
Abstract
Background:
Women are more likely to experience thyroid diseases than men. However, thyroid dysfunction risk in women undergoing the menopausal transition remains largely unknown. We explored the prevalence of thyroid dysfunction across menopausal stages.
Methods:
We conducted a cross-sectional study of 53,230 women aged 40 years or older who underwent health screening between 2014 and 2018. Menopausal stages were categorized into 4 based on the Stages of Reproductive Aging Workshop +10 criteria. A multinomial logistic regression model was used to estimate the prevalence ratios (PRs) with confidence intervals [CIs] for thyroid dysfunction in menopausal stages compared with that in premenopause.
Results:
The prevalence of overt hypothyroidism was significantly increased during late transition and postmenopause; it remained significant after further adjustments for potential confounders (age, center, year of examination, age at menarche, parity, education level, smoking status, alcohol consumption, physical activity, and body mass index) with corresponding multivariable-adjusted PRs [CI] of 1.61 [1.12–2.30] and 1.66 [1.16–2.37] in the late transition and postmenopausal stages, respectively. A significant increase in the prevalence of subclinical hypothyroidism was also observed in the late transition and postmenopausal stage with multivariable-adjusted PRs [CI] of 1.22 [1.06–1.40] and 1.24 [1.07–1.44], respectively. In contrast, subclinical and overt hyperthyroidism were not significantly associated with menopausal stages.
Conclusions:
In this study of pre- and perimenopausal Korean women, the prevalence of overt and subclinical hypothyroidism was significantly elevated in the late menopausal transition. Future prospective studies are warranted to investigate the clinical and prognostic significance of thyroid dysfunction in women during menopausal transition.
Introduction
Thyroid dysfunction is one of the most common endocrine disorders in the U.S. general population with previously unrecognized thyroid disease (1,2); ∼4.6% have hypothyroidism (0.3% overt and 4.3% subclinical) and 1.3% have hyperthyroidism (0.5% overt and 0.7% subclinical) (3). Thyroid abnormalities also have important consequences with respect to long-term health outcomes such as cardiovascular diseases (4,5), diabetes (4,5), various malignant conditions (6), and psychiatric conditions (7).
Menopause, a critical period in a woman's life cycle, is typically preceded by the menopausal transition, which encompasses a period of dynamic changes in the reproductive and nonreproductive tissues accompanied by various climacteric symptoms. Owing to the high prevalence of thyroid dysfunction among women, which is ∼10 times greater than that among men (8 –10), a considerable amount of research has been conducted to explore thyroid abnormalities in women. However, most of the available epidemiological studies have focused on pregnancy and postmenopause, and very little is known about the status of thyroid abnormalities specific to women undergoing menopausal transition.
Menopausal transition is characterized by a progressive deterioration of the hypothalamic–pituitary–ovarian (HPO) axis function, which manifests as dynamic changes in estradiol and follicle-stimulating hormone (FSH) levels (11). Previous studies have documented a bidirectional relationship of the thyroid and HPO axis function with female reproductive hormones (12,13). However, the effect of the dysregulation of the HPO axis on thyroid function in the different stages of menopausal transition is poorly understood. In addition, while thyroid function naturally declines with age (3), whether this trend is consistent among women during the menopausal transition and how the risks of overt and subclinical hyperthyroidism and hypothyroidism differ across menopausal stages remain unknown.
Substantial resemblance between symptoms of menopause and those of thyroid abnormalities such as weight gain, fatigue, cold intolerance, mood swings, and/or anxiety may increase the likelihood of overlooking an existing thyroid problem and thereby delaying treatment (1,14,15). Thyroid dysfunction, if left untreated, may be associated with significant morbidity as well as debilitating long-term consequences such as increased mortality (16). Therefore, the prevalence and risk distributions of thyroid abnormalities during perimenopause should be clearly defined to facilitate timely intervention in this population.
In this study, we investigated the distribution of risks for thyroid dysfunctions associated with the menopausal transition stage in perimenopausal women based on the Stages of Reproductive Aging Workshop (STRAW +10) criteria (premenopause, early and late menopausal transition, and postmenopause).
Materials and Methods
Study population
This study of middle-aged women was performed using data from Kangbuk Samsung Health Study, a cohort study of health screening examinees at the Kangbuk Samsung Hospital Total Healthcare Centers in Seoul and Suwon, South Korea (17 –19). Thyroid hormones were routinely measured as part of the health examination for all participants irrespective of symptoms.
This study included 87,455 women aged >40 years who participated in a health examination between 2014 and 2018. After excluding 34,225 participants who met one or more exclusion criteria, 53,230 participants were included in the final analysis (Fig. 1). This study was approved by the institutional review board of Kangbuk Samsung Hospital (IRB No. 2021-10-003), which waived the requirement for obtaining informed consent as deidentified retrospective data routinely collected during health screening were used.
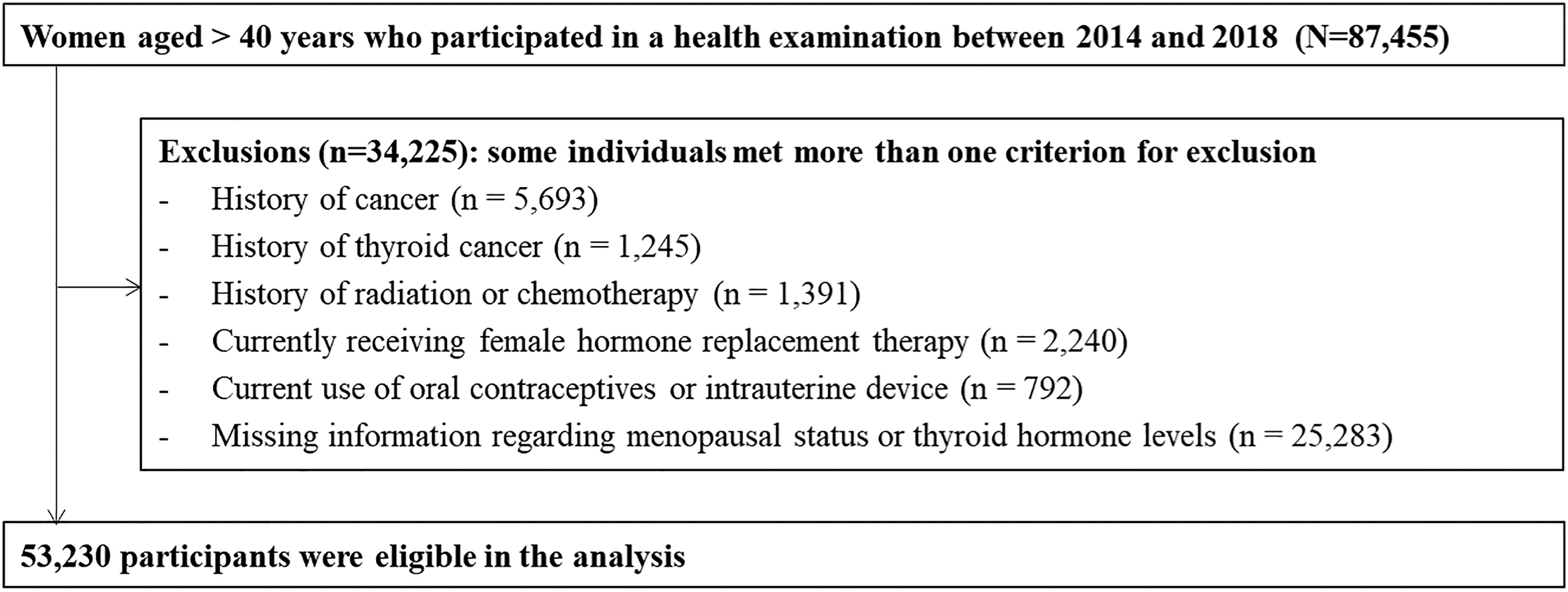
Flow chart describing the selection of the study participants.
Data collection
A standardized self-administered questionnaire was used to determine demographic information, health behaviors, history of thyroid disease or use of thyroid medications, and other medical conditions (17,18).
The STRAW +10 criteria were used to determine the menopausal stage (Fig. 2) (19 –21). The questions used to determine menopausal stages with the corresponding responses of the participants are presented in Supplementary Table S1. Other reproductive factors that were assessed include age at menarche, parity (the number of previous pregnancies, including stillbirths and live births), use of oral contraceptives or intrauterine device, and use of female hormone therapy.

Definition of menopausal transition based on STRAW +10 staging system.
Trained nurses measured height, weight, and sitting blood pressure (BP). Diabetes mellitus was defined as fasting serum glucose level ≥126 mg/dL or self-reported use of insulin or antidiabetic medication. Hypertension was defined as BP ≥140/90 mmHg or current use of antihypertensive medication. In a subsample of women who underwent pelvic ultrasonographic examinations, experienced gynecologists blinded to the study routinely asked examinees whether they had been diagnosed with any gynecological disorders, including polycystic ovary syndrome (PCOS), and examined them for the presence of ovarian cysts, including size, echogenicity, echotexture, internal pattern, and content. Previous gynecological disorders or abnormal findings on pelvic ultrasonographic examinations have been documented in ultrasonography reports (22).
The fasting blood sample measurements included lipid profiles, glucose levels, high-sensitivity C-reactive protein levels, and thyroid function tests. Insulin resistance was assessed using the homeostatic model assessment of insulin resistance according to the following equation: fasting blood insulin (mU/mL) × fasting blood glucose (mmol/L)/22.5.
Measurement of thyroid function and definitions of thyroid abnormalities
Electrochemiluminescent immunoassay (Roche, Tokyo, Japan) was used for measuring serum thyrotropin (TSH) levels, free thyroxine (fT4), and free triiodothyronine (fT3), corresponding lower limits of detection, and the coefficient of variation for low- and high-level quality control specimens: 0.005 μIU/mL, 2.1–3.2% and 2.2–3.1% for TSH; 0.023 pg/dL, 1.6–2.6% and 1.9–3.6% for fT4; and 0.26 pg/mL, 1.2–3.9% and 1.7–4.1% for fT3, respectively.
The normal ranges for serum TSH, fT4, and fT3 levels were 0.25–5.0 μIU/mL, 0.93–1.7 ng/dL, and 2.0–4.4 pg/mL, respectively. Serum fT4 and TSH levels were used to define overt and subclinical thyroid dysfunction as follows: (i) <0.93 ng/dL and ≥5.0 μI/mL for hypothyroidism; (ii) >1.7 ng/dL and <0.25 μIU/mL for hyperthyroidism; (iii) 0.93–1.7 ng/dL and ≥5.0 μIU/mL for subclinical hypothyroidism; and (iv) 0.93–1.7 ng/dL and <0.25 μIU/mL for subclinical hyperthyroidism, respectively.
Statistical analysis
The participants' characteristics were summarized across the menopausal stage. To test for linear trends, the number of categories was included as a continuous variable in the regression models.
The prevalence ratios (PRs) with confidence intervals [CIs] for thyroid dysfunction were estimated using a multinomial logistic regression model across menopausal transition stages compared with those for the premenopausal stage. The prevalence of women with abnormal values of any of the thyroid hormones (TSH, fT4, and fT3) was also estimated across the menopausal transition stage. First, the age-adjusted PRs were estimated.
Other confounders were further adjusted in the multivariable-adjusted model, which included age, center, year of examination, education level, age at menarche, smoking status (never smokers, ex-smokers, current smokers, or unknown), average alcohol intake (0, <10, ≥10 g/day, or unknown), physical activity level (being active, being minimally active, being health enhancing physically active, or unknown), body mass index (BMI, continuous variable), and parity (nulliparous, 1–2 parity, parity of ≥3).
Statistical analyses were conducted using STATA software (version 15.0; StataCorp LP, College Station, TX). The p-value for statistical significance was defined as p < 0.05 using two-tailed tests.
Results
Baseline characteristics
The mean age ± standard deviation of study participants was 47.1 ± 7.8 years (Table 1). Menopausal stage was positively associated with parity, diabetes, hypertension, hyperlipidemia medication, BMI, BP, glucose, and unfavorable lipid profiles. Conversely, early menarche and education level were inversely associated with menopausal stage. A slight J-shaped relationship was found between menopausal stages and age-adjusted mean values [CI] of serum fT3, fT4, and TSH among women not using thyroid disease medication (Supplementary Table S2). Pre- and postmenopausal fT4 levels were similar, whereas the highest fT3 and TSH levels were observed in the postmenopausal stages.
Characteristics of Study Participants Across Menopausal Stages (n = 53,230)
Data are the mean (standard deviation).
Less than 12 years.
≥ 3 times.
Ethanol ≥10 g/day.
Meeting either of the following 2 criteria: (i) vigorous intensity activity 3 or more days per week accumulating ≥1500 MET minutes per week or (ii) 7 days of any combination of walking, moderate intensity, or vigorous intensity activities achieving at least 3000 MET minutes per week.
Greater than or equal to college graduate.
Median (interquartile range), or percentage.
BMI, body mass index; fT3, free triiodothyronine; fT4, free thyroxine; HDL, high-density lipoprotein; HOMA-IR, homeostasis model assessment of insulin resistance; hsCRP, high-sensitivity C-reactive protein; LDL, low-density lipoprotein; MET, metabolic equivalent of task; TSH, thyrotropin.
Overt and subclinical hypo- and hyperthyroidism by menopausal stage
The age-adjusted PRs [CI] of overt hypothyroidism comparing early, late transition, and postmenopause to premenopause were 1.10 [0.74–1.64], 1.79 [1.25–2.54], and 1.92 [1.35–2.71], respectively (p for trend = <0.001) (Table 2). This association remained significant after additional adjusting for covariates. The prevalence of subclinical hypothyroidism significantly increased in the late transition and postmenopausal stages with a multivariable-adjusted PR [CI] of 1.22 [1.06–1.40] and 1.24 [1.07–1.44], respectively.
Prevalence Ratios [Confidence Intervals] of Overt and Subclinical Hypo- and Hyperthyroidism According to Menopausal Stage
Estimated from multinomial logistic regression models. The multivariable-adjusted model was adjusted for age, center, year of examination, education level (high school graduate or less, community college or university graduate, graduate school or higher, or unknown), smoking status, alcohol consumption, physical activity level, BMI, parity, and age at menarche.
CI, confidence interval; PR, prevalence ratio.
For overt and subclinical hyperthyroidism, no significant associations were found between the prevalence and menopausal stages. Similar associations were observed when the same analyses were performed using a sample of (i) women aged <60 years (Supplementary Table S3) and (ii) women who underwent pelvic ultrasonography without signs of PCOS (Supplementary Table S4). In addition, the associations did not materially change after further adjustment for a history of oral contraceptive use when analyses were conducted without excluding those currently using oral contraceptives (Supplementary Table S5).
When analyses were conducted without excluding postmenopausal women using female hormone therapy to explore the influence of female hormone therapy on postmenopausal women, the higher prevalence of overt hypothyroidism was no longer observed in postmenopausal women with current use of female hormone therapy but was consistently observed in those without hormone use (Supplementary Table S6).
Menopausal stage and risk of having abnormal thyroid hormone levels
The prevalence of each thyroid hormone abnormality during each menopausal stage was evaluated (Table 3). For serum TSH, the age-adjusted PRs [CI] of high TSH levels (>5 μIU/mL) comparing early, late transition, and postmenopause with premenopause were 1.02 [0.90–1.15], 1.26 [1.11–1.43], and 1.29 [1.13–1.48], respectively (p for trend = <0.001). After further adjustments for center, year of examination, education level, smoking status, alcohol consumption, physical activity, parity, age at menarche, and BMI, the association was consistently observed (p for trend = <0.001). There was no significant association between menopausal stage and the prevalence of low TSH levels (<0.25 μIU/mL).
Prevalence Ratios [Confidence Intervals] of Abnormal Thyroid Hormone Level According to Menopausal Status Among Women Who Did Not Use Medications for Thyroid Disease (n = 51,918)
Estimated from multinomial logistic regression models. The multivariable-adjusted model was adjusted for age, center, year of examination, education level (high school graduate or less, community college or university graduate, graduate school or higher, or unknown), smoking status, alcohol consumption, physical activity level, BMI, parity, and age at menarche.
For serum fT4, the age-adjusted PRs [CI] for low fT4 levels (<0.93 ng/dL) comparing early, late transition, and postmenopause with premenopause were 1.10 [0.74–1.64], 1.76 [1.24–2.51], and 1.90 [1.34–2.68], respectively (p for trend = <0.001). For serum fT3 levels, the age-adjusted PRs [CI] for low fT3 levels (<2 pg/mL) comparing early, late transition, and postmenopause with premenopause were 1.10 [0.56–2.17], 2.40 [1.36–4.23], and 1.78 [0.89–3.55], respectively (p for trend = 0.014).
After adjusting for the other covariates, the prevalence patterns for both fT3 and fT4 remained similar. No significant association was found between the prevalence of high fT4 and high fT3 levels across menopausal stages. Similar associations were observed in women aged <60 years (Supplementary Table S7).
Discussion
In this study of 53,230 perimenopausal women, we found that the prevalence of overt and subclinical hypothyroidism increased as the menopausal stage progressed, beginning in the late transition stage. The significant association between late menopausal stage and the prevalence of overt and subclinical hypothyroidism persisted after adjusting for potential confounders. To the best of our knowledge, this is the first large-scale study to examine the prevalence of thyroid dysfunction across the menopausal stages as defined by the STRAW +10 criteria, including the early and late transition stages.
Although evidence on how thyroid function changes during the menopausal transition is limited, the available data suggest that TSH levels tend to increase around menopause (23,24). In the Study of Women's Health Across the Nations that included 3242 women, no significant difference in TSH concentrations was found between premenopause and early perimenopause (25). In this study, the women were categorized as premenopausal versus early perimenopausal and, therefore, the prevalence patterns of thyroid dysfunction in the later stages of the menopausal transition could not specifically be addressed. Furthermore, TSH concentrations were the sole variable used to define thyroid status in this study. Our study showed that the prevalence of hypothyroidism significantly increased during the late menopausal transition stage and continued into the postmenopausal stage. This trend toward a hypothyroid state in the late transition and postmenopausal stages was also observed in the analyses of both fT3 and fT4 levels.
When a subsample of women who underwent pelvic ultrasonographic examination without signs of PCOS, which may have affected the menstrual cycle, was examined, an increased prevalence of subclinical hypothyroidism during the late menopausal transition stage followed by a slight decline in the prevalence was observed; the same trend was observed in the analyses of women aged <60 years. Accumulated data suggest that the late menopausal transition stage is a critical period wherein various menopause-associated symptoms and measurable physiological changes are most likely to manifest (26). Our findings add to the existing line of evidence reflecting an increasing trend in the occurrence of abnormal thyroid function in the late menopausal stage, which should be confirmed by conducting further longitudinal studies.
As per the current guidelines, routine screening of serum TSH is discouraged in asymptomatic nonpregnant women under the age of 60 years (27,28). However, aggressive case finding is recommended in women at increased risk for hypothyroidism or those with nonspecific symptoms (27,28). Although there are ongoing controversies over the need for routine thyroid screening in premenopausal women, our findings suggest that the benefit of thyroid hormone screening may be extended to perimenopausal women, specifically to the subgroup of women with nonspecific thyroid-related symptoms that bear a resemblance to menopausal symptoms. According to a recent study, high fT4 levels were positively correlated with the frequency of menopausal symptoms such as general weakness, palpitations, and paresthesia in perimenopausal women (29). In another study, when thyroid dysfunctions were treated in women with severe menopausal symptoms, there was marked improvement in the menopausal-like symptoms and they no longer needed estrogen therapy or other nonspecific treatments (30). These findings highlight that the thyroid hormone status does affect the intensity and frequency of certain climacteric symptoms, which may suggest that the possibility of thyroid dysfunction should be ruled out in perimenopausal women before initiating estrogen therapy. In fact, in women with underlying hypothyroidism being treated with thyroxine, estrogen therapy is known to increase the need for thyroxine (31). Therefore, it is critical for clinicians to be able to identify and differentiate the nature of the symptoms for optimal management. Future studies should examine the potential prognostic benefits of thyroid screening in women undergoing the menopausal transition who present with nonspecific symptoms.
The mechanism underlying the increased tendency toward hypothyroidism in the late menopausal transition is not well understood. Estrogen, also thought to be a major contributor of gender-associated disparity in thyroid dysfunction risk, upregulates thyroxine-binding globulin, which may lead to a decrease in serum fT4 concentrations and an increase in TSH levels, characteristic of a hypothyroid state (32). Contrary to that the menopausal transition is previously characterized by a steady drop in estrogen levels, studies suggest that serum estrogen levels may fluctuate or even become abnormally high toward the final menstrual period, after which it becomes lower and stabilizes (33 –35). Furthermore, the potential impact of other reproductive hormones on the thyroid gland may also need to be considered, although the evidence is far more limited. Thyroid hormones act synergistically with FSH to produce progesterone (1,36). Furthermore, progesterone is known to cause an increase in fT4 levels, as well as a trend toward lower TSH levels (37), and can directly influence thyroid function by upregulating gene expression related to thyroid function (38). These findings may have ramifications for women undergoing menopausal transition, during which the number of oocytes decreases exponentially, which may in turn affect the progesterone concentration. Additional studies considering the effects of gonadal hormones are necessary to elucidate the underlying mechanisms of the association between a hypothyroid state and the late menopausal transition.
Our study had several limitations. First, since the menopausal stage was determined on the basis of the menstrual pattern and due to the inherent limitation of the cross-sectional design, further longitudinal studies are warranted to determine temporal associations between menopausal stages and thyroid function. Second, female reproductive hormones such as FSH or estradiol were not assessed, which could have affected the dynamics of thyroid hormones and have minimized misclassification of menopausal stage. Reproductive hormone levels, which vary throughout the menstrual cycle, need to be measured in the early follicular phase, which typically overlaps the menstruation period. However, we used data routinely collected in comprehensive screening examinations, which include urinalysis as a basic test that women were instructed to avoid during menstruation corresponding to the early follicular phase. Thus, obtaining accurate measures of serum reproductive hormone levels was not feasible owing to the nature of our health checkup examination. Further studies with data on sex hormone status, a supplementary objective measure of menopausal stage, would be preferable to support and confirm the relationship between menopausal stages and thyroid function. Third, data on thyroid antibody measurements were not available in our study. Autoimmune hypothyroidism shows a clear predominance among women with an increase in the prevalence with age, as seen in most autoimmune conditions; it is also the most common cause of hypothyroidism (39,40). Of note, there is a report that thyroid peroxidase antibody levels were positively correlated with estradiol and estradiol/progesterone ratios in women with PCOS, suggesting that, although the causal association is not clear, this may also be the case in the later stages of the menopausal transition wherein estradiol fluctuation with concomitant drop in progesterone levels due to the emergence of anovulation is similarly observed (34,41). Therefore, consideration of autoimmune thyroid dysfunction and dynamics between reproductive hormones and thyroid-specific antibodies would be necessary to better understand the changes in thyroid function across the menopausal transition. Fourth, when we collected the data on current medication use for thyroid disorders, thyroid hormone replacement therapy and antithyroid hormone medication were not differentiated. Thus, cautions need to be taken in interpreting our results on thyroid medication use. Lastly, relatively healthy Korean women who were employees or their spouses underwent routine health examinations. These individuals were likely to have a distinct socioeconomic status or level of education, which possibly differed from that of the general population. Therefore, the findings of this study may not be generalizable to populations with different race/ethnicity, or demographic characteristics.
Nevertheless, our study has several notable strengths. We used a newly updated menopausal staging system (STRAW +10 criteria), which is currently considered the reference standard for assessing reproductive aging. In addition, the large sample of a well-characterized population of perimenopausal women; use of carefully standardized clinical, imaging, and laboratory procedures; and inclusion of lifestyle factors enabled us to directly measure the main parameters of thyroid function, including TSH, fT4, and fT3 levels, and account for possible confounders to ensure the quality of our study outcomes.
In conclusion, in this large-scale study of perimenopausal women, the risk of overt and subclinical hypothyroidism significantly increased from the late menopausal transition. Our study suggests that targeted monitoring may be necessary in women in the late menopausal transition, presenting with menopausal symptoms that may resemble thyroid abnormalities. Future prospective studies are needed to further investigate the clinical and prognostic significance of thyroid dysfunction during menopausal transition.
Footnotes
Authors' Contributions
Y.K. contributed to analysis and interpretation of data, drafting and critical revision of the article.
Y.C. was involved in study concept and design, acquisition of data, interpretation of data, and drafting and critical revision of the article.
I.Y.C. carried out interpretation of data and critical revision of the article.
R.K. contributed to acquisition of data and critical revision of the article.
G.L. acquired data and critically revised the article.
J.H.J. interpreted data and critically revised the article.
S.R. carried out study concept and design, acquisition of data, interpretation of data, and drafting and critical revision of the article.
M.K. was involved in study concept and design, acquisition of data, interpretation of data, and drafting and critical revision of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This article was supported by the SKKU Excellence in Research Award Research Fund, Sungkyunkwan University, 2020.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7