
Abstract
Background:
Thyroid hormone has a differential action on healthy and ischemic heart. Triiodothyronine (T3) administration improved postischemic cardiac function while it limited apoptosis in experimentally induced ischemia. Thus, the present study investigated the potential effects of acute liothyronine (LT3) treatment in patients with anterior myocardial infarction.
Methods:
This study is a pilot, randomized, double-blind, placebo-controlled trial (ThyRepair study). We randomized 52 patients and analyzed data from 37 patients (n = 16 placebo and n = 21 LT3), per prespecified per protocol analysis. We excluded three patients who had died of cardiovascular causes (one in placebo and two in LT3 arm), four with small infarct size below a pre-specified threshold (in the placebo arm), and the rest, who lacked follow-up data. LT3 treatment started after stenting as an intravenous (i.v.) bolus injection of 0.8 μg/kg of LT3 followed by a constant infusion of 0.113 μg/kg/h i.v. for 48 hours. All patients had cardiac magnetic resonance (CMR) at hospital discharge and 6 months follow-up. The primary end point was CMR left ventricular (LV) ejection fraction (LVEF) and secondary endpoints were LV volumes, infarct volume (IV), and safety.
Results:
The CMR LVEF% at 6 months was 53.6 ± 9.5 for the LT3-treated group and 48.6 ± 11 for placebo, p = 0.15. Acute LT3 treatment resulted in a significantly lower LV end-diastolic volume index (92.2 ± 16.8 mL/m2 vs. 107.5 ± 22.2, p = 0.022) and LV systolic volume index (47.5 ± 13.9 mL/m2 vs. 61.3 ± 21.7, p = 0.024) at hospital discharge, but not at 6 months. There was no statistically significant difference in CMR IV at hospital discharge between the groups (p = 0.24). CMR IV tended to be lower in the LT3-treated group at 6 months (18.7 ± 9.5 vs. 25.9 ± 11.7, in placebo, p = 0.05). Serious, life-threatening events related to LT3 treatment were not observed. A tendency for an increased incidence of atrial fibrillation (AF) was found in the LT3 group during the first 48 hours (19% for T3 group vs. 5% for placebo, p = 0.13).
Conclusion:
This pilot randomized, placebo-controlled trial study suggests potential favorable effects (acute cardiac dilatation and 6-month IV) as well as potential concerns regarding a higher risk of AF after LT3 administration early after myocardial infarction, which should be tested in a larger scale study.
Introduction
Despite the advances in the therapy of acute myocardial infarction (AMI), the number of patients in whom heart failure develops is increasing (1,2). Cardiac dilatation occurs early in these patients and is associated with poor prognosis (3). Reperfusion injury and cardiac remodeling are considered the main causes of postischemic cardiac dysfunction.
Cardiac remodeling starts after restoration of blood flow and is characterized by reactivation of the fetal transcriptional program (4). Interestingly, the damaged heart seems to resemble the developing heart, suggesting that the same regulatory network drives both embryonic heart development and heart repair. Thus, cell-based treatments and hormones such as thyroid hormone (TH) implicated in organ maturation are considered as potential therapies for the repair of the injured myocardium (4,5).
TH signaling has been implicated in the pathophysiology of postinfarcted cardiac remodeling (6 –8), and low triiodothyronine (T3) syndrome and subclinical hypothyroidism are associated with poor prognosis in patients with AMI (9 –11). TH when administered early and above physiologic doses was shown to prevent cardiac remodeling in experimental AMI (12 –15) without increasing cardiac damage due to the differential effect of TH on the injured and healthy myocardium (13,16,17). Along this line, T3 administration could prevent tissue hypoxia (18) and erythrocyte aggregation in critically ill patients with an impact on microcirculation and cardiac damage (19).
TH has been administered as replacement therapy late after AMI and as early treatment at high dose in bypass surgery (20). Thus, T3 was administered after 72 hours and continued for 6 months in patients with reperfused AMI without any effect on cardiac magnetic resonance (CMR) infarct volume (IV), left ventricular (LV) volumes, and ejection fraction. The CMR wall motion score index recovered in both placebo and T3 groups but to a greater extent in T3-treated patients (21). Similarly, thyroxine (T4) replacement therapy was initiated within 21 days in patients with AMI and subclinical hypothyroidism and no significant changes in cardiac function and damage were observed (22). In contrast to those studies, acute, high-dose T3 administration improved hemodynamics and reduced troponin release without major safety issues in bypass surgery (20), indicating that early administration of T3 may be of benefit in the clinical setting of ischemia-reperfusion.
On the basis of this evidence, the present pilot study aims at investigating the potential effects and safety of early, high-dose liothyronine (LT3) administration on LV function, volumes, and infarct healing in patients with anterior myocardial infarction.
Methods
Study design
The present pilot, double-blinded, randomized, controlled trial was designed to investigate the potential effects of acute T3 treatment in patients with AMI. The study (ThyRepair study, EudraCT: 2016-000631-40) was performed in accordance with the Declaration of Helsinki (revised version, 1996) and the European Guidelines for Good Clinical Practice (version July 11, 1990). Study protocol was approved by the National Independent Ethics Committee (26/16, 31-3-2016) and the Greek Drug Agency. All subjects gave written informed consent. The study was conducted in two clinical centers.
The primary endpoint of the study was LV ejection fraction (LVEF%) at 6 months assessed by CMR. Prespecified secondary outcomes were LVEF% at discharge from hospital, LV and right ventricular (RV) volumes (end-systolic and end-diastolic per meter squared body surface area), LV mass index, IV of LV myocardium at discharge and at 6 months follow-up, and microvascular obstruction (MVO) at hospital discharge and safety. LVEF% and LV volumes have been previously reported to be powerful predictors of all-cause mortality and heart failure hospitalizations in patients with ST-elevation myocardial infarction (STEMI) treated with primary percutaneous coronary intervention (PCI) (23).
According to previous reports (24,25), a difference in ejection fraction ≥5 U in response to treatment is considered clinically important. Thus, the present study was set to detect a minimum difference of 7 U in ejection fraction at 6 months between the groups (in favor of treatment group). Mean ± standard deviation (SD) of LVEF% in the placebo group at 6 months after anterior or antero-lateral STEMI was roughly estimated as 40 ± 7%.
With these assumptions a sample size of 50 patients (that indicates 25 subjects for each group) was estimated to detect a mean difference of at least 7 U in the ejection fraction at 6 months between the two study groups with 93% power. The criterion for significance (alpha) was set at 0.05, and the test was two-tailed. The effect size of this difference was estimated to be large (d = 1.0).
Men and women, 18 years of age or older who presented within 12 hours after the onset of chest pain and were diagnosed with anterior or anterolateral STEMI according to the ESC guidelines were included in the study. Patients were eligible to participate whether they had primary PCI or rescue PCI of the culprit lesion with a successful result (Thrombolysis in myocardial infarction flow grade 2 or 3).
Patients older than 75 years or patients with acute cardiac decompensation, stroke within 90 days, or major surgery within 30 days before screening or severe systemic disease (e.g., cancer, auto-immune) accompanied by reduced life expectancy <1 year, patients with previous AMI, previous history of thyroid disease, significant chronic hepatic impairment, patients with impaired renal function and GFR <60 mL/min, patients with known hypersensitivity to THs, and pregnant women or at childbearing age and not using contraception were excluded from the study. Patients on treatment with amiodarone, anti-thyroid drugs, or T4 at the time of admission were not included. Patients holding mechanical cardiac valves, pacemakers, implantable cardioverter defibrillator, or magnetic materials such as metallic clips and prosthesis who could not be subjected to CMR were excluded.
Safety and adverse events were assessed throughout the study. The following expected serious adverse events related to AMI were assessed: death, sudden cardiac death, syncope, myocardial rupture, mitral valve dysfunction and regurgitation, acute pericarditis, Dressler syndrome, LV aneurysm, LV mural thrombus and/or embolism, congestive heart failure, acute pulmonary edema, cardiogenic shock and hypotension, coronary revascularization, RV failure, new myocardial infarction, angina, stroke, severe renal failure, bleeding, ventricular fibrillation or sustained ventricular tachycardia, rhythm disturbances, and serious bradycardia that require a pacemaker implantation, paroxysmal supraventricular tachycardia, atrial flutter, and atrial fibrillation (AF).
Further, the following potential side effects associated with T3 treatment were assessed: allergic reactions, chest pain, shortness of breath, arrhythmias and tachycardia, hypotension, myocardial infarction, angina and congestive heart failure, insomnia, headache, leg cramps, diarrhea, abdominal cramps, seizures, tremors, nervousness, or irritability, menstrual irregularities, phlebitis, nausea or vomiting, fever, sweating, or heat intolerance, changes in appetite, or weight loss, hypertension, skin flushing, hypoglycemia, and adrenal insufficiency.
Interventions
After coronary angiography was performed but before the stent was implanted, patients were randomly allocated with a 1:1 ratio to receive LT3 treatment or placebo starting immediately after reperfusion for 48 hours. Simple randomization without restriction and stratification was performed with the use of a computer-generated randomization sequence. Allocation concealment was performed with the use of sealed, sequentially numbered identical containers of the drug or placebo according to the allocation sequence. Assignments were enclosed in sequentially numbered, opaque, sealed envelopes that were monitored diligently. Trial investigators, medical and nursing staff, as well as recruited patients were blinded to allocation.
LΤ3 was administered as intravenous (i.v.) bolus injection of 0.8 μg/kg of 3,3′,5 triiodo-L-thyronine sodium followed by a constant infusion of 0.113 μg/kg/h i.v. for 48 hours by using a pump. The median dose of LT3 during the 48 hour period was calculated at 500 μg. This dose was in accordance with preclinical evidence (Section A in Supplementary Material) and previous use of T3 treatment in bypass surgery (20). LT3 was dissolved in water for injection containing dextran 70 (60 mg/mL) and NaOH 1N to produce T3®Solution for injection with a final concentration of 10 μg/mL (UniPharma Pharmaceutical Laboratories S.A., Greece). Patients in the placebo group received equivalent volumes of vehicle with an identical composition apart from the active substance.
Study procedures
Participants had standard laboratory assessment, physical examination, and electrocardiograms on admission and at 24, 48, and 72 hours, discharge, and 3 and 6 months after the index event.
Coronary angiography was performed just before revascularization. Coronary angiographic findings and ischemic time (calculated from onset of symptoms to the time of the coronary intervention) for patients with STEMI were recorded. The area at risk, a major determinant of infarct size, was estimated for each patient by calculating the modified APPROACH score based on angiographic findings (26).
The CMR was performed at discharge and at 6 months at a single center (Department of Radiology, IASO Hospital of Athens). All MRI analyses were performed at the same core laboratory by using the freely available for research purposes software Segment, version 2.0 R5201 (
Standardized transthoracic echocardiography exams were performed at 48 hours by using a commercially available system (Vivid E9; GE-Vingmed Ultrasound, Athens, Greece) and a 3.5-MHz transducer (Fig. 1).
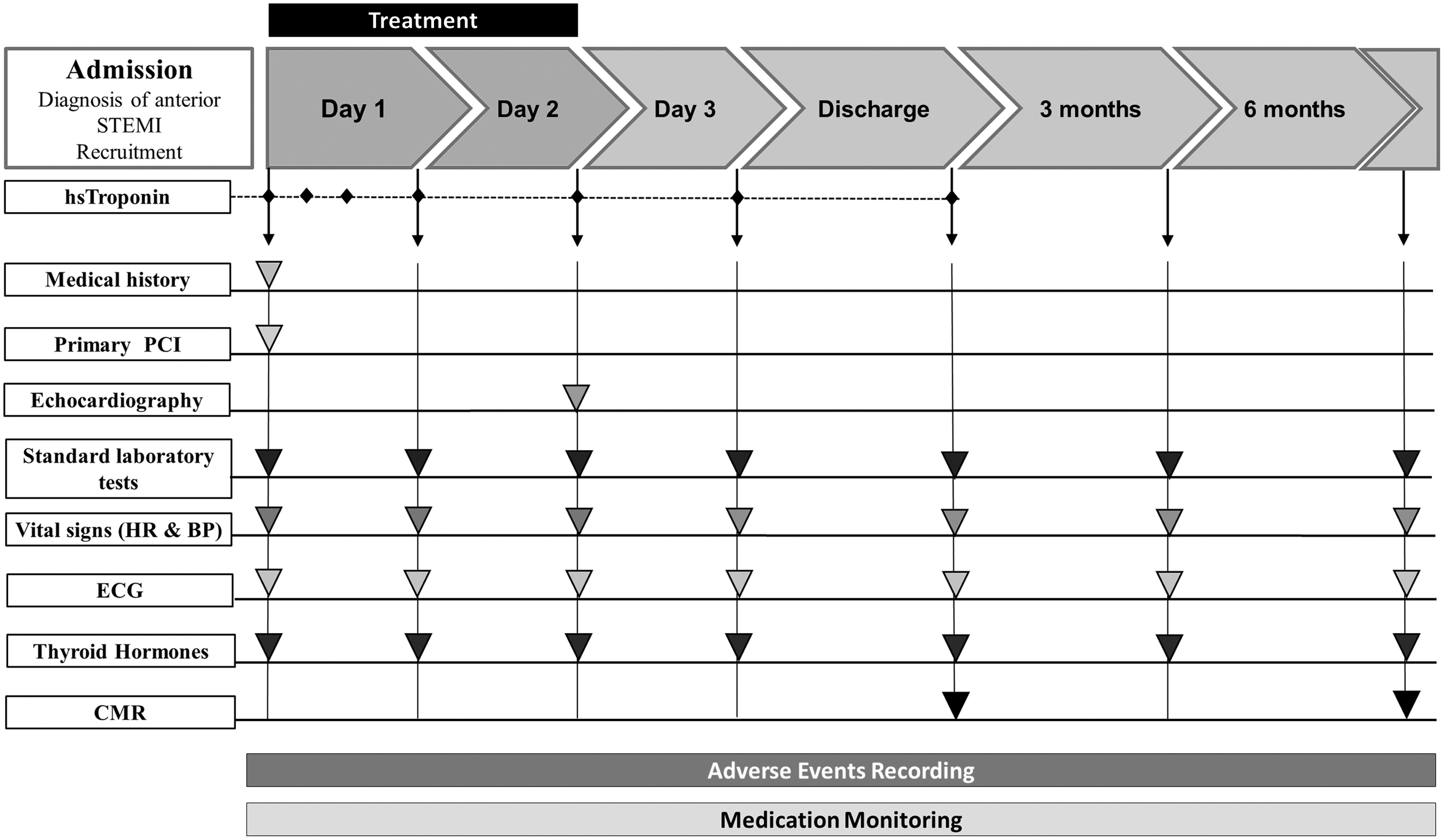
A study scheme figure including timing and procedures of the ThyRepair trial. BP, blood pressure; CMR, cardiac magnetic resonance; ECG, electrocardiogram; HR, heart rate; LV, left ventricle; PCI, percutaneous coronary intervention; STEMI, ST-elevation myocardial infarction.
Biochemical analyses
High-sensitive (hs) Troponin was evaluated on admission, at 6, 12, 24, 48, and 72 hours, and on discharge. Sequential hs troponin I measurements were used to determine the area under the curve (AUC) (expressed in arbitrary units) in each patient by computerized planimetry. Troponin AUC was used to determine the extent of myocardial injury, which was a prespecified secondary outcome (Fig. 1).
TH profile, including thyrotropin (TSH), total T3, and total T4, was determined in blood samples at different time points (admission, 24 hours, 48 hours, 72 hours, discharge, 3 months, and 6 months) and sequential T3 measurements during hospitalization were used to estimate the AUC (expressed in ng*h/mL) in each patient by computerized planimetry (T3 treatment exposure). Blood samples for TH levels on admission were taken immediately before T3 treatment (Fig. 1).
A detailed description of measurement of THs and troponin and reference ranges is included in the Supplemental Methods Section in Section B of Supplementary Material.
Statistical analysis
Data analysis was based on a prespecified plan. A complete case analysis was performed since missing data were very low. Efficacy (per protocol) analysis was used to assess treatment efficacy. This pilot randomized, placebo-controlled trial (RCT) was not planned to address treatment effectiveness and thus, intention-to-treat analysis was not performed. Categorical data are shown as numbers of patients and percentages, whereas continuous variables are expressed as means ± SDs.
An additional analysis showing primary and secondary endpoints as means or medians with 95% confidence intervals (CI) was included in the Supplemental Results Section in Section B of Supplementary Material to present the range of possible responses. Categorical data were compared by using Chi-square and the Fisher's exact test. Normal distribution of variables was estimated with Shapiro–Wilk test of normality. Normally distributed data were compared by using an independent t-test. Comparisons between CMR variables at discharge and at 6 months were performed with a paired-samples t-test.
Skewed data (total ischemic time, area at risk, MVO at discharge, and LVEDVI and LVESVI at 6 months) were analyzed non-parametrically by using the Mann–Whitney U test. Simple linear regression analysis was used to assess the correlation between total T3 treatment exposure and response (e.g., heart rate).
All reported p-values are two-sided, and a value of <0.05 is deemed as indicative of statistical significance. Analyses were performed by using the statistical software package SPSS version23 (IBM).
Results
CONSORT guidelines on the reporting of pilot RCTs were followed (27). Patient enrolment started in September 2016 and was completed in June 2020. The last visit of the last completed patient was in November 2020. During the study enrolment period, 155 patients were admitted to two participating hospitals with anterior, anterolateral ST-elevation AMI and 52 patients were recruited in the study based on the inclusion/exclusion criteria (recruitment rate 35.5%) and the consent to participate (rate 94.5%).
Of these 52 participants, 28 participants were randomized to the LT3 group and 24 to the placebo group (Fig. 2). Four participants dropped out during the first 48 hours due to the following reasons: unsuccessful revascularization of the culprit lesion, violation of criteria for diagnosis of anterior STEMI, not eligible due to hemodynamic instability, and improper investigational drug administration. One participant was lost to follow-up, while another two patients could not be subjected to CMR due to claustrophobia. One participant dropped out from the study after amiodarone treatment due to AF.
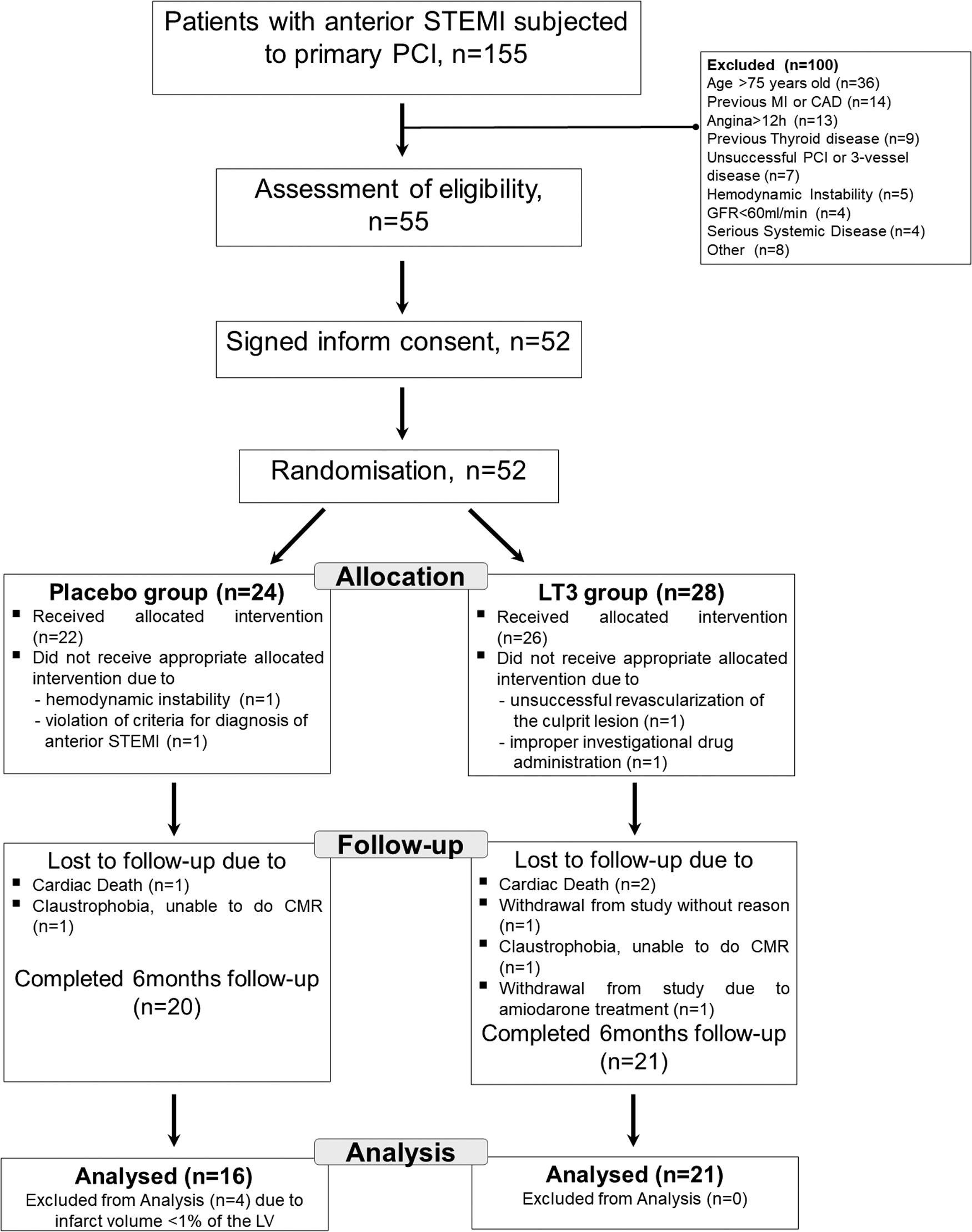
CONSORT flow diagram of the ThyRepair trial. CAD, coronary artery disease; GFR, glomerular filtration rate; MI, myocardial infarction.
Three randomized participants did not complete follow-up at 6 months due to cardiac death (1 in the placebo arm and 2 in the LT3 arm). According to a prespecified analysis plan, four patients with minimal cardiac injury at discharge (defined as CMR infarct size <1% of the LV) were not included in the final analysis. Thus, four patients with CMR scar volumes at discharge (0.6%, 0.84%, 0.2%, and 0.43% of the LV) were excluded. Patients with myocardial infarction are a heterogeneous population and minimal cardiac injury can occur due to early intervention, collateral flow, and pre-infarction angina resulting in a preconditioning-like cardioprotective effect.
The aim of the present study was to investigate treatment efficacy in patients with large infarctions that lead to cardiac remodeling and dysfunction. The inclusion of patients with minimal infarctions introduces significant variation and masks treatment efficacy.
A total of 37 patients were included in the final per-protocol efficacy analysis (16 for the placebo group and 21 for the LT3 group). The database of the final analysis included 71% of randomized patients. In this group of patients, the scar area was between 11% and 42% of the left ventricle as assessed by CMR. A CONSORT flow diagram of the ThyRepair trial is shown in Figure 2.
Baseline characteristics
Baseline characteristics were balanced between groups (Table 1). The mean age of participants was 57.5 ± 7.4 for placebo and 53.7 ± 10.1 years for LT3 group and 87% and 95% were men, respectively. There was no statistically significant difference in standard medication treatment between the two groups (Table 3 in Section B of Supplementary Material).
Study Population Characteristics
Values are expressed as mean ± SD.
LAD, left anterior descending artery; LT3, liothyronine; PCI, percutaneous coronary intervention; SD, standard deviation; TIMI, thrombolysis in myocardial infarction.
The area at risk was 39.4 ± 8.5% and 37.5 ± 7.1% in placebo and LT3-treated groups, respectively, p = 0.49. Peak levels of troponin and the AUC were 173279 ± 87229 and 283180 ± 112185, respectively, in placebo group compared with 162656 ± 96592 and 260293 ± 141599 in LT3 group, p = 0.73 and p = 0.6 respectively.
Echocardiography LV ejection fraction at 48 hours was 43 ± 5.7% for LT3-treated group versus 41 ± 8.2% for placebo, p = 0.4. LV end-diastolic and LV end-systolic diameter was 49.7 ± 3.3 mm and 35.7 ± 4.9 mm for LT3-treated group versus 50.4 ± 5.5 and 36.4 ± 5.7 for placebo, p = 0.65 and p = 0.69 respectively.
Circulating TH levels
Total T3 was significantly increased in the LT3 group compared with placebo at 24, 48, and 72 hours (5.8 ± 1.5 ng/mL, 4.9 ± 1.6, and 2.7 ± 1.8 for LT3 group vs. 0.8 ± 0.18, 0.74 ± 0.16, and 0.67 ± 0.17 for placebo, p = 10−10, p = 10−8, and p = 0.00008 respectively), while T3 levels on admission and discharge were 1.1 ± 0.42 ng/mL, 0.81 ± 0.19 for LT3 group versus 0.93 ± 0.23 and 0.80 ± 0.16 for placebo, respectively, p = 0.2 and p = 0.47 (Fig. 3).
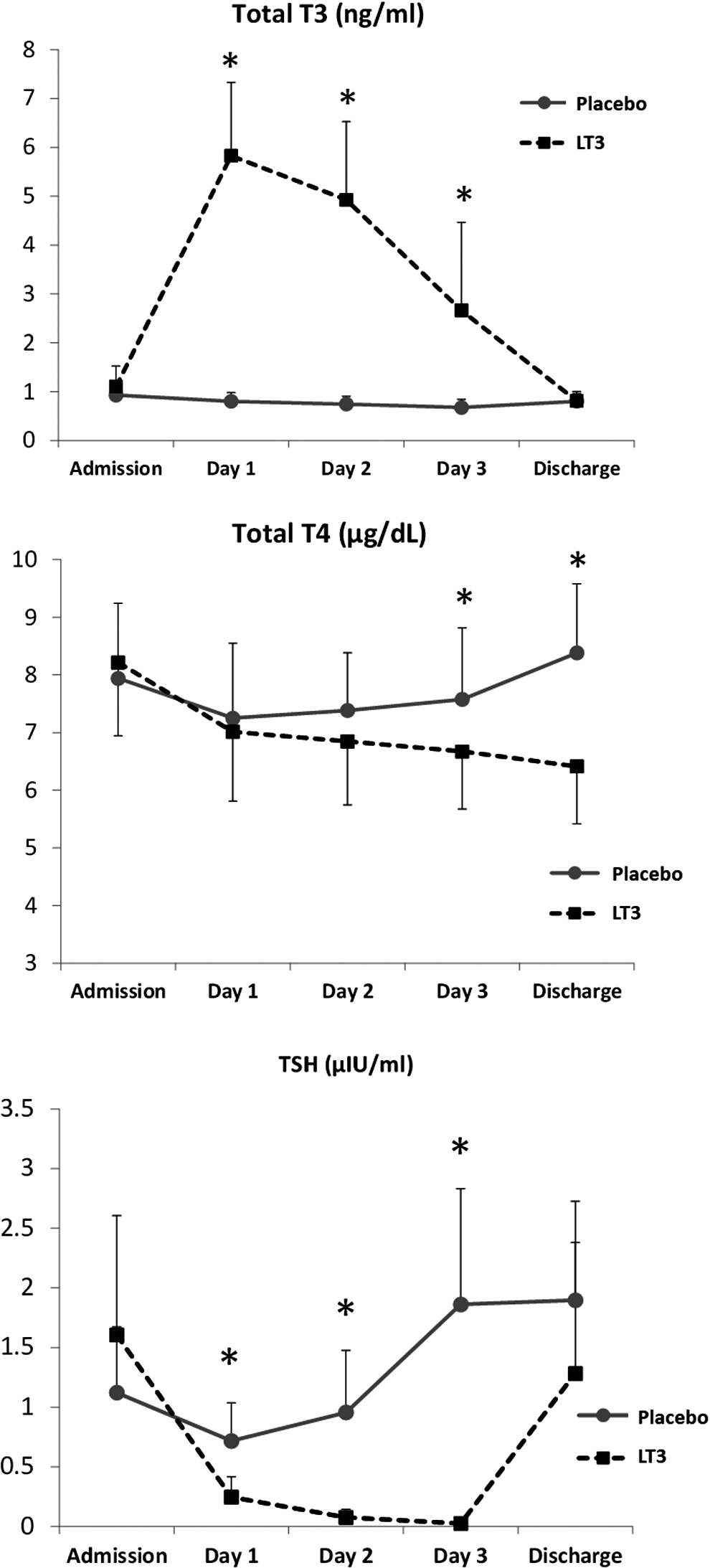
TH profile. Levels of total T3 (upper panel), total T4 (middle panel) and TSH (lower panel) at admission, at 24, 48, and 72 hours, and at discharge in placebo (n = 16) and LT3-treated (n = 21) STEMI patients. *p < 0.05 between the placebo and LT3 groups; all reported p-values are two-sided. LT3, liothyronine; T3, triiodothyronine; TSH, thyrotropin.
Total T4 was similar between the two groups on admission, at 24 and 48 hours but total T4 was lower in the LT3 group as compared with placebo at 72 hours and discharge (p = 0.0023 and p = 0.00008, respectively).
TSH was significantly lower in the LT3 group compared with placebo at 24, 48, and 72 hours (p = 0.002, p = 0.00002, and p = 0.00002, respectively), while TSH levels were similar between the two groups on admission and at discharge (p = 0.1 and p = 0.17, respectively) (Fig. 3). There was no statistically significant difference in total T3, total T4 and TSH between the two groups at 3 and 6 months follow-up (Table 4 in Section B of Supplementary Material).
CMR assessment of LV cardiac function, dilatation, and myocardial injury
CMR LVEF% at discharge and at 6 months follow-up was not statistically different in the LT3-treated group compared with placebo (Table 2).
Cardiac Magnetic Resonance Measurements at Discharge and 6 Months Follow-Up
Values are expressed as mean ± SD. All reported p-values are two-sided. Normal distribution of variables was estimated with Shapiro–Wilk test of normality. Normally distributed data were compared by using an independent t-test. Skewed data (LVEDVi and LVESVi) at 6 months were analyzed non-parametrically by using Mann–Whitney U test.
LVEDVi, left ventricular end-diastolic volume index; LVEF, left ventricular ejection fraction; LVESVi, left ventricular end-systolic volume index; LVMI, left ventricular mass index; MVO, microvascular obstruction; RVEDVi, right ventricular end-diastolic volume index; RVEF, right ventricular ejection fraction; RVESVi, right ventricular end-systolic volume index.
CMR LV end-diastolic volume index (LVEDVi) and end-systolic volume index (LVESVi) at hospital discharge were significantly decreased in the LT3-treated group compared with placebo (Table 2 and Fig. 4). LVEDVi and LVESVi at 6 months follow-up were not different compared with discharge values in either group (p = 0.76 and p = 0.62 for placebo and p = 0.44 and p = 0.3 for LT3 group, respectively) (Table 2 and Fig. 4). IV at discharge was similar between the two groups but tended to be lower in LT3 group compared with placebo at 6 months follow-up (p = 0.05).
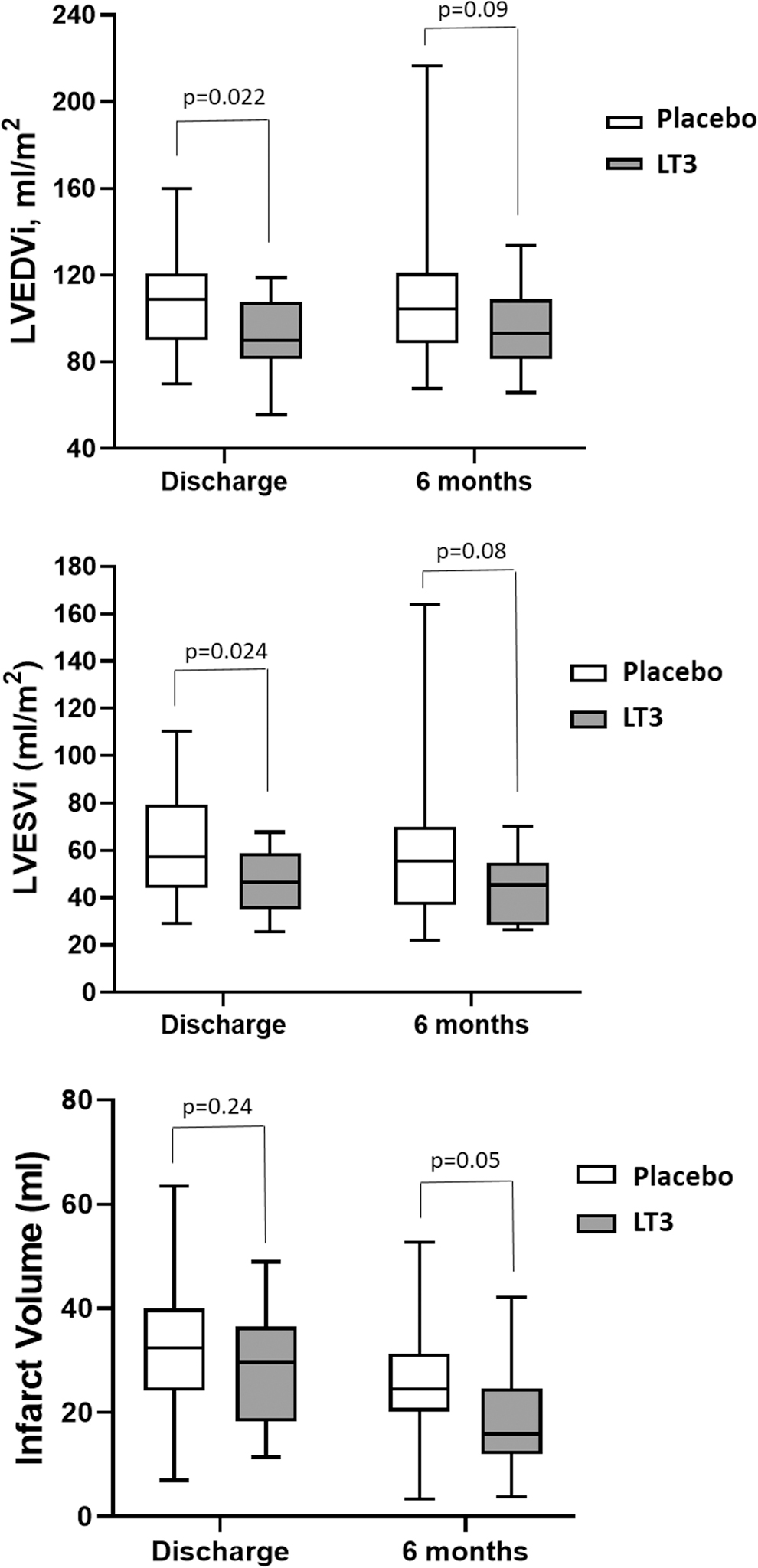
LV volumes and cardiac damage in placebo (n = 16) and LT3-treated (n = 21) STEMI patients. LVEDVi
Further, IV was lower at 6 months follow-up compared with discharge in both groups (p = 0.0001 for placebo and p = 0.00004 for LT3 group) (Table 2 and Fig. 4). There was no statistically significant difference in RV end-diastolic and end-systolic volume indices and RV ejection fraction between the two groups at discharge and 6 months follow-up (Table 2).
The range of functional responses and cardiac injury in LT3 group was found to be narrow in contrast to the placebo group, as indicated by the CIs shown in Table 1 in Section B of Supplementary Material. Interestingly, the range of possible responses of LVESVi at discharge, which indicates the treatment effect on viable myocardium, was limited in LT3 group (CI: 41.6–53.4), as compared with a wide range of possible responses (50.7–71.9) in the placebo group. Further, the range of responses of MVO, which is related to healing, was limited (0.23–0.97) after LT3 treatment as compared with a wide range (0.64–2.56) in placebo group (Table 1 in Section B of Supplementary Material).
A post hoc analysis including the four individuals who were excluded due to minimal IV (in the placebo arm) has been performed (Table 2 in Section B of Supplementary Material). In this analysis, there was no statistically significant difference in the parameters between groups, either at discharge or at 6 months.
Adverse effects
Serious, life-threatening events related to LT3 treatment were not observed. Vital signs (heart rate, blood pressure) and standard biochemical tests were similar between groups (Tables 5–8 in Section B of Supplementary Material). An increase in heart rate was observed in LT3-treated patients only during 72 hours. There was a strong negative correlation between LT3 treatment exposure and heart rate within LT3 group at day 1 (r = −0.64, p = 0.002) and at day 2 (r = −0.53, p = 0.021) after the initiation of treatment.
There was no statistically significant difference in heart rate between the two groups at discharge, 3 and 6 months. Electrocardiogram (ECG) corrected QT interval duration at day 1–3 and discharge was similar between the two groups (Table 8 in Section B of Supplementary Material). The duration of the QRS complex in ECG was significantly lower in the LT3 treatment group at 6 months follow-up (89.8 ± 15 mseconds vs. 103.9 ± 24.1 in placebo, p = 0.04). The incidence of atrial and ventricular arrhythmias during the first 72 hours is shown in Table 9 in Section B of Supplementary Material.
Serious ventricular arrhythmias (sustained ventricular tachycardia or ventricular fibrillation) were not observed during hospitalization in both groups. A trend for an increased incidence of AF was observed in LT3 group during the first 48 hours (19% for T3 group vs. 5% for placebo, p = 0.13). However, LT3 treatment exposure was 432 ± 192 versus 491 ± 130, in patients with and without AF, respectively, p = 0.42. All cases of AF in the LT3-treated group resolved either spontaneously with beta-blocker treatment or with electrical cardioversion.
There was no statistically significant difference in the incidence of LV thrombus formation, minor hemorrhage, and pericarditis between the two groups. Transient episodes of increased temperature (>37.8°C) were recorded during hospitalization in 30% of patients in LT3 group due to the hypermetabolic effect of T3 and resolved with paracetamol administration. No death was recorded during treatment exposure and at hospital stay. During follow-up, two cardiac deaths occurred in LT3 group. One death was due to reinfarction, and one death was due to rupture of the LV wall. In the placebo group, one sudden arrhythmic death occurred. A detailed analysis of adverse events and deaths is included in Section B of Supplementary Material.
Discussion
Several observational studies demonstrate that low T3 is an independent risk marker for poor outcomes in cardiac disease, and TH therapy has been shown to improve recovery of cardiac function in experimental models of myocardial infarction (14). However, the use of T3 therapy in the clinical setting of AMI has been deliberated for many years. In this context, long-term, low-dose T3 or T4 to restore TH levels to normal values were used in two recent studies as potential beneficial treatments in patients with myocardial infarction. These studies concluded no or small effect of TH treatment (T3 or T4) on the recovery of cardiac function and injury (21,22).
The dose and timing of TH administration is likely to have played a role in this response. On ischemic stress, the conversion of T4 to T3 is impaired and inactivation of T3 is increased due to changes in deiodinase activity. Further, changes at the level of TH receptors occur and alter the response of the myocardium to THs (14). Thus, the myocardium seems to be resistant to TH treatment and higher doses of T3 may be required to restore myocardial tissue hypothyroidism. The timing of TH administration is also critical.
Cardiac remodeling is a process that starts after reperfusion, and an early therapeutic window seems to exist for interventions to demonstrate potential effects on post-ischemic cardiac dysfunction and damage (28). In fact, early administration of high-dose T3 in bypass surgery improved recovery of function after blood flow restoration (20). Along this line, early administration and higher doses of T3 improved LV ejection fraction after 2 weeks in experimental myocardial infarction (unpublished data shown in Section A of Supplementary Material). Based on this evidence, a therapeutic regime consisting of early administration of high dose LT3 was used in this study and tested for its potential effects in patients with AMI.
There was no statistically significant difference in patients' baseline characteristics and treatment at discharge and 6 months between study groups (Table 1 in Section B of Supplementary Material). Early cardiac function was assessed by echocardiography, and no differences were found between groups. Further, there was no statistically significant difference in the extent of cardiac damage between the groups as assessed enzymatically by sequential troponin measurements.
The effects of acute LT3 treatment on cardiac function, remodeling, and extent of injury were assessed by CMR at hospital discharge and at 6 months follow-up. The CMR LVEF%, which was the primary endpoint of the present study, was higher in the LT3-treated group as compared with placebo but this difference did not reach statistical significance. It is likely that, at this stage, the greater dilatation of the left ventricle that was observed in untreated patients could contribute to preserved LVEF% via Starling's Law effect (3).
This may mask the effect of LT3 on LVEF% (14,29,30) early after AMI. However, left ventricle decompensates at later stages and differences in LVEF% between groups may be augmented. In fact, the incidence of heart failure after AMI is 13% at 30 days and 20–30% at 1 year (31). This issue merits further investigation in future studies (see Section C of Supplementary Material).
The difference in LVEF% between groups that was detected at 6 months follow-up in the present study was at the magnitude of 5 U, which is of clinical importance since LVEF% change more than 5 U can powerfully predict both survival and heart failure hospitalizations (24). It seems that a larger sample size was needed to designate a significant change in LVEF% at this stage.
In fact, based on a difference of 5 U in favor of LT3 group and a CMR LVEF% of 48.6 ± 11 at 6 months in placebo group (resulting in a medium effect size, d = 0.5), the study needed at least 172 subjects (86 per group) to be included to reach a statistical power of 90% and a probability of a type I error of 0.05 using a two-sided test. However, the present study was designed to designate a large effect size in LVEF%.
The LT3 treatment appeared to have some acute positive effect on early LV chamber remodeling. Both LVEDVi and LVESVi at discharge were significantly reduced in LT3 group as compared with placebo, but the difference between groups was not statistically significant at 6 months (Table 2). The observed initial difference was not due to changes in the extent of cardiac damage since no difference in IV at discharge was observed between groups.
It is more likely to be a direct effect of LT3 on the viable myocardium, as this has been demonstrated in experimental studies (14,29,30). CMR LVEDVi and LVESVi between hospital discharge and 6 months were not different in either group. These findings may be of clinical importance. Early LV dilatation detected by CMR was shown to carry 57% long-term mortality versus 27% and 26% of late and no dilatation, respectively (3). Further, early dilatation was an exclusive independent predictor of long-term mortality after adjustment for age and ejection fraction (3).
CMR IV at hospital discharge was not significantly different in LT3-treated patients as compared with placebo, indicating that acute, high-dose LT3 did not worsen myocardial injury. Interestingly, LT3 administration resulted in a trend in reduction in IV at 6 months follow-up (p = 0.05), suggesting a potential favorable modulatory effect on myocardial injury and healing. This finding was not observed when four patients from the placebo arm who had small IV were included in a post hoc secondary analysis.
T3 may limit cell injury via suppression of the pro-apoptotic p38 MAPK signaling pathway (17) and reduce infarct size in experimental models of myocardial infarction (32,33). This finding may be clinically important. Infarct size, measured by CMR or technetium-99m sestamibi SPECT within 1 month after primary PCI, is strongly associated with all-cause mortality and hospitalization for heart failure within 1 year (34).
Life-threatening events related to LT3 treatment were not observed in this study. Early AF was evident in both groups, with a trend toward a higher incidence in LT3-treated patients. The AF in patients with AMI may occur at an early stage (early AF) in 6.4% and at later stages (late AF) in 7.7% of patients. Early AF is more benign while late AF is associated with adverse effects and death (35). In the present study, the episodes of AF occurred early and were reversible without an impact on cardiac function and hemodynamic stability.
Whether LT3 treatment can increase the incidence of early AF in this clinical setting cannot be addressed in this study due to the small number of patients and merits further investigation in larger trials. However, there was not a statistically significant correlation between T3 treatment exposure and the incidence of AF in LT3-treated patients.
Another interesting observation was that the ECG QRS duration was significantly lower in the LT3-treated group at 6 months follow-up as compared with placebo. This finding is of clinical significance since prolonged duration of QRS complex after AMI is correlated with increased mortality (36). A modest increase in heart rate was observed in LT3-treated patients during 72 hours without detrimental effects on cardiac function and injury.
In the setting of myocardial infarction, increased heart rate is a compensatory mechanism to cardiac dysfunction in order for cardiac output to be preserved. Thus, the effect of LT3 on cardiac function and the compensatory response could partly offset the direct effect of T3 on heart rate. This may explain the negative correlation between heart rate and LT3 treatment exposure that was observed in this study.
The present study is the first pilot, randomized, double-blind, placebo-controlled trial to investigate the potential effects of acute, high-dose LT3 treatment in the setting of AMI. Novel effects of LT3 on injured myocardium were observed, which are in accordance with experimental evidence. However, this study included a small number of patients and 29% (15/52) of the randomized patients were not included in the final analysis (per the pre-specified analysis plan). Despite these limitations, the present study also provides valuable information regarding the study feasibility, safety, and range of treatment responses, allowing an appropriate design of a large-scale, randomized, double-blind, placebo-controlled trial. For details, see Section C of Supplementary Material.
In conclusion, in this pilot trial, acute LT3 administration in AMI appeared to be promising in improving LVEF% at 6 months (primary endpoint) as compared with placebo; however, this difference did not reach statistical significance due to the small number of patients included. This effect was associated with significant improvement in acute cardiac dilatation at hospital discharge and a trend in improvement of 6-month IV (also subject to limited data). This preliminary evidence demonstrates the need for a large-scale, randomized, controlled trial of LT3 administration in AMI. Such a trial may be informed by the observations, challenges in processes, and safety data from this pilot study.
Footnotes
Acknowledgments
The authors acknowledge the great contribution of Alexander S. Onassis Foundation to the Department of Pharmacology research infrastructure.
Authors' Contributions
C.I.P.: conceptualization, formal analysis, funding acquisition, project administration, supervision, writing original draft, and review article. A.G.T.: data curation, investigation, supervision, methodology, and review article. E.G.P.: data curation, investigation, supervision, methodology, and review article. K.P.G.: data curation, investigation, methodology, and review article. P.N.S.: investigation, methodology, and review article. A.K.D.: investigation, methodology, and review article. S.I.L.: data curation, methodology, and review article. N.A.A.: data curation, methodology, and review article. C.G.E.: investigation, methodology, and review article. G.D.G.: investigation, methodology, and review article. N.G.P. investigation, methodology, and review article. N.D.P: investigation, methodology, and review article. A.D.-T.G.: investigation, methodology, and review article. I.S.M.: conceptualization, formal analysis, validation, supervision, writing original draft, and review article.
Author Disclosure Statement
The following patent is relevant to the work in this article: PCT/EP2019/087056. L-T3 for use in limiting MVO. C.I.P. and I.S.M. are the inventors and hold royalties in relation to this patent. Other authors have no disclosures to report.
Funding Information
This work was supported by Uni-Pharma Pharmaceutical Laboratories (Athens, Greece). Uni-Pharma had no contribution in the design of the study, in data collection, analysis, and interpretation of the data, and in the preparation, review, or approval of the article.
Supplementary Material
Supplementary Material