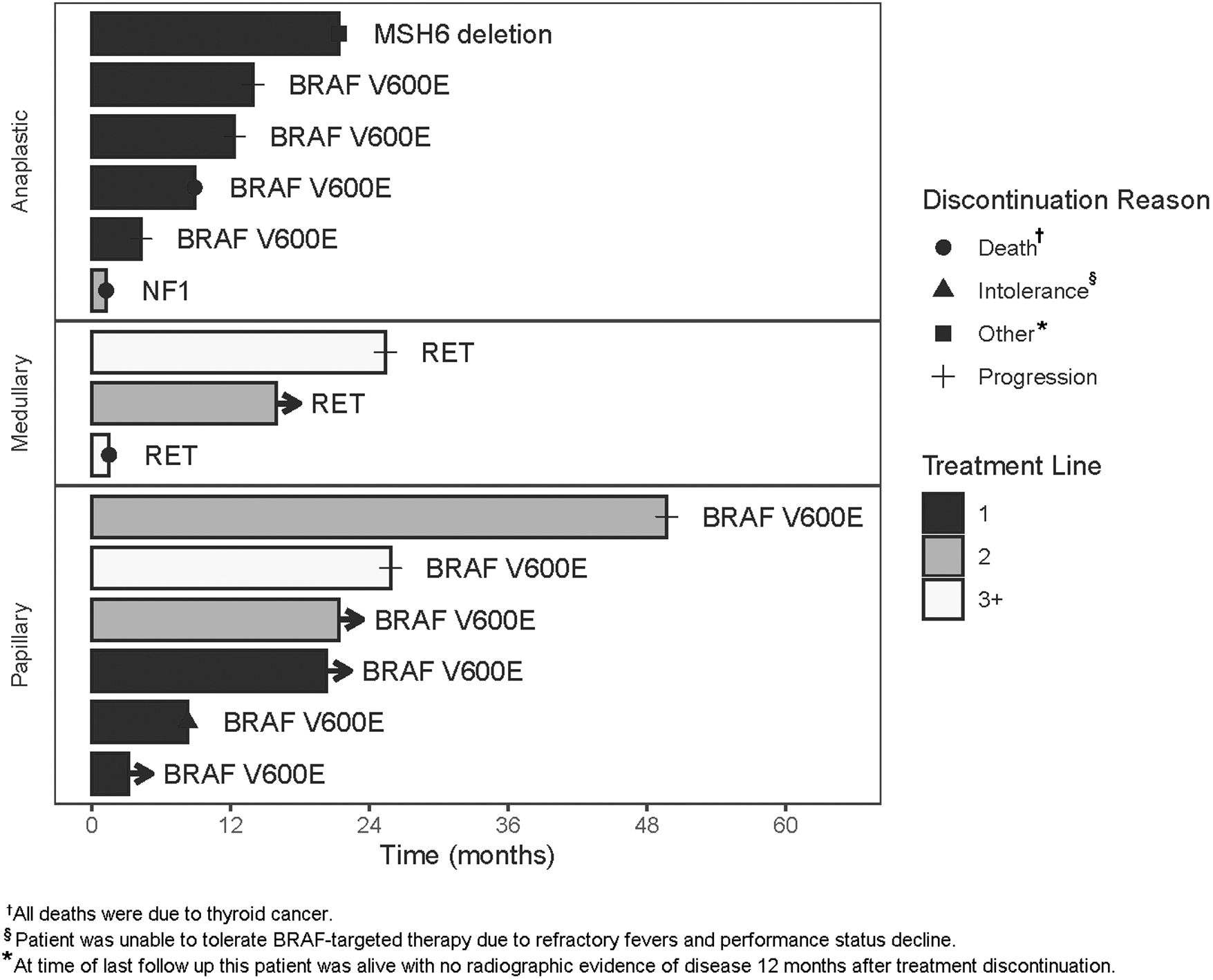
Swimmer plot of advanced thyroid cancer patients receiving matched therapy.
In one patient with ATC enrolled on OCTANE, a frameshift deletion in MSH6 was identified. He initially underwent total thyroidectomy and lymph node dissection for angioinvasive ATC with extrathyroidal extension and lymph node involvement, followed by adjuvant external beam radiotherapy. Follow-up imaging showed locoregional recurrence and lung metastases. He was treated on a Phase I/II clinical trial with an antiprogrammed death cell protein 1 antibody and received 23 cycles of treatment with complete response. He was followed on surveillance for an additional 12 months with no disease recurrence.
Discussion
Although several groups have analyzed the mutational landscape of thyroid cancer, these studies focused on comprehensive genomic characterization rather than clinical and treatment outcomes (22 –25). While the type and frequency of molecular alterations in our study are largely consistent with prior studies, our study adds to the existing literature by using a structured framework to define the actionability of alterations and categorize patients' genomic findings in a clinically relevant manner for patients potentially requiring systemic therapy (26 –28). This is important because there are now several mutation-based therapies that can be utilized in thyroid cancer, including BRAF and MEK inhibitors for BRAF V600E mutations, selective RET inhibitors for RET alterations, and tumor agnostic therapies for alterations such as NTRK fusions or microsatellite instability-high (MSI-H) tumors.
In our study, more than half of patients had a Level 1 or 2 actionable alteration, signifying Food and Drug Administration (FDA)-recognized or standard of care biomarkers predictive of response to an FDA-approved drug. BRAF V600E and RET alterations comprised 86% of Level 1 or 2 actionable mutations. Another third of patients had a Level 3 or 4 alteration, signifying compelling clinical or biological evidence supporting the biomarker as being predictive of response to an existing drug. A matched therapeutic approach was undertaken in 13% of patients, predominantly consisting of BRAF-targeted therapy.
We anticipate this number will increase with time, as half of patients with a Level 1 or 2 alteration in our cohort either had not yet started any systemic therapy, or were still on first-line treatment at the time of analysis. Because there is not yet Phase III evidence supporting first-line BRAF-targeted therapy, most BRAF V600E-mutated DTC patients still received lenvatinib first line. Even so, having a known BRAF V600E mutation provides an additional therapeutic option for later lines, and for those with a contraindication or intolerance to lenvatinib.
Few other studies have reported on patients with prospectively performed NGS. Chen et al. investigated 216 patients with advanced thyroid cancer who underwent NGS, of whom 68% had mutations in targetable pathways (29). More recently, Iñiguez-Ariza et al. analyzed 55 patients with metastatic thyroid cancer treated at Mayo Clinic sites who underwent molecular profiling using FoundationOne and found that 72% of DTC and 79% of ATC had potentially targetable alterations, although these included variants of unknown significance (30). FoundationOne results specifically guided the initiation of targeted therapy in 17% of patients (N = 9) in this study, which is similar to our findings.
The ongoing development of mutation-based systemic therapies has increased utilization of molecular immunohistochemistry tools during the diagnostic clinical workup, and subsequent molecular profiling has become an increasingly important part of clinical practice (28,31,32). There are no consensus guidelines about how this technology should be used in advanced thyroid cancer treatment (Table 5). ESMO recommendations for NGS in metastatic cancers recommends tumor mutational burden (TMB) and NTRK testing in advanced thyroid cancer, but otherwise leaves the decision of larger multigene panels to the physician and patient (11).
Society Guideline Recommendations for Molecular Testing in Advanced Thyroid Cancer
ATA, American Thyroid Association; dMMR, DNA mismatch repair; ESMO, European Society of Medical Oncology; IHC, immunohistochemistry; MSI, microsatellite instability; NCCN, National Comprehensive Cancer Network; TMB, tumor mutational burden.
Meanwhile for ATC, both American Thyroid Association and ESMO clinical practice guidelines recommend NGS molecular profiling at the time of diagnosis if available, and incorporate BRAF V600E testing into management algorithms (12,15). For DTC, however, ESMO guidelines state that the need for routine BRAF genotyping of PTC has not been established. The National Comprehensive Cancer Network (NCCN) guidelines recommend genomic testing for actionable mutations, including ALK, NTRK, RET, DNA mismatch repair, and TMB for advanced WDTC cancer; BRAF, NTRK, ALK, RET, microsatellite instability, and TMB for ATC; and RET and TMB testing for MTC (16).
Our study included patients with progressive unresectable or distant metastatic disease being considered for systemic treatment; therefore, our recommendations apply only to this patient population. We overall support the NCCN recommendations for genomic testing, although we would additionally advocate for BRAF testing for all patients requiring systemic therapy. For BRAF V600E-mutated ATC, treatment with the BRAF and MEK inhibitors dabrafenib and trametinib was greatly promising in a Phase II trial, with high rates of durable response, and a 12-month survival of 80% compared with historical rates of 20–40% (7). For BRAF-mutated PTC, a Phase II trial showed that treatment with the BRAF inhibitor vemurafenib had a response rate of ∼30%; a Phase III study is pending (NCT04940052) (8). Finally, the selective RET inhibitors selpercatinib and pralsetinib have each been shown to have high rates of durable response in patients with RET-altered thyroid cancers in Phase I/II trials (9,10).
While the majority of Level 1 and 2 alterations in our cohort consisted of BRAF and RET mutations, other infrequent alterations that may significantly benefit patients were also found. One patient with ATC was found to have an MSH6 deletion on NGS and was enrolled on an immunotherapy clinical trial. He had a complete response to therapy, which is in stark contrast to the usual dismal prognosis of ATC. A different patient with PTC had an NTRK fusion found on NGS, opening the option of treatment with a TRK inhibitor, which has been shown to have response rates of 75–80% in solid tumors (33). The FDA has approved multiple tumor-agnostic therapies to be used on the basis of molecular results, such as immunotherapy for MSI-H solid tumors, and larotrectinib for NTRK fusions (33 –35).
With the rapid advancement in oncology research and drug development, the third of our patients with Level 3 or 4 alterations and those with currently untargetable pathogenic alterations may still have treatment implications and potential for benefit from targeted therapies in the future. For example, mutations in KRAS were traditionally deemed to be untargetable, until the recent development of KRAS G12C inhibitors, which has shown promise in lung cancers and other solid tumors with a KRAS G12C mutation (36,37). Future therapeutic developments in RAS inhibition would be of interest, given the prevalence of RAS mutations in thyroid cancer. Thus, the use of a broader NGS panel would be our preferred option whenever possible, since this would allow for simultaneous detection of rarer variants with potential for significant clinical benefit in addition to testing known common variants.
Despite the commercial availability of NGS panels, cost is a barrier that may limit the feasibility of profiling each patient, especially in resource-limited jurisdictions. Based on our findings, in a setting where NGS is not possible, reflex testing for BRAF V600E mutations by immunohistochemistry in differentiated and anaplastic thyroid cancers, and testing for the most common RET alterations in MTC (e.g., RET M918T) should be performed, as these comprised the majority of actionable mutations (31).
Although we would advocate for molecular profiling of all patients for whom systemic therapy is being considered, the optimal selection of specimen and timing to perform this testing remains unclear. Many thyroid cancer patients live for years before disease recurrence, and even those with distant metastases may be managed with active surveillance for months to years before commencing systemic treatment. It is uncertain whether molecular profiling results of an archival tumor sample remain representative of the genomic features of the cancer at the time of treatment. One method to overcome this would be taking a fresh biopsy before starting systemic treatment; however, this comes with risk of morbidity to the patient and delays while awaiting results. An alternative method would be blood-based mutation profiling of circulating cell-free DNA, which would be less invasive to the patient and could provide results in a timelier manner.
We acknowledge the limitations of our study, which was a single institution series with a limited sample size. In our study, three different NGS panels were used, each with differing operating characteristics. None of the panels included TMB testing, and two of the panels used did not test for TERT promoter mutations. Events such as large deletions or insertions, gene amplifications or losses, and gene fusions were not detectable by the earlier panels. Thus, our study underestimates the frequency of these events, of which, gene fusions are likely the most clinically relevant. All patients included in our study underwent NGS testing, so we were unable to compare clinical outcomes with those who did not have NGS performed.
Similarly, due to the low number of patients, we could not compare survival outcomes of patients who received matched versus unmatched therapy. In addition, because of the evolution of levels of actionability of gene alterations over time, not all matched drug therapies were available for patients during the entire study period. Notwithstanding these limitations, our study provides valuable clinical insight into the actionability of molecular alterations in advanced thyroid cancers within a real-world practice, and helps inform discussion between physicians and patient about the potential benefits for NGS testing.
Conclusion
This study uses a structured framework to analyze the actionability and clinical use of NGS findings in patients with unresectable locally advanced or distant metastatic thyroid cancer for whom systemic therapy is being considered. The majority of patients had at least one potentially actionable mutation, and half of patients had a Level 1 or 2 alteration for which there is an FDA-approved drug. While the BRAF V600E and RET mutations were the most prevalent actionable alterations, other infrequent mutations were found with potential for significant clinical benefit. Based on these findings, we would advocate for multigene NGS of archival tissue before starting systemic therapy whenever possible, and for reflex testing for common BRAF and RET mutations in jurisdictions where NGS is not feasible.
Footnotes
Authors' Contributions
Data collection, data analysis, article preparation, and editing by L.X.M. Data analysis and biostatistical support, article preparation, and editing by O.E.-G. Article preparation and editing by P.L.B., T.S., and R.P. Data analysis, article preparation, and editing by O.M. and M.K.K.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was conducted with the support of the Ontario Institute for Cancer Research (OICR) through funding provided by the Government of Ontario and by the Princess Margaret Cancer Foundation.
Supplementary Material
Supplementary Table S1