
Abstract
Background:
The current American Joint Committee on Cancer (AJCC) staging system (8th edition) for medullary thyroid cancer (MTC) was originally extrapolated from the staging system for differentiated thyroid cancer. However, the current staging system does not accurately predict the prognosis of patients with MTC.
Patients and Methods:
The present study was based on data from the Surveillance, Epidemiology, and End Results (SEER) database and validated by multicenter data from the Shanghai Tenth People's Hospital, Tongji University School of Medicine, Xuzhou City Central Hospital, and Suzhou Ninth People's Hospital. Hazard ratio with its 95% confidence interval [CI] was estimated by Cox proportional hazards regression analysis. The concordance index (C-index) was used to evaluate the discrimination accuracy of the current AJCC tumor-node-metastasis (TNM) staging system and the modified AJCC (mAJCC) TNM staging system.
Results:
A total of 1175 MTC patients were selected from the SEER database and 312 from the three hospitals in China. We redefined the N category according to the number of metastatic lymph nodes (LNs) as follows: N’0 category (0 metastatic LNs), N’1 category (1–9 metastatic LNs), and N’2 category (≥10 metastatic LNs). The four distinct tumor stages were reclassified in the mAJCC staging system as follows: stage I (T1-4N’0M0, T1N’1M0), stage II (T2-3N’1M0, T1N’2M0), stage III (T4N’1M0, T2-4N’2M0), and stage IV (TanyN'anyM1). The C-index of the current AJCC staging system and the mAJCC staging system was 0.72 [CI, 0.67–0.78] and 0.78 [CI, 0.73–0.84], respectively. Similar results were observed in the survival analysis of the multicenter data set.
Conclusions:
The mAJCC staging system could discriminate the prognosis of MTC patients more effectively than the current AJCC staging system, indicating that it is feasible and appropriate to modify the current AJCC staging system by introducing the number of metastatic LNs instead of the location of LNs. These findings might be adopted in the next edition of the AJCC staging system and be used to guide clinical practice.
Introduction
Medullary thyroid cancer (MTC) is a relatively rare malignancy compared with differentiated thyroid cancer (DTC), approximately accounting for 1–2% of thyroid cancer (1). MTC is regarded as a neuroendocrine tumor arising from calcitonin-producing parafollicular cells (C cells) of the thyroid gland (2). The majority of MTC cases (∼75%) are sporadic, while the remaining 25% are hereditary (3,4). Its incidence has been rapidly increasing over the past few decades worldwide (5 –7). Early-stage MTC has a favorable prognosis. However, almost half of the MTC patients have lymph node (LN) or distant metastasis when initially diagnosed, thereby resulting in poor clinical outcomes (5,8). Therefore, the accurate prognostic evaluation is crucial for risk stratification and individualized precision therapy strategy of MTC patients.
The current American Joint Committee on Cancer (AJCC) tumor-node-metastasis (TNM) staging system (8th edition) for MTC was originally extrapolated from the staging system for DTC (9). However, MTC and DTC are derived from two distinct cells: the former from parafollicular cells (C cells) and the latter from follicular epithelial cells (10). Differences in the cellular origin determine different clinical features and outcomes. DTC is characterized by an excellent prognosis, and age is a highly significant prognostic factor in DTC, which has been included in the AJCC TNM staging system (11). In contrast, MTC patients usually have a relatively worse prognosis and the effect of age on MTC remains controversial (12 –14). This suggests that the current AJCC TNM staging system might not accurately predict the prognosis of MTC patients.
Wang et al. (15) showed that MTC patients with stage I, II, and III had a similar prognosis (p > 0.05). Park et al. (16) validated the prognostic performance of the current AJCC TNM staging system using the data from a single tertiary Korean hospital and found that the death risk is not significantly distinguishable among all the four tumor stages. The 10-year cancer-specific survival rates of patients with stage IV were even much higher than those with stage III (79.7% vs. 54.7%). This indicates that the improvement of the current AJCC TNM staging system is warranted.
The N category is defined by the location of metastatic LNs in the current AJCC TNM staging system. However, prior studies have shown that the number of LN metastases may correlate better with risk of mortality in patients with MTC (17,18). Therefore, we aimed to evaluate whether the LN number-based AJCC TNM staging system could provide more accurate prognostic information than the current location-based staging system.
Materials and Methods
Patient data
The LN number-based AJCC TNM staging system was developed based on data from the Surveillance, Epidemiology, and End Results (SEER) database. The SEER database is one of the largest clinical databases globally, which covers ∼26% of the US population (19). We identified MTC patients according to the 3rd edition of the International Classification of Diseases for Oncology (codes 8345/3 and 8510/3). MTC patients diagnosed between 2004 and 2015 (2329 cases in total) were selected from the SEER database because information regarding pathologic tumor stages was incomplete before 2004. Demographic and clinical features were collected, including age, gender, race/ethnicity, AJCC TNM stage, the number of metastatic LNs, survival time, and mortality.
The inclusion criteria were as follows: (i) aged 18 years or older; (ii) histopathological confirmation of MTC; (iii) MTC as first primary malignancy; (iv) definite T category, N category, and M category according to the 8th edition of AJCC TNM staging system (detailed definitions: T1, tumor ≤2 cm or less in greatest dimension limited to the thyroid; T2, tumor >2 cm but ≤4 cm in greatest dimension limited to the thyroid; T3, tumor >4 cm limited to the thyroid, or gross extrathyroidal extension invading only strap muscles; T4, including gross extrathyroidal extension beyond the strap muscle; N0, no evidence of locoregional LN metastasis; N1, metastasis to regional LNs; M0, no distant metastasis; M1, distant metastasis); (v) definite number of metastatic LNs; and (vi) available follow-up information. Patients were excluded if any of the above data were missing.
The primary endpoint of the study is overall survival (OS), which refers to the period from the initial diagnosis of MTC to the date of death from all causes or the last follow-up time. The follow-up period ranged from 0 to 143 months with a median follow-up of 53 months. A total of 144 cases died during the follow-up period.
External validation data sets were obtained from the multicenter cohort, which included the Shanghai Tenth People's Hospital, Tongji University School of Medicine, Xuzhou City Central Hospital, and Suzhou Ninth People's Hospital (2010–2017). All the participants were Chinese. The inclusion criteria were the same as those of the SEER database. The follow-up period ranged from 1 to 94 months with a median follow-up of 31 months. The present study followed the STROBE reporting guidelines (20) and was approved by the Bioethics Committee of Shanghai Tenth People's Hospital, Tongji University School of Medicine, P.R. China.
Statistical analysis
The optimal cutoff value of metastatic LNs was determined by the X-tile software (version 3.6.1; Yale University). The X-tile software would try every possible cutoff value and automatically calculate the corresponding survival differences between the three subgroups using the Kaplan–Meier (KM) methods and the log-rank test. The cutoff value was defined as the optimal cutoff value when the most significant survival difference was reached. The minimum number of LNs examined was also determined by the X-tile software. The rationale was that as the number of LNs examined increased, the survival difference increased between patients with an adequate LN number and those with an inadequate LN number. When the number of LNs examined continued to increase, the survival difference stopped increasing, and the LN number was regarded as the minimum number of LNs examined.
The survival analysis was performed using the KM methods. Hazard ratio (HR) with its 95% confidence interval [CI] was estimated by Cox proportional hazards regression analysis. Both the KM methods and Cox analysis were conducted in IBM SPSS Statistics 22.0 (IBM SPSS, Inc.). The concordance index (C-index) and likelihood ratio test were used to evaluate the discrimination accuracy of the current AJCC TNM staging system and the modified AJCC (mAJCC) TNM staging system, which were conducted in RStudio (R Version 3.6.2). p < 0.05 was considered statistically significant.
Results
Demographic and clinical features
After applying the inclusion criteria, a total of 1175 MTC patients were selected from the SEER database between 2004 and 2015 in the study (median age [range], 52 [18–99]). As shown in Table 1, there was a female predominance with a male-to-female ratio of 1:1.38. Most of the patients were white. Three hundred twenty-two (27.4%) patients were classified as stage I, 224 (19.1%) as stage II, 154 (13.1%) as stage III, and 475 (40.4%) as stage IV. Five hundred fifty-six patients were classified as N0 category, 184 as N1a category, and 422 as N1b category according to the 8th edition of AJCC TNM staging system.
Clinicopathologic Factors of Medullary Thyroid Cancer Patients
Including American Indian/Alaskan Native, Asian/Pacific Islander, Chinese, and unknown race/ethnicity.
AJCC, American Joint Committee on Cancer; LN, lymph node; NOS; not otherwise specified; SEER, Surveillance, Epidemiology, and End Results.
The optimal cutoff value of metastatic LNs
The optimal cutoff value of metastatic LNs determined by the X-tile software is shown in Figure 1A. All the patients with metastatic LNs (619) were divided into three risk groups. There were 355 patients with 1–9 LNs in the low-risk group, 198 patients with 10–24 LNs in the intermediate-risk group, and 66 patients with ≥25 LNs in the high-risk group (Fig. 1B). The HRs of the high-risk group and intermediate-risk group were 1.55 [CI, 1.03–2.32] and 2.64 [CI, 1.63–4.29] with the low-risk group as the reference, respectively (Fig. 1C). Due to the low number of patients in the high-risk group, the high-risk group and intermediate-risk group were combined into a single group.

The optimal cutoff value of metastatic LNs. Panels displaying the cutoff points. Each point represents a possible partition and the corresponding χ2 log-rank value was generated. The darker (blacker) the color is, the weaker the correlation between LN and survival. The brighter (redder or greener) the color is, the greater the correlation between LN and survival. (
Thus, we redefined the N category according to the number of metastatic LNs as follows: N’0 category (0 metastatic LNs), N’1 category (1–9 metastatic LNs), and N’2 category (≥10 metastatic LNs). The HR of N’2 category was 1.82 [CI, 1.27–2.62] with N’1 category as the reference. In addition, at least 17 LNs should be examined to guarantee the accuracy of the new N category.
mAJCC staging system
The entire cohort was divided into 13 subgroups as follows: T1N’0M0, T2N’0M0, T3N’0M0, T4N’0M0, T1N’1M0, T2N’1M0, T3N’1M0, T4N’1M0, T1N’2M0, T2N’2M0, T3N’2M0, T4N’2M0, and TanyN'anyM1. The survival analysis was performed, and the 5-year survival rate of each group was calculated (Supplementary Fig. S1). According to the principle of similar survival rates within the same tumor stage and maximum survival differences among different tumor stages, the above 13 subgroups were reclassified as 4 distinct tumor stages as follows: stage I (T1-4N’0M0, T1N’1M0), stage II (T2-3N’1M0, T1N’2M0), stage III (T4N’1M0, T2-4N’2M0), and stage IV (TanyN'anyM1) (Table 2). The C-index of the current AJCC TNM staging system and the mAJCC TNM staging system was 0.72 [CI, 0.67–0.78] and 0.78 [CI, 0.73–0.84], respectively (Fig. 2A, B).
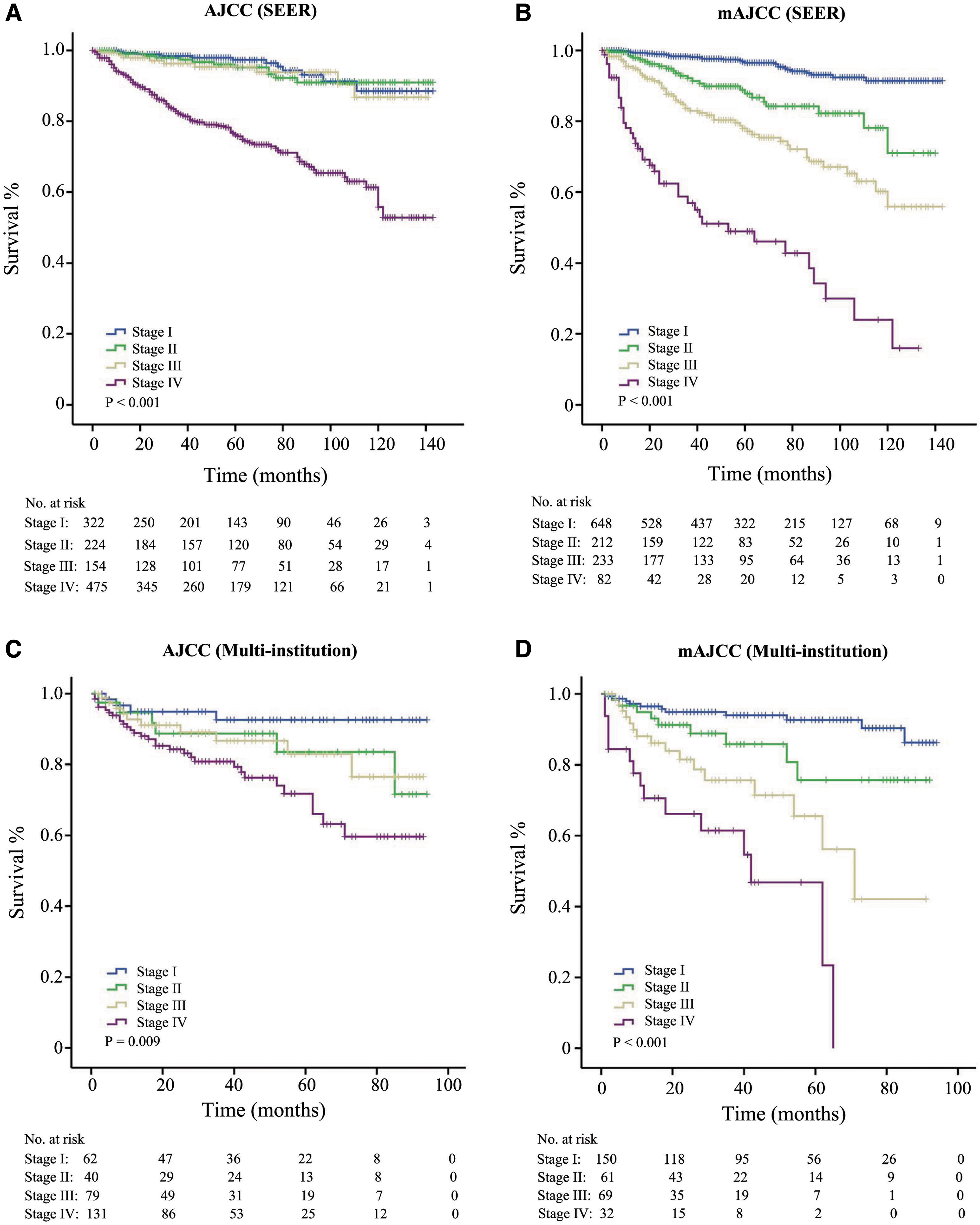
KM survival curves. (
Comparison of Different Tumor-Node-Metastasis Groupings Between the American Joint Committee on Cancer and Modified American Joint Committee on Cancer Tumor-Node-Metastasis Staging System
mAJCC, modified AJCC.
The likelihood ratio test (χ2 = 66.43, p < 0.001) indicated that the mAJCC TNM staging system fitted the patient data better than the current AJCC TNM staging system. Cox proportional hazards regression analysis revealed that there were no significant survival differences among stage I, II, and III according to the current AJCC staging system (Table 3, p > 0.05). However, highly significant differences were observed among stage I, II, and III according to the mAJCC staging system (Table 3, p < 0.001).
Comparison of 5-Year Survival Rates and Hazard Ratios Between the American Joint Committee on Cancer and Modified American Joint Committee on Cancer Tumor-Node-Metastasis Staging System
CI, confidence interval; HR, hazard ratio.
Multicenter validation
A total of 312 MTC patients were selected from the multicenter (median age [range], 57 [23–76]). Similar results were observed. The AJCC staging system showed that the HRs of stage II, III, and IV were 2.39 ([CI, 0.67–8.46], p = 0.178), 2.42 ([CI, 0.76–7.71], p = 0.136), and 4.51 ([CI, 1.59–12.79], p = 0.005) with stage I as the reference, respectively (Fig. 2C). The mAJCC staging system showed that the HRs of stage II, III, and IV were 2.48 ([CI, 1.02–5.99], p = 0.044), 5.60 ([CI, 2.56–12.30], p < 0.001), and 13.01 ([CI, 5.79–29.22], p < 0.001), with stage I as the reference, respectively (Fig. 2D).
Discussion
Many staging and prognostic scoring systems have been proposed worldwide, including the European Organization for Research and Treatment of Cancer (EORTC), National Thyroid Cancer Treatment Cooperative Study (NTCTCS), SEER staging system, and AJCC TNM staging system (9,13,21). The AJCC TNM staging system is the most widely used staging system for MTC in clinical practice, which is also recommended by the British Thyroid Association (BTA) and American Thyroid Association (ATA) (22,23).
In the present study, we used the data from the SEER database to modify the current AJCC TNM staging system and confirmed the prediction accuracy of the mAJCC staging system using the multicenter data. The mAJCC staging system could discriminate the prognosis of MTC patients more effectively than the current AJCC staging system, indicating that it is feasible and appropriate to modify the current AJCC TNM staging system by introducing the number of metastatic LNs instead of the location. These findings might be adopted in the next edition of AJCC staging system and be used to guide clinical practice.
The number of metastatic LNs has been reported as an independent prognostic factor for MTC in various studies (17,18,24). Tang et al. (24) categorized MTC patients into three groups: classification I (0–1 positive LNs), classification II (2–9 positive LNs), and classification III (10–58 positive LNs). Although the death risk of classification II and III was much higher than classification I, there was no significant survival difference between classification II and III (with classification I as the reference: HRs with CI for classification II, 7.68 [4.00–14.73]; HRs with CI for classification III, 9.62 [4.97–19.61], p > 0.05). Esfandiari et al. (17) found that the OS for 1–5, 6–10, 11–16, and ≥16 positive cervical LN metastases was 90, 76, 74, 61, 69, and 55%, respectively.
Similar to our findings, Meng et al. (25) classified patients into 0 positive LN, 1–10 positive LNs, and ≥11 positive LNs, and statistically significant risk differences were observed among three classifications (with 0 LN as the reference: HRs with CI for 1–10 LNs, 1.76 [1.18–2.64]; HRs with CI for ≥11 LNs, 2.66 [1.76–4.02]). In fact, numerous efforts had been made to improve the N classification. Lymph node ratio (LNR) refers to the ratio of positive to resected LNs and the log odds of positive lymph nodes (LODDS) refer to the log of the ratio of positive to negative LNs, both of which were also reported to be important prognostic predictors in a variety of malignancies, including MTC (26 –33). However, their predictive power is considerably limited by both positive LNs and negative LNs, and the complex computational method also largely hinders a wide range of their application in clinical practice.
The current AJCC staging system could not precisely distinguish the prognosis gap among patients with stage I, II, and III. Therefore, in the present study, all patients with stage II and a significant number of patients with stage III and IV in the AJCC staging system were downstaged to stage I in the mAJCC staging system. This could not only reflect their death risk more precisely, but also make the survival differences across stage I–III more apparent. Of note, most T4 patients (96.9%, 126/130) developed LN or distant metastasis and only four T4 patients (T4N0M0) did not. It is still debatable to classify T4N0M0 into stage I.
Unlike our results, Wang et al. (15) proposed a new TNM staging system, in which patients with T4N0M0 were classified as stage III. However, only seven patients with T4N0M0 were included for survival analysis in their study. Therefore, more data samples are needed to evaluate the prognosis of such patients.
Stage IV of our mAJCC staging system only included patients with distant metastasis. The 5-year survival rates declined significantly from 76.1% of the AJCC staging system to 48.9% of the mAJCC staging system. The change highlighted that patients with distant metastasis were a high-risk population with higher mortality. The same view was also supported by other proposed staging systems for MTC (9,15).
There are a few limitations in the present study. First, both the SEER and multicenter data sets are retrospective with selection bias, which might have an influence on the predictive accuracy. However, validating in a completely different cohort (Chinese vs. US population) decreased the risk of selection bias and increased generalizability.
Second, the mAJCC staging system did not include carcinoembryonic antigen (CEA) levels or calcitonin levels, which were important prognostic indicators for MTC. Preoperative basal serum calcitonin levels were reported to be associated with the extent and recurrence of MTC (34,35), and the calcitonin doubling time was also an important prognostic and predictive marker in MTC (36). Studies have revealed that CEA levels usually had a significant positive correlation with the severity of MTC (37). A higher CEA level may lead to a higher likelihood of LN metastasis (38). Thus, inclusion of CEA and calcitonin could be more reflective of the biological characteristics of MTC and distinguish patients with significantly different prognoses more effectively.
Third, the sample size with available long-term follow-up was small in the multicenter data sets, which might weaken the power of the external validation cohort to some extent. Fourth, combining the high-risk group and intermediate-risk group may slightly reduce the accuracy of the mAJCC staging system. Larger sample sizes are needed to further refine the staging system in the future.
In summary, the mAJCC staging system could discriminate the prognosis of MTC patients more effectively than the current AJCC staging system, indicating that it is feasible and appropriate to modify the current AJCC staging system by introducing the number of metastatic LNs instead of the location. These findings might be adopted in the next edition of AJCC staging system and be used to guide clinical practice.
Footnotes
Authors' Contributions
Z.W.: data generation and article preparation. C.T. and Y.W.: data generation. Z.Y. and Y.R.: data generation and article review.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Z.Y.: Shanghai Municipal Commission of Health and Family Planning Commission (2019SY062).
Supplementary Material
Supplementary Figure S1