
Abstract
Background:
Primary thyroid lymphoma (PTL) is known to develop mostly in patients with Hashimoto's thyroiditis (HT), and it is rare for it to develop in patients with Graves' disease (GD). The objective of this study was to investigate the clinical features, pathological findings, and long-term outcomes of PTL patients, grouped according to the presence of GD, HT, or no autoimmune thyroid disease (AITDs). The GD group was of major interest due to limited knowledge of the relationship with PTL.
Methods:
In this single-center retrospective cohort study, we reviewed the medical records of all patients diagnosed with PTL between August 1979 and October 2021, and we characterized the patients according to the presence of HT, GD, or no AITDs. Pathological specimens were classified according to the World Health Organization classification. Staging was performed in accordance with the Ann Arbor classification.
Results:
During the 42-year period, 498 participants were diagnosed with PTL. The median age was 68 (interquartile range 61–76) years, and 221 patients were stage IE, whereas the remaining 277 patients were stage IIE. Of the PTL patients, 431 (86.6%) were diagnosed with HT, 9 (1.8%) were diagnosed with GD, and 58 (11.6%) did not have AITDs. All nine patients with GD were positive for anti-thyroglobulin antibody and/or anti-thyroid peroxidase antibody. All patients with GD were treated with anti-thyroid medication. There were no significant differences in the proportions of each subtype of PTL between the PTL patients with GD and all subjects with PTL (p = 0.51), PTL patients with HT (p = 0.51), or PTL patients without AITDs (p = 0.48). The median follow-up time was 6.2 (interquartile range 3.0–10.7) years after the diagnosis of PTL. The Kaplan-Meier curve analyses showed no significant differences in overall survival and event-free survival between PTL patients with GD and those with HT (p = 0.37), or between PTL patients with GD and those without AITDs (p = 0.43).
Conclusions:
The PTL was observed with HT in a majority of cases, and rarely with GD (1.8%). The proportions of each pathological subtype of PTL and the prognosis of PTL were not different between the patients with GD and those with HT or those without AITDs.
Introduction
Primary thyroid lymphoma (PTL) is an uncommon malignant tumor that represents about 1–5% of all thyroid malignancies, 1–2.5% of all malignant lymphomas, and 2.5–7% of all extra-nodal lymphomas (1 –3). It has been shown that PTL typically occurs with a female predominance, with a female to male ratio of 2.2–4:1 (3,4), and it occurs especially in elderly people with a mean age in their 60s (3 –7).
Hashimoto's thyroiditis (HT) is believed to be a basis for PTL, and it is reported that having HT increases the risk of PTL 67 to 80 times higher than the general population (8,9). Indeed, previous reports showed that about 60–90% of patients with PTL also had HT (5,6,10), and a correlation between HT and PTL has been discussed. In contrast, only a few articles about PTL that developed in patients with Graves' disease (GD) have been published, and most were case presentations (11 –14).
Since the prevalence of PTL with GD is even rarer, information about their clinical features and the differences in pathological findings between PTL with HT and those with GD are uncertain. In this retrospective cohort study, our primary objective was to examine the clinical features, pathological findings of PTL patients, grouped according to the presence of GD, HT, or no autoimmune thyroid diseases (AITDs). A secondary objective was to examine the long-term outcomes of these patients. We described in detail the features of patients with PTL and GD, given the limited knowledge about this group.
Materials and Methods
Subjects
All subjects were patients of Ito Hospital and their medical records were reviewed to obtain information about their clinical outcomes, pathological findings, and laboratory data. Clinical follow-up data were acquired from medical records and communication with the referring physicians. Between August 1979 and October 2021, 610 patients were diagnosed with malignant lymphoma according to pathological findings from thyroid specimens acquired by open biopsy or wider surgical procedures, including lobectomy or total thyroidectomy.
The clinical stage was evaluated by imaging modalities such as thyroid ultrasonography, computed tomography, 67Ga-scintigraphy, 2-deoxy-2-fluoro-
According to this definition, because the primary site of the lymphoma was uncertain, 112 patients whose stages were higher than IIIE were excluded from this study. Figure 1 shows the patient flow diagram. Subsequently, 498 patients were diagnosed with PTL. This study included only the primary PTL patients; thus, patients with PTL occurring as a result of relapse or progression of a previous lymphoma were excluded. A relapse of PTL was defined as the involvement of new sites or recurrence in original sites after having completed initial treatment for PTL.

Patients' flow diagram. A total of 610 patients were diagnosed with lymphoma from thyroid histological findings, and 112 patients were excluded due to high stage level, leaving 498 patients with final diagnoses of primary thyroid lymphoma. For the outcome analyses, 32 patients were excluded due to short follow-up duration. Thus, 465 subjects were included in the outcome analyses.
The diagnosis of GD was made based on both hyperthyroidism and positive thyrotropin receptor antibody (TRAb) or high radioactive iodine uptake (RAIU). In our facility, medication with antithyroid drugs (ATDs) or potassium iodide (KI) was the first-line treatment for GD (15,16); all GD patients were treated with medication from their diagnoses. In addition, HT was diagnosed based on positive anti-thyroid peroxidase antibody (TPOAb) and/or anti-thyroid globulin antibody, with hypothyroidism or normal thyroid function. This study was approved by the Ethics Committee of Ito Hospital (Approval No. 341), and signed patient consent was not required.
Laboratory methods
Serum-free triiodothyronine (fT3), serum-free thyroxine (fT4), and thyrotropin (TSH) levels were measured by using kits that were commercially available at that time. A TRAb evaluation kit has been available since June 1982 in our facility, and the value was measured by using radioimmunoassay (RIA) kits (normal range: <10%; Cosmic Corporation, Tokyo, Japan) until September 2008; the ECLusys TRAb Electrochemiluminescence immunoassay kit (normal range: <2.0 IU/L; Roche Diagnostics, Basel, Switzerland) was then used to measure TRAb from October 2008. TPOAb and thyroglobulin antibody (TgAb) were evaluated by using TPOAb and TgAb RIA kits (Cosmic Corporation) from December 1994. The measurement methods of TgAb and TPOAb used before December 1994 were explained in Supplemental Methods.
Cut-off values of TgAb and TPOAb were decided based on the receiver operating characteristic curve analysis that showed the highest specificity and the pathological findings (17).
Pathological examination
The pathological diagnosis was established by the examination of thyroid specimens obtained by open biopsy or wider surgical procedures, including lobectomy and total thyroidectomy. Pathological diagnoses were confirmed according to the World Health Organization (WHO) classification. Since this study included patients who were diagnosed before the development of the WHO classification, the specimens of those patients had been reviewed and reclassified according to the WHO classification in 2010 for our prior study (6). Paraffin blocks of the thyroid specimens were obtained and re-immuno-stained for review. An expert hematologist and an expert thyroid pathologist reviewed the specimens separately, and they made the diagnosis for each patient.
The histological criteria of chronic lymphocytic thyroiditis are described as follows: (a) focal or diffuse lymphocytic aggregation or infiltration; (b) degeneration of thyroid follicular cells (enlargement and collapse); (c) fibrosis; and (d) oxyphilic metaplasia of thyroid epithelial cells. When these findings were partially and/or totally recognized in the specimens, the diagnosis was chronic lymphocytic thyroiditis (HT) (18).
Statistical analysis
Data are expressed as medians and interquartile range for continuous variables. Fisher's exact test was used to compare the proportion of histopathological types of PTL among the AITDs in the subjects, and Pearson's chi-squared test was used to compare thyroid function outcomes. The patients who underwent lobectomy (n = 50) and total thyroidectomy (n = 16) were excluded from the analysis of thyroid function outcomes.
Kaplan-Meier curve analysis was performed to calculate overall survival (OS) and event-free survival (EFS). For the prognostic analysis, 32 patients whose follow-up times were shorter than 90 days were excluded. The OS was calculated from the date of the initial surgical procedure to the last follow-up or death from any cause, and EFS was defined as the time from the initial surgical procedure to relapse or death in remission.
Data on patients who were alive at the last follow-up were censored for the analysis of OS, and the data on patients who were alive without relapse of PTL at the last follow-up were censored for the analysis of EFS. The log-rank test was used to compare the differences in OS and EFS between the groups. A p-value <0.05 was considered statistically significant. Baseline parameters and the collected data were analyzed by using JMP version 14.0 software (SAS Institute, Cary, NC).
Results
Characteristics of the patients with PTL and GD
During the observation period, 498 patients (102 males and 396 females) were diagnosed with PTL. Detailed information of the 498 patients is shown in Table 1. Their median age was 68 (interquartile range 61–76) years, and median follow-up time was 6.2 (interquartile range 3.0–10.7) years after the diagnosis of PTL. Two hundred twenty-one patients were stage IE, whereas the remaining 277 patients were stage IIE. The pathological diagnoses were 207 diffuse large B cell lymphomas (DLBCLs), 257 mucosa-associated lymphoid tissue (MALT) lymphomas, 28 DLBCLs with MALT lymphoma, and 6 follicular lymphomas.
Characteristics of Primary Thyroid Lymphoma Patients and Comparison of Pathological Diagnoses, Treatment, and Outcomes of Primary Thyroid Lymphoma Patients by Background Thyroid Autoimmune Status
AITDs, autoimmune thyroid disease; CI, confidence interval; CMT, combined modality therapy; DLBCL, diffuse large B cell lymphoma; EFS, event-free survival; GD, Graves' disease; HT, Hashimoto's thyroiditis; MALT, mucosa-associated lymphoid tissue lymphoma; OS, overall survival; PTL, primary thyroid lymphoma; RT, radiation therapy.
Of the 498 patients with PTL, 9 (1.8%) (8 females, 1 male) had diagnoses of GD before or simultaneously with the diagnosis of PTL (Table 2). The median age at diagnosis of PTL was 64 (interquartile range 58.5–76) years, and the median time between the GD and PTL diagnosis was 13.3 (interquartile range 4.65–23.6) years. In patients with a history of GD, the median follow-up time was 5.0 (interquartile range 1.3–12.0) years after the diagnosis of PTL.
Characteristics of the Nine Patients with Primary Thyroid Lymphoma with Graves' Disease
Staging was decided according to the Ann Arbor classification.
CMT, combined modality therapy; KI, potassium iodide; MMI, methimazole; NA, not available; PTU, propylthiouracil; STT, subtotal thyroidectomy; TgAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; TRAb, thyrotropin receptor antibody; TT, total thyroidectomy.
Seven of nine patients were in the remission period of GD at the time of PTL diagnosis, and two of the six patients were on treatment with levothyroxine for subsequently developed hypothyroidism. One patient who was initially treated with methimazole (MMI) developed recurrence of GD two years before the diagnosis of PTL and received treatment with KI alone. Another patient who was on medication with MMI at the diagnosis of PTL had one remission, though relapse with GD occurred 10 years before the PTL diagnosis, and treatment with MMI was re-started.
One male patient diagnosed with GD and PTL simultaneously was also treated with KI alone due to concern about the side effects of ATDs, and he was also expecting to undergo surgery within a short time. Of the nine subjects, three were diagnosed by RAIU, four were diagnosed by positive TRAb, and the remaining two were diagnosed at other hospitals, and, therefore, their TRAb values were not available.
Conversely, the TRAb titer at the diagnosis of PTL was available in seven patients; six of the seven patients were negative for TRAb, whereas one patient who was diagnosed with GD at the same time was positive for TRAb. As initial treatment for GD, all patients were treated with medication. In detail, six patients were treated with MMI, two patients were treated with propylthiouracil, and one patient was treated with KI. One of the patients treated with MMI underwent subtotal thyroidectomy one year after the diagnosis of GD due to a huge goiter.
TgAb and TPOAb were tested in all nine patients at the diagnosis of PTL, and all subjects were positive in at least one of the tests.
Before they were diagnosed with PTL, all nine patients underwent ultrasound examination, and the images showed focal low echoic areas that were suspected to be PTL. The reasons for the ultrasound examinations were as follows: enlargement of the thyroid gland in six patients, regular monitoring for previously detected adenomatous nodules in two patients, and an initial screening test in one patient.
Open biopsy was performed in six of the nine subjects to obtain thyroid specimens, whereas one patient underwent lobectomy, and the remaining two underwent total thyroidectomy. The reason for lobectomy was that the tumor was small, and it was difficult to detect the tumor from the superficial appearance. In addition, the reasons for total thyroidectomy were that one patient was diagnosed with GD and PTL at the same time, and he also had atrial fibrillation, and another patient had had GD for almost 20 years. Thus, they preferred definitive therapy for GD to medication.
Pathological diagnoses and treatment for PTL with GD
The pathological diagnoses of the nine patients with PTL and GD consisted of DLBCL (n = 2, 22.2%), MALT lymphoma (n = 6, 66.6%), and DLBCL with MALT lymphoma (n = 1, 11.1%). There were no significant differences in the proportions of each subtype of PTL between the PTL patients with GD and all subjects with PTL (p = 0.51). Of the nine patients, six were stage IE (DLBCL: MALT = 1:5), whereas the remaining three patients were stage IIE (DLBCL:DLBCL with MALT:MALT = 1:1:1).
Examination of the thyroid specimens of three subjects who underwent surgery showed lymphocyte infiltration in the tissue without lymphoma structures. Figures 2 and 3 show the pathological findings of case 8. Figure 2A shows diffuse hyperplasia representing GD, and Figure 2B to D show lymphocytic infiltration in the thyroid, swelling and degenerated follicular cells, and Hurthle cells, which represent HT.
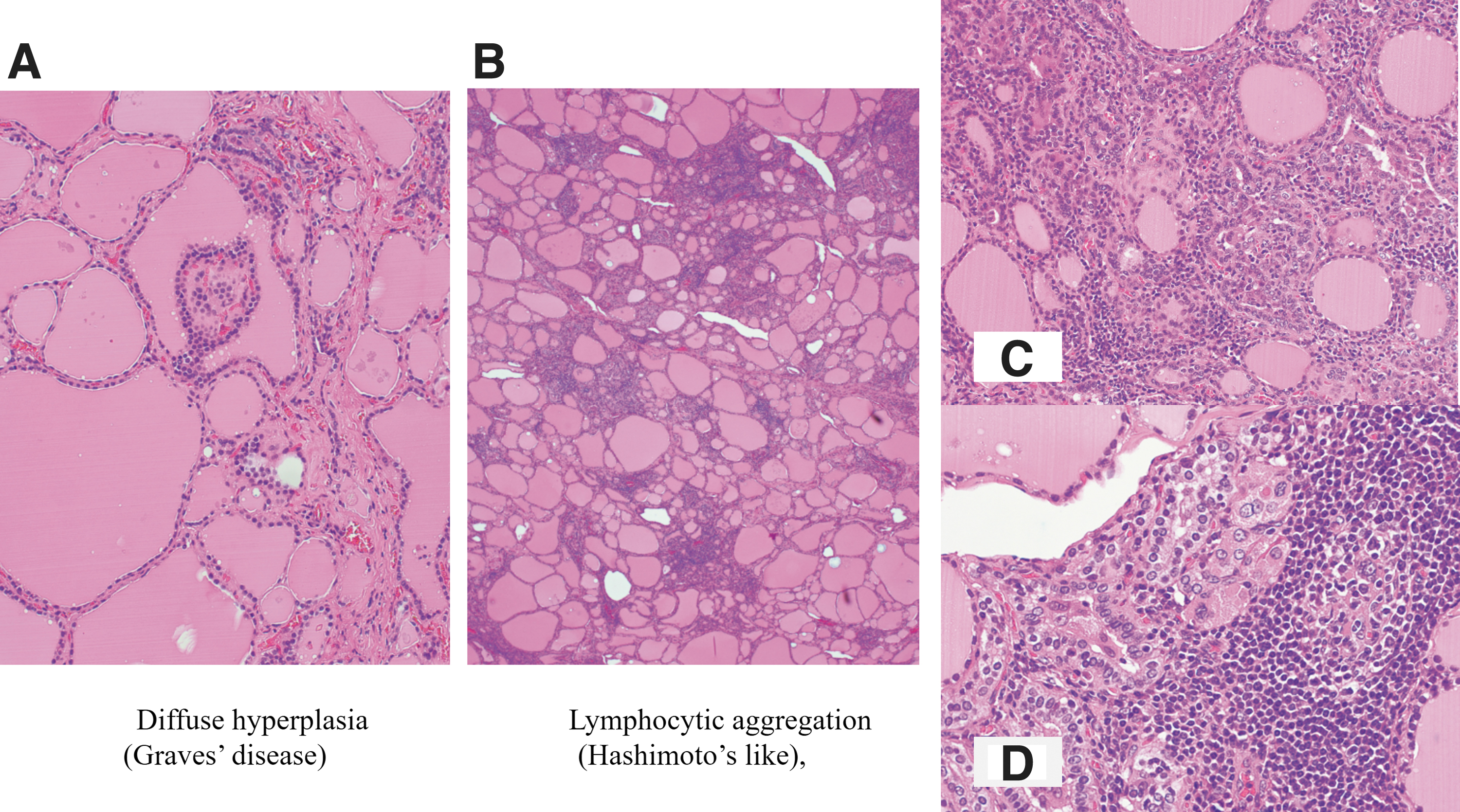
Pathological findings of the thyroid showing autoimmune thyroiditis in case 8. (

Pathological findings of MALT lymphoid tissue in case 8. (
As treatment for PTL, radiation therapy (RT), chemotherapy, combined modality therapy (CMT) (RT+chemotherapy), and surgery were provided. Three patients received RT alone, one received chemotherapy, three were treated with CMT, and two underwent total thyroidectomy. All the patients achieved complete response, though one with MALT lymphoma relapsed two years later.
Comparison of the pathological diagnoses and outcomes in the PTL patients with HT to those in patients with GD
During the 42-year period, 498 subjects were diagnosed with PTL. Of these patients, 431 (86.5%) (343 females and 88 males) were diagnosed with HT. The median follow-up time for the patients with HT was 5.9 (interquartile range 2.5–10.3) years after the diagnosis of PTL. Detailed pathological diagnoses were DLBCL (n = 178, 41.3%), MALT lymphoma (n = 223, 51.7%), DLBCL with MALT lymphoma (n = 24, 5.6%), and follicular lymphoma (n = 6, 1.4%) (Table 1).
Since DLBCL with MALT lymphoma contained DLBCL tissue, and it is clinically treated as aggressive lymphoma, DLBCL with MALT lymphoma was classified as DLBCL lymphoma in the statistical analysis. Then, the prevalence of DLBCL lymphoma became 46.9% (n = 202). When the distribution of the pathological diagnoses in patients with HT was compared with that in patients with GD, there was no significant difference between the two groups (p = 0.51).
The Kaplan-Meier curve analysis showed that the 5-year OS rates of the PTL patients with GD and those with HT were 100% [confidence interval (CI) 1.0–1.0] and 92.1% [CI 0.89–0.95], respectively, and the 10-year OS rates of the PTL patients with GD and those with HT were 100% [CI 1.0–1.0] and 88.6% [CI 0.85–0.92], respectively (p = 0.37) (Fig. 4A).
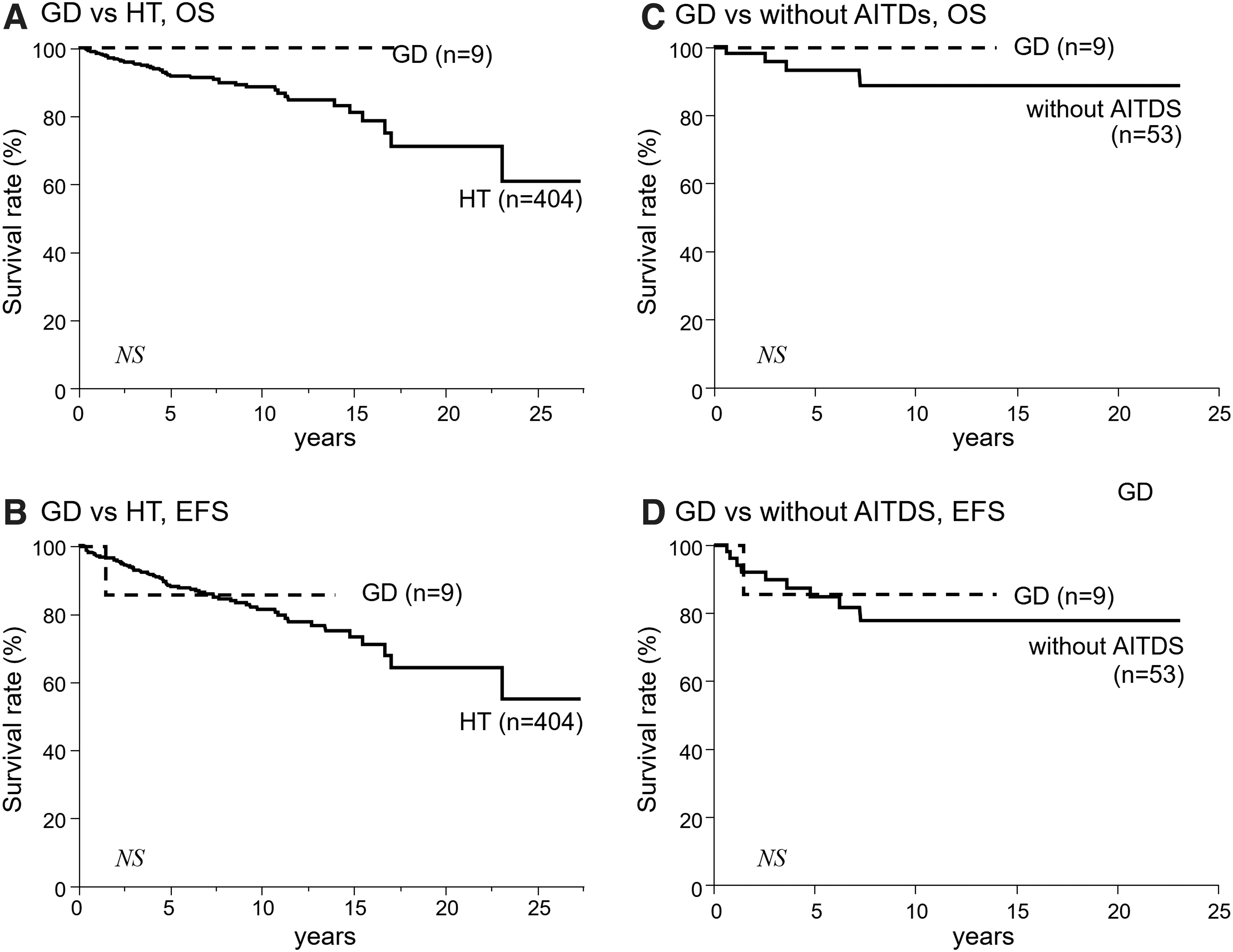
Kaplan-Meier curve analyses showing OS and EFS according to the background thyroid autoimmune status. The OS and EFS are compared between the groups with GD and with HT and between the group with GD and the group without AITDs. There are no significant differences in OS and EFS between the group with GD and with HT
The Kaplan-Meier curve analysis also showed that the 5-year EFS rates of the PTL patients with GD and those with HT were 85.7% [CI 0.60–1.12] and 88.3% [CI 0.85–0.92], respectively, and the 10-year EFS rates of the PTL patients with GD and those with HT were 85.7% [CI 0.60–1.12] and 81.3% [CI 0.76–0.86], respectively (p = 0.83) (Fig. 4B). There was no significant difference in the rate of developing hypothyroidism after treatment for PTL between the PTL patients with GD and the PTL patients with HT (p = 0.98).
Comparison of the pathological diagnoses and outcomes in the patients with PTL with GD to those without AITDs
Of the 498 patients with PTL, 58 (11.6%) (45 females and 13 males) did not show positive results for any AITDs, including GD and HT. The median follow-up time of the PTL patients without AITDs was 5.7 (interquartile range 1.9–10.4) years after the diagnosis of PTL. Their pathological diagnoses of PTL were DLBCL (n = 27, 46.6%), MALT type lymphoma (n = 28, 48.2%), and DLBCL with MALT (n = 3, 5.2%) (Table 1).
Comparing the distribution of the pathological diagnoses in PTL patients with GD to that without AITDs, no significant difference was seen between the two groups (p = 0.48). Similarly, when the distribution of pathological diagnoses in PTL patients with any AITDs was compared with that of the patients without AITDs, there was also no significant difference between the two groups (p = 0.58).
The Kaplan-Meier curve analysis showed that the 5- and 10-year OS rates of the PTL patients without AITDs were 93.1% [CI 0.85–1.01] and 88.6% [CI 0.78–1.00], respectively (Fig. 4C), and the 5- and 10-year EFS rates of the PTL patients without AITDs were 86.5% [CI 0.74–0.95] and 79.4% [CI 0.64–0.91], respectively (Fig. 4D). There was no significant difference in these rates between the PTL patients with GD and those without AITDs (p = 0.43 for OS rates and p = 0.77 for EFS rates).
Comparing the thyroid function outcomes, there was no significant difference in developing hypothyroidism after PTL treatment between the two groups (p = 0.41). However, when the thyroid function outcome was compared between the groups of PTL with AITDs (n = 373) and without AITDs (n = 51), there was a significant difference in the prevalence of becoming hypothyroid (312/373 patients vs. 34/51 patients) (p = 0.003).
Discussion
It has been reported that PTL usually occurs in patients with HT, and having HT increases the risk of developing PTL 67–80 times higher than not having HT (8,9). Even though the prevalence of PTL is quite low, there have been some reports of the characteristics, treatment methods, and even prognostic factors of the tumor (3,6,19,20). In contrast, PTL in patients with GD is much rarer than in those with HT.
Zeki et al. reported the first case of PTL associated with GD in 1985 (11), and other case reports followed (12 –14). However, due to the rarity of PTL with GD, it was difficult to understand the general outline and characteristics of this disease. The present study was able to show the prevalence of PTL in GD, which was 1.8% of all PTL.
As previously reported, lymphocyte infiltration and chronic inflammation due to HT are considered to be the basis of PTL (8,9); however, nine PTL patients in the present study had a background of GD. From the viewpoint of thyroid histopathology, lymphocyte infiltration, in particular, is also one of the characteristics of the thyroid in GD, as shown in Figure 1 (21), similar to the thyroid in HT.
Taking this into account, it could be suggested that the thyroid tissue of the patients with GD might also be a basis for PTL. Another possible reason that these nine GD patients developed PTL was that they were all positive for at least one of the antibodies for auto-immune thyroiditis (antibody to thyroid peroxidase or thyroglobulin).
It has been reported that TPOAb and/or TgAb were positive in some patients with GD, though Mclachlan et al. showed that these antibodies in patients with GD were polyclonal (22), and thus may represent a secondary immune response reflecting controlled autoimmune thyroiditis. However, a transition in thyroid function in patients with HD, from hypothyroidism to hyperthyroidism with positive TRAb, the development of GD, has been reported (23).
The pathogenesis of GD is believed to be due to both genetic and environmental factors, but it has not been fully clarified. Stefan et al. identified the disease-associated genetic variants (24), and according to their hypothesis, GD develops in a background of a genetically susceptible individual who has lost proper epigenetic interaction, resulting in the development of TSH receptor auto-immunity. This suggests that, for patients who have both TRAb and TPOAb and/or TgAb, they might have the possibility of not only developing both hyperthyroidism and hypothyroidism, but also having an increased risk of developing PTL.
This study also clarified the pathological diagnoses of PTL by an auto-immune thyroid background and analyzed the differences between the groups. The present study did not show any significant differences in the pathological diagnoses between the groups with and without AITDs, suggesting that there may be other factors that evoke lymphoma tissue.
Wu et al. (25) recently showed a significant association between CD274 and TNFRSF14 genetic changes and thyroid MALT lymphoma accompanied with HT, and they assumed that the inactivation of CD274 and TNFRSF14 in thyroid MALT lymphoma B cells may be one of the causes for the development of MALT lymphoma. According to their results, even though patients do not have any AITDs, these specific genetic changes could be another cause of lymphoma development.
As limitations, there are a few points to consider. First, the number of patients was still small and included only Asian, especially Japanese, patients. Thus, further investigations that include larger numbers of patients from diverse ethnic groups will be needed. Second, genetic examinations, such as human leukocyte antigen (26), were not conducted in the present subjects.
Since the relationship between HT and MALT lymphoma at the genetic level has been reported, it would be valuable if it could be evaluated. Finally, since this was a retrospective, observational study, the data obtained from the medical records were limited.
In conclusion, PTL was observed with HT in the majority of cases (86.6%), rarely with GD (1.8%), and the remaining cases (11.6%) were without AITDs. The proportions of each pathological subtype of PTL and the prognosis of PTL were not different between the patients with GD and those with HT or those without AITDs.
Footnotes
Authors' Contributions
Data curation: N.S., R.Y., K.M., A.K., A.S., T.M., M.F., and M.M.
Writing original draft: N.S.
Critical revision of the article: J.Y.N., A.Y., N.W.
Supervision: R.K., K.S., and K.I.
All authors read and approved this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data