
Abstract
Background:
Active surveillance (AS) is offered as a choice to patients with low-risk papillary thyroid microcarcinoma (PTMC). This study aimed to identify patient and physician factors associated with the choice of AS.
Methods:
We conducted a cross-sectional survey of patients with low-risk PTMC who were enrolled in a prospective study comparing outcomes following AS and surgery. Patients completed a questionnaire to assess their prior knowledge of the disease, considerations in the decision-making process, and reasons for choosing the treatment. We also surveyed 19 physician investigators about their disease management preferences. Variables affecting the patients' choice of AS, including patients' characteristics and their decision-making process, were analyzed in a multivariable analysis.
Results:
The response rate of the patient survey was 72.8% (857/1177). Among the patients who responded to the survey, 554 patients (128 male; mean age 49.4 ± 11.6 years; response rate 73.4%) with low-risk PTMC chose AS (AS group), whereas 303 patients (55 male; 46.6 ± 10.7 years; 71.8%) chose immediate surgery (iOP group). In the AS group, 424 patients (76.5%) used a decision aid, and 144 (47.5%) used it in the iOP group. The choice of AS was associated with the following variables: patient age >50 years (odds ratio 1.713 [confidence interval, CI 1.090–2.690], p = 0.020), primary tumor size ≤5 mm (odds ratio 1.960 [CI 1.137–3.379], p = 0.015), and consulting an endocrinologist (odds ratio 114.960 [CI 48.756–271.057], p < 0.001), and use of a decision aid (odds ratio 2.469 [CI 1.320–4.616], p = 0.005). The proportion of patients who were aware of AS before their initial consultation for treatment decision was higher in the AS group than in the iOP group (64.6% vs. 56.8%). Family members were reported to have influenced the treatment decisions more in the iOP group (p = 0.025), whereas the AS group was more influenced by information from the media (p = 0.017). Physicians' attitudes regarding AS of low-risk PTMC tended to be more favorable among endocrinologists than surgeons and all became more favorable as the study progressed.
Conclusions:
Emerging evidence suggests that physicians' attitudes and communication tools influence the treatment decision of low-risk PTMC patients. Support is needed for patient-centered decision making. (Clinical trial No: NCT02938702).
Introduction
Active surveillance (AS) has been adopted as an alternative to immediate surgery in patients with low-risk papillary thyroid microcarcinoma (PTMC), which is defined as a papillary thyroid carcinoma (PTC) measuring ≤10 mm without clinically evident metastases or local invasion and no convincing cytological evidence of aggressive disease. 1 –3 Guidelines for the management of thyroid nodules and cancer describe AS as a treatment option for low-risk PTMC. 1,4 –6 A Japanese clinical practice guideline recommended adopting AS for low-risk PTMC after an extensive explanation of the situation and the patient giving informed consent, 4 and a clinical framework for risk stratification. 7 A choice between AS or immediate surgery of low-risk PTMC has largely been determined by the patient's choice after discussing treatment modalities with the physician. Therefore, it is important to understand the factors that influence patients' treatment choice to inform optimal physician–patient communication.
Previous studies of healthy subjects using a hypothetical scenario about low-risk PTC reported that the terminology for describing small PTC and health literacy influenced treatment decision making for PTC. 8 –10 Our previous studies identified that patients with low-risk PTMC who chose AS displayed a better psychosocial quality of life (QoL) at the time of the treatment decision than those who chose immediate surgery. 11,12 Recent studies investigated the factors influencing treatment choice through interviews with patients with low-risk PTMC, and similarities and differences were noted between those who chose AS and immediate surgery. 13,14 In addition to the patient's understanding of the disease and their individual characteristics, the physician who provides information about the prognosis, specific adverse events, and medical cost of each treatment strategy may also have a major influence on a patient's decision. In this regard, Brito et al 15 developed a conversation aid called “Thyroid Cancer Treatment Choice” and reported that its use increased acceptance of AS in low-risk Korean PTMC patients.
In this study, our aim was to identify factors that influence the patient's decision about initial treatment for their low-risk PTMC from both a patient and physician perspective. We analyzed surveys from 857 patients enrolled in an ongoing Korean multicenter prospective study as well as from 19 physician investigators involved in the study. Data on patients' characteristics and their decision-making process were also analyzed.
Materials and Methods
Study participants
This study was a cross-sectional survey and part of the ongoing multicentered prospective cohort study on AS of PTMC (MAeSTro), which has completed the recruitment of participants. The diagnosis and enrollment criteria of patients and the cohort protocol were described previously. 16 Patients diagnosed with PTMC without suspected major organ involvement, lymph node or distant metastasis, poorly differentiated histology, or a variant with a poor prognosis were included. The patients were enrolled from May 2016 to January 2020. In a process of selecting an initial treatment, the participants chose AS or immediate surgery. During this process, patients were provided with a standardized and balanced explanation about the pros and cons of each treatment modality and were allowed to choose their preferred management. The contents of the explanations provided to the patients were discussed and shared among the physicians participating in this study before patient enrollment. The Korean version of the Thyroid Cancer Treatment Choice 15 was also used according to the preference of each physician.
The study was approved by the Institutional Review Boards of Seoul National University Hospital (SNUH, Seoul, Korea; IRB# 1603-044-747), Seoul National University Bundang Hospital (SNUBH, Seongnam, Korea, IRB# B-1605-348-402), and the National Cancer Center (NCC, Goyang, Korea, IRB# NCC2016-0183). Informed consent was obtained from all participants.
Surveys from study participants and physicians
The survey for the study participants consisted of five questions about their prior knowledge of thyroid cancer treatment, opinions or information considered in the decision-making process, and reasons for choosing AS or immediate surgery (Supplementary Material S1). The endocrinologists (Y.H., J.H.M.) and thyroid surgeons (J.Y.C., K.E.L.) on the research committee of MAeSTro drafted the surveys for patients and physicians, and all committee members, including endocrinologists, thyroid surgeons, radiologists, and preventive medicine doctors, approved the final versions. Some physicians and nurses who were not on the research committee at SNUH also reviewed the survey items (Supplementary Table S3).
Study participants were asked to provide the opinions or information they considered when choosing treatment for low-risk PTMC. This survey item provided five examples that are commonly considered in the initial treatment choice, including the opinions of the patients, their physicians, family and friends or coworkers, information from the media, and an open-ended “others” item. Participants were requested to give 10 points to the item that influenced their choice the most and give the rest relative scores. Each score was converted to a number multiplied by 10 and divided by the sum of the scores given for each item, and used in the analyses. This converted score represents the relative impact of each item, taking the total impact on each patient's treatment choice as 10. Each study participant was surveyed by a research assistant after consulting with their physician and making a decision about their treatment strategy.
They completed a written questionnaire, and if necessary, the research assistant provided guidance. When the participants answered the question about prior knowledge of thyroid cancer treatment, the research assistant explained that the question was about their knowledge of the condition before their initial consultation. For the questions about their reasons for choosing AS or immediate surgery, participants were requested to choose one answer. Study participants did not receive remuneration for the survey.
The survey for physicians was developed to investigate their attitudes and beliefs regarding AS for low-risk PTMC (Supplementary Material S2). This survey consisted of seven questions about the physicians' recommendation to patients with low-risk PTMC who had >10 years of life expectancy, their view of AS as a major treatment option for low-risk PTMC, their opinion about the effect of AS on survival rate, their opinion on the treatment of low-risk PTMC, the cases where immediate surgery should be recommended first, and advantages and disadvantages of AS for patients with low-risk PTMC. The survey items were adopted from previous studies 17,18 and approved by the members of the research committee. This survey was conducted online through email in June 2021 after subject enrollment was completed, and follow-up was underway. For some questions, physicians were asked to distinguish their thoughts at the beginning of the study and their current thoughts.
Clinical and laboratory data
A comprehensive physical examination and a general health interview were performed for each patient, as previously reported. 16 Height and weight were measured with the patient in an upright position wearing light clothing without shoes or accessories using an electronic scale. Body mass index was calculated as weight (kg)/height2 (m2). Laboratory data were collected as described in Moon et al. 16 Serum thyrotropin levels were measured using an immunoradiometric assay (DiaSorin SPA, Saluggia, Italy at SNUH; and Cisbio International, Gif-sur-Yvette, France at SNUBH and NCC).
Statistical analyses
Categorical variables were presented as numbers and percentages, whereas continuous variables with a normal distribution were expressed as mean ± standard deviation, and variables with a non-normal distribution were expressed as median values (interquartile ranges). Pearson's chi-square test or Fisher–Freeman–Halton's exact test was used to compare categorical variables. Student's t-test was used to compare continuous variables with a normal distribution, and the Mann–Whitney U test was used for variables with a non-normal distribution. Multivariable logistic regression analysis was used to estimate the association between patients' baseline characteristics and decision-making process and choosing AS. A two-tailed p < 0.05 was considered statistically significant. All statistical analyses and data preparation were performed using IBM SPSS Statistics (version 28.0; IBM Corporation, Armonk, NY).
Results
Baseline clinical characteristics
The study population was a total of 1177 of 1182 screened patients who were enrolled in MAeSTro at 3 participating centers (SNUH, SNUBH, and NCC) (Fig. 1). Among these, 554 patients who chose AS (AS group) as their initial treatment of low-risk PTMC and 303 who chose immediate surgery (iOP group), completed the survey about their treatment choice (response rate, 72.8% [857/1177] in total, 73.4% [554/755] in the AS group, 71.8% [303/422] in the iOP group). The survey for physicians was completed by all 19 eligible physicians (SNUH, 5 endocrinologists and 2 surgeons; SNUBH, 5 endocrinologists; NCC, 3 endocrinologists and 4 surgeons) who consulted with each study participant and signed an informed consent form (response rate, 100%).
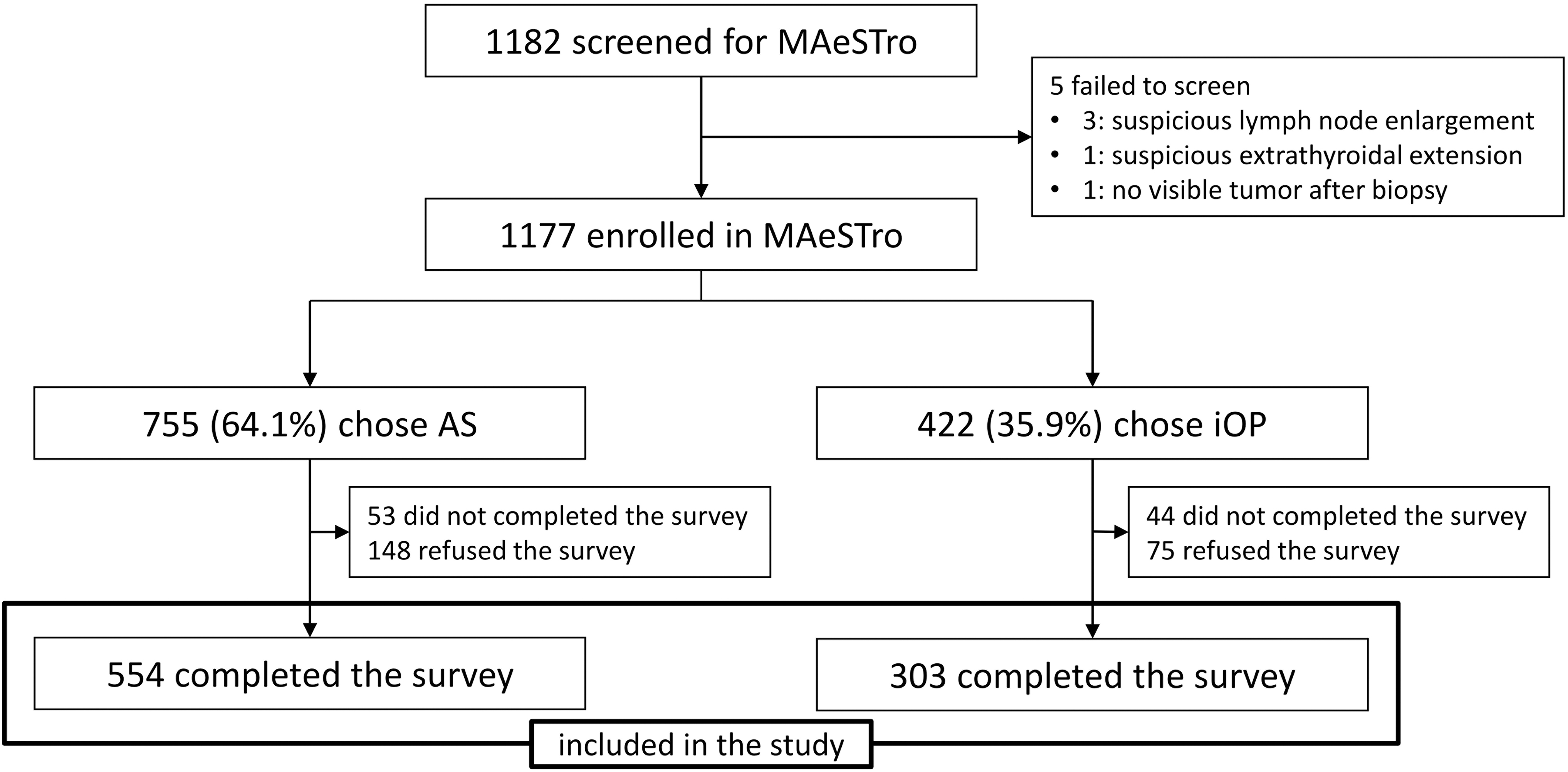
Study population and flow chart. AS, active surveillance; iOP, immediate surgery.
Analysis of the baseline characteristics of the 857 patients revealed that patients in the AS group were older and had smaller tumors than those in the iOP group (age, 49.4 ± 11.6 vs. 46.6 ± 10.7 years, p < 0.001; tumor size, 6.2 ± 1.6 vs. 6.8 ± 1.9 mm, p < 0.001; Table 1). Although the times since study enrollment, occupation, and comorbid malignancy of patients were not different between the AS and iOP groups, the proportion of patients with children was higher in the iOP group than in the AS group (67.3% vs. 46.4%, p < 0.001). The proportion of patients using the decision aid (Thyroid Cancer Treatment Choice) 15 was higher in the AS group than in the iOP group (76.5% vs. 47.5%, p < 0.001). The treatment choice was associated with the consulting physician's specialty and the center where the study was conducted.
Baseline Characteristics of Active Surveillance and Immediate Surgery Group
Data are expressed as mean ± SD or median (interquartile range).
Derived by Student's t-test.
Derived by chi-squared test.
Derived by Mann–Whitney U test.
p < 0.05.
AS, active surveillance; BMI, body mass index; DBP, diastolic blood pressure; iOP, immediate surgery; NCC, National Cancer Center; SBP, systolic blood pressure; SD, standard deviation; SNUBH, Seoul National University Bundang Hospital; SNUH, Seoul National University Hospital; Tg, thyroglobulin; TgAb, anti-Tg antibody; TSH, thyrotropin.
Patients who consulted with an endocrinologist chose AS more often than immediate surgery (530 vs. 76 patients, p < 0.001), and those who consulted with a surgeon chose immediate surgery more often than AS (227 vs. 24 patients, p < 0.001). In a multivariable analysis, patients who were >50 years of age (p = 0.020), whose tumor size was ≤5 mm (p = 0.015), and who consulted with an endocrinologist (p < 0.001) and used the decision aid (p = 0.005) in their decision-making process were more likely to choose AS (Table 2).
Multivariable Logistic Regression Analyses for Choosing Active Surveillance as the Initial Treatment of Low-Risk Papillary Thyroid Microcarcinoma According to Patients' Baseline Characteristics and Decision-Making Process
Dependent variable is choosing AS between AS and immediate surgery. Age, tumor size, children, use of decision aid, consulting physician, and center were entered as independent variables.
p < 0.05.
CI, confidence interval; PTMC, papillary thyroid microcarcinoma.
Patients' prior knowledge of low-risk PTMC treatment
Survey results on the patients' prior knowledge of low-risk PTMC treatment revealed that the proportion of those who were aware of AS as a treatment option for low-risk PTMC at the time of their treatment decision was higher in the AS group than in the iOP group (64.6% vs. 56.8%, p < 0.001; Table 3). In contrast, the proportion of patients who answered that they knew little about thyroid cancer treatment was higher in the iOP group than in the AS group (28.7% vs. 16.2%, p < 0.001).
Patients' Prior Knowledge of Low-Risk Papillary Thyroid Microcarcinoma Treatment
Data are expressed as n (%).
Derived by Fisher–Freeman–Halton's exact test.
p < 0.05.
Opinions or information influencing the treatment choice for low-risk PTMC
The opinions of patients and their physicians influenced the treatment choice of patients with low-risk PTMC (Table 4). Specifically, patients who chose immediate surgery were more influenced by the opinions of their family members than patients who chose AS (2.27 ± 1.79 vs. 1.97 ± 2.10, p = 0.025), whereas information from the media more strongly influenced patients who chose AS (0.79 ± 1.33 vs. 0.59 ± 1.02, p = 0.017).
Opinions or Information Influencing the Treatment Choice of Low-Risk Papillary Thyroid Microcarcinoma
Data are expressed as mean ± SD. Each value represents a relative value when the total influence to the treatment choice is 10.
Derived by Student's t-test.
p < 0.05.
Reasons for the initial treatment choice of low-risk PTMC
Among the patients who chose AS, 252 (45.5%) patients chose AS because surgery would be effective even after PTMC progression during AS, 107 (19.3%) answered they were worried about the complications of surgery, and 90 (16.2%) said they did not want to take thyroid hormone medication (Supplementary Table S1). Most patients who chose immediate surgery (250, 82.5%) answered that they chose surgery because they were worried about the progression of the thyroid cancer and were concerned about the expansion of the surgical range or additional treatment required after delayed surgery (Supplementary Table S1).
Physicians' attitudes and beliefs regarding AS
The attitudes and beliefs of physicians who consulted with patients with low-risk PTMC and discussed AS as an initial treatment choice were analyzed (Fig. 2). For the questionnaire, their opinions at the beginning of the study and their more recent opinions (June 2021), were both collected. None of the surgeons answered that they prefer AS for treatment of low-risk PTMC at the beginning of the study, whereas 3 of 13 endocrinologists reported that they preferred AS. Two physicians reported that at the beginning of the study their recommended treatment for low-risk PTMC was immediate surgery, without considering AS. However, at last evaluation, all physicians reported that they currently considered both AS and immediate surgery. At the beginning of the study, 2 of 13 endocrinologists and 3 of 6 surgeons did not accept AS as a major treatment option. All physicians answered that they currently accept AS as a major option for the treatment of low-risk PTMC. Most physicians reported that they believed that AS would not affect the survival rate of low-risk PTMC patients.

Survey results were collected from 19 physicians who consulted with the study participants and obtained informed consent from each patient. Thoughts at the beginning of the study and more recently (June 2021) were provided separately. PTMC, papillary thyroid microcarcinoma; RFA, radiofrequency ablation.
Compared with endocrinologists, surgeons tended to recommend immediate surgery when asked about the treatment recommended for patients with a life expectancy of >10 years (4 of 6 surgeons, 66.7% vs. 7 of 13 endocrinologists, 53.8%). Nonsurgical treatment, including AS and local therapy, was recommended more often in the more recent survey than at the beginning of the study (at the beginning of the study, 8 of 19 physicians, 42.1% vs. more recent, 11 of 19, 57.9%).
Discussion
In this study, the patients' age, tumor size, the use of a decision aid, and their consulting physician's specialty, were independently associated with the initial treatment choice for low-risk PTMC. Older patients with smaller tumors may have been more likely to choose AS because they learned about their excellent prognosis during the consulting process. The influence of the decision aid and the consulting physician's specialty on patient choice suggests the importance of the patient's knowledge of their disease, the source of information, method of communication, and attitude of their health care provider.
The results of our surveys of patients and physicians have several implications. Among low-risk PTMC patients who chose AS, the proportion aware that AS was a possible treatment option for low-risk PTMC was higher, and the proportion who knew little about thyroid cancer treatment was lower than among those who chose immediate surgery. These results imply that those patients aware of the good prognosis of low-risk PTMC and knowledgeable of AS were more likely to choose AS. Our results are consistent with previous studies. In a study of a focus group and individual interviews with 15 patients with PTMC, D'Agostino et al. 13 reported that those who chose AS considered PTMC as a common, indolent, and low-risk disease. The previous study that investigated QoL in the participants of MAeSTro reported that patients who opted for AS had a lower level of stress from their low-risk PTMC diagnosis than those who opted for immediate surgery. 11 In addition, the results indicated that patients who chose AS considered information from the media in their decision-making process more than those who chose immediate surgery, which suggested that patients who actively seek and study information about their disease tend to choose AS.
Notably, patients who chose immediate surgery were more influenced by their family members' opinions in their treatment decision. Family members have been reported to be not supportive of AS as a treatment option for localized prostate cancer. 19 An earlier study reported that “total eradication of cancer” was cited as the most important factor for the partners of patients with localized prostate cancer in deciding on the primary therapy. 20 Although 55% of partners acknowledged side-effects as an important aspect in decision making, only 6% cited this as the most important determinant. 20 Other studies of localized prostate cancer revealed that patients value the side-effects of treatment more in the decision process than their partners. 21,22 A qualitative study in patients with low-risk PTC reported that family consideration was a factor that contributed to the patients' decisions regarding cancer treatment and cited “family members wanted to get rid of cancer” as a reflection from patients who chose surgery. 14 In the current study, a univariate analysis indicated that patients with children were more likely to choose immediate surgery than AS but there was no significant association in the multivariable model.
In the current study, regardless of initial treatment choice, the most important considerations in the decision-making process for patients with low-risk PTMC were the opinions of the patient, their physician, and their family members. This result is consistent with a Canadian study reporting that personal perceptions about cancer or thyroidectomy and trust in health care providers strongly influenced a patients' disease management choices. 14 Among these factors, the influence of physician's opinion is noteworthy. According to the MAeSTro study protocol, 16 the physicians in this study shared explanatory material, including the pros and cons of AS and immediate surgery for low-risk PTMC, before initiating subject enrollment. Based on this, they were required to provide a sufficient and balanced explanation of the treatment options for low-risk PTMC and maintain a neutral attitude without intervening in the patient's decision-making process in choosing an initial treatment. Nevertheless, the study results revealed that the proportion of patients choosing AS varied according to the attitude of physicians regarding AS.
This suggests that the consulting physician's unbalanced framing of the treatment options is inevitable and nonverbal and intuitive communication in the explanation process can influence the patient's decision. In our study, all participants who enrolled at SNUBH, 85.6% of those who enrolled at SNUH, and 30.6% of those who enrolled at NCC consulted with endocrinologists, and the proportion of those choosing AS was highest at SNUBH and lowest at NCC. These data also suggest that the influence of the physician's attitudes might have contributed to differences in AS rates related to the center where the patients were treated.
Our study has some important clinical implications. Even though the physicians in the study were asked to employ neutral attitudes regarding AS, the proportion of patients choosing AS was associated with the physician's preference for AS. Moreover, the patients answered that their physicians' opinions influenced their treatment choice. Therefore, it is predicted that the information and opinions provided by the physician have a greater influence on the patient's treatment decision in actual practice than in this study. Moreover, physicians' recommendations have been reported to be not patient centered and influenced by nonclinical factors, such as personal preference and specialty. 23,24 Thus, physicians should have up-to-date clinical knowledge of low-risk PTMC treatment to provide sufficient, accurate, and balanced information to their patients and help them make the best decisions for their condition.
Considering the higher proportion of use of the decision aid in the AS group, a standardized and updated tool for the decision process could be of practical help for both patients and physicians. In this study, some of the survey items asked physicians to distinguish between their thoughts at the beginning of the study and their current thoughts. The results of these survey items from 19 physicians who consulted the study participants revealed that physicians' attitudes and beliefs about AS were more favorable as this prospective study progressed. Two survey studies reported in 2022 showed that 23% and 36% of physicians recommended AS for the treatment of low-risk PTMC. 25,26 The physicians in this study cited the lack of clear inclusion criteria and follow-up protocols, the anxiety of patients, and the possibility of missing an opportunity to cure as disadvantages of AS (Supplementary Table S2).
An advantage of AS mentioned was that the patient can avoid surgical complications and lifelong medication with thyroid hormones (Supplementary Table S2). These results are consistent with a recent national survey of endocrinologists and surgeons in the United States regarding AS for low-risk PTMC. 27 Therefore, if clinical evidence for AS in low-risk PTMC is accumulated and clearer inclusion criteria and follow-up protocols are established, physicians should be more supportive of AS, and the use of AS as a primary treatment option should increase. Altogether, a multifaceted approach, including improved terminology for thyroid cancer and nodules, the use of auxiliary tools for explanations and counseling, and education on the latest research results for physicians, is needed to produce the optimal patient-centered decisions in low-risk PTMC treatment.
Nonetheless, the current study has some limitations that should be considered when interpreting the results. First, the survey of the 19 physicians was conducted in June 2021, and the physicians were asked to answer some questions by recalling their opinions at the beginning of the study. Therefore, we could not perform statistical analyses with the small number of survey participants and the possibility of bias in the survey due to the inability to recall initial opinions cannot be excluded. Although the survey items were verified by the MAeSTro research committee, a survey expert was not involved in the survey design, and the possibility of bias due to the survey design cannot be excluded. Second, we collected survey data from the physicians who consulted with each study participant and signed informed consent. Although the physician who signed the informed consent generally conducted the consultations, some patients discussed their initial treatment of low-risk PTMC with two or more physicians over a variable time frame. Therefore, the results of this study, which only analyzed the opinion of the main counselor, may not accurately reflect these circumstances.
In addition, selection bias cannot be excluded because we did not randomize the consultation process with endocrinologists and surgeons. Third, this study did not include comprehensive demographic data of the study participants, such as education, employment, marriage, and socioeconomic status. There is a possibility that these demographic characteristics influence the treatment choice of patients with low-risk PTMC, and subsequent investigations considering more comprehensive factors are needed.
In conclusion, this study found that patient characteristics, physician-related factors, and the use of communication tools were significantly associated with the choice of AS in low-risk PTMC. The patient's prior knowledge of thyroid cancer treatment, the opinions or information the patient considers in the decision-making process, and the attitude and belief regarding AS of the physician can be considered as influencing factors. Therefore, sufficient support, including accurate and balanced information about the treatment of low-risk PTMC, should be provided to physicians and patients so that they can participate in a shared decision and choose the optimal disease management option.
Footnotes
Authors' Contributions
J.H.M., K.E.L., Y.J.P., E.K.L., Y.H., and J.Y.C. designed the study. Y.H., J.Y.C., E.K.L., C.H.R., S.W.C., E.-J.C., J.H.H., W.-J.J., Y.-S.J., S.-J.K., Y.J.L., H.W.Y., D.J.P., J.R., Y.J.P., K.E.L., and J.H.M. collected the data. J.H.M., S.K.P., and Y.J.P. analyzed the data. Y.H., J.Y.C., K.E.L., and J.H.M. wrote the article. Y.H., J.Y.C., E.K.L., C.H.R., S.W.C., E.-J.C., J.H.H., W.-J.J., Y.-S.J., S.-J.K., Y.J.L., H.W.Y., D.J.P., J.R., Y.J.P., K.E.L., J.H.M., J.-H.K., M.J.K., Y.K.K., C.Y.L., and J.Y.L. reviewed the article. All authors agreed on the final content of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by Seoul National University Hospital (Research Grant 25-2016-0010) and National Cancer Center (Research Grant 1810151).
Supplementary Material
Supplementary Material S1
Supplementary Material S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3