
Abstract
Background:
Thyroid cancer incidence has increased over the past decades. Differences in incidence trends have been observed depending on socioeconomic status. Here, we describe trends in the incidence of papillary thyroid cancer (PTC) and follicular thyroid cancer (FTC) in Denmark by level of education and income.
Methods:
All PTC and FTC cases registered in the Danish Cancer Registry from 1995 to 2019 were identified. Individual-level information on education and income was obtained from nationwide registries. We calculated age-standardized incidence rates according to sex, tumor size, education and income, and estimated incidence trends by average annual percentage change (AAPC) and corresponding confidence intervals [CIs] for the periods 1995 to 2004 and 2005 to 2019 by using Poisson regression models.
Results:
We identified 3454 cases of PTC and 972 cases of FTC. From 2005 to 2019 among women, the incidence of PTC increased across all levels of education (AAPCshort education = 12.5% [CI 9.8 to 15.3]; AAPCmedium education = 8.1% [CI 6.4 to 9.9]; AAPClong education = 7.3% [CI 5.4 to 9.2]). The same pattern was seen for income. The incidence of FTC increased in all levels of education (AAPCshort education = 10.5% [CI 5.8 to 15.4]; AAPCmedium education = 4.0% [CI 0.9 to 7.3]; AAPClong education = 4.3% [CI 0.6 to 8.1]), with the same pattern for income. Similar trends were observed among men, in both small (≤2 cm) and large (>2 cm) PTCs and from 1995 to 2004 in both sexes.
Conclusions:
Enhanced detection of thyroid cancer among all levels of education and income cannot be ruled out, and in addition, our results may suggest a true increase in the incidence of differentiated thyroid cancer.
Introduction
Thyroid cancer is the most common endocrine malignancy worldwide (1), with papillary thyroid cancer (PTC) and follicular thyroid cancer (FTC) as the most common histological subtypes (2). The worldwide number of new thyroid cancer cases has increased remarkably during the past three decades, from ∼95,000 cases in 1990 to 250,000 cases in 2017 (3). In Denmark, the overall incidence of thyroid cancer as well as PTC and FTC also increased substantially from 1980 to 2014 (4). In a recent meta-analysis, it was reported that the increase was primarily due to an increasing number of small (<2 cm) papillary carcinomas (5), but the reason for the increase is still not fully understood.
Previous studies have found higher incidence rates of thyroid cancer among individuals with high socioeconomic status (SES) compared with individuals with low SES (6 –12); however, results from studies assessing whether the increasing incidence trends are found in all levels of SES are equivocal. Some studies found the increase to be more pronounced among individuals with high SES compared with low SES (8 –10), whereas other studies reported that the increase in thyroid cancer incidence (6) or in PTC (7) was similar across all levels of SES. To our knowledge, trends in incidence according to SES in FTC have not previously been reported.
The majority of previous studies have been performed in countries where health care access varies depending on, for example, health insurance status. In addition, most studies were based on area-level socioeconomic data (6,7,9,10), and only a few had individual-level data (8,12).
In Denmark, the Danish National Health Service guarantees access to free-of-charge health care for all citizens and the nationwide Danish registries contain individual-level socioeconomic data (13).
The aim of the present study was to assess the temporal trends in PTC and FTC incidence in adults in Denmark during a period of 25 years according to level of education and income. For PTC we also aimed at investigating the trends stratified by tumor size according to SES.
Materials and Methods
Data sources and study population
Danish nationwide health registries hold validated and accurate information on cancer diagnoses, medical history, and socioeconomic parameters with virtually complete population coverage. All Danish citizens are assigned a unique 10-digit civil registration number at birth or migration into Denmark, enabling individual-level linkage of data between registries (14). The Danish Cancer Registry contains information on nearly all primary incident cancers diagnosed in Denmark since 1987 (15). Information includes date of birth, sex, age at diagnosis, and tumor characteristics (topography, morphology, and TNM T-stage).
The study population was defined as all women and men, diagnosed with a histologically verified thyroid cancer (International Classification of Disease [ICD]-10 code: C73) in the Danish Cancer Registry from 1995 to 2019 with papillary or follicular morphology (ICD-O-3 morphology codes: 8050, 8260, 8340–8343, 8350 for PTC and 8290, 8330–8335 for FTC, with 3 as the last digit). Of the 5195 identified cases, we excluded individuals below the age of 30 years at diagnosis (n = 521), as the majority of individuals would reach the age of 30 before they have established their socioeconomic position.
To avoid a possible impact by the cancer diagnosis on SES, information on education and income was obtained one year before the time of diagnosis, which was why patients were excluded if they did not reside in Denmark at this time (n = 75). Patients were also excluded if they had missing information on education (n = 173) to maintain the same study population throughout the analyses.
Education and income were used as parameters of SES. We obtained data on disposable income and the highest achieved educational level from Statistics Denmark (16,17). Educational level was categorized into short (≤7 years for individuals born before 1958 and ≤9 years for individuals born 1958 and after), medium (8–12 years for individuals born before 1958 and 10–12 years for individuals born 1958 and after), and long (≥13 years). We differentiated between individuals born before and from 1958 onward, as the mandatory length of education for children in Denmark increased from seven to nine years in 1958. Years of education was the standard length for that particular education and not the time that the individual used to complete that specific education.
Information on disposable income was divided into quintiles based on the distribution of income in the general population for all combinations of calendar year, sex, and age. We categorized income into low (first quintile), medium (second to fourth quintile), and high (fifth quintile). Income was divided into quintiles, as this was the categorization available in Statistics Denmark on the general population. Calendar period was categorized into five 5-year intervals.
Information on tumor size was available from 2005, based on TNM-stage and categorized into small tumors ≤2 cm corresponding to T-stage = T1 and large tumors >2 cm corresponding to T-stage >T1.
Statistical analysis
We estimated age-standardized incidence rates and corresponding confidence intervals [CIs] as the number of new cases per 100,000 person-years. Incidence rates were calculated as the ratio between the number of incident cases and the total risk time for the background population. Person-time at risk was obtained from Statistics Denmark for all combinations of calendar periods, sex, age group, educational level, and income, and risk time was included from age 30 years. Incidence rates were age-standardized according to the WHO 2000 World Standard Population (18) and estimated by calendar periods, educational level, and income, separately for PTC, FTC, and sex.
To evaluate incidence trends over time, we calculated the average annual percentage change (AAPC) and corresponding [CI] by Poisson regression analysis, with log link and with log of the person-time at risk as offset. Incidence time trends were evaluated within the different levels of education and income, and separately for PTC, FTC, sex and for the calendar periods 1995 to 2004 and 2005 to 2019, as our data showed different trends in the incidence of PTC and FTC during these two periods. In cases with PTC, we additionally estimated incidence rates according to tumor size by calendar periods, educational level, and income, separately for each sex.
The corresponding AAPCs were calculated according to tumor size and SES-level, separately for each sex. The TNM-stage was available from 2005, which was why analyses on tumor size were restricted to the period 2005 to 2019. Tumor size analyses were only possible in cases with PTC due to a lower number of FTC cases. We conducted the statistical analyses by using the statistical software R, version 3.6.3, with a statistical significance level of 5% (19).
Results
Over the study period of 25 years, we identified 3454 cases of PTC and 972 cases of FTC in women and men aged 30 years and older in Denmark (Table 1).
Characteristics of the Study Population of Women and Men Diagnosed with Papillary or Follicular Thyroid Cancer in Denmark 1995–2019
Thyroid cancer occurred more often in women (PTC: 72%, FTC: 69%) compared with men, and in patients younger than 60 years (median age in PTC: 51 years, median age in FTC: 59 years). The larger part of both patients with PTC and FTC had a medium level of education (PTC: 46%, FTC: 47%), and a medium level of income (PTC: 62%, FTC: 65%) (Table 1). In patients with PTC diagnosed from 2005 to 2019 (n = 2766), 41% presented with tumors ≤2 cm, 38% with tumors >2 cm, and 21% were registered with an unknown tumor size.
Papillary thyroid cancer
Educational level
The incidence rates of PTC among women and men increased across all educational levels from 1995 to 2019 (Fig. 1A, B and Supplementary Tables S1 and S2). From 2005 to 2019, the incidence rate increased on average by 12.5% [CI 9.8 to 15.3] per year in women with short education, 8.1% [CI 6.4 to 9.9] in women with medium education, and 7.3% [CI 5.4 to 9.2] in women with high education (Table 2). Similar trends were found among men in the period from 2005 to 2019, with AAPCs of 13.6% [CI 9.2 to 18.2] in men with short education, 9.7% [CI 7.0 to 12.4] in men with medium education, and 10.2% [CI 6.8 to 13.7] in men with high education (Table 2).
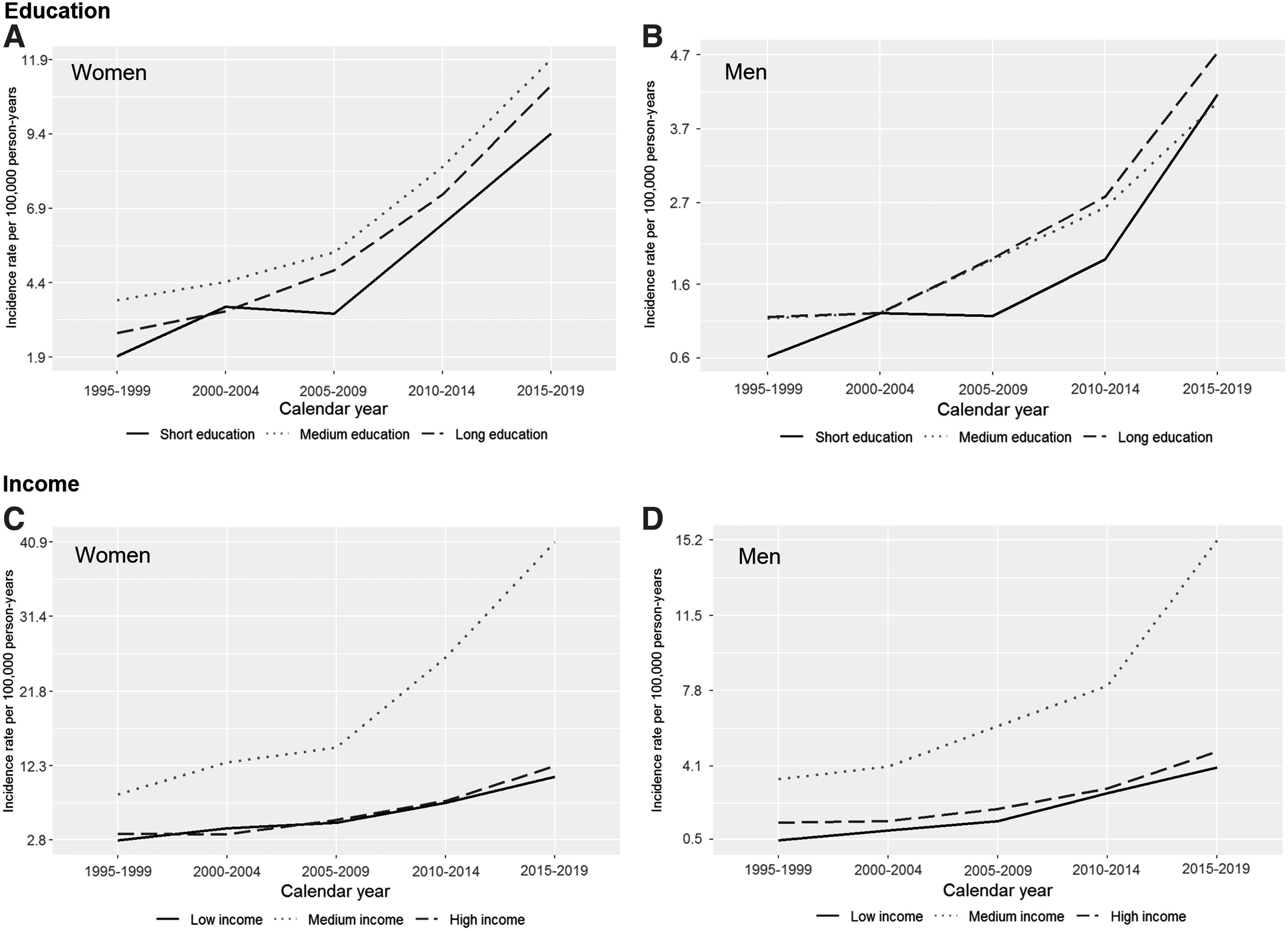
Age-standardized incidence rates of papillary thyroid cancer in Denmark, 1995–2019, according to level of education (upper panel,
Average Annual Percentage Change in Papillary and Follicular Thyroid Cancer Incidence in Denmark, During 1995–2004 and 2005–2019, Stratified by Sex, Educational and Income Level
Bold signifies the histological subtypes.
AAPC, average annual percentage change; [CI], confidence interval.
Income level
Figure 1C and D display the incidence rates of PTC stratified by level of income. From 2005 to 2019, the incidence of PTC increased on average by 7.4% [CI 4.8 to 10.1] per year in women with low income, 10.2% [CI 8.7 to 11.7] in women with medium income, and 9.4% [CI 6.8 to 12.1] in women with high income (Table 2). We found similar results in men, where the incidence of PTC increased on average by 11.6% [CI 7.1 to 16.3] per year in men with low income, 11.8% [CI 9.4 to 14.3] in men with medium income, and 9.7% [CI 5.6 to 13.9] in men with high income (Table 2).
Tumor size
The incidence of small (≤2 cm), large (>2 cm) and PTCs of an unknown size increased in all levels of education from 2005 to 2019 in both women and men (Table 3 and Figs. 2 and 3). In women with short education, the AAPC for small PTCs was: 13.2% [CI 8.9 to 17.6] and 7.9 [CI 3.8 to 12.1] for large PTCs. The corresponding AAPCs for women with medium education were, respectively, 9.6% [CI 7.1 to 12.2] and 2.9 [CI 0.3 to 5.6]. Finally, in women with high education, the AAPC was 6.2% [CI 3.3 to 9.2] for small PTCs and 4.4 [CI 1.4 to 7.5] for large PTCs.
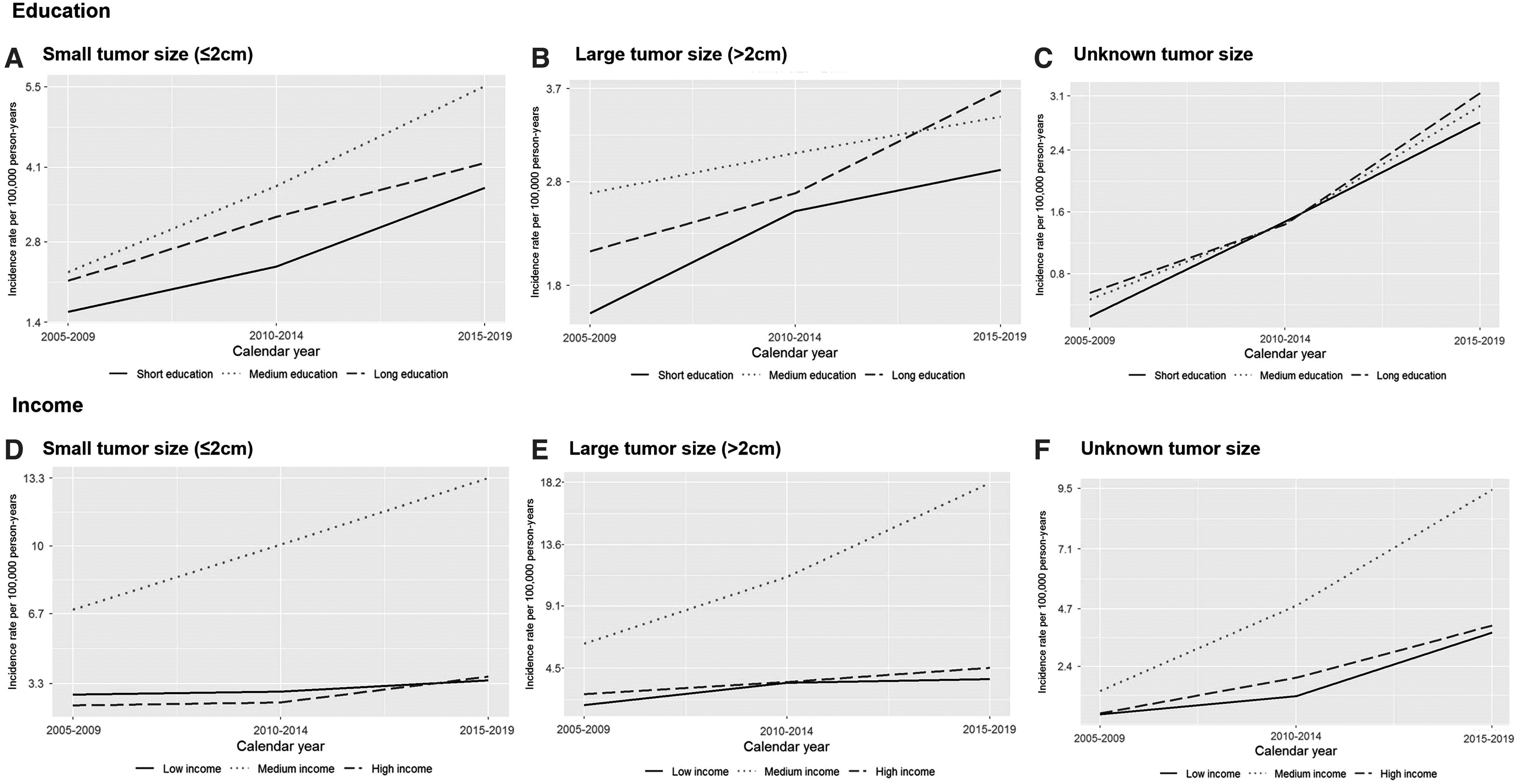
Age-standardized incidence rates of papillary thyroid cancer according to level of education (upper panel), income (lower panel), and tumor size (

Age-standardized incidence rates of papillary thyroid cancer according to level of education (upper panel), income (lower panel), and tumor size (
Average Annual Percentage Change in Papillary Thyroid Cancer Incidence in Denmark, During 2005–2019, Stratified by Sex, Tumor Size, and Educational and Income Level
Similarly, when stratified by income level, the incidence of PTC generally increased among all tumor sizes in all levels of income from 2005 to 2019 in both women and men (Table 3 and Figs. 2 and 3).
Follicular thyroid cancer
Educational level
Figure 4A and B show the incidence rates of FTC in women and men from 1995 to 2019 stratified by educational level. From 2005 to 2019, the incidence increased among women on average by 10.5% [CI 5.8 to 15.4] in women with short education, 4.0% [CI 0.9 to 7.3] in women with medium education, and 4.3% [CI 0.6 to 8.1] in women with high education (Table 2). Similarly, the incidence of FTC increased from 2005 to 2019 among men of all educational levels with an AAPC of 15.5% [CI 7.9 to 23.7] in men with short education, 7.7% [CI 3.0 to 12.6] in men with medium education, and 7.8% [CI 1.8 to 14.1] in men with high education (Table 2). From 1995 to 2004, similar trends in incidence were observed in both sexes, except for the small group of men with short education (n = 12).
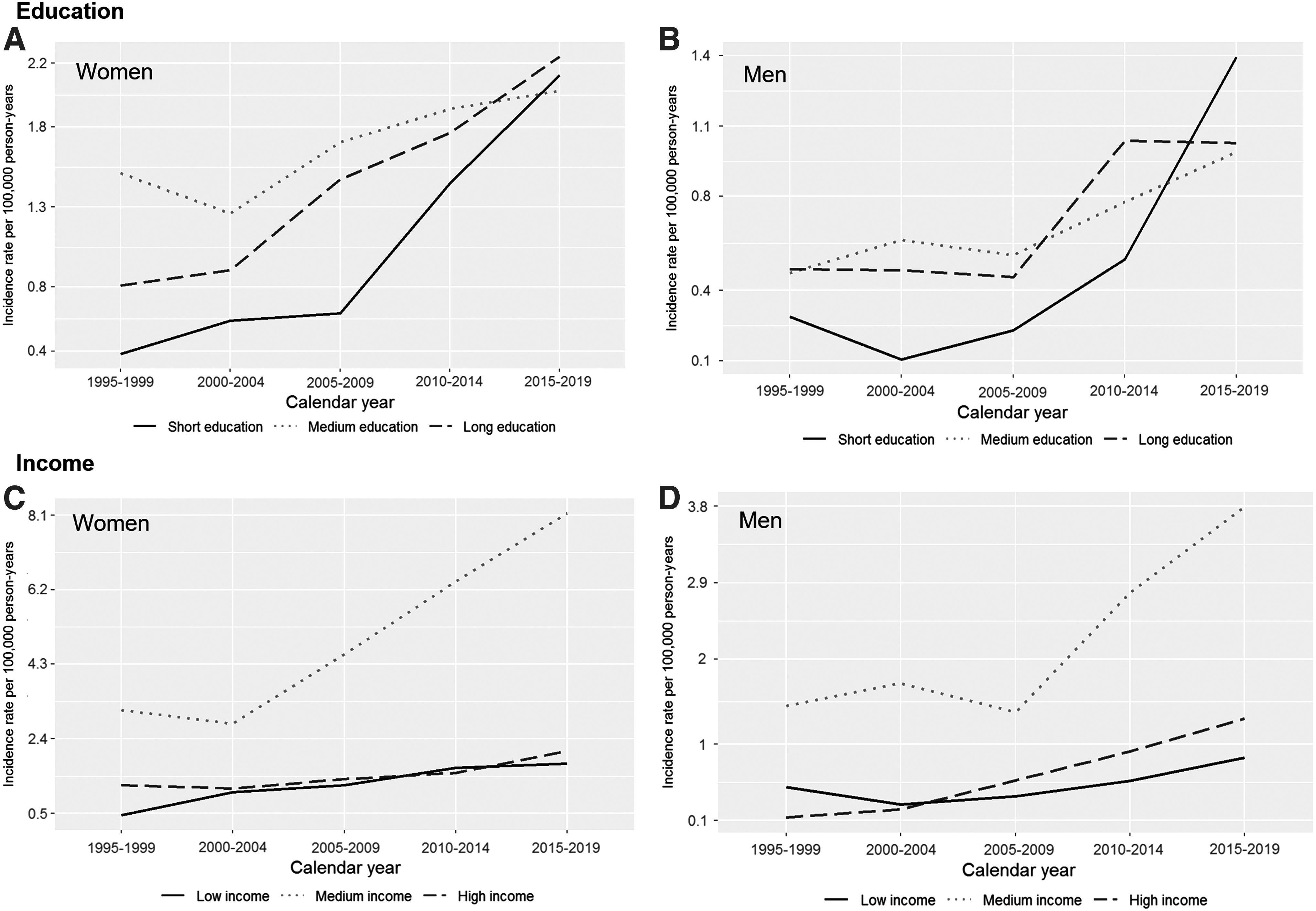
Age-standardized incidence rates of follicular thyroid cancer in Denmark 1995–2019, according to level of education (upper panel,
Income level
When stratified by income level, the incidence of FTC tended to be higher in individuals with a medium level income from 1995 to 2019. We observed an increase over time in all levels of income (Fig. 4C, D and Supplementary Tables S1 and S2). From 2005 to 2019, the incidence rates increased in women with low income (AAPC: 5.9% [CI 0.7 to 11.2]), and medium income (AAPC: 7.2% [CI 4.5 to 10.0]). An increasing tendency was also observed among women with high income (AAPC: 2.5 [CI −2.3 to 7.7]) (Table 2). Similar patterns were observed in men, with increases in FTC incidence found in all levels of income from 2005 to 2019 with an AAPC of 9.2% [CI 0.7 to 18.5] in men with low income, 10.6% [CI 6.3 to 15.1] in men with medium income, and 8.8% [CI 1.9 to 16.2] in men with high income (Table 2).
Discussion
We investigated trends in PTC and FTC incidence in Denmark over nearly three decades (1995 to 2019), and we demonstrated an increasing incidence rate of PTC of all sizes and FTC among women and men in all levels of education and income.
To our knowledge, only one study has previously investigated the temporal trends in PTC incidence according to SES. In line with the present study, Horn-Ross et al. found an increase in the incidence of PTC across all SES levels on comparing the incidence rate in the period from 1988 to 1992 with the period from 1995 to 2002 (7). Similar trends were found in men. The study was based on a neighborhood-level socioeconomic index.
We also found increasing incidence rates of FTC regardless of education and income. To our knowledge, no previous studies have investigated temporal trends in FTC incidence according to SES.
Support for our finding comes from studies examining the different histologic types of thyroid cancer as a combined group. However, most of the studies did not have individual-level information on SES. Pandeya et al. found similar increases in thyroid cancer incidence in Queensland, Australia from 1996 to 2008 across levels of SES (6) by using area-level information on SES. Similarly, in a study based on county-level SES information, Li et al. found an increasing incidence of thyroid cancer from 1980 to 2008 in U.S. counties with both low and high median household income (10).
Finally, Reitzel et al. investigated incidence trends of thyroid cancer in Texas, USA, from 1995 to 2008 with area-level SES information (9). They found an increasing incidence of thyroid cancer in both areas with low and high median household income.
Only two previous studies of trends in thyroid cancer incidence according to SES used individual-level information on SES (8,12). A Canadian study (12) found an increasing incidence in thyroid cancer among all levels of education and family income quintiles when comparing the period from 1991 to 2000 with that from 2001 to 2010. This was also the only study with a similar health care system to Denmark. In contrast, Kang et al. found an increasing thyroid cancer incidence rate in Korea among all household income quintiles from 2006 to 2012 but a declining incidence rate in all household income quintiles in the most recent period (2013 to 2015), particularly in the highest income quintile (8). However, the latter period only covered three years, and no AAPCs were reported. The authors concluded that the observed decrease in thyroid cancer incidence from 2013 was caused by general concerns among physicians about thyroid cancer over-diagnosis.
The observed increase in thyroid cancer incidence over the past decades has primarily been due to an increase in PTC, and it has been reported that this was particularly related to papillary microcarcinomas (size ≤1 cm) (20,21). However, a parallel rise in mortality has not been observed (22 –24). Based on these findings, a commonly proposed explanation for the rising thyroid cancer incidence is the improvements in diagnostic tests, and thereby the diagnosis of subclinical disease that would not otherwise have been detected or led to death (23,25).
As individuals with high SES generally have better health care access and more health-oriented behavior (26), enhanced detection could be an explanation for why some studies have found thyroid cancer incidence to differ between SES levels. Even in Denmark, where citizens have free-of-charge health care and thus presumably equal access to health services and examination, individuals with high SES show higher participation in screening programs and more frequent visits to specialized private practitioners (27).
Some previous studies investigating trends in thyroid cancer incidence by SES and tumor size found an increase in thyroid cancer tumors of all sizes in individuals with both high and low SES (7,10). This is in line with the present study, where we found an increase in both small and large PTCs as well as in FTC, among all levels of education and income. Thus, if enhanced detection is the sole cause of the rising thyroid cancer incidence in Denmark, it appears to occur generally for patients with both PTC and FTC, small and large PTCs, and among all levels of SES.
Our findings could also potentially point toward a true increase in thyroid cancer incidence in Denmark. As obesity is a proposed risk factor for thyroid cancer development (28), the rising rates of thyroid cancer could potentially by attributed to the globally rising incidence of obesity (29). The prevalence of obesity differs according to SES, and it is strongly associated with low SES in high-income countries (30). Another proposed explanation of the increasing incidence is increased exposure to ionizing radiation, a well-documented risk factor of thyroid cancer (20). In the United States, the individual dosage of radiation doubled over a period of 25 years, mainly due to the increased use of medical diagnostic procedures (31).
We generally found increasing incidence rates of both PTC and FTC over the whole study period of 25 years, with the increase being most pronounced in the most recent study period (2005 to 2019). In 2007, a fast-track program was introduced in Denmark for patients with suspected head and neck malignancies. The program included a series of systematized, accelerated consultations with the purpose of determining a potential cancer diagnosis and treatment plan (32). This may have resulted in enhanced detection of thyroid cancer from 2007 and onward, among individuals of all levels of education and income as supported by our findings.
The present study has several strengths. The results were based on data from a nationwide, high-quality register with close to complete coverage. We were able to cover a long study period of 25 years, resulting in a large number of histologically verified thyroid cancer cases. Data on SES were obtained on an individual level, and education and income are considered valid indicators of SES over a life span, as education reflects early life circumstances and resources in young adulthood, while income may be indicative of resources in later adulthood (33,34).
Further, by differentiating between individuals born before and after 1958, we were able to take into account the changing social value of educational level, as older birth cohorts generally have shorter education than younger birth cohorts. Our study also has some limitations. First, a subset of cases (3%) had missing information on education and were excluded from the study population, and 21% of cases with PTC had missing information on tumor size. Second, income typically follows a u-shaped curve with age and may be less reliable as an indicator of SES in young and elderly adults (33).
However, in the present study, all participants were above the age of 30 years, the majority of participants were younger than 60 years, and incidence rates were age-standardized.
In conclusion, our study shows an increase in the incidence of PTC and FTC from 1995 to 2019 as well as of small and large PTCs from 2005 to 2019 in Denmark across all levels of education and income. Several studies have suggested that enhanced detection may be the primary cause of the increasing rates of thyroid cancer, based on the observation that in some studies the incidence of thyroid cancer, and especially papillary micro-carcinomas, has increased more in individuals with high SES than in individuals with low SES (8,9,11).
The Danish health care system provides free-of-charge health services, which may complicate a comparison with studies of thyroid cancer incidence trends conducted in populations where access to health care may vary. Enhanced detection of thyroid cancer within the population and regardless of socioeconomic level and tumor size cannot be ruled out, but our results could also suggest that a true increase in PTC and FTC incidence exists.
Footnotes
Authors' Contributions
All people who meet the authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. Further, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in THYROID.
Acknowledgments
The authors would like to thank Tatiana Hansen for valuable assistance with data extraction and management.
Ethical Approval and Data Availability
The study was approved by Statistics Denmark's Scientific Board (Project No. 708043) and registered internally at the Danish Cancer Society Research Center (Project No. 2020-DCRC-0037). Ethical approval is not required for retrospective registry-based studies, according to Danish law (![]() ). All data were stored on a secure platform at Statistics Denmark, which can be accessed given obtainment of the relevant permissions.
). All data were stored on a secure platform at Statistics Denmark, which can be accessed given obtainment of the relevant permissions.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2