
Abstract
Background:
Low levels of the active thyroid hormone triiodothyronine (T3) in cardiac patients are associated with worse outcomes. The aim of this analysis was to assess if T3 treatment is beneficial and safe in patients undergoing cardiac surgery or those with cardiovascular diseases in whom there is observed or expected reduction in serum T3 levels.
Methods:
A systematic review and meta-analysis of randomized controlled trials (RCTs) was performed as per the PRISMA guidelines. Pubmed, EMBASE, and Web of Science databases were searched for RCTs published between January 1, 1960 and March 30, 2022 that evaluated the effects of T3 therapy in patients undergoing cardiac surgery or with cardiovascular diseases. The primary outcomes were measures of cardiac function. Weighted mean difference (MD) or relative risk was calculated using a random effects model. PROSPERO registration number CRD42020211966.
Results:
Of the 3181 full-text articles screened, 34 studies with 2547 participants (number ranging between 13 and 223, mean ages between 0.5 and 73 years, mean percentage of women between 7% and 64%) were included. In 12 RCTs with 1093 adults undergoing cardiac surgery T3 therapy was associated with improvement in cardiac index (MD [95% confidence interval], 0.24 [0.08 to 0.40] L/min/m2, I 2 = 74%). The quality of evidence was high to moderate. In 3 RCTs with 188 children undergoing cardiac surgery, 3 RCTs with 131 adult cardiac donors, 3 RCTs with 83 adult patients with heart failure, and 2 RCTs with 89 adults with acute myocardial infarction, T3 therapy did not improve cardiac index or left ventricular function; the quality of evidence ranged from high (pediatric cardiac surgery) to low (other groups). No detrimental effect of T3 therapy was observed on heart rate, risk of in-hospital atrial fibrillation, or mortality.
Conclusions:
Short-term T3 therapy is safe and trials in adults undergoing cardiac surgical procedures to evaluate longer term clinical endpoints are required. Current data do not support the routine use of T3 therapy in children undergoing cardiac surgery or in cardiac donors. Adequately designed trials are required to determine if T3 therapy improves cardiac function and clinical outcomes in patients with heart failure or acute myocardial infarction.
Introduction
The cardiovascular system in general and the myocardium in particular is a major target of thyroid hormone action (1). The active thyroid hormone triiodothyronine (T3) has a strong influence on several structural and regulatory proteins of the cardiac myocyte and is important for myocardial contractility, acts as a vasodilator and has a direct positive action on myocardial mitochondrial function (2). Furthermore, myocardial injury, caused by either disease or surgical intervention, leads to reduced intra- and extracellular T3 levels owing to the effects on thyroid hormone-modulating enzymes (3). Epidemiological studies have consistently demonstrated that low serum T3 levels are a strong prognostic marker of higher mortality in patients with cardiac disease or those undergoing cardiac surgical procedures (4,5).
Trials of T3 in a small number of patients either undergoing cardiac surgery or with cardiovascular disease have shown conflicting results (6). This uncertainty regarding the utility and safety of T3 in high-risk patients has led to variations in clinical practice, which is best observed by its use in cardiac donor procedures. Some cardiac centers in the United States routinely use T3 and/or thyroxine (T4) in brain dead cardiac donors before organ retrieval, although this practice is not universally shared (7), despite a meta-analysis of randomized controlled trials (RCTs) showing no benefit (8). Similarly, experience from routine clinical practice has suggested that therapy with T3 may be useful in weaning patients from cardiopulmonary bypass who are on maximal inotropic support (9). Previous systematic reviews have evaluated the use of thyroid hormones in specific patient groups such as organ donors, postoperative nonthyroidal illness in adults or children after surgery for congenital heart defects (8,10,11). However, systematically synthesizing and analyzing the literature pertaining to T3 supplementation in the various cardiac conditions including cardiovascular diseases could clarify its role and guide clinical practice.
We performed a systematic review and meta-analysis of RCTs with the primary aim to identify the effects of T3 therapy or control on cardiac function in patients undergoing cardiac surgery or with cardiovascular disease. Our secondary aims were to investigate the impact of T3 treatment on hospital length of stay (LOS), postoperative inotrope use, thyroid function parameters, and to assess any adverse effects. The results of this analysis could provide clinicians with evidence to guide clinical practice regarding the potential efficacy and safety of T3 treatment in patients with cardiac conditions.
Materials and Methods
This systematic review was conducted as per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for evidence-based reporting of randomized trials. The protocol was published on PROSPERO (CRD42020211966), available at
Data sources and search strategy
We searched three electronic databases (PubMed, EMBASE, and Web-of-Science) for articles written in English from 1960 to March 30, 2022, with the help of expert librarians. The searches were a combined result of the terms thyroid hormone (T3, triiodothyronine, liothyronine) and cardiovascular disease (cardiovascular, heart, cardiac, cardiology, heart failure, congestive heart failure, cardiac arrest, MI, myocardial infarction, coronary heart bypass, coronary artery bypass graft, heart bypass, valvular, pediatric cardiac surgery, and adult cardiac surgery). References of the full-text articles identified by the search were reviewed to identify any additional studies that could be eligible for inclusion. In addition, global database of clinical trials was also interrogated (
Study selection and data extraction
RCTs that evaluated the effects of T3 therapy in patients with cardiac disorders were eligible to be included in the systematic review. Low serum T3 levels at recruitment were not criteria for inclusion in the cardiac surgical studies as T3 levels are known to decrease in these patients (3). Two independent reviewers (M.T. and S.R.) reviewed the titles and abstracts of each citation and differences were resolved through discussion. A semi-automated app was utilized for the initial screening of titles and abstracts identified from the various sources to expedite the initial screening of titles and abstracts and to help identify duplicates (12). Duplicates between each database were then individually removed and the full texts of relevant articles were independently reviewed. Studies that reported any cardiac procedures including cardiopulmonary bypass grafting, valvular surgery, or repair of heart defects were classed as cardiac surgeries. And, studies that included patients with cardiac conditions such as heart failure, ischemic heart disease, or acute myocardial infarction were classed as cardiovascular diseases. For studies that utilized more than one dose of T3, the results for the highest dose were included. If studies reported results for an outcome at multiple time points during or after the intervention, only the latest measurement was used in the statistical analyses. Using a predesigned data collection format, one of the authors (M.T.) gathered information from the studies and a second author (S.R.) checked the information for accuracy (Supplementary Methods section in the Supplementary Data).
Quality assessment
Risk of bias assessment tool version 2 (ROB2) was utilized to assess for potential bias for each RCT (13). The Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to evaluate the quality of evidence for each outcome being evaluated based on five domains including risk of bias, inconsistency, indirectness, imprecision, and publication bias. The quality of evidence was then summarized to range from high, moderate, low to very low (14).
Data synthesis and analysis
The main outcome for assessment was measures of cardiac function. Other secondary outcomes included parameters of safety of T3, resource utilization, and thyroid function parameters. For continuous variables, mean difference in changes for each treatment arm (T3 or placebo) and its standard deviation were calculated for each trial. Weighted mean differences (MD) and their 95% confidence intervals (CIs) using the random effects model of Hartung–Knapp–Sidik–Jonkman method, which is considered more robust than the commonly reported DerSimonian–Laird method when the number of included studies is <20, were calculated (15). For binary outcomes, pooled risk ratios (RRs) and their CIs using random effects model were estimated. For outcomes that were measured differently across trials (such as reporting the measured thyroid hormone as either the total or the free fraction, measure of systemic vascular resistance as the direct value or its derived index, or infarct size as either the late gadolinium enhancement extent as percentage of mass or the absolute volume), standardized mean differences (SMD) were calculated (Supplementary Methods section in the Supplementary Data). Studies that reported zero events in both the arms were included and 0.5 events were added to both arms (16). Heterogeneity was assessed by the I 2 method and tau (τ2) (17). I 2 levels between 0% and 40%, 41% and 60%, and >60% were classed as being indicative of low, moderate, and substantial heterogeneity, respectively (18). To assess the underlying causes of the observed variation and to test the robustness of our findings, meta-regression of outcomes that included 10 or more studies was performed. The influence of mean daily dose of T3, route of T3 administration (intravenous [IV] or oral), duration of T3 therapy, and baseline left ventricular ejection fraction (LVEF < or >40%) was analyzed in the meta-regression. In addition, prediction intervals were calculated for outcomes that included 10 or more studies to help in the clinical interpretation of the heterogeneity by estimating the range of true effects to be expected in future settings (19). Contour enhanced funnel plots were utilized to assess for evidence of publication bias and small study effects (20). Various sensitivity analyses were performed post hoc for outcomes that included 10 or more studies. Further details of statistical techniques are provided in Supplementary Methods section in the Supplementary Data. The statistical package R (meta, metasens, metareg) was used for all analyses.
Results
The PRISMA checklist is provided in Supplementary Results section in the Supplementary Data.
Literature search
The systematic literature search retrieved 3900 studies from databases, 127 studies from trial registry, and an additional three articles from the full-text studies reviewed (Fig. 1). From the studies identified from databases, duplicates (n = 721) were removed, and, subsequently, 2 reviewers (M.T. and A.T.) independently screened 3182 unique articles for potential eligibility based on title and abstract. Among these, 3129 studies did not meet the inclusion criteria. None of the studies identified from the trial registry were eligible for inclusion. Of the remaining 53 studies, 19 articles did not meet the study criteria and were therefore excluded (eTable 1 in the Supplementary Data). To obtain additional data an attempt was made to contact authors of eligible studies; five authors indicated that data were no longer available, three authors did not respond, and one refused to share data.
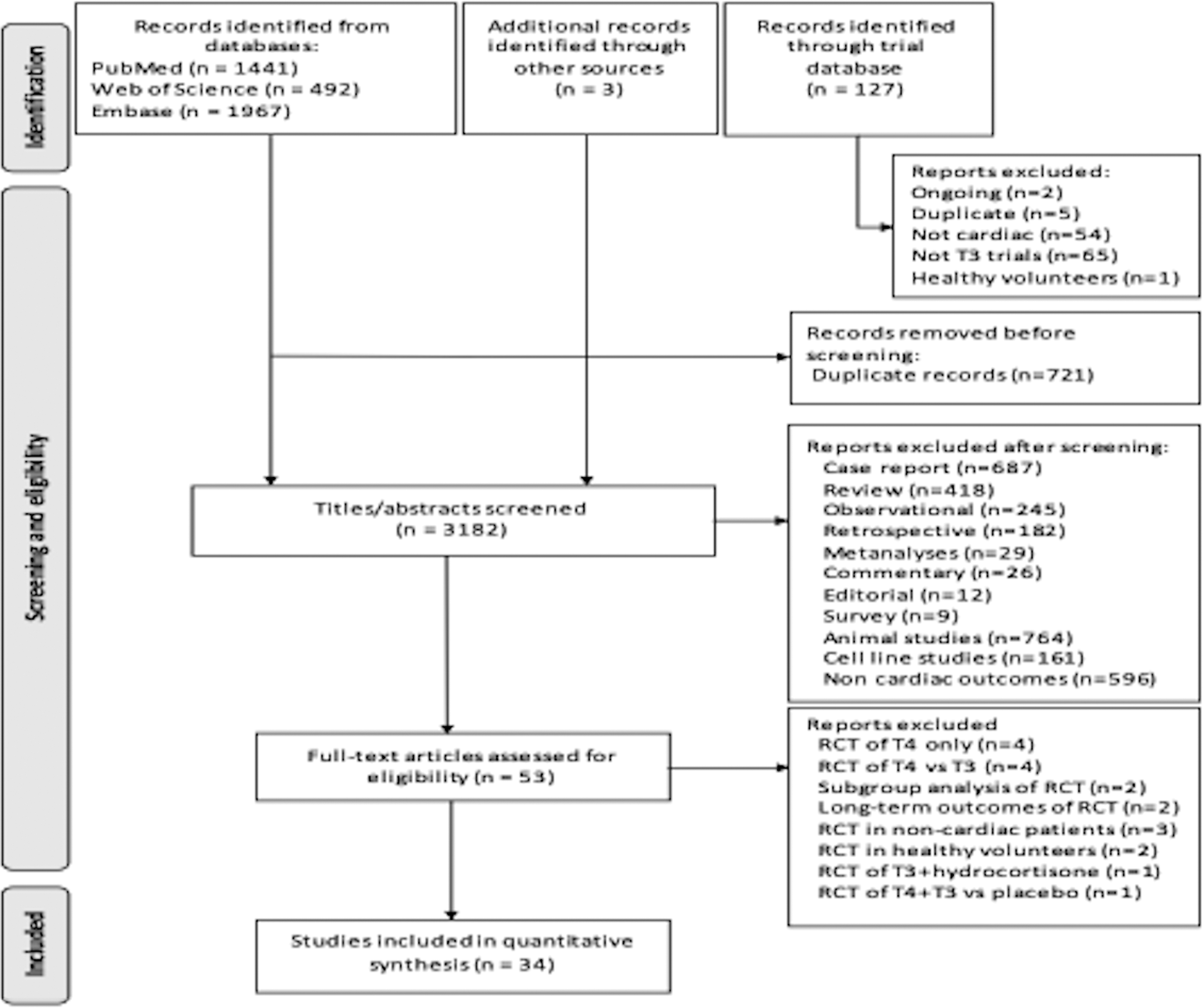
PRISMA flow diagram for systematic review of databases, trial registry, and other sources.
Details of Randomized Controlled Trials of Triiodothyronine Therapy in Cardiac Conditions
Assuming 70 kg body weight.
Number of participants in the analyses may differ than stated in the article or this table as this study compared varying doses of T3 and the group receiving the highest dose was utilized for analyses.
Assuming 10 kg body weight.
CABG, coronary artery bypass grafting; HF, heart failure; hsCRP, high sensitivity C reactive protein; ICU, intensive care unit; IV, intravenous; LOS, length of stay; LVEF, left ventricular ejection fraction; ns, not stated; NT-proBNP, N-terminal pro-brain natriuretic peptide; NYHA, New York Heart Association; P, placebo; STEMI, ST-elevation myocardial infarction; T3, triiodothyronine; TISS, therapeutic intervention scoring system; TTE, time to extubation; 6MWD, 6 minute walking distance test.
Thirty-four studies with 2547 participants met the inclusion criteria (10,11,21 –52) (Table 1). Study sizes ranged from 13 to 223 participants; mean ages ranged from 0.1 to 73 years; percentages of women ranged from 7% to 64%; and the mean daily dose of administered T3 ranged from 4 to 246 μg, administered as a single dose, repeated boluses, or continuous infusion.
Quality of evidence
Overall, the quality of evidence ranged from high for outcomes such as risk of atrial fibrillation (AF) and LOS in cardiac surgery to very low in the two studies evaluating the effects of T3 on LVEF in patients with acute myocardial infarction (Table 2).
Summary of Findings of Triiodothyronine Treatment in Various Cardiac Conditions
ROB was assessed based on seven domains (random sequence generation, allocation concealment, blinding of participants and study personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias). Inconsistency was assessed by degree of heterogeneity or if point estimates and CIs varied considerably. Indirectness was assessed based on variations in populations, intervention, comparator, or outcomes. Imprecision was based on number of participants and/or events included. Publication bias was assessed by visual inspection and also quantitatively analyzing funnel plots. GRADE is a transparent framework for developing and presenting summaries of evidence and provides a systematic approach for making clinical practice recommendations. GRADE has four levels of evidence: Very low (◯◯◯◯ or ⨁◯◯◯)—the true effect is probably markedly different from the estimated effect. Low (⨁⨁◯◯)—The true effect might be markedly different from the estimated effect. Moderate (⨁⨁⨁◯)—The authors believe that the true effect is probably close to the estimated effect. High (⨁⨁⨁⨁)—The authors have a lot of confidence that the true effect is similar to the estimated effect. Evidence from randomized controlled trials starts at high quality. The certainty in the evidence may be decreased for several reasons such as ROB, imprecision, inconsistency, indirectness, and publication bias; authors have the option of decreasing their level of certainty one or two levels (e.g., from high to moderate).
Serious inconsistency (high I 2 value with some trials not overlapping with each other).
Some concern for ROB (owing to no prespecified analysis plan and selection of the outcome) and serious concern regarding small sample sizes in the trials.
Serious concern regarding imprecision owing to very small number of participants in each trial.
Serious ROB and only one trial with small number, no details of blinding or prespecified analysis plan.
AF, atrial fibrillation; CI, confidence interval; GRADE, Grading of Recommendations Assessment, Development and Evaluation; MD, weighted mean difference; ROB, risk of bias; RR, risk ratio; SMD, standardized mean difference; SVT, supraventricular tachycardia.
T3 in cardiac surgery
T3 treatment in adult cardiac surgery
Cardiac index
In 12 studies including 1093 adults undergoing cardiac surgery, T3 therapy was associated with increased cardiac index (MD of 0.24 L/min/m2; CI, 0.08–0.40, I 2 = 74%) (Fig. 2) (21,23 –33). Prediction interval ranged from −0.29 to 0.77 L/min/m2. Meta-regression demonstrated that duration of treatment with T3 (ranging from 6 hours to a few days postoperatively) was positively associated with increased cardiac index (p = 0.04), whereas the mean daily dose of T3 (p = 0.11), route of administration (IV or oral; p = 0.10), or baseline LVEF (< or >40%; p = 0.69) were not significant predictors.
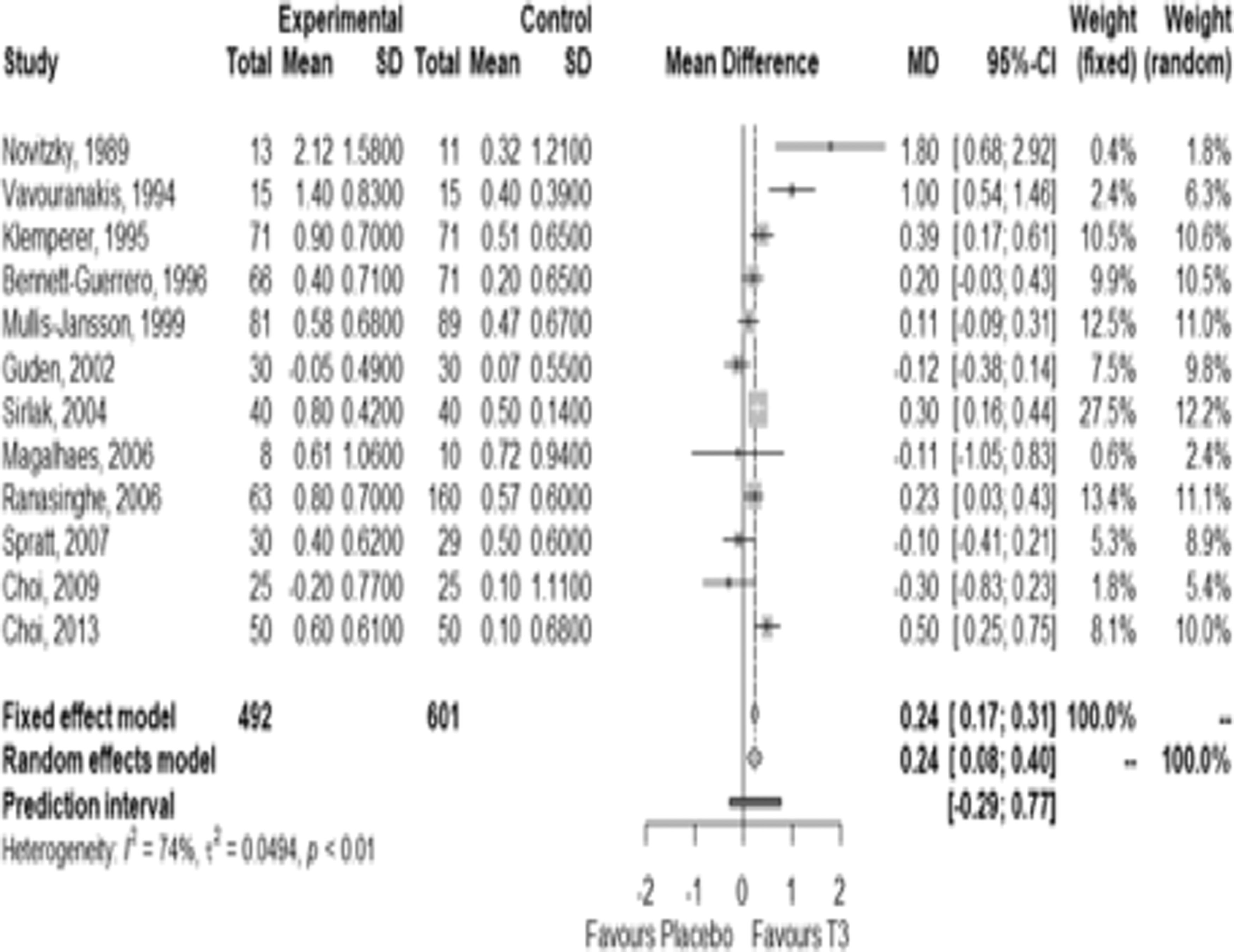
Forest plot of effect of T3 therapy on cardiac index in adults undergoing cardiac surgery. T3, triiodothyronine.
Systemic vascular resistance
In 11 studies including 1069 adult patients undergoing cardiac surgery, T3 therapy was not associated with any significant reduction in systemic vascular resistance (SVR) (SMD of −0.18; CI, −0.43 to 0.08, I 2 = 74%) (eFigure 1 in the Supplementary Data) (23 –33). Prediction interval ranged from −1.04 to 0.69. The mean daily dose of T3 (p = 0.82), route of T3 administration (IV or oral; p = 0.43), baseline LVEF (p = 0.49), or duration of treatment (p = 0.16) were not associated with variation in SVR in adults undergoing cardiac surgery on meta-regression.
T3 treatment in pediatric cardiac surgery
Cardiac index
In three studies including 188 children undergoing cardiac surgery therapy with T3 was associated with no significant change in the cardiac index (MD of 0.0 L/min/m2; CI, −0.01 to 0.01, I 2 = 0%) (eFigure 2 in the Supplementary Data) (36,38,43).
T3 treatment in cardiac donors
Cardiac index and systemic vascular resistance
In three studies including 131 cardiac donors, T3 therapy did not significantly alter cardiac index (MD of −0.15 L/min/m2; CI, −0.64 to 0.33, I 2 = 0%) (Fig. 3) (45,47,48). Similarly, in 2 studies including 79 cardiac donors T3 therapy was not associated with significant reduction in SVR (MD of −93.6 dyn·s/cm5; CI, −423 to 236, I 2 = 0%) (eFigure 3 in the Supplementary Data) (45,48).
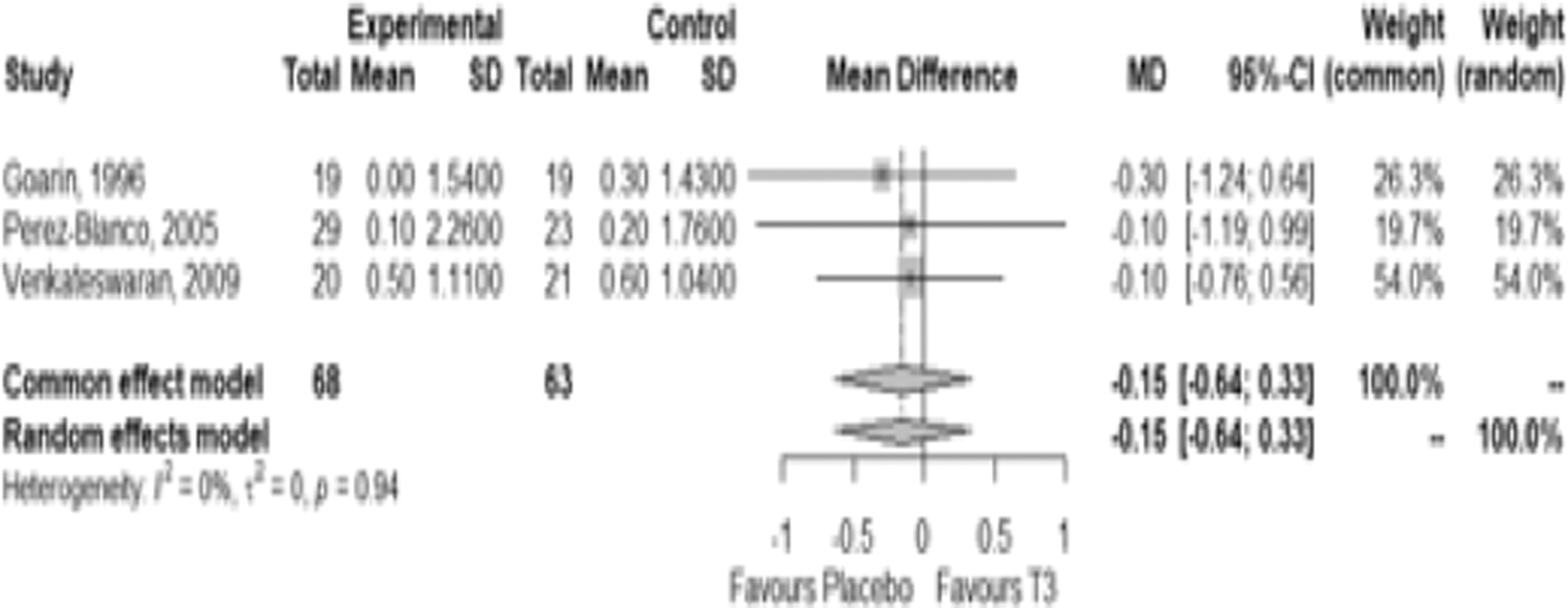
Forest plot of effect of T3 therapy on cardiac index in cardiac donor procedures.
T3 in cardiovascular diseases
T3 treatment in heart failure
In three studies including 83 adults with stable heart failure with reduced ejection fraction and low serum T3 levels, T3 therapy did not significantly improve LVEF (MD of 2.95%; CI, −1.54% to 7.44%, I 2 = 0%) (Fig. 4) (50 –52). Similarly, in these three studies, there was no significant association of T3 therapy with change in N-terminal pro-brain natriuretic peptide (NT-proBNP) levels (MD of −1050.9 ng/L; CI, −2345.0 to 243.2, I 2 = 86%) (eFigure 4 in the Supplementary Data) (50 –52).
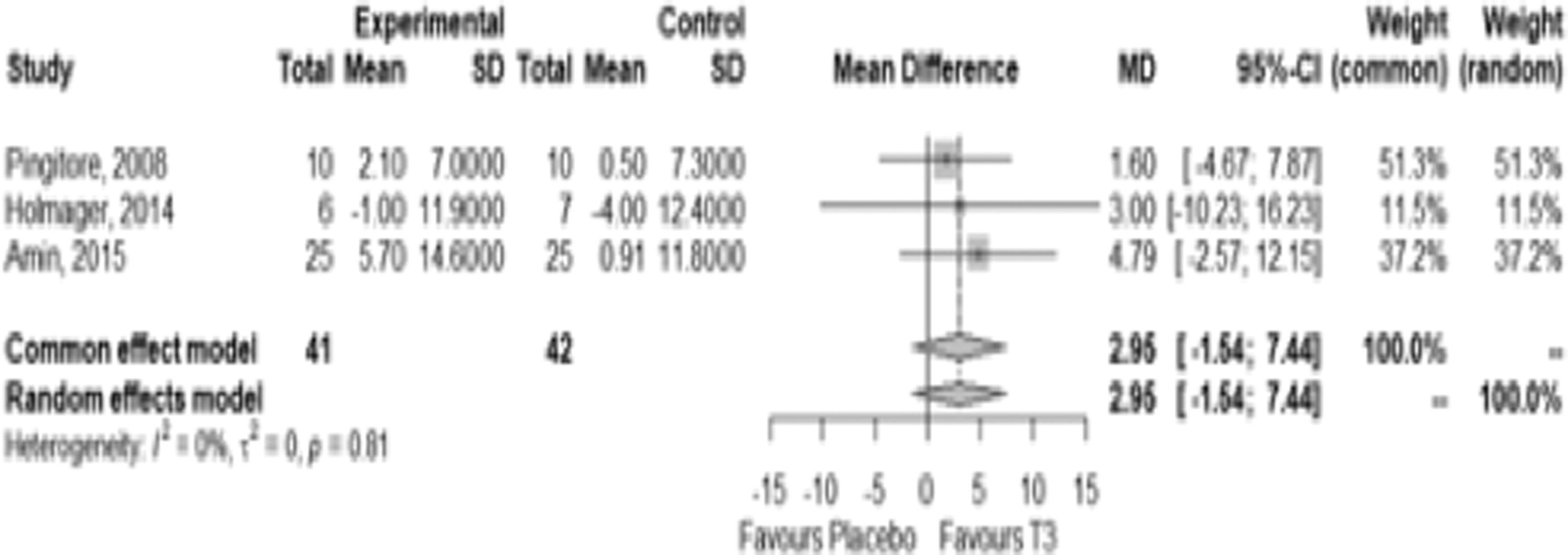
Forest plot of effect of T3 therapy on left ventricular ejection fraction in patients with heart failure and low serum T3 levels.
T3 treatment in acute myocardial infarction
Two studies including 89 participants assessed the utility of T3 supplementation in adult patients with acute myocardial infarction and low or low normal serum T3 levels (10,11). There was no evidence of significant improvement in LVEF over 6 months in these patients (MD of 1.78%; CI, −1.91% to 5.47%, I 2 = 0%) (eFigure 5 in the Supplementary Data). Likewise, there was no significant reduction in infarct volume over 6 months in the T3 group compared with the placebo group (SMD of −0.19; CI, −0.65 to 0.27, I 2 = 0%) (eFigure 6 in the Supplementary Data).

Forest plot of effect of T3 therapy on risk of developing atrial fibrillation in adults and children undergoing cardiac surgical procedures.
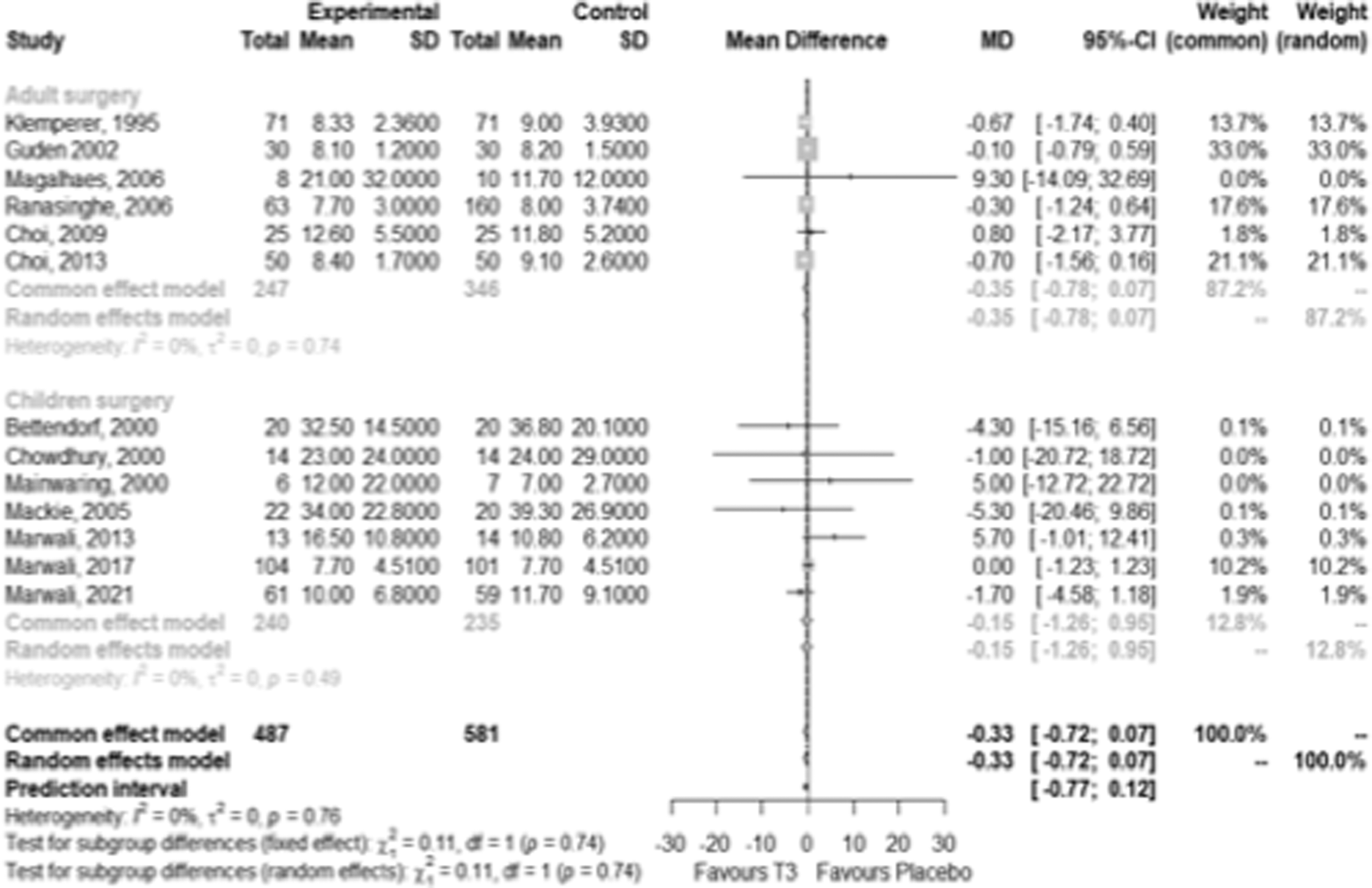
Forest plot of effect of T3 therapy on length of stay in hospital.
Effect of T3 treatment on safety parameters
Heart rate
In 18 studies including 1063 participants (11 studies in adult cardiac surgery, 1 study in children undergoing cardiac surgery, 2 studies in cardiac donors, 3 studies in adults with heart failure, and 1 study in adults with acute myocardial infarction), T3 therapy had no significant effect on heart rate (MD of 2.21 bpm; CI, −0.96 to 5.39, I 2 = 68%) overall nor in any of the subgroups included (eFigure 7 in the Supplementary Data) (11,22 –29,31 –33,35,45,46,50 –52). The prediction interval ranged from −9.45 to 13.87 bpm. The mean daily T3 dose (p = 0.002), duration of treatment (p = 0.04) and studies with LVEF >40% (p = 0.03) were positively associated with heart rate on meta-regression.
Atrial fibrillation
In seven studies in adults (n = 793) and five studies in children (n = 599) undergoing cardiac surgical procedures, T3 therapy was not associated with a higher risk of incident AF with RR of 1.03; CI, 0.84–1.27, I 2 = 0% and RR of 0.77; CI, 0.47–1.26, I 2 = 0%, respectively (Fig. 5) (24,26 –30,33,35,36,41,43,44). The mean duration of follow-up in the studies that were included in the analysis for incident AF ranged from 2.3 to 21 days. In a pilot study that utilized an IV infusion of T3 at relatively high doses (median of 500 μg T3 over 48 hours) in patients with acute anterior myocardial infarction, the incidence of AF was nonsignificantly higher in the T3 group (5/26) compared with the placebo group (1/22) (11).
Mortality
In 9 studies including 839 adults undergoing cardiac surgery, T3 therapy was not associated with higher risk of in-hospital mortality (RR of 1.22; CI, 0.57–2.62, I 2 = 0%) (eFigure 8 in the Supplementary Data) (21,24,26 –30,33). The mean duration of follow-up in the studies that were included in the analysis for mortality ranged from 2.3 to 21 days. In 8 studies including 816 children undergoing cardiac surgery, T3 therapy was associated with lower risk of mortality (RR of 0.52; CI, 0.31–0.87, I 2 = 0%) (eFigure 9 in the Supplementary Data) (34,35,38 –41,43,44). However, the beneficial effect of T3 on mortality outcome in children was mainly influenced by a single trial with high event rates that contributed 61.5% weight to the pooled analysis (43). The pooled RR did not show evidence of benefit of T3 once this trial was removed from the analysis (RR of 0.67; CI, 0.29–1.54, I 2 = 0%). The mean duration of follow-up ranged between 3 days and 24 months.
Effect of T3 treatment on LOS in hospital including intensive care
In 6 studies including 593 adults undergoing cardiac surgery, T3 therapy had no association with LOS in hospital (MD of −0.35 days; CI, −0.78 to 0.07, I 2 = 0%) (Fig. 6) (24,27,29,30,32,33). In 7 studies including 475 children undergoing cardiac surgery T3 therapy was not associated with any significant changes in hospital LOS (MD of −0.15 days; CI, −1.26 to 0.95, I 2 = 0%) (34,36 –38,40,41,43) (Fig. 6). LOS in intensive care postcardiac surgery was no different in the T3 or control groups in both adults and children (eFigure 10 in the Supplementary Data).
Effect of T3 treatment on postoperative inotrope, mechanical assist devices, and ventilation time
In 10 studies including 950 adults and 5 studies with 549 adults postcardiac surgery, T3 treatment was not associated with reduced use of inotropic support or circulatory assist devices (eFigures 11 and 12 in the Supplementary Data and Table 2). On meta-regression, neither the dose, route, or duration of T3 therapy nor underlying LVEF predicted inotrope requirements. In 8 studies assessing postsurgical ventilation duration in 595 children, there was no difference in the T3 versus the placebo groups (eFigure 13 in the Supplementary Data).
Effect of T3 treatment on thyroid function parameters
Overall, serum T3 levels increased, serum thyrotropin (TSH) levels were lower, and T4 levels remained unchanged in the T3 therapy group (eFigures 14–16 in the Supplementary Data). Serum reverse T3 levels were measured in three studies and did not change with T3 therapy (eFigure 17 in the Supplementary Data).
Bias assessment
Risk of bias assessment for each included study is provided in eTable 2 in the Supplementary Data. Overall, no evidence of small study or publication bias was observed (eFigures 18 and 19 in the Supplementary Data).
Sensitivity analysis
Several sensitivity analyses were performed. The main findings was that the risk of using inotropic support postcardiac surgery in adults was lower when fixed effects model was used owing to low heterogeneity between studies (Supplementary Results section in the Supplementary Data).
Discussion
This systematic review and meta-analysis evaluated RCTs of T3 therapy in patients with acute and chronic cardiac conditions. We observed an association between T3 therapy and an improvement in cardiac index in adults undergoing cardiac surgery. However, the quality of the evidence was moderate. In other cardiac conditions including pediatric cardiac surgical procedures, cardiac donor procedures, heart failure, or acute myocardial infarction, T3 therapy was not associated with any evidence of benefit or harm, although this finding was limited by the small number of trials of low to moderate quality included in the meta-analysis.
Compared with previous systematic reviews and meta-analyses of thyroid hormone therapy for postoperative nonthyroidal illness (8,53,54), this systematic review and meta-analysis has included more studies, has assessed other patient groups such as pediatric cardiac surgery, cardiac donors, heart failure, and acute myocardial infarction, and evaluated the economically vital parameter of LOS in hospital in the cardiac surgical procedure groups. Overall, the quality of evidence varied from high to moderate across most outcomes except for the effect of T3 in acute myocardial infarction patients, where the quality was deemed to be poor owing to the inclusion of two pilot RCTs with small number of participants (10,11).
Most experts do not advocate T3 therapy in hospitalized patients with low serum T3 levels as, in their view, the reduced T3 is an adaptive physiological phenomenon (55,56). However, some others argue that nonthyroidal illness and the resultant low T3 level is a manifestation of hypothalamic-pituitary dysfunction and should be corrected (57). Such conflicting views probably explain, at least in part, the variation in thyroid hormone use in cardiac conditions with 31% of intensive care physicians in Canada (58) and 72% of organ procurement organizations in the United States reporting use of thyroid hormone (including T4) for all cardiac donors (59).
Data on the routine use of thyroid hormones in cardiac surgical procedures are not available. Guidelines formulated by the American Thyroid Association recommend against the use of T3 therapy in hospitalized patients with critical illness or heart failure with low T3 levels (60). The results of this meta-analysis suggest that there may be short-term benefits of T3 therapy in adult patients undergoing cardiac surgery but more research is required to assess long-term safety and efficacy as well as patient reported outcomes.
Our systematic review and meta-analysis suggests that T3 use in adult cardiac surgery improves short-term cardiac function with no apparent immediate safety concerns. However, the quality of the evidence is moderate and longer term effects of T3 therapy on important clinical outcomes have not been evaluated. Furthermore, there is no accepted minimal clinically important difference for cardiac index or systemic vascular resistance. Thus, it is unclear whether the observed improvement in cardiac index in adults undergoing cardiac surgery is of clinical value. The benefit of improved cardiac performance that is most likely to be observed in a clinical setting is in the reduced requirement for inotropic support in the immediate postsurgical period and a consequent reduction in the length of intensive care and hospital stay.
Our results suggest that the short-term improvement in cardiac performance may be associated with the trend observed in reduced inotrope use and hospital LOS in adults treated with T3 postcardiac surgery. However, larger adequate designed trials are required to confirm this finding. The other important finding of our analysis is the reassuring short-term safety profile of T3 in high-risk individuals and/or situations. In one study, the occurrence of AF in adults undergoing cardiac surgery was not significantly different in the T3 group during the period of drug infusion and up to 18 hours postsurgery (24). However, the T3-treated group had a lower incidence of AF and fewer required cardioversion when they were followed-up to 5 postoperative days (61).
Conversely, there was a worrying trend of a fourfold higher risk of incident AF in the first 48 hours in a study that utilized high-dose T3 infusion in patients with acute myocardial infarction (11). This finding highlights that close monitoring of high-risk patients is essential, especially when high-dose T3 is used. Moreover, the possible benefits of short-term T3 use in high-risk adults on cardiac function has to be balanced with cost of using and monitoring T3, particularly if an infusion is utilized. Our analysis also suggests that the duration of treatment with T3 may have a direct effect on the improvement in cardiac index and increased heart rate and that the dose of T3 may also influence heart rate.
Thus, adequately designed trials are required to assess the safest, most effective dose and duration of therapy as well as evaluate the long-term benefits and risks of T3 in this group. In children followed for 10 years after cardiac surgery, no effect of T3 therapy was observed on neurocognitive, growth, and cardiac parameters (62). Owing to the limited number of low-quality studies analyzed in pediatric cardiac surgery, cardiac donor operations, heart failure, and acute myocardial infarction patients with low T3 levels, more well-designed trials are required in these groups. Based on the evidence obtained so far, the routine clinical use of T3 in these groups of patients does not appear to be justified, outside a clinical trial.
This systematic review and meta-analysis collected data from RCTs and hence the results obtained are robust. Other strengths of this analysis include the broad clinical outcomes analyzed, multiple sensitivity analyses were performed, and the utilization of GRADE assessment to evaluate quality. However, most studies included relatively small number of participants and long-term outcome data are lacking. Assessment of bias including bias related to small study did not suggest that this could have influenced the results. Another limitation is the high heterogeneity observed for certain outcomes that may be, at least in part, owing to differences in dose, route, and duration of T3 therapy and variations in populations and outcomes being assessed. For example, some studies (adults with heart failure or acute myocardial infarction) only recruited participants with low serum T3 levels, whereas this was not the case with studies in cardiac surgery (where reduction in serum T3 levels is expected but was not a prerequisite for inclusion). In addition, our literature search did not include the gray literature or studies that were published in languages other than English and therefore may have missed some relevant studies.
Conclusions
Based on moderate quality evidence, T3 therapy improves cardiac index in adult patients undergoing cardiac surgery. Trials evaluating longer term clinical outcomes are needed to assess the utility and safety of T3 treatment. There is no improvement in short-term cardiovascular parameters in pediatric patients undergoing cardiac surgery or cardiac donors and, therefore, routine use of T3 is not justified unless used as part of research. Evidence for efficacy and safety for the use of T3 therapy in patients with heart failure or acute myocardial infarction and low circulating T3 levels is inconclusive and potential for benefit or harm cannot be excluded owing to the small number of participants studied and the low quality of evidence. Appropriately designed trials are needed in this group to clarify the role of T3 supplementation.
Footnotes
Data Sharing
The data utilized in this meta-analysis was obtained from published literature. Data for two studies were obtained from the authors directly and can be obtained from the corresponding author on request.
Authors' Contributions
M.T. and A.T. performed literature search and collated data. R.P.W.K., A.B., and S.R. did the statistical analyses. M.T. wrote the first draft of the report with input from A.T., A.B., and S.R.; M.T., A.T., R.P.W.K., A.P., G.I., J.D., A.B., and S.R. provided critical input for the final version of the report. M.T. and S.R. accessed and verified the data. All authors had full access to all the data in the study and have final responsibility for the decision to submit for publication.
Acknowledgments
The authors thank the librarians at Newcastle University for their help and guidance in performing the relevant searches of the various databases.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data