
Abstract
Background:
The goal of radioactive iodine (RAI) in differentiated thyroid cancer (DTC) is to treat metastasis and reduce recurrence risk. International guidelines provide broad risk stratification to aid treatment decisions, but a more nuanced approach to individualize care is warranted. We developed a predictive risk model for DTC.
Methods:
We performed a retrospective multivariable analysis of 899 patients who received RAI after thyroidectomy at a quaternary center in Australia between 2008 and 2016. Collected data included age, gender, histology, stimulated thyroglobulin (sTg), and 8th American Joint Committee Cancer (AJCC) staging. The ATA Modified Initial Risk (ATA) was calculated retrospectively. Recurrence was defined as clinically significant progression requiring either surgical intervention or administration of a second activity of RAI. Synchronous metastasis was defined as distant metastasis (i.e., outside of the neck) that was present at the time of diagnosis on structural imaging or initial post-iodine treatment scan. The features significantly associated with synchronous metastasis or recurrence were employed in the generation of a predictive risk model. A separate cohort of 393 patients who received RAI in 2017–2021 was used for validation.
Results:
On multivariate analysis, sTg ≥10 μg/L, extrathyroidal extension (ETE) and lymph node involvement predicted recurrence. Independent of ATA, patients with sTg ≥10 μg/L had a shorter disease-free survival (DFS) than those with sTg <10 μg/L (p < 0.001). The ETE stratified by four histological categories was significantly associated with worse DFS (p < 0.001). In a subset of patients, the presence of thyroglobulin antibody (TgAb) did not influence recurrence in patients with sTg <10 μg/L. On multivariate analysis, widespread ETE, sTg ≥10 μg/L, multifocal papillary thyroid cancer and follicular thyroid cancer were positively associated with synchronous metastasis. A predictive risk model was developed to estimate synchronous metastasis/recurrence risk and validated successfully in the second cohort.
Conclusions:
Our novel predictive risk model modifies and extends ATA stratification by including sTg and ETE, which we found to be independent predictors of both recurrence and synchronous metastasis in DTC.
Introduction
Differentiated thyroid cancer (DTC) is frequently managed with total thyroidectomy followed by radioactive iodine (RAI) to treat remnant tissue or residual disease. Determining personalized risk of recurrence for DTC patients would assist in the prescription of RAI therapy and minimize both over- and undertreatment. More than 50% of patients with distant metastatic disease manifest this at the time of diagnosis (1), and correctly identifying these patients is important to ensure an appropriate choice of RAI. Moreover, 95% of selected patients with low-risk DTC may never recur, and avoiding RAI altogether may be appropriate (2).
The 2015 ATA Modified Initial Risk (ATA) Stratification is a three-tiered risk system used to guide treatment decisions (3); however, it has some shortcomings: “Low” ATA does not adequately identify patients with sufficiently low risk to avoid RAI treatment (4), and up to 60% patients treated with RAI are classified as “Intermediate” risk (5), which does not specifically guide clinicians as to the choice of RAI treatment (6).
Clinical and histopathological factors outside the ATA Modified Initial Risk Stratification, including postoperative serum thyroglobulin (Tg) and histological extrathyroidal extension (ETE), have been found to predict the risk of both synchronous metastases and recurrence. Tg is used as a tumor marker in DTC to assess recurrent disease. After total thyroidectomy, levothyroxine suppressed Tg levels ≥0.2 μg/L using a high sensitivity assay suggesting at least microscopic disease, while stimulated thyroglobulin (sTg) ≥30 μg/L raises suspicion for metastatic disease (3,7).
Undetectable Tg in low-risk patients is associated with a very low risk of recurrence (8,9). Undetectable Tg in high-risk patients, however, does not reliably exclude recurrent disease (10 –12). Although measurement of postoperative Tg is recommended by ATA guidelines, it is not incorporated into initial risk stratification due to uncertainty around threshold values (3).
The ETE has also been shown to predict recurrence. The ETE is present in 10–15% of DTC cases, and in 50% of these cases it involves strap muscles (3). The ATA Modified Initial Risk Stratification (3) stratifies ETE into three distinct categories depending on the presence or absence of ETE intraoperatively: (i) no ETE, (ii) microscopic (minimal) ETE, or (iii) macroscopic (gross) ETE. Minimal ETE (mETE) is classified as indicating an intermediate risk of recurrence, while gross ETE is classified as high risk.
While gross ETE is associated with poor prognosis and a high risk of recurrence, the influence of mETE on ATA defined risk is less apparent (13 –15). Pathological assessment of mETE may be subjective and histological definitions vary across institutions, in contrast to the more objective assessment of gross ETE determined at surgery (16 –19).
Here, we aimed at developing a predictive risk model based upon personalized risk of either synchronous metastasis or recurrence, incorporating both ATA features together with histological ETE and postoperative sTg. Validation of the predictive risk model was performed on a separate cohort of DTC patients treated with RAI at our institution.
Methods
Retrospective analysis of thyroid cancer patients after their first treatment with RAI between 2008 and 2016 at Royal North Shore Hospital was performed. Data were collected from a prospectively maintained thyroid cancer database. Inclusion criteria included all patients aged older than 18, who were treated with RAI after completion or total thyroidectomy. sTg was measured when thyrotropin (TSH) ≥30 mIU/L. sTg was measured using the Immulite Assay from 2008 to 2014 and Roche Cobas (e601) assay from 2014 onward. TgAb was measured using the Abbott Architect assay. The method of TSH stimulation was not recorded in the dataset; however, since 2007, the Australian government has subsidized the cost of recombinant TSH in DTC patients, making it widely utilized.
The ATA Modified Initial Risk categories were retrospectively assigned for each patient (by A.W.; as per Supplementary Fig. S5). During this time period, surgical pathology of thyroid carcinomas was reported using a structured template into four distinct categories of ETE based on pathological assessment alone: Category 1: tumor completely confined to thyroid parenchyma away from the capsule; Category 2: tumor underlies the junction of the thyroid and adjacent soft tissue (so called thyroid “pseudocapsule”) but without clear extension into soft tissue; Category 3: tumor shows microscopic evidence of growth out of the thyroid into adjacent perithyroidal fibroadipose tissue; and Category 4: widespread extrathyroidal spread into soft tissue and/or extension into skeletal muscle, including the strap muscles (we presume many of these category 4 patients would have had “grossly identified” invasion at the time of surgery but do not have this data to confirm) (Fig. 1).
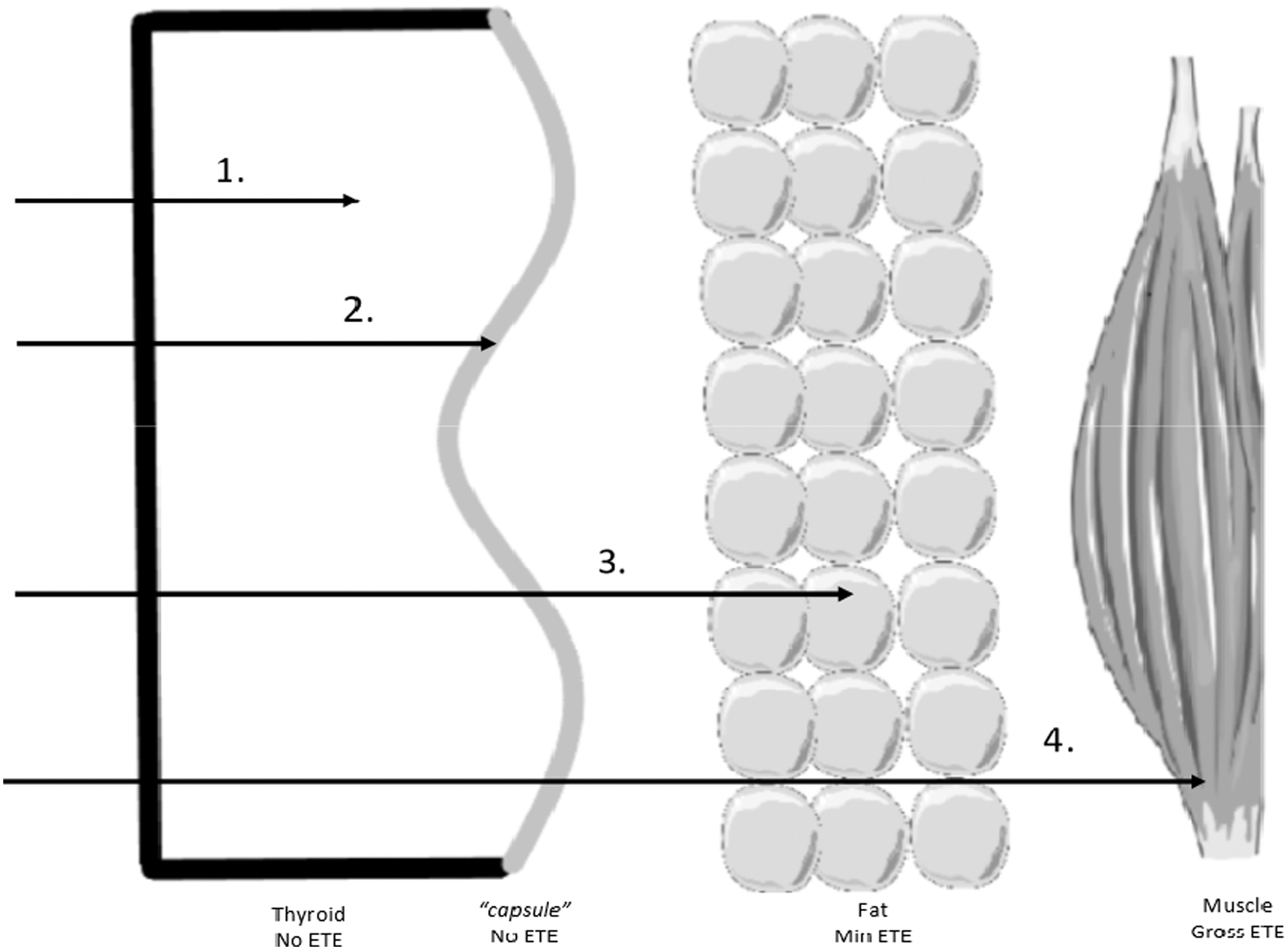
Illustration of four ETE categories. ETE, extrathyroidal extension; Gross ETE, gross extrathyroidal extension; Min ETE, minimal extrathyroidal extension; No ETE, no extrathyroidal extension.
To prevent overdiagnosis of blood vessel invasion, our institution uses strict criteria to define the presence of vascular invasion similar to that of Mete and Asa (20). Further, for follicular thyroid cancer (FTC) and Oncocytic carcinoma of the thyroid (Oncocytic), the entire capsule of the neoplasm is embedded for histological analysis before a tumor can be considered negative for vascular space invasion earlier. Vascular invasion was defined as infiltration into blood vessels, while lymphatic invasion involved infiltration into the lymphatic vessels. In practice, we and others often find it difficult to separate invasion of lymphatics from invasion of capillaries when small vessel invasion only is present (16).
In our institution, we approach this problem by reporting lymphovascular invasion as involving small vessels (lymphatic or capillaries), large vessels (usually veins), or both. For our study, we presumed that most patients with papillary thyroid cancer (PTC) and small vessel only invasion had lymphatic space invasion while most patients with FTC or Oncocytic and small vessel only invasion had capillary (that is vascular) invasion; however, all patients with large vessel invasion had vascular invasion. However, we accept that some authorities feel they can separate lymphatic from capillary invasion more confidently in most cases (16). The extent of vascular invasion was available for FTC and Oncocytic carcinomas. Other pathological features were assessed prospectively based on standard criteria and definitions.
Synchronous metastasis was defined as distant metastasis (i.e., outside the neck) present at time of the first diagnosis of DTC on structural imaging or noted on the initial post-treatment whole body iodine scan. Metachronous metastasis was defined as distant metastasis occurring at any time after the first RAI scan. Recurrence was defined to capture only clinically significant progression that warranted either surgical intervention or administration of a second activity of RAI, and not including synchronous metastasis.
Disease-free survival (DFS) was defined as time to synchronous metastasis or recurrence and was censored to death or end of study period. Overall, survival data were obtained from medical records and publicly available death notices and was defined as time from surgery until any-cause death (21). No local guidelines exist at our institution, and follow-up was at the discretion of the treating clinician.
Our predictive risk model was developed by incorporating additional features associated with recurrence and synchronous metastasis into the 2015 ATA Modified Initial Risk guidelines. The predictive risk model was validated on a separate cohort of 393 patients after their first treatment with RAI between 2017 and 2021.
The Human Research Ethics Committee at Northern Sydney Local Health District approved the study (ETH00360/STE006443 and ETH02787/STE05282).
Statistical analysis
Usually, distributed data were presented as mean (±standard deviation) and continuous non-normally distributed variables as median (interquartile range, IQR). Categorical variables were expressed as frequency and proportions. Mann-Whitney tests were used to compare median values. Categorical groups, including histology, gender, ATA, and American Joint Committee Cancer (AJCC) staging, were assessed by chi-square analysis.
Receiver operating curves (ROC) were used to assess the diagnostic accuracy of sTg and to compare our novel predictive risk model with the ATA classification system. Kaplan-Meier curves analyzed DFS, defined as the time to recurrence. Univariate and multivariate binomial regression analysis was used to elicit the factors associated with recurrence and synchronous metastasis. Age, gender, sTg, ETE, lymph node involvement, tumor size, vascular invasion, lymphatic invasion, the extent of vascular invasion in FTC, and oncocytic carcinomas and histology were analyzed on univariate analysis, with variables with a p-value ≤0.2 included in the multivariate analysis.
McNemar's test compared recurrence risk between our predictive risk model and ATA guidelines. p ≤ 0.05 was considered statistically significant. Statistical analyses were conducted using Statistical Package for Social Sciences (SPSS) version 26 (SPSS, Inc.). Figures were created using GraphPad Prism version 8.0.0 for Windows (GraphPad Software).
Results
Baseline characteristics of the discovery and validation cohorts
The discovery cohort included 899 patients, and the validation cohort comprised 393 patients (Supplementary Fig. S1). Baseline characteristics of both cohorts (Table 1) showed no significant differences in age, gender or histology, but did differ in ATA and AJCC stage 4.
Baseline Characteristics of Discovery and Validation Cohorts
Bold indicates statistically significant p ≤ 0.05.
AJCC, American Joint Committee Cancer; ATA, ATA Modified Initial Risk; FTC, follicular thyroid cancer; FVPTC, follicular variant papillary thyroid cancer; Oncocytic, oncocytic carcinoma of the thyroid; PTC, papillary thyroid cancer; RAI, radioactive iodine; TSH, thyrotropin.
The discovery cohort had a median follow-up of 84 months and median time to recurrence of 13 months (IQR 11–16 months). In the validation cohort, median follow-up was 34 months with a median time to recurrence of 11 months (IQR 6–15 months). Details of recurrence in discovery and validation cohorts are described in Supplementary Table S1 and Supplementary Fig. S4 shows RAI treatments received in both cohorts.
Factors associated with synchronous metastasis
Between 2008 and 2016, 26 (2.9%) patients were identified as having synchronous metastasis (23 identified at initial post-treatment iodine scan and 3 by structural imaging at diagnosis), and 9 (1%) patients were identified with metachronous metastasis. Compared with patients without metastasis, univariate analysis found sTg ≥10 μg/L, widespread ETE, lateral neck lymph node (N1b) disease, larger tumor size, venous invasion, multifocal PTC, and follicular variant PTC and FTC to be associated with synchronous metastasis (Table 2). Widespread ETE, sTg ≥10 μg/L and histological subtype remained significant on multivariate analysis.
Factors Associated with Synchronous Metastasis on Univariate and Multivariate Analysis (n = 895)
Bold on univariate analysis p ≤ 0.2.
Bold on multivariate analysis p ≤ 0.05.
CI, 95% confidence interval; ETE, extrathyroidal extension; LN, lymph node; N1a, central neck lymph node; N1b, lateral neck lymph node; OR, odds ratio; sTg, stimulated thyroglobulin.
Factors associated with recurrence
Univariate analysis of the discovery cohort found histological ETE, sTg ≥10 μg/L, lymphatic invasion, and lymph node involvement to predict recurrence (Table 3). sTg ≥10 μg/L, lymph node involvement, and widespread ETE remained significant in multivariate analysis (Table 3).
Univariate and Multivariate Analysis on Predictors of Recurrence in Patients Treated with Radioactive Iodine Between 2008 and 2016 (n = 871)
Bold on univariate analysis p ≤ 0.2.
Bold on multivariate analysis p ≤ 0.05.
Additional supplementary analyses are shown in Supplementary Tables S4 and S5.
Association between sTg and recurrence
Median sTg was 0.9 μg/L (range 0–48,100, IQR 0.9–3.7) collected at a median of 61 days (IQR 44–92 days) postoperatively. When recurrence was restricted to patients treated for disease outside the thyroid bed, sTg 8.5 μg/L afforded optimal sensitivity and specificity (J value 0.36). Setting sTg at 10 μg/L gave a J value 0.35 and was accepted as a more pragmatic value for incorporation into a clinical predictive risk model. Baseline characteristics of patients with sTg <10 μg/L and sTg ≥10 μg/L are outlined in Supplementary Table S2. Patients with sTg ≥10 μg/L were 9.57 times more likely to recur than patients with sTg <10 μg/L (p < 0.001, 95% confidence interval 6.03–15.8).
In a subset analysis, a sTg >30 μg/L identified patients with recurrence and synchronous metastasis, with a specificity of 98% (651/661), sensitivity 21% (51/238), negative predictive value of 78% (651/838), and positive predictive value of 84% (51/61).
Disease-free survival
The DFS was longer in individuals with sTg <10 μg/L than in those with sTg ≥10 μg/L across all ATA groups (p < 0.001, Fig. 2). Notably, DFS in individuals defined as low ATA but sTg ≥10 μg/L was comparable to those with high ATA and sTg <10 μg/L (p = 0.33). In individuals with sTg ≥10 μg/L, there was no difference in DFS between intermediate and high ATA (p = 0.56).
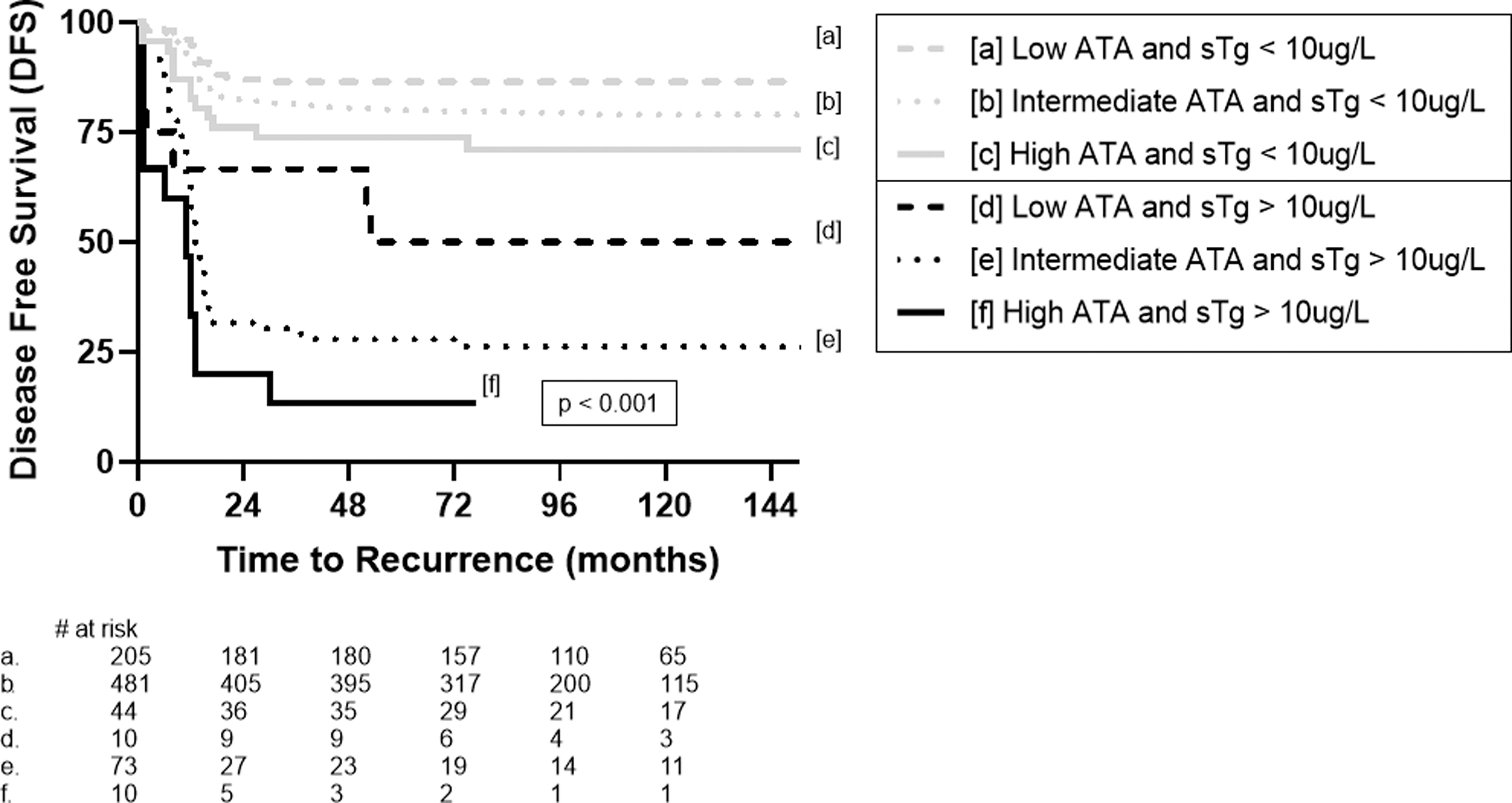
Disease-free survival stratified by ATA and sTg (≥10 or <10 μg/L). ATA, ATA Modified Initial Risk; sTg, stimulated thyroglobulin.
A subset analysis of 497 patients with thyroglobulin antibody (TgAb) data found no difference in DFS between antibody-positive and antibody-negative patients with an sTg <10 μg/L in each ATA category (low p = 0.78, intermediate p = 0.30 and high p = 0.27; Supplementary Fig. S2). In patients with absence of TgAb, DFS was longer in individuals with sTg <10 μg/L than in those with sTg ≥10 μg/L across all ATA groups (p < 0.001, Supplementary Fig. S3).
Extrathyroidal extension
The DFS was significantly different across ETE groups (p < 0.001, Fig. 3). The DFS was longer for DTC, where tumor cells extend microscopically to underlie the junction of the thyroid and adjacent soft tissue (classified as no ETE by ATA guidelines) (15) compared with DTC extending focally out of the thyroid into adjacent perithyroidal connective tissue (classified as minimal/microscopic ETE under ATA guidelines) (15); p = 0.01. There was no difference in DFS between DTC confined to the thyroid and DTC underlying the junction of the thyroid and adjacent soft tissue (p = 0.98), which are grouped together as no ETE in ATA guidelines (15).
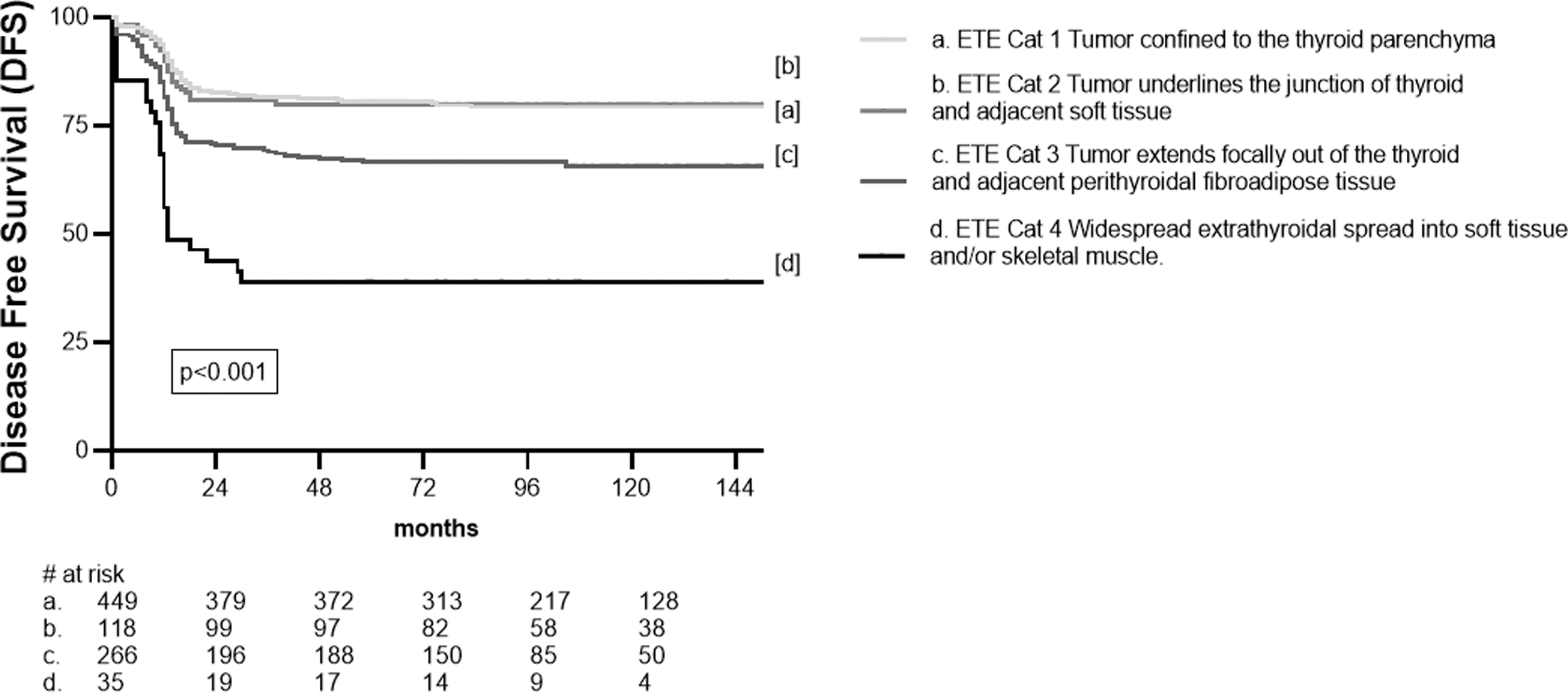
Disease-free survival based on degree of histological ETE. ETE Cat, extrathyroidal extension categories.
Generation of a predictive risk model using the discovery cohort
We created a four-tiered predictive risk model that modified and extended the ATA guidelines by including sTg, tumor size, extent of lymph node involvement, and histological ETE (Fig. 4). Of the 26 patients with synchronous metastases in the discovery cohort, our predictive risk model identified 15 (58%) as high risk, 9 (35%) as intermediate risk, and only 2 (8%) as low risk. Recurrence (defined as receiving a second dose of RAI or further surgery) was identified in 193 patients with complete datasets. Our predictive risk model identified a recurrence rate of 44% (62/142) in the high-risk group compared with 31% (19/61) by ATA Modified Initial Risk stratification (p < 0.001, Supplementary Table S6).
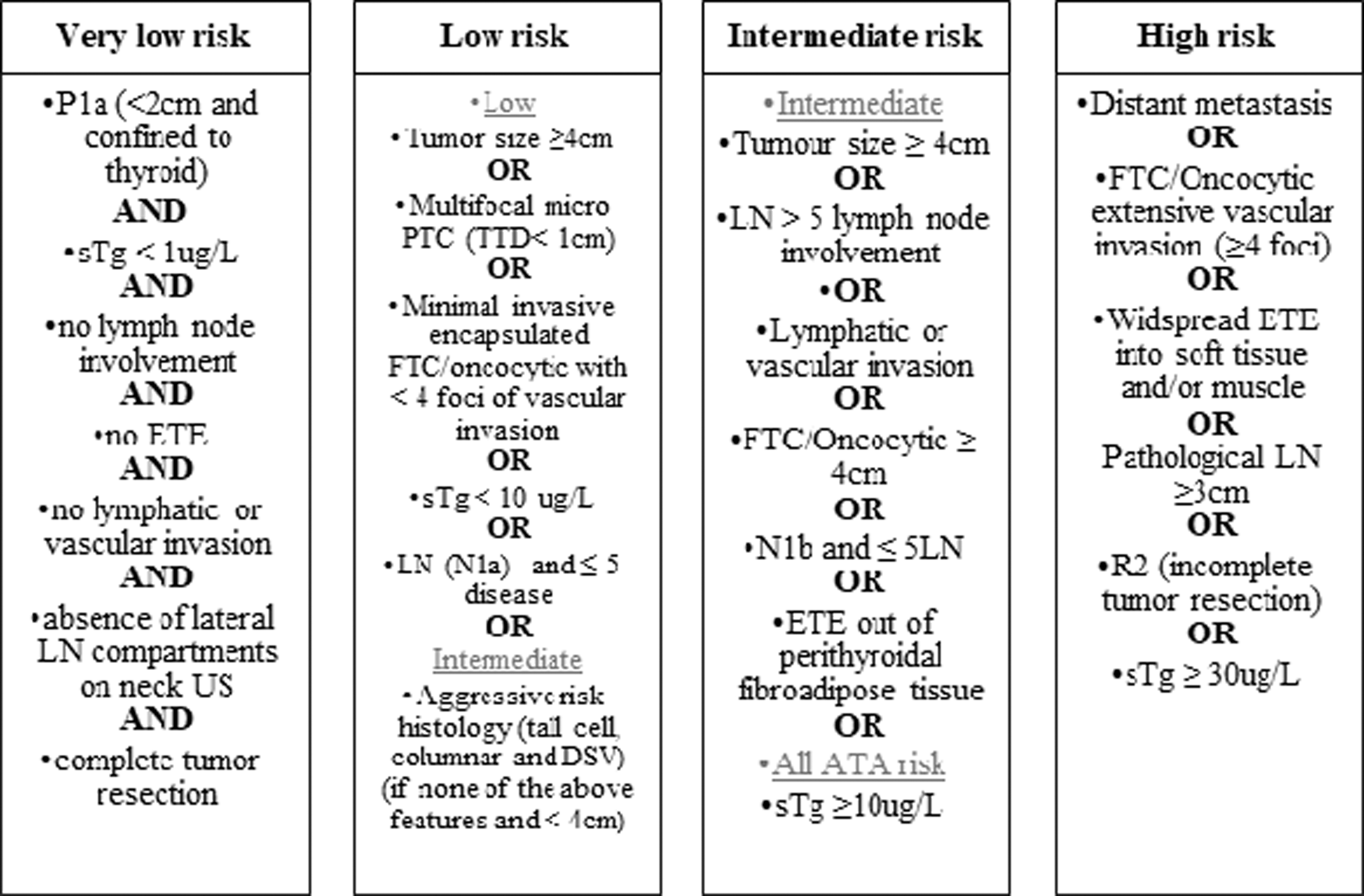
Novel Predictive Risk Model comprising four-tiered risk stratification. DSV, diffuse sclerosing variant; FTC, follicular thyroid cancer; LN, lymph nodes; N1a, central neck lymph node; N1b, lateral neck lymph node; Oncocytic, oncocytic carcinoma of the thyroid; PTC, papillary thyroid cancer; R2, incomplete tumor resection; TTD, total tumor diameter; US, ultrasound.
To avoid confounding by temporal change in the way patients with only central neck disease (including thyroid bed uptake) were treated, further analysis was conducted wherein recurrence included only patients who had received a second dose of RAI for lateral neck or distant disease or further surgical management (n = 51). In this analysis, our predictive risk model identified a recurrence rate of 17/142 (12%) in our high-risk group, 28/426 (7%) in intermediate risk group, 6/217 (3%) in low-risk group, and 0/64 (0%) in very low-risk group (Table 4).
Synchronous Metastasis and Recurrence by Predictive Risk Model vs. ATA in Discovery Cohort (2008–2016)
Synchronous metastasis was defined as distant metastasis (i.e., outside of the neck) that was present at the time of diagnosis on structural imaging or initial post-iodine treatment scan.
ATA, ATA Modified Initial Risk.
Our predictive risk model identified more patients with synchronous metastases or recurrence as high risk (32/77, 42%) compared with ATA Modified Initial Risk stratification (9/77, 12%; p < 0.001) (Fig. 5A). Notably, of the 17 patients stratified as low ATA who had synchronous metastasis or recurrence, our predictive risk model reclassified 7 of these as intermediate or high risk. Further, in our models very low-risk category, no patient had synchronous metastasis or recurrence.
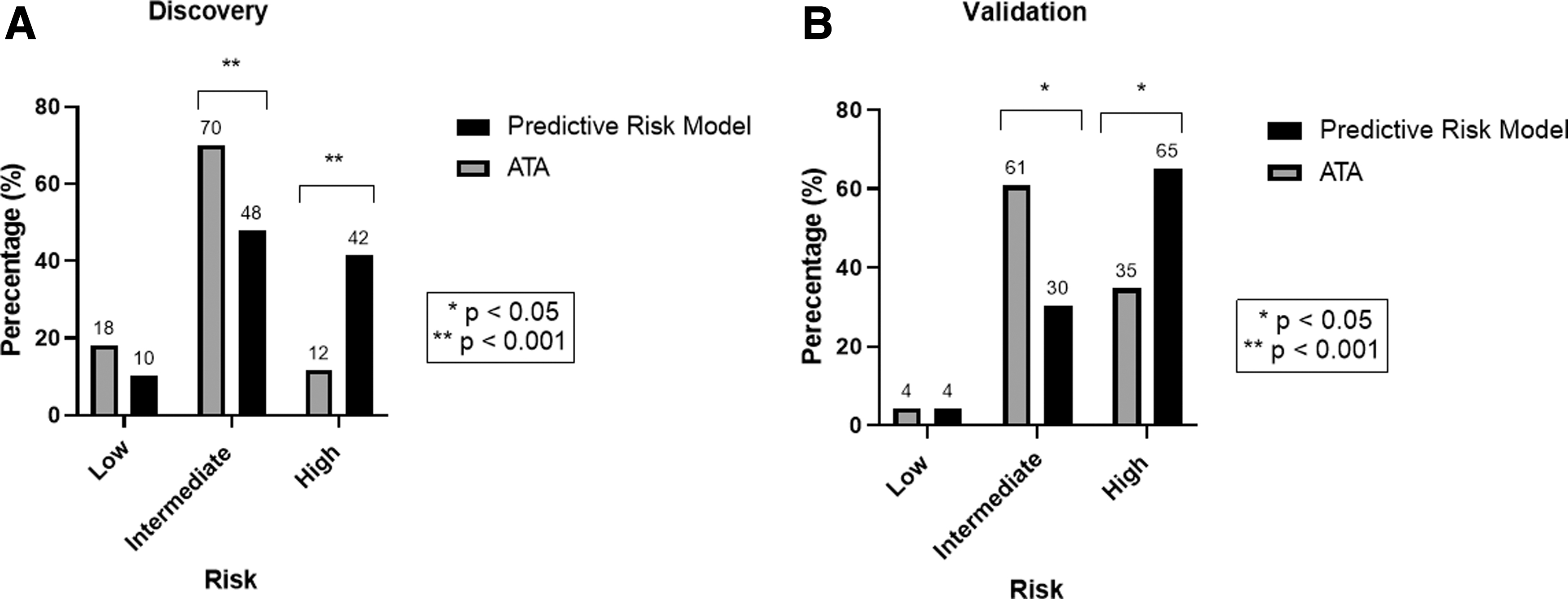
Predictive Risk Model vs. ATA in patients with synchronous metastasis or recurrence. (
Validation of the predictive risk model
Our predictive risk model was validated on a separate cohort of 393 patients after their first treatment with RAI between 2017 and 2021. In the validation cohort, 23 patients had synchronous metastasis (n = 17, 12 identified at initial post-treatment iodine scan and 5 by structural imaging at diagnosis) or clinically significant recurrence (n = 6) (Supplementary Table S1). In our validation cohort, we again identified more patients with synchronous metastases or recurrence as high risk (15/23, 65%) compared with ATA Modified Initial Risk stratification (8/23, 35% p = 0.02) (Fig. 5B and Supplementary Table S3).
Diagnostic accuracy was assessed using ROC analyses and was better using our predictive risk model compared with the ATA classification in both the discovery (area under the curve [AUC] 0.70 vs. 0.56) and validation cohort (AUC 0.75 vs. 0.68).
Discussion
Our study demonstrates that sTg and histological ETE are important additions to the 2015 ATA guidelines for calculating recurrence risk in DTC patients. While the highly validated ATA Modified Initial Risk is now interpreted as a continuum of risk in DTC (3,22), for even the most experienced of clinicians, interpreting the multiple variables together to determine a personalized risk can be challenging. Our predictive risk model not only modifies but also extends the 2015 ATA Modified Initial Risk by creating a four-tiered structured risk stratification, including sTg and histological ETE as well as tumor size, extent of lymph node, and a spectrum of risk in aggressive histology (23,24).
Our predictive risk model included vascular invasion in PTC and extent of vascular invasion in FTC or oncocytic carcinoma, despite our data not showing association with recurrence or synchronous metastasis. We were cautious of removing these variables that have been previously validated and are part of the 2015 ATA Modified Initial Risk. Our new predictive risk model identified patients with synchronous metastasis and recurrence with greater accuracy than the ATA guidelines, while clearly stratifying a group of very low-risk patients who may not require ablative RAI therapy. Further, we were able to significantly reduce the patients stratified as intermediate risk (p < 0.001) for whom the selection of appropriate therapy, in the absence of guidelines, is frequently performed on a “case by case” basis (6).
Although current ATA guidelines do not incorporate Tg into initial risk stratification, an undetectable postoperative Tg has been associated with low likelihood of biochemical or structural recurrence in a low ATA patient (25 –27), while higher postoperative Tg values are associated with an increased risk of recurrence (28). Tian et al. recently demonstrated that sTg <10 μg/L had a high negative predictive value in all three ATA groups and was associated with longer DFS (29). Our data confirm this finding and found that sTg ≥10 μg/L was a critical determinant of recurrence risk, irrespective of ATA. The ATA modified initial risk acknowledges the role of Tg in predicting distant metastasis, however no cutoff was recommended. We found that using a sTg ≥30 μg/L was able to stratify patients as high risk with a specificity of 98%, consistent with other literature (30,31). Further, our data suggest that the presence of TgAbs in patients with an sTg <10 μg/L did not alter recurrence risk.
We used a four-tiered system to classify histologically defined ETE, which divides the tumors into category 1 (confined to the thyroid), category 2 (abuts pseudocapsule of thyroid), category 3 (microscopic invasion into the fat), and category 4 (gross/widespread ETE or invasion into skeletal muscle). It is notable that using this four-tiered system, we have demonstrated that minimal/microscopic ETE (our category 3) predicts recurrent disease.
This contrasts with previous studies, which have found microscopic ETE to not independently predict recurrence-free survival, or disease-specific survival (14,16 –19,32,33). Indeed, it is on the basis of these studies that microscopic ETE alone no longer upstages tumors under the current eighth editions of the AJCC and Union for International Cancer Control staging systems (17,34). To explain this apparent discrepancy, it should be noted that most institutions currently group together our defined ETE category 1 (confined to thyroid away from capsule) and ETE category 2 (confined to thyroid but abuts/underlies the capsule without clear extension into fibroadipose tissue) into the broad group “confined to thyroid.”
In our cohort, 13.5% of patients had tumors that directly underlie the capsule of the thyroid (our category 2). Our data indicate that these tumors clearly behave similarly to those confined to the thyroid (our category 1) and significantly better than those with microscopic extension (our category 3), p = 0.01; they are, therefore indeed, appropriately considered confined to the thyroid. However, other studies indicate that if pathologists are forced to divide these category 2 tumors into either definitely confined to the thyroid or definitely showing microscopic ETE there would be significant interobserver discordance (17 –19).
That is, many of these good prognosis tumors would be misclassified as “microscopic extrathyroidal extension.” This misclassification has the potential to mask the prognostic distinction between tumors with microscopic ETE and those confined to the thyroid—an example of stage migration artificially improving the apparent prognosis of tumors with microscopic ETE, which can be considered an example of the “Will Rogers phenomenon” (35).
In any case, we demonstrate that patients who would have been classified as having microscopic ETE according to the ATA guidelines had worse DFS compared with those with tumors confined to the thyroid (including those that abut the thyroid capsule without clear extension into fat), but better DFS compared with patients whose tumors demonstrated gross/macroscopic/skeletal ETE (most of whom would have been identified in our ETE category 4) (16), and it justifies this approach. Importantly, the use of different systems to grade ETE in different institutions supports the need for clearly defined histological criteria for different degrees of ETE that can be employed across different institutions (36).
A challenge in managing patients with DTC is distinguishing those who require adjuvant treatment from those who require treatment for known or suspected distant metastatic disease. Of all thyroid cancer patients who develop distant metastases, ∼40–55% have these at diagnosis (i.e., synchronous) most commonly in the lung (1,37,38). In our dataset, only 8 of the 45 (18%) patients with synchronous metastasis were known before initial RAI treatment, a similar finding to that of a larger cohort of 140 patients with metastatic DTC (39). With pretreatment whole body iodine scans being less frequently utilized, correctly identifying patients at risk of synchronous metastasis is important for an appropriate selection of RAI activity.
More than 50% of patients with synchronous metastasis are reported to have resolution or stable disease after treatment (37). Our data found that ETE and sTg ≥10 μg/L, in conjunction with multifocal PTC and FTC, predicted synchronous metastasis. By incorporating sTg and histological ETE into our predictive risk model, we were able to identify patients with synchronous metastasis with greater confidence than ATA guidelines.
Our study represents a large cohort of individuals with DTC from a single center, which has not previously had a local protocol to guide specific risk stratification. A particular strength of our study was routine measurement of sTg at the time of RAI treatment, which enabled its strong association between sTg and outcomes to be identified, and more importantly to define thresholds that are incorporated into our risk predictive risk model. The limitations of the study include its retrospective nature, limited follow-up time for our validation cohort, and the absence of data for patients who did not receive RAI treatment.
Notably, sTg was measured at the time of RAI administration, and its incorporation into treatment decisions will require some logistic re-organization. The absence of Tg antibody data from our predictive risk model may lead to an underestimation of recurrence risk; however, on the basis of our findings and that of a previous study from our center, a positive TgAb was associated with a very low risk of recurrence if accompanied by undetectable Tg using an ultrasensitive assay (40). The difficulty in separating invasion of lymphatics from invasion of capillaries with certainty when only small vessel invasion is present may explain the lack of significance of vascular space invasion found in this study.
Indeed, there remains some uncertainty about how confidently capillary and lymphatic space invasion can be separated in routine clinical practice (16). Further, our data did not show association between recurrence and extent of vascular invasion in FTC and Oncocytic carcinoma, which may be due to the small number of patients in our cohort with >4 foci of vascular invasion (n = 18). This would warrant further study in an expanded cohort. Only patients treated with a total thyroidectomy were included in this study, and we have not assessed the utility of our findings in those treated with a lobectomy or hemithyroidectomy. Finally, it is possible that a few patients with recurrence may have been treated outside our institution and therefore not included in our database.
In conclusion, our novel predictive risk model has modified and extended ATA stratification with inclusion of sTg and histological ETE, both identified as independent predictors of recurrence and synchronous metastasis in DTC. Our predictive risk model identified patients with either high or very low risk of synchronous metastasis and recurrence with greater accuracy than the ATA guidelines. Our predictive risk model serves as a platform for future studies to guide RAI treatment decisions in the management of DTC.
Footnotes
Authors' Contributions
A.W.: Ethics approval, analyzed data, developed predictive risk model, and wrote article. A.J.G., M.G., D.L.L., A.R.G., M.S., S.S., P.R., G.S., J.H., B.R., and L.T.: Contributed to predictive risk model development, reviewed and edited article. R.C.-B.: Review of data analysis, idea for predictive risk model and developed predictive risk model, and reviewed and edited article.
Acknowledgments
The authors acknowledge Dr. Adam Aniss, the custodian of the thyroid cancer database at RNSH. The authors acknowledge the technical assistance of Alex Shaw of the Sydney Informatics Hub, a Core Research Facility of the University of Sydney.
Author Disclosure Statement
All authors have no competing financial interests.
Funding Information
No funding was involved in this study.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6